
Abstract
To analyze and evaluate the clinical efficacy of Chinese and Western medical techniques in the treatment of severe diabetic foot ulcers complicated with necrotizing fasciitis of the lower leg and summarize the treatment experience of such patients to identify a new method of limb salvage treatment. A total of 46 patients with severe diabetic foot ulcers and necrotizing fasciitis of the lower leg were treated with such techniques as surgical debridement, bone drilling, open joint fusion, and microskin implantation. Wounds were treated with moisture-exposed burn therapy (a regenerative medical treatment for burns, wounds, and ulcers) and moisture-exposed burn ointment (a traditional Chinese medicine); underlying diseases were also treated effectively. The wound healing time, rate of high amputation, and mortality of these patients were summarized, and the clinical efficacy of such treatments was evaluated. Of the 46 patients enrolled, 38 patients were cured, with a cure rate of 82.61%. The average wound healing time was 130 ± 74.37 days. Two patients underwent high amputations, with an amputation rate of 4.35%, and 4 deaths occurred, with a mortality rate of 8.70%. The combination of Chinese and Western medical techniques in the treatment of severe diabetic foot ulcers complicated with necrotizing fasciitis of the lower leg not only effectively saved patients’ lives and promoted wound healing but also greatly reduced the rates of high amputation and disability.
Introduction
In an ageing population, diabetes and diabetic foot ulcers have become clinically frequent and common diseases. In current Western medicine, high amputation is the main treatment for severe diabetic foot disease. Research data1,2 revealed the limb/toe amputation rate in patients with mildly, moderately, and severely infected diabetic foot who were treated with Western medicine treatment to be 2.8%, 46.0%, and 77.7%, respectively. A study by Aiping Wang 3 suggested that the amputation rate of patients with diabetic foot disease increased with Wagner's grading, and the rate of high amputation in patients with Wagner's grade-5 diabetic foot reached up to 100%.
Patients with diabetic foot also have high mortality. Foreign epidemiological surveys have suggested the 5-year mortality of patients with diabetic foot to be as high as 43% to 50%, increasing with the severity of the disease. 4 The mortality of patients within 1 year after high amputation was reported to be as high as 30%, the risk of serious diseases in the other limb within 2 years was 50%, and the mortality within 5 years after initial amputation was 70%. 5 In recent years, many clinical summaries have reported that the regenerative medical technology for burns, wounds, and ulcers in the treatment of severe diabetic foot ulcers at grades 3 to 5 can effectively promote wound healing, improve healing quality, and significantly reduce the rate of high amputation. 6 In addition to patients with grade-5 severe diabetic foot and entire gangrene (Wagner's classification), in clinical practice, some patients may have infected and necrotic diabetic foot ulcers that have broken through the ankle joint, rapidly spreading to and invading the lower limb, causing necrotizing fasciitis of the lower leg. These patients have complex, critical conditions and rapid disease progression. According to the surgical experience of Western medicine, the majority of such patients are treated by high amputation. However, if patients have underlying diseases or poor general health and do not meet the criteria for anesthesia and amputation, their treatment will be largely difficult, with high mortality.
Therefore, besides high amputation for patients with diabetic foot ulcers and necrotizing fasciitis of the lower leg, are other feasible treatments available in clinical practice, and can high amputation be avoided? What are the risks and mortality of limb salvage treatment? To answer these questions, the author treated 46 patients using combined Chinese and Western medical techniques in recent years. The combination regimen not only effectively saved patients’ lives, but it significantly reduced the rates of high amputation and disability. This article was written to share the author's extensive experience in the treatment of patients with severe diabetic foot ulcers complicated with necrotizing fasciitis of the lower leg and report their breakthroughs in this field.
Clinical Data
Diagnostic and Inclusion Criteria of Diabetic Foot Ulcer With Necrotizing Fasciitis of Lower Leg
Patients with diabetic foot ulcers whose infection and necrosis of the foot broke through the ankle joint and spread to and invaded the lower leg met the diagnostic criteria and were included in this clinical observation study.
Clinical Data
A total of 46 patients with diabetic foot ulcers complicated with necrotizing fasciitis of the lower leg who met the above diagnostic criteria were admitted to the hospital between January 2013 and December 2019. According to a comprehensive evaluation of wound manifestations and vascular conditions, these patients had mixed diabetic foot ulcers with necrotizing fasciitis of the lower leg (ie, infected with gangrene). None of these 46 patients were examined for severe vascular damage such as vascular occlusion.
The 46 patients comprised 34 males (73.91%) and 12 females (26.09%). Among them, the left foot was affected in 28 cases (60.87%), and the right foot was affected in 18 cases (39.13%). The patients’ ages ranged from 37 to 96 years, with an overall average age of 65.5 years. The males were aged 40 to 90 years, with an average age of 64.6 years, and the females were aged 37 to 96 years, with an average age of 67.6 years. There were 31 (67.39%) patients aged over 60 years. A total of 22 (47.83%) patients had serious infections with systemic inflammatory response and septic shock. During hospitalization, 5 (10.87%) patients were diagnosed with diabetes. Twelve patients had a 1 to 5-year history of diabetes, 21 (45.65%) patients had a 6 to 10-year history of diabetes, and 8 (17.39%) patients had a diabetes history longer than 10 years. A total of 21 (45.65%) patients had complicated hypertension and coronary heart disease, and 11 (23.91%) patients had complicated cerebral infarction.
Course of Wound Ulceration or Infection With Gangrene
There were 21 patients with acute onset (within 30 days) and 25 patients with acute aggravation of chronic ulcers due to infection. Six patients had a 30- to 60-day history of chronic ulcers, 12 patients had a history of 61 to 180 days, and 7 patients had 181-day histories or longer (the longest was an 11-year history of foot, ankle, and lower leg ulcers in 1 patient).
Special Conditions for Wounds
Twenty-six patients had a gangrene infection from the foot through the ankle joint to the inferior lower leg, 11 patients had an infection to the middle lower leg, and 9 patients had an infection to the superior lower leg. x-ray or computed tomography examination of the foot revealed soft tissue infection, subcutaneous pneumatosis, and/or pneumatosis in the joint cavity as well as bone destruction, osteomyelitis, and other manifestations. The affected feet of the 46 patients had black skin, necrosis, ulceration, discharge of pus, flushing, and obvious swelling, and there was high tension in the lower leg. During wound debridement, multiple latent cavities and sinus tracts with empyema, pneumatosis, and cacosmia were observed in the tendon, tendon sheath, and intermuscular space. After the latent cavities and sinus tracts were opened, the main findings were black degenerative necrotic fascia, tendons, and joint capsules as well as necrotic bone.
Methods
Systemic Therapy
Anti-Infective Therapy
After admission, the patients were given antibiotics effective against G− bacilli, G+ cocci, and anaerobes combined with anti-infective therapy by the experience of the clinicians, based on the characteristics of the patients’ microflora in the ward of our department, patients’ renal function, and the severity of infection. Any necessary adjustments to the treatment were made based on the results of a drug sensitivity test on the bacteria in the wound secretions. If patients with severe infection and systemic inflammatory response, sepsis, or septic shock showed a poor response after 1 to 2 days of empirical antibiotic treatment and there was no improvement (in shock or disease) and even aggravation, adjustments were made; alternatively, patients were administered efficient broad-spectrum antibiotics or a combination of antibiotics and anti-infective therapy. Generally, antibiotics were used for 7 to 10 days. During the use of broad-spectrum antibiotics or the combined use of antibiotics, wound secretions were sent regularly for culture to identify double infections. Based on the results of bacterial drug sensitivity, sensitive narrow-spectrum antibiotics were used promptly, and anti-infective de-escalation therapy was implemented.
Anti-Shock and Fluid Resuscitation Therapy
Patients with complicated shock received prompt anti-shock and fluid supplementation therapy; the fluids included lactated Ringer's solution, isotonic saline and other crystalloid solutions, human serum albumin, human blood plasma, succinylated gelatin, 706 plasma substitute, and other colloidal solutions. In the antishock and fluid supplementation process, blood pressure, heart rate, central venous pressure, urine volume, and blood circulation of the limb were observed closely, and the volume and speed of fluid supplementation were adjusted appropriately.
When treating hypovolemic shock, attention should be paid to preventing the occurrence of heart failure. If elderly patients and patients with cardiac insufficiency show a poor response after receiving fluid supplementation and anti-shock treatment, cardiotonic drugs (eg, Cedilanid and dobutamine) should be used promptly to increase heart output, while vasoactive drugs (eg, dopamine, metaraminol, and norepinephrine) should be used to improve and maintain blood pressure and increase the perfusion volume of tissues and organs.
Nutrition and Immunopotentiation Therapy
Enteral and intravenous nutrition were combined to replenish energy and calories.
Nerve Nutrition and Circulation Improvement Therapy
Intravenous circulation improvement drugs (eg, alprostadil and papaverine), lipoic acid for oxidation resistance, intramuscular cobamamide for nerve nutrition, and Chinese patent medicines, including Tongsaimai tablets and Mudan granules, were used in combination.
Maintenance and Consolidation Therapy for Underlying Diseases
The patients’ preprandial blood glucose levels were controlled below 10 mmol/L as much as possible, and the 2-h postprandial blood glucose level was maintained below 12 mmol/L. The blood glucose level was monitored to prevent hypoglycemia. Treatments were given to maintain the water–electrolyte balance and the acid–base balance, protect gastrointestinal function, and prevent the bleeding of gastrointestinal stress ulcers. Underlying diseases in internal medicine continued to be medicated to maintain a stable condition.
Psychological Counseling and Treatment
Most of the patients went from hospital to hospital and obtained unsatisfactory therapeutic effects or were advised to undergo high amputation. Thus, these patients were depressed, pessimistic, and refused treatment. They were given Chinese and Western medicines and psychological counseling services to help them rebuild their confidence and actively cooperate with the treatment regime.
Local Therapy
Local Debridement
Debridement was performed as early as possible if the patient's underlying diseases met the operation conditions and the shock symptom in the patient were initially controlled. The procedure was performed according to the wound treatment principles of surgical debridement and moisture-exposed burn therapy (MEBT) for necrotizing fasciitis of the lower leg.
After debridement, residual necrotic tissues were removed using the drug-and-knife combination, batch-by-batch method, and nibbling technique. If the wound was exposed for too long, moisture-exposed burn ointment (MEBO) was applied appropriately to prevent desiccation. If any deep latent cavity or sinus tract was newly found, it was opened as far as possible and drained fully. After the operation, MEBT or MEBO was used, as appropriate, to treat the wound.
Local Therapy With MEBT/MEBO
Early medication should be performed following the requirements of surgical sterility. The procedures of local dressing changing and wrapping for MEBT were as follows: (1) an appropriate quantity of MEBO was squeezed onto the sterile gauze and mixed them well to ensure that the MEBO was filled with the gauze. (2) MEBO was applied evenly on the wound surface at a thickness of 2 to 3 mm after cleaning the wound, followed by covering the wound with the prepared gauze containing MEBO. (3) The gauze was covered and wrapped with a cotton pad (1-3 cm thick), which extended 3 to 5 cm beyond the wound edge. The dressing was wrapped with a bandage or gauze. The dressing was changed 2 to 3 times a day according to wound exudation, and plaster fixation was used, if necessary, in the later stage to shape the wound. During the entire treatment process, liquefied substances, exudates, and necrotic tissues should be removed swiftly, and fresh MEBO should be applied promptly.
Treatment of Bone Tissue and Exposed Joint Wound
The bone marrow cavity drilling technique was used to drill holes in the exposed bone wound. A drill bit in an appropriate size was selected according to the size of the exposed bone area (generally, 1.5-2.5 mm). Drilling followed the bleeding standard for depth (ie, into the marrow cavity or cancellous bone) and the principle of a smaller spacing for a small drill bit and larger spacing for a large drill bit. For suppurative arthritis and exposed wounds of the joint cavity, the necrotic joint capsule and articular cartilage surface were removed, the joint cavity was opened, and joint fixation fusion was performed in the functional position using Kirschner wires (ie, open joint fusion). After the operation, the wound was treated carefully with MEBT/MEBO to retain healthy tissue, limb length, and limb function to the greatest extent.
Microskin Implantation and Culture Technique
When the granulation tissues in the wound grew well in the later stage, the microskin implantation and culture technique was used to accelerate wound closure. The specific steps used were as follows: (1) Skin removal: In the operating room, routine disinfection and draping were performed, and the granulation tissue was gently rinsed with normal saline. An area of skin with good elasticity and quality was selected as the skin donor site, and the skin removal area was determined by a ratio of approximately 1:20 (removal area to wound area). After local infiltration anesthesia was administered via local anesthetic, the epidermis was cut off with scissors (depth: about 0.2-0.3 mm, size: about 1-2 mm, spacing: about 2 mm) so that there was no bleeding at the skin donor site. (2) Microskin preparation: The removed epidermis was cut into microskin of about 0.5 to 1.0 mm in size using small scissors, and a small amount of normal saline was applied to keep it moist and prevent cell necrosis. (3) Implantation: The prepared microskin was implanted one by one into the granulation tissue of the wound using tweezers. The implantation depth was about 1.5 to 2.0 mm, and the spacing was about 0.5 to 1.0 cm (determined based on the quantity of microskin appropriate for the wound size). During the implantation, gauze containing a 1:100 000 ratio of epinephrine to normal saline was used to remove oozing blood. (4) Postoperative tissue culture: After implantation, the wound and the skin donor site were covered with the prepared MEBO gauze and cotton pad and were bandaged. After the operation, MEBO was used appropriately to treat the wound and was changed daily to encourage the growth of the skin tissue.
Scar Prevention Treatment and Functional Exercise in Convalescence
The patients were instructed to apply MEBO for consolidation and scar prevention treatment, attend regular outpatient appointments, and perform functional exercises and rehabilitation after discharge.
Results
Of the 46 patients, 38 were cured (closure of the wound), with a cure rate of 82.61%. Four patients who gave up treatment were discharged from the hospital automatically and were not followed up. Four deaths occurred, with a mortality rate of 8.70%, including 1 death each from myocardial infarction after high amputation, pulmonary infection, gas gangrene with septic shock, and decompensated liver cirrhosis with septic shock. Two patients underwent high amputation, with a high-amputation rate of 4.35%. Among the 38 cured patients, the wound healing time was 50 to 90 days in 2 patients, 91 to 120 days in 6 patients, 121 to 150 days in 10 patients, 151 to 180 days in 9 patients, 181 to 240 days in 4 patients, and 241 to 300 days in 7 patients, with an average of 130 ± 74.37 days. In 36 patients with successful limb salvage, 10 patients were paralyzed due to cerebral infarction, and 26 patients retained most limb functions and returned to self-care after treatment. Eleven patients under 60 years of age were cured and resumed their normal work.
Typical Case 1
General Condition
A 60-year-old male, Mr Zhang, was admitted to hospital on August 21, 2014, due to “ulceration and exudation of [the] left foot of more than 3 months’ duration and aggravated blackening and necrosis with redness, swelling, and heat pain of [the] lower leg of 1 week's duration.” He had a temperature of 38.7 °C, blood pressure of 79/51 mmHg, a heart rate of 106 bpm, and a respiratory rate of 22 bpm.
Specific Condition
Obvious redness, swelling, heat pain, and high tension were observed in the left foot, ankle, and middle inferior segment of the lower leg. The patient experienced wave-like sensations in that area. A black necrotic defective wound of 4 × 3 cm was observed on the lateral side of the foot; inside the wound were many necrotic soft tissues, with a discharge of pus with cacosmia. The deep latent cavity extended to the foot bottom, ankle, and lower leg.
Diagnosis on Admission
The diagnosis was a left diabetic foot ulcer complicated with necrotizing fasciitis of the lower leg, septic shock, systemic inflammatory response syndrome, type-2 diabetes, etc.
Course of Treatment
On the day of admission, the patient received active anti-shock treatment. On the fourth day, the patient's condition was stable, and he underwent debridement and drainage. During the operation, black necrotic tissues were removed, the latent cavity in the lower leg was cut open, and the wound was fully drained and opened. After the operation, the wound was treated appropriately using regenerative medical technology for burns, wounds, and ulcers. On September 23, 2014, the patient underwent microskin implantation. The postoperative local wound was treated with MEBT/MEBO, and the dressing was changed. On November 25, 2014, the patient was cured and discharged from the hospital. During the 5-year follow-up period, he had no recurrence or obvious scar hyperplasia, contracture, or dysfunction (Figure 1). The patient returned to normal walking and resumed work (Figure 3.1).

The treatment process of typical case 1 with a left diabetic foot ulcer complicated with necrotizing fasciitis of the lower leg using Chinese and western medical techniques. Wound condition (1) on admission, (2) after debridement on day 4 of admission, (3) after 40 days of treatment with MEBT/MEBO, (4) after 86 days of treatment with MEBT/MEBO and microskin implantation. (5) No scar hyperplasia or contracture during 1-month follow-up after discharge. (6) No scar hyperplasia or dysfunction (extension) during 30-month follow-up. (7) No scar hyperplasia or dysfunction (flexion) during 30-month follow-up. (8) No scar hyperplasia or dysfunction (extension) during 5-year follow-up. (9) No scar hyperplasia or dysfunction (flexion) during 5-year follow-up. Abbreviations: MEBO, moisture-exposed burn ointment; MEBT, moisture-exposed burn therapy.
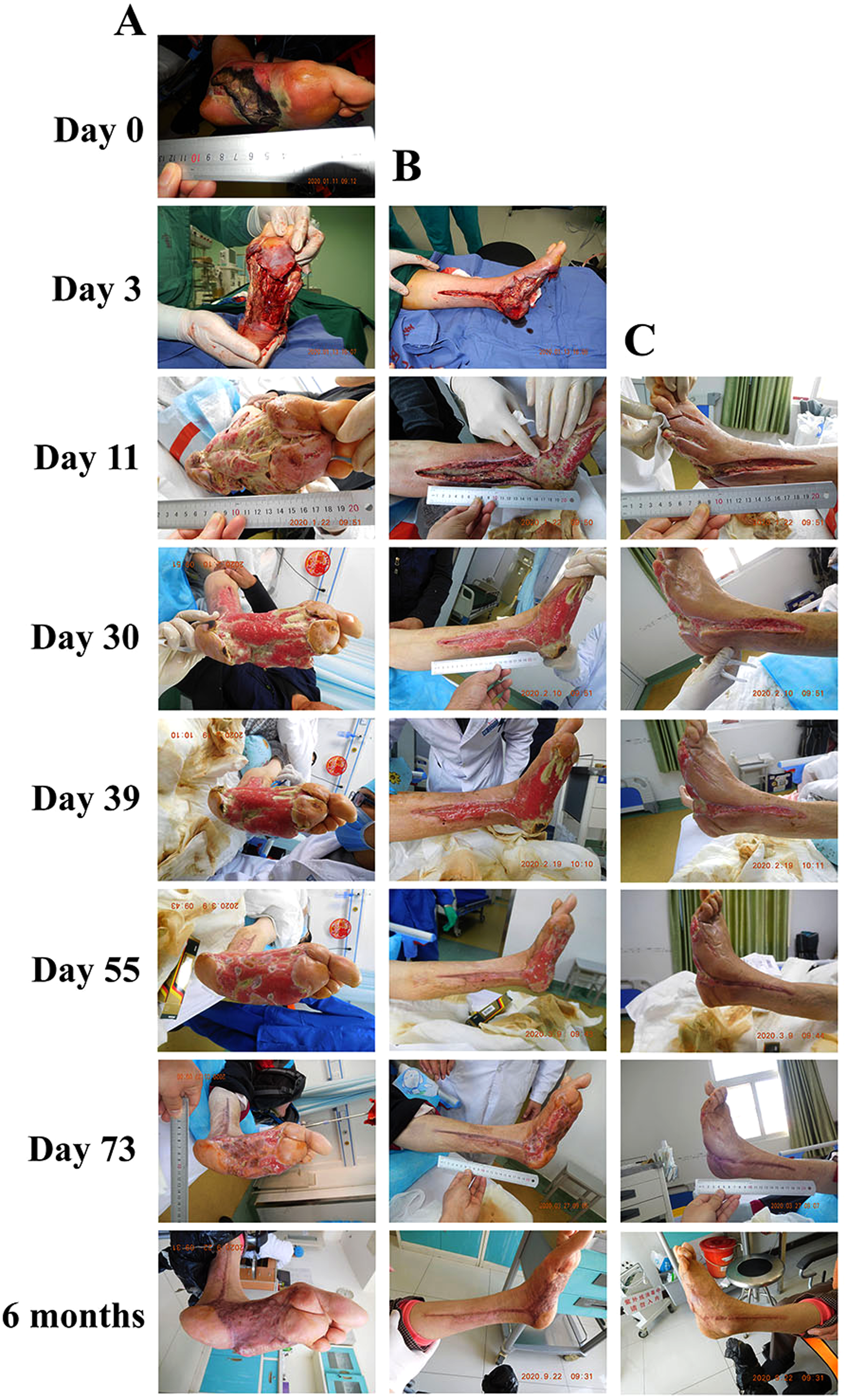
The treatment process of typical case 2 with a left diabetic foot ulcer complicated with necrotizing fasciitis of the lower leg using Chinese and western medical techniques. Wound condition on admission (Day 0), after debridement (Day 3), treating with MEBT/MEBO (Day 11) and after treating with MEBT/MEBO and microskin implantation (Day 30, day 39, day 55, day 73, and 6 months) in (A) pelma, (B) medial lower leg and (C) lateral lower leg. Abbreviations: MEBO, moisture-exposed burn ointment; MEBT, moisture-exposed burn therapy.

(1) The typical case 1 returned to normal walking and was satisfied with the therapeutic effect. (2) The typical case 2 was satisfied with the therapeutic effect.
Typical Case 2
General Condition
A 54-year-old female, Ms. Li, was admitted to the hospital due to “ulceration of left diabetic foot for 6-months period, and aggravated redness and swelling, blackening as well as festering pus for 1 week's duration.” The body temperature, blood pressure, heart rate, and respiratory rate of this patient were 39.8 °C, 76/43 mmHg, 112 bpm, and 28 bpm, respectively.
Specific Condition
The patient exhibited a series of symptoms including unclear mind, poor mental status, apathism, lower surface temperature of the extremities, and poor circulation at the extremities. The left foot of this patient presents as redness, swelling, ulceration, color blackening Pus flowing and stink, with marked redness and swelling in the local lower and middle calves (Figure 2A Day0-Day3, Figure 2B Day 0).
Diagnosis on Admission
The patient was professionally diagnosed with left diabetic foot ulcer complicated with necrotizing fasciitis of the lower leg, septic shock, type 2 diabetes, hypoproteinemia, water electrolytes and acid–base disturbances including hypokalemia, hyponatremia and hypochloremia, and asthma.
Course of Treatment
On the day of admission, the patient immediately received systemic therapies including antishock, anti-infection, cardiac strengthening, blood glucose control, and nutritional support, while her wound was treated with MEBT/MEBO accompanied with changing the dressing. After the shock was initially controlled, “the dilation in left foot and lower leg” was performed under peripheral nerve block anesthesia on the third day after admission. Apparently, necrotic tissue of the foot was removed from via above-mentioned operation, and the latent cavity of the dorsal foot, medial lower leg, and lateral lower leg was incised to help adequate drainage of the wound. After the operation, MEBT/MEBO accompanied with changing dressing strategy was applied to treat the local wound (1-2 times/day). On the 30th day after treatment, the dorsal foot wound healed naturally, and satisfactory growth of local tissue in the wounds of plantar, medial, and lateral lower leg wounds could be observed. Then the patient underwent microskin implantation, followed by intervening with MEBT/MEBO accompanied with changing dressing (1-2 times/day). On the 55th day, we could observe that the medial and lateral lower leg wounds have healed without keloidal hyperplasia. On the 73th day, the foot wound of patient was basically healed and she was discharged from the hospital. During the 6-month follow-up period, the patient had no recurrence or obvious scar hyperplasia or dysfunction, and she returned to normal walking (Figure 2A, B and C). The patient was satisfied with the efficacy (Figure 3.2).
Discussion
Diabetic foot is a serious complication of type-2 diabetes. In current Western medicine, the diagnosis of diabetic foot is mainly based on Wagner's classification. In diabetic foot grades 0 to 2, the success rate of limb salvage treatment is high. The rate of high amputation increases with severity for diabetic foot grades 3 to 5, and the high-amputation rate in patients with Wagner's grade-5 diabetic foot reaches up to 100%. The disease is characterized by its protracted course, recurrent condition, and high treatment costs, which severely impact patients’ physical and mental conditions and impose a heavy economic burden on their families. 7 The disease has become the leading cause of nontraumatic lower-limb amputations worldwide , 8 and according to statistics, 1 case of diabetic foot ulcer occurs every 30 s around the world. 9 A study by Chen Yongchong 6 on the high amputation of diabetic foot ulcers shows that high amputation cannot resolve underlying problems. Even if high amputation saves patients’ lives and improves subsequent survival rates, the associated psychological damage, amputation costs, postsurgery complications, the ability of patients to look after themselves following discharge, and family and social burdens are serious issues. At present, in Western surgery, the wounds of diabetic foot ulcers in grades 1 to 3 are treated mainly using negative pressure drainage, growth factors, platelet-rich plasma, functional dressings, and skin grafts. High amputation is the main therapy for the diabetic foot in grades 4 to 5, and unfortunately, the procedure is unavoidable for some patients.
Breakthroughs in limb salvage treatment for severe diabetic foot ulcers are difficult. In particular, patients with diabetic foot who have an infection breaking through the ankle joint are mostly complicated with acute necrotizing myofasciitis and accompanied by systemic inflammatory syndrome and septic shock. In Western surgery, most patients choose high amputation. Although some patients have indications for surgery, they do not meet the criteria for anesthesia and surgery due to age, complex underlying diseases, and complications, and they have to give up treatment. Therefore, the amputation and mortality rates in these patients are high. Despite aggressive treatment, the mortality of such patients ranges from 9.3% to 76%. 10 Therefore, when faced with such levels of high amputation and mortality in patients with severe diabetic foot, how can we effectively reduce the rates of high amputation and mortality under the premise of saving lives? Treatment with surgery alone still faces severe challenges and tests.
Great progress has been made in the diagnosis and treatment of diabetic foot, and specialist clinical experience has been accumulated in the limb salvage treatment of severe diabetic foot ulcers. Of note, the combination of Chinese and western medicine performed attracting advantages in facilitating limb salvage treatment for diabetic foot ulcers with necrotizing fasciitis of the lower leg, mainly manifesting as a higher healing rate, reducing the recovery time of the wound, avoiding amputation as well as high safety. For example, Ye et al 11 applied debridement of foot wounds combined with footbath by Chinese herbs for treating diabetic foot of patients and the total effective rate was 85.0% (50% in control) as compared to that of patients who were only treated with debridement of foot wounds. Zhong et al 12 treated patients with diabetic foot by the strategy of debridement of foot wounds combined with Chinese intervening (footbath and oral herbal Compounding) and a higher total effective rate (98.21%) was obtained.
The results of the present study show that when the anesthesia requirements are not high, less invasive debridement can be performed provided the patient's vital signs are relatively stable. Microskin implantation, bone marrow drilling, open joint fusion, and other techniques used in the later stage are minimally invasive and cause minimal trauma to patients. Moreover, after surgery, the wounds are treated properly with MEBT/MEBO. These Chinese combines western medical treatments effectively promote tissue regeneration, accelerate wound healing, and improve healing quality.
It is worth to note that many clinical reports have revealed that MEBT/MEBO for the treatment of severe diabetic foot ulcers in grades 3 to 5 can effectively promote wound healing, improve healing quality, and significantly reduce the rate of high amputation. Chen et al 6 used MEBT/MEBO to treat grade-5 diabetic foot ulcers. The cure rate was as high as 90.91%, the high-amputation rate was 9.09%, the wound healing time was 34 to 196 days (average = 71.16 days), and the costs were relatively low. Fu et al 13 demonstrated that the efficacy of MEBT/MEBO in treating diabetic foot was shown, with a high total effective rate of 90.0%. Similarly, a high cure rate (82.61%), as well as the lower high amputation rate (4.35%) have been observed in this report, in sharp contrast to the patients with severe diabetic foot ulcers intervened with western treatment, for example, Skin flap surgery with a high amputation rate at 16.22% reported by Chen et al. 14
Therefore, the combination of Western surgical techniques and Chinese medicine MEBT/MEBO can not only effectively promote wound healing and save patients’ lives but also greatly reduce the rates of high amputation and disability. This enables the limb salvage treatment of severe diabetic foot ulcers with necrotizing fasciitis of the lower leg and brings new hope to patients.
Regenerative medical technology for burns, wounds, and ulcers is a new treatment system that mainly involves MEBT/MEBO. Invented by Professor Xu Rongxiang, the technique's core mechanism induces and activates surviving cells in and around a wound into stem cells, and it cultures in situ tissue stem cells to regenerate skin tissues and organs. 15 The key technological link in the treatment of diabetic foot above grade 5 is the removal of necrotic wound tissues by liquefaction (necrosis removal) and the culture and regeneration of the remaining skin tissues (tissue regeneration) to eventually achieve wound healing. 16
Keeping the wound moist is the primary principle in treating various chronic wounds. A moist wound microenvironment can promote wound healing by preventing dehydration, promoting angiogenesis and collagen synthesis, and increasing the breakdown of necrotic tissue and fibrin. 17 Regenerative medical technology for burns, wounds, and ulcers (MEBT/MEBO) can not only provide a physiologically moist environment and achieve the physiological healing of chronic refractory wounds but also inhibit microbial proliferation, reduce exposure of the wound's surface, prevent the invasion of external bacteria in the wound, improve the body's immune defense mechanism, and prevent wound infection.18,19
As the core drug of the therapy, MEBO is a Chinese medicinal compound preparation ointment containing β-sitosterol, baicalin, berberine, and other antibacterial ingredients. The drug functions by controlling bacterial infection and keeping the wound moist. It can induce vascular reconstruction of new tissues, reduce vascular permeability, promote local blood circulation, improve tissue ischemia and hypoxia, regulate tissue metabolism, provide nutrients for regenerative tissues, and stimulate cell reproduction, thereby eventually promoting granulation growth, vascular reconstruction, and wound repair.20,21 A study 22 showed that moist wounds can maintain cell viability, promote the release of various growth factors, and up-regulate their activity. MEBO regulated the level of growth factors, including transforming growth factor-β1, vascular endothelial growth factor, and basic fibroblast growth factor, in the wounds of rats and promoted wound healing.
Furthermore, amino acids, fatty acids, vitamins, trace elements, and other ingredients in MEBO can act directly on wounds, be absorbed by local tissues, provide adequate nutrients for regeneration and repair of wound tissues, and promote wound healing. 23 After MEBO combines with necrotic tissues within a wound, it steadily penetrates the tissue layer. Various chemical reactions occur, and the tissue layer continually discharges yellowish liquefied substances. The necrotic tissues are liquified and discharged, ie, the necrotic tissues are expelled from the wound in a liquefied and invasive form to avoid the damage of mechanical debridement to wound tissues. 24 Meanwhile, MEBO can effectively and reasonably regulate the proportion of epithelial cells and collagenous fibers, the regeneration of necrotic tissues into normal tissues and preventing scarring. Finally, MEBO can preserve tissues to the greatest extent, maintain functions, and reduce the incidence of pigmentation. 25
Additionally, microskin implantation and culture technology could effectively accelerate the regeneration and healing of granulation wounds by accelerating the epithelium coverage speed of the flap-defective area by culturing epidermal tissue blocks and cell masses in the granulation wound, inducing and transforming them into skin stem cells, and culturing stem cells in the wound for proliferation, division, connection, and combination to form new skin organs. In recent years, the method has been widely used in the treatment of various chronic wounds and in patients with extensive burns, where it has shown good safety and effectiveness. It is characterized by low surgical trauma, low risk, low technical difficulty, simple operation, and greatly reduced treatment costs. 26 Compared with other skin-grafting techniques, this method can save skin sources, a reduction in the number of surgeries required, and shorten the course of treatment. One study 27 indicated that microskin implantation accelerates the wound closure rate by 40 times, thoroughly removes necrotic tissues, and reduces the risk of infection. Furthermore, the technique has a certain inhibitory effect on the formation of long-term scars and can reduce both scar formation and limb dysfunction caused by scar contraction. 28
Conclusion
This observational study of 46 patients with diabetic foot ulcers complicated with necrotizing fasciitis of the lower leg preliminarily confirmed that the combination of Chinese and Western medical techniques in the treatment of such cases can not only effectively save patients’ lives but also greatly reduce the rates of amputation and disability and maximize the integrity and functionality of the limb. The low-cost combined technique causes minimal pain during treatment and greatly reduces social and familial burdens. The clinical experience gained from the study can be used as an important reference for the treatment of severe diabetic foot ulcers with necrotizing fasciitis of the lower leg and provides a new method for treating severe diabetic foot ulcers. As the study was limited by its small sample size, further multicenter studies with larger sample sizes are required to demonstrate the rationality and universality of the findings.
Footnotes
Acknowledgments
The authors would like to acknowledge the hard and dedicated work of all the staff who implemented the intervention and evaluation components of the study.
Authors’ Contributions
Yongchong Chen conceived the idea and conceptualized the study. Taian Zhang and Kai Zhang collected the data. Yunzhu Wang, Chao Meng, Chunfang Qin, and Bohui Zhang analysed the data. Qing Li and Yunzhu Wang drafted the manuscript, then Yongchong Chen reviewed the manuscript. All authors read and approved the final draft.
Data Availability Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
The authors confirm that they have read the Editorial Policy pages. This study was conducted with approval from the Ethics Committee of Beijing Fengtai Hospital of Chinese Medicine (Nanyuan Hospital, Fengtai District, Beijing). The approval date is July 14, 2019, and the approval number is 2019NY-024. This study was conducted in accordance with the declaration of Helsinki.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from all participants.