
Abstract
We aimed to investigate adherence to at-home monitoring of foot temperature and its association with patient-, disease- and behavior-related factors, in people with diabetes at high risk of ulceration. We analyzed 151 participants in the enhanced therapy arm of the DIATEMP trial (all at high diabetes-related foot ulcer risk) who aimed to perform and log foot temperatures daily for 18 months or until ulceration. Adherence was the proportion of measurement days covered (PDC), with being adherent defined as PDC≥70%. If a hotspot was recorded, adherence to subsequently reducing ambulatory activity was assessed. Multivariate logistic regression analysis was performed to investigate associations with adherence. We found ninety-four participants (62.3%) adherent to measuring foot temperatures. This was higher in months 1-3 versus months 4-18: 118 (78.1%) versus 78 (57.4%; P < .001). Of 83 participants with a hotspot, 24 (28.9%) reduced ambulatory activity. Increasing age (P = .021, OR = 1.045) and better self-care (P = .007, OR = 1.513) were positively associated with adherence to measuring foot temperature. In conclusion, in people at high diabetes-related foot ulcer risk, adherence to measuring foot temperature was high in the first months after study commencing, but dropped over time. Adherence to reducing ambulatory activity when a hotspot was found was low over the entire study period.
With the continued rise in prevalence of diabetes, diabetes-related complications including foot ulceration also increase.1-4 Infected ulcers are the main cause for diabetes-related hospitalization and lower-extremity amputation.5,6 Furthermore, approximately 40% of people with diabetes who heal from an ulcer will have a recurrent ulcer within one year. 7 Therefore, prevention of (recurrent) foot ulcers is important.
Treatment for the prevention of foot ulcers includes patient education, routinely wearing appropriate footwear, regular (self-) inspections, foot examination by health care providers of the at-risk foot, and treatment of risk factors for ulceration (eg abundant callus). 8 Most of these approaches require people with diabetes to conduct frequent, most often daily, foot-related self-management activities. However, adherence to these activities is challenging for people with diabetes at high risk of ulceration. 9 For example, rates around 60% for footwear adherence were found in one review, 10 and two other studies found rates of adherence to daily foot inspection of 38.7% and 47%.11,12 Despite the importance of adherence in ulcer prevention, a recent systematic review showed that interventions to improve this adherence to self-management strategies for high-risk people with diabetes have hardly been investigated. 13
A self-management intervention recommended in international guidelines that reduces the risk of foot ulceration and requires patients to be adherent is at-home monitoring of foot temperature, followed by a reduction of ambulatory activity if a locally increased foot temperature is found. 8 This intervention is based on the premise that ulcers are preceded by increased local skin temperature due to inflammation and enzymatic autolysis of tissue as a result of being ambulatory. 14 Two meta-analyzes showed that at-home monitoring of foot temperature is an effective intervention in reducing risk for ulcer recurrence in people with diabetes.15,16 One of the four Randomized Controlled Trials (RCT) informing these meta-analyzes showed that ulcers were significantly less likely to develop in participants that were adherent to measuring foot temperatures compared to those who were non-adherent. 12 The most recent, and largest RCT on the topic, that was not yet included in these meta-analyzes, showed a smaller but still positive effect for the intervention. 17 More importantly, the study confirmed the importance of adherence, with a large preventative effect shown in participants who were adherent to measuring foot temperature and reducing ambulatory activity when a hotspot was found. 17 Given the importance of adherence to this self-management intervention and the lack of studies investigating factors associated with this adherence, more insight is needed. Such insights are important for future research and clinical practice, as it may help determine avenues to improve adherence, and strategies to determine who may benefit most from this intervention.
The aim of this study was to assess the level of adherence of at-home monitoring of foot temperature and in reducing ambulatory activity when a hotspot was found in people with diabetes at high risk of foot ulceration. Furthermore, we aimed to investigate patient-, disease- and behavior-related characteristics associated with adherence to at-home monitoring of foot temperature.
Subjects
The study population consisted of people with diabetes who were at high risk of developing a foot ulcer. These were people with diabetes mellitus type 1 or 2, aged 18 or above, with loss of protective sensation based on peripheral neuropathy and a history of foot ulceration in the preceding four years, or a diagnosis of Charcot neuro-osteoarthropathy (ie International Working Group on the Diabetic Foot (IWGDF); IWGDF risk 3). 8 Exclusion criteria were a foot ulcer, foot infection (including cellulitis of the lower limb), active Charcot neuro-osteo-arthropathy or severe illness that would make 18-months survival improbable. 17
Materials and Methods
We used data derived from the enhanced therapy group of a multi-centre randomized controlled trial (RCT) on the effectiveness of at-home monitoring of foot temperature to prevent foot ulcer recurrence in diabetes (DIATEMP). 17 To analyze adherence to measuring foot temperatures, we included participants who were randomly assigned to enhanced therapy, consisting of usual care plus daily at-home infrared foot temperature monitoring. The DIATEMP study was conducted according to the principles of the Declaration of Helsinki (64th version, October 2013) and in accordance with the Medical Research Involving Human Subjects Act. In addition, the study was registered in the Netherlands Trial Registration (ID: NTR5403), approved by the research ethics committee of the participating centers, and written informed consent was obtained prior to inclusion from all participants. Details of the DIATEMP study are described and published elsewhere. 17 The following sections only contain key methods relevant for the current analyzes.
A sample size calculation for clinical effectiveness was performed in the DIATEMP study (304 eligible participants were required). However, no specific sample size calculation was performed for the analyzes described in this manuscript.
Setting of the Study
Participants were enrolled from the multidisciplinary diabetic foot clinics of three university hospitals and four community hospitals, and from four affiliated podiatry practices, spread across the Netherlands. Follow-up was 18 months or until ulceration at or adjacent to a measurement site, or death. Prematurely terminating at-home foot temperature measurements was not considered an endpoint of this study. If a participant decided to stop daily foot temperature measurements, their reason for this was obtained (where possible) and categorized as either “for personal reasons’, “not returning the temperature log without reason” or “unknown, due to loss of contact with the participant”.
At-Home Foot Temperature Monitoring
At-home monitoring of foot temperature took place on a daily basis using an infrared thermometer (TempTouch®, Diabetica Solutions, San Antonio, TX, USA). Participants measured temperatures at six to eight predefined locations on the plantar surface of both feet. Participants entered recorded temperature values at each location in a logbook and were instructed to return the logbook to the study coordinators. In order to remind participants, standardized text messages were sent (twice a week to participants that were not adherent, and once every 4 weeks to participants that were adherent) and 3-monthly phone calls by the researchers were performed to monitor progress, adherence and outcomes.
Participants were asked to measure foot temperatures daily, preferably in the morning directly after waking up. If skin temperature measured in a region was >2.2 °C higher than in the corresponding region on the contralateral foot for two consecutive days, this was called a “hotspot”. In that event, the participant was instructed to reduce ambulatory activity with approximately 50% until foot temperature differences normalized (≤2.2 °C temperature difference) and to contact their podiatrist. Participants who recorded a hotspot were instructed to mark the hotspot in the logbook and record their subsequent actions (ie reducing ambulatory activity by 50% and contacting their podiatrist). All above instructions were also stated in the logbooks, to help remind the participant for the actions needed.
Primary and Secondary Outcomes
The primary outcomes for the current study were: [1] adherence to daily at-home monitoring of foot temperature; and [2] adherence to reducing ambulatory activity following hotspot detection (only applicable in participants with at least one hotspot). Participants were considered to have adequate adherence when measured temperature values were recorded in the logbook on ≥70% of the days that a participant participated in the study (days from study commencement until a study endpoint). This percentage was expressed as the “proportion of days covered” (PDC), calculated by dividing the number of days a participant entered their recorded temperature values in the logbook by the total number of days participated in the study (ie until a study endpoint occurred).
Adherence to at-home monitoring of foot temperature included measuring and logging foot temperatures at all pre-defined locations on the plantar surface of each foot on a given day, and returning the logbooks to the study coordinator. In order to assess adherence in a broader perspective and for sensitivity analysis, additional cut-off values (PDC ≥50% and PDC ≥80%) were used for secondary analysis. Adherence to daily foot temperature measurements was also assessed separately for months 1-3 of follow-up and for months 4-18, to investigate differences between short- and long-term adherence.
Adherence to reducing ambulatory activity when participants marked a hotspot included a participant recording in their logbook to have reduced ambulatory activity by approximately 50% for each day the hotspot was present. Being adherent was defined as reporting offloading the foot by reducing ambulatory activity with at least one hotspot detection during follow-up. We also reported the number of participants who contacted their podiatrist when identifying a hotspot, but this aspect was not part of the analysis of adherence in this study.
Associations with Adherence
Participant-, disease- and behavior-related characteristics used in the regression analysis to investigate their association with adherence were assessed at baseline through physical examination, anamnesis and questionnaires.
All factors are listed in Table 1. Alcohol consumption was classified as none vs. more than 1 unit per week and employment as none vs. any; retirement was considered as unemployed. If participants were treated by a nephrologist or ophthalmologist, they were considered to have diabetic nephropathy or diabetic retinopathy, respectively. The social economic score (SES) was assessed per participant using their postal code, with status per postal code provided by the Netherlands Institute for Social Research (outcome ranging from −5 for lowest possible SES to + 5 for highest possible SES). The assessment of self-care is described in appendix A.
Participant-, Disease- and Behavioural-Related Characteristics for all Participants During the Total Study Period.
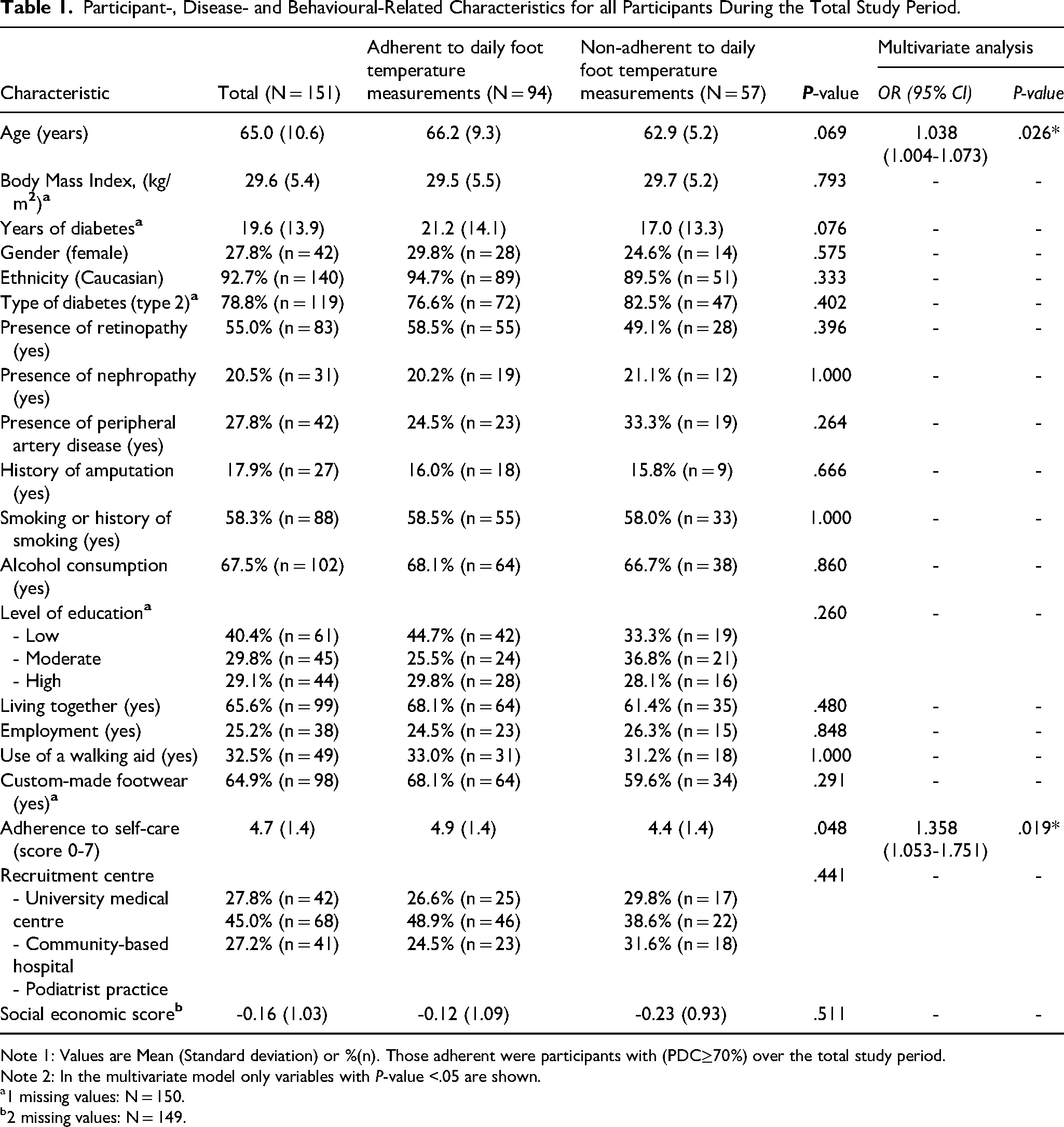
Note 1: Values are Mean (Standard deviation) or %(n). Those adherent were participants with (PDC≥70%) over the total study period.
Note 2: In the multivariate model only variables with P-value <.05 are shown.
1 missing values: N = 150.
2 missing values: N = 149.
Statistical Analysis
For all participant characteristics and outcomes, descriptive statistics using numbers, percentages, means and standard deviations (SD) were obtained. To assess group difference, Wilcoxon signed rank tests were performed. This non-parametric statistical test was performed due to violating the condition of a normal distribution of data. To investigate associations with being adherent (expressed as adherent / non-adherent), univariate logistic regression analyzes were performed and all variables with a P < .20 were entered in a multivariate logistic regression using backward selection. Linear regression with adherence (expressed as PDC) as outcome was not possible due to violating the condition of a normal distribution. All statistical analyzes were performed using SPSS statistical software (version 26, IBM Corporation, Armonk, NY). All tests were two-sided and used P < .05 as significance level.
Results
Study Population
Participant characteristics for the 151 included participants are described in Table 1 and stratified for: all participants, those adherent, and those non-adherent to at-home monitoring of foot temperature (using PDC≥70% cut-off).
Out of a maximum 548 possible measurement days in 18 months follow-up, mean days until study endpoint was 435 (range 16-548) (Figure 1). Concerning study endpoints, 44 participants (29.1%) developed an ulcer, 5 participants (3.3%) died and 102 participants (67.5%) completed follow-up. Key reasons for prematurely ending foot temperature measurements are shown in Figure 1.
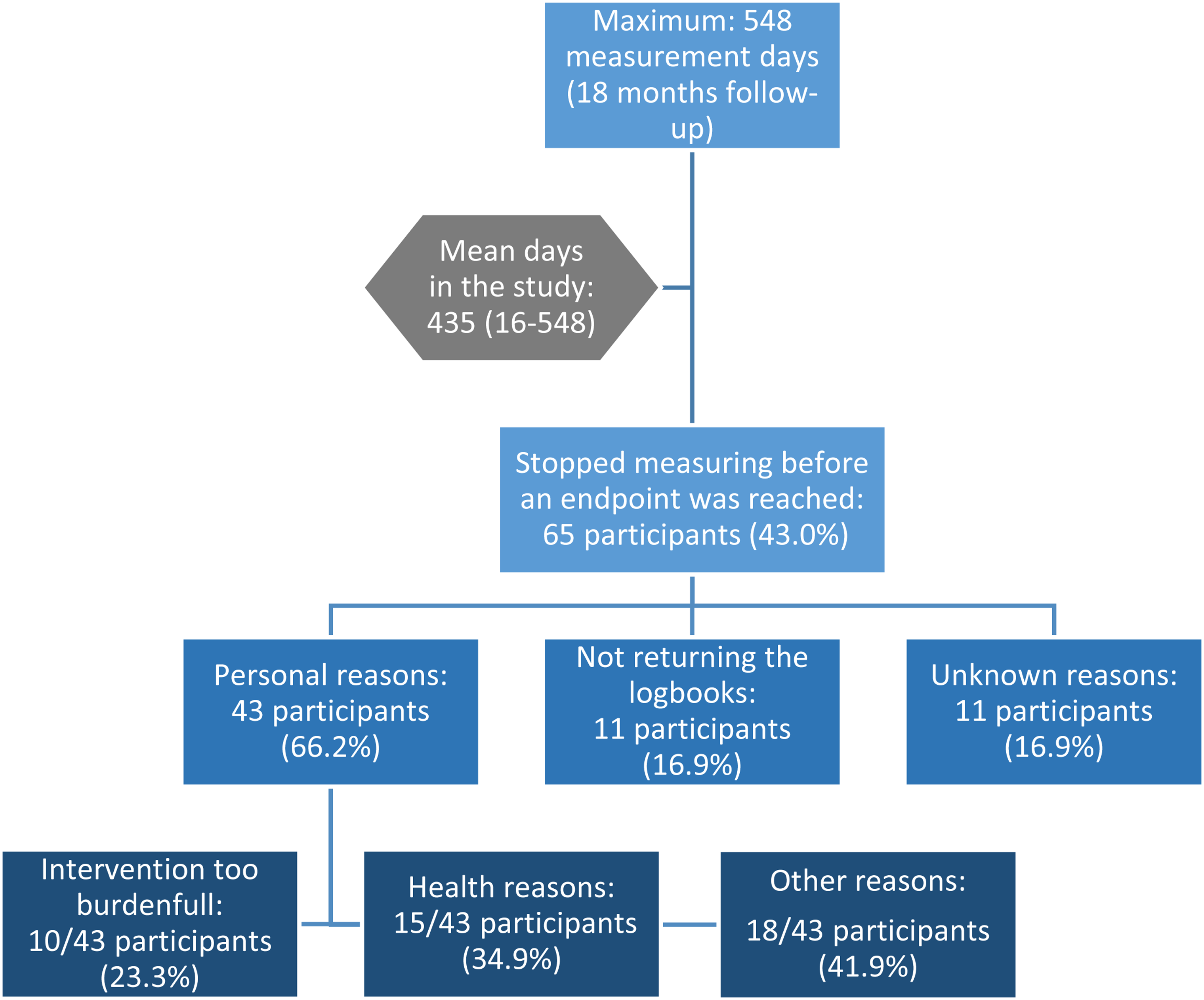
Key reasons for prematurely ending foot temperature measurements.
Fifteen participants (9.9%) did not measure their foot temperature at all, another 15 participants (9.9%) developed an ulcer within the first 3 months. A total 40 participants (26.5%) measured foot temperature for ≥500 study days.
Adherence to Measuring Foot Temperatures
Proportion of Days Covered (PDC)
In 151 participants, the mean PDC was 65.2%. Seventeen participants (11.3%) measured all study days (PDC = 100%), of which 7 until 18 months follow-up and 10 until ulceration. In months 1-3 of the study, mean PDC of 151 participants was 79.8%, and 58 participants (38.4%) measured all study days in month 1-3. In months 4-18, mean PDC was 59.3% in 136 participants and 16 participants (11.8%) measured all study days.
Adherent and non-Adherent Participants
A total 94 participants (62.3%) were adherent to at-home monitoring of foot temperature (PDC ≥70%) until a study endpoint. In multivariate analyzes, being adherent was positively associated with increasing age (P = .026, OR 1.038, 95% CI 1.004-1.073) and a higher self-care score (P = .019, OR 1.358, 95%CI 1.053-1.751), see Table 1.
With cut-off values of PDC ≥50% and PDC ≥80% for being adherent, a total 102 (67.5%) and 84 participants (55.6%), respectively, were adherent. Multivariate analyzes using these secondary cut-off values showed the same associated characteristics as for the cut-off value PDC ≥70%: increasing age (P = .007 with PDC≥50% and P = .045 with PDC≥80%) and higher self-care score (P = .014 for both PDC≥50% and PDC≥80%).
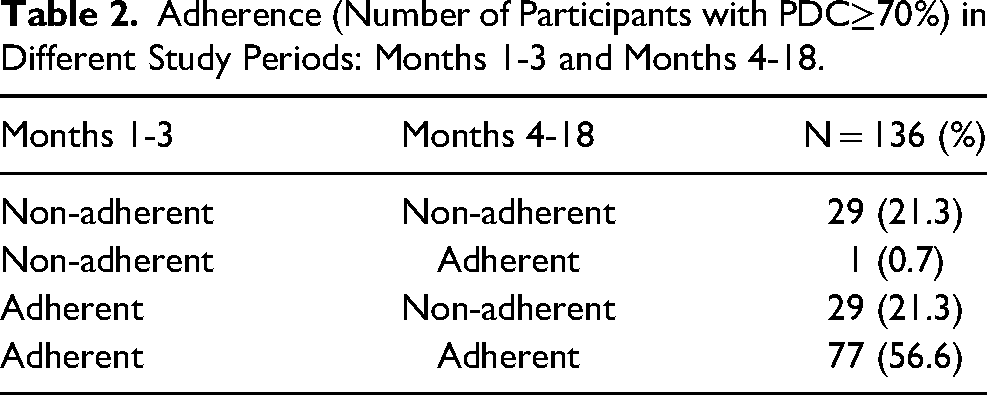
Of the 151 participants, 118 (78.1%) were adherent to monitoring foot temperature in months 1-3 versus 78 participants (of 136 participants) (57.4%) in months 4-18 (P < .001). Of the 136 participants that still participated after the first three months, adherence for both periods (months 1-3 vs. months 4-18) is shown in Table 2. Of the 106 participants that were adherent in months 1-3, 77 participants (72.6%) remained adherent during the rest of the study period. Of the 30 participants that were non-adherent in months 1-3, 1 participant (3.3%) became adherent in months 4-18.
Adherence (Number of Participants with PDC≥70%) in Different Study Periods: Months 1-3 and Months 4-18.
Adherence Following Hotspot Detection
A total 83 participants measured at least one hotspot during follow-up as based on their temperature data recorded in their logbook. Of these 83 participants, 50 participants (60.2%) actually indicated that they found a hotspot by checking the box in their logbook. Following the hotspot, 24 participants (28.9%) reported to have decreased their ambulatory activity and 14 (16.9%) to have contacted their podiatrist. Of these, 12 participants (14.5%) indicated they both reduced their ambulatory activity and contacted their podiatrist. Following multivariate analyzes, participants who were adherent to decreasing their ambulatory activity following hotspot detection had a lower mean self-care score (P = .044, OR 1.502, 95%CI 1.011-2.231; Table 3).
Associations of Participant Disease and Behavioural Characteristics with Adherence in Participants That Measured at Least one Hotspot During Follow-up as Based on Their Temperature Data Recorded in Their Logbook.
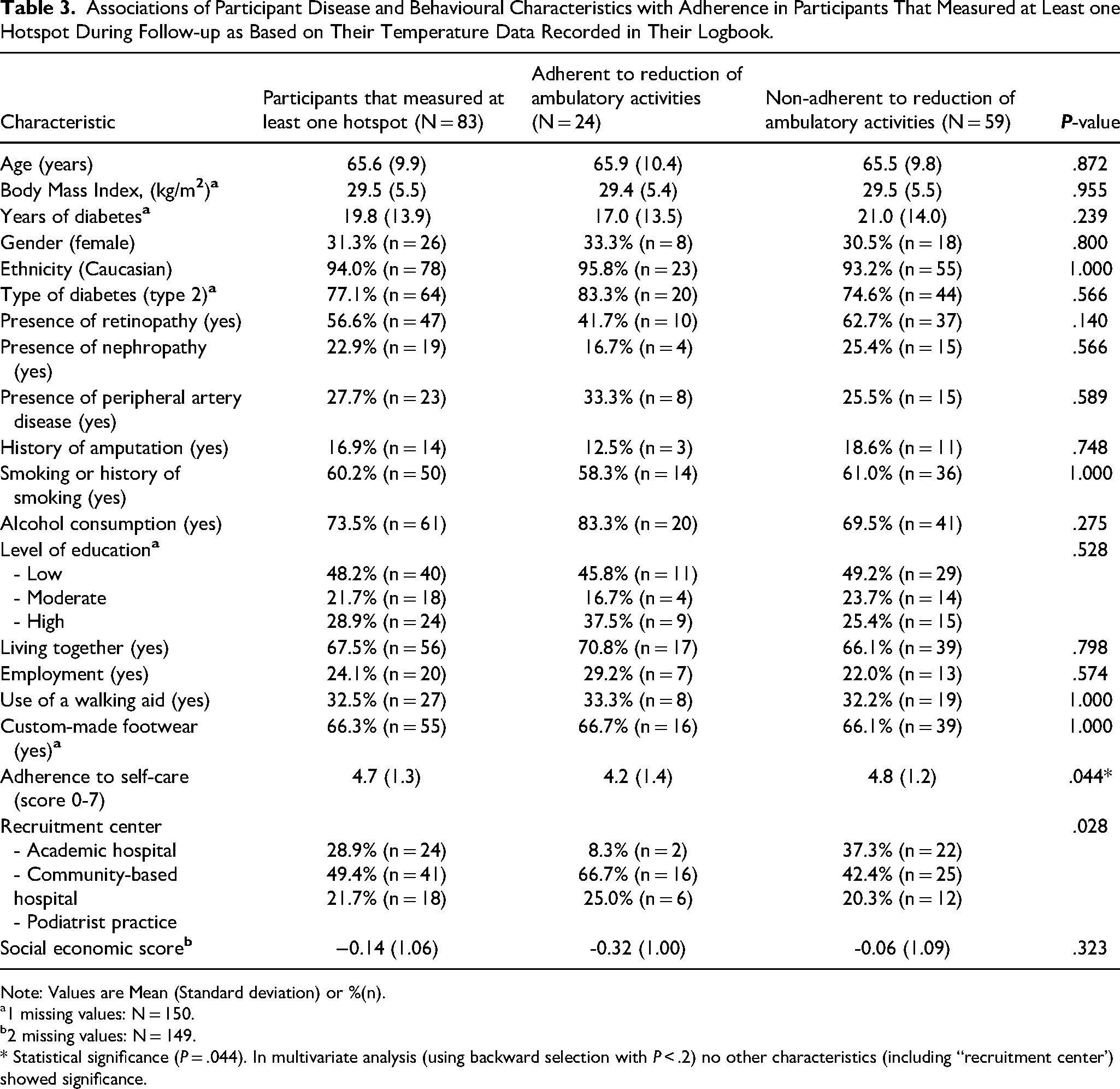
Note: Values are Mean (Standard deviation) or %(n).
1 missing values: N = 150.
2 missing values: N = 149.
* Statistical significance (P = .044). In multivariate analysis (using backward selection with P < .2) no other characteristics (including “recruitment center’) showed significance.
Discussion
At-home measurement of foot temperatures in people with diabetes at high risk of ulceration is a self-management strategy with the highest reported reduction in incidence of foot ulcer recurrence compared to usual care of all prevention strategies.15,16 This is especially the case for people who are adherent to reducing their activity when a hotspot is measured.12,17 We investigated in detail, adherence to at-home measurement of foot temperature, adherence to reducing activity when a hotspot was found, and factors associated with being adherent.
We found 62.3% adherence to measuring and logging foot skin temperature, while adherence to activity reduction following hotspot detection was low (28.9%). A recently completed RCT conducted in a low income setting (Peru) showed that 87% of the study participants were adherent to ≥80% of daily temperature measurements among those who returned their logbook. 18 This seems higher compared to our study, but if participants who did not return their logbook were counted as non-adherent, adherence was similar with 60%. 18 This percentage is also similar to percentages found for other behaviors on self-management in high-risk people with diabetes, such as an adherence of 61% and 52.5% to wearing custom-made footwear found in two different studies, and general adherence to a variety of self-management methods in people with diabetes, with a reported rate of 67.5% based on a meta-analysis of 23 studies. 12,19,20 The necessity of having to measure foot temperature on a daily basis with the aim of not getting an outcome (in this case a foot ulcer) can be described as a performance avoidance goal. 21 Such goals are challenging to maintain, and finding around 60% of participants adherent to this self-management strategy during a study that lasted 1.5 years can still be seen as a relatively high adherence. However, in order for at-home monitoring of foot temperature to be effective in reducing risk of ulcer recurrence, reducing ambulatory activity following hotspot detection is crucial. The 28.9% adherence to this activity reduction clearly shows that this adherence needs to be improved for the intervention to be of more value in the reduction of risk for foot ulcer recurrence.
We found a significantly higher adherence in the first 3 months (78.1%) compared to the following 15 months (57.4%), which suggests that the participants had difficulties with remaining adherent over time. Such a reduction in adherence is understandable considering the performance avoidance goal, and stresses that it is important to continue to support patients with maintaining their self-management routine in ulcer prevention, as preventing foot ulcers is a life-long challenge for people with diabetes who are at high risk.
Two factors were associated with higher adherence in foot temperature monitoring in multivariate analyzes, higher age and better self-care. Increased age (over 55 years old), has previously been associated with a higher adherence to general self-management practices in people with diabetes.19,22 However, the contrary is also reported. 23 An overview of systematic reviews showed a “concave pattern” of the influence of age on medication adherence, ie “lower adherence in young age groups, increasing adherence with a peak in middle to older age groups and lower adherence in very old age groups”. 24 As our population predominantly consisted of those in middle to older age, and few of very old age, this might be an explanation for our findings. The association between higher self-care scores and higher adherence is understandable, as patients who are already adherent to foot-related self-management can be expected to better integrate foot temperature measurements in their daily routine.
The most frequently reported reason for discontinuing the intervention, and thereby becoming non-adherent, were related to the burden of the intervention. Either because the intervention itself was perceived as too much work, or it was the burden of yet another self-management intervention in a situation of poor health that participants did not wish to add to their daily routine of managing their disease. Current technological developments in this intervention may decrease this burden and help improving adherence. For example, automatic logging of measurement data and automatic calculation of temperature difference and identification of a hotspot via foot mats, socks, or smartphone applications.25-27 However, none of these instruments have yet been tested for efficacy in reducing ulcer incidence in people with diabetes, and also each of these new techniques has its disadvantages. 28
A key finding in our study was the poor adherence in reducing ambulatory activity after participants identified a hotspot. This change of behavior following hotspot detection is the most important aspect of this intervention, mediating the ulcer risk by changing the mechanical load on the foot; measuring foot temperature is merely a conduit to identify the potential risk. Surprisingly, in our analysis we found lower self-care scores to be associated with higher adherence in reducing ambulatory activity, which contrasts with the association of this factor with adherence to the temperature monitoring, and also with clinical reasoning. While there is no clear explanation for this finding, a potential hypothesis could be that those with higher self-care scores implement the measuring of foot temperature in their daily routine, yet without fully understanding the necessity of changing their behaviors following hotspot detection. As such, they have a higher likelihood of detecting a hotspot and failing to act upon it. However, the analysis was performed on a smaller subgroup (n = 83) and with a mean difference of only 0.6 (on a score of 0-7) between those adherent and those not, clinical significance of this finding might be limited. With no other factors associated with low adherence to reduction in ambulatory activity, we unfortunately could not identify groups to target to improve this aspect of the intervention, more research is needed to identify ways to improve this aspect of the intervention.
Limitations
This is the first study with an in-depth analysis of the adherence of people with diabetes at high risk of foot ulceration to at-home foot temperature measuring for ulcer prevention. However, some limitations apply. First, adherence was determined based on self-reported data of foot temperature measurements in logbooks. Secondly, the cut-off criterion of PDC≥70% to classify a participant to being adherent was not evidence-based. In studies assessing adherence to medication or use of custom-made footwear, an 80% cut-off is more common. 29 Using 70% as cut-off value was based on clinical reasoning that recording foot skin temperature on 70% of the days would still result in a high chance for hotspot detection when temperature differences would be found. A third limitation was that we could not take patients’ (health) beliefs or other behavioral characteristics into account. Previous studies show that increased adherence to medical treatment and self-care in diabetes is associated with higher perceived disease severity and positive attitudes. 30 In addition, no specific sample size calculation was performed for this study, as no information on adherence from other studies on at-home monitoring of foot temperature was available at the start of the study. Finally, we used a non-validated questionnaire, commonly used by Dutch podiatrists, to assess self-care behavior. However, most of the items in this questionnaire are identical to some validated self-care scales (ie the “diabetes foot self-care behavior scale’), so we expect that this lack of validation did not affect our results to a significant extent. 31
Conclusion
In people with diabetes at high risk of ulceration, adherence to measuring foot temperature at home was high in the first months after commencing. However, adherence dropped over the longer-term, while adherence to reducing ambulatory activity when a hotspot was found was low over the entire period. We could not identify specific target groups for this aspect of the intervention.
The implication of the study findings for clinical practice is the importance of continuous support to measuring foot temperatures over time, to ensure people with diabetes at high risk of ulceration understand the mechanism and adhere to activity reduction following hotspot detection.
Footnotes
Acknowledgments
We thank all the employees and colleagues from the participating hospitals and podiatrist practices for their cooperation. The DIATEMP trial was funded by ZonMw (the Netherlands Organization for Health Research and Development, project nr. 837002508), the NVvP (Dutch Society for Podiatrists) and ProVoet (branch organization for pedicures).
Author Contributions
SB conceived and designed the DIATEMP trial, obtained ethical approval, and registered the trial. MD contributed to trial design. JvN, TB, WadS and SB drafted or edited the trial protocols. JvN, WadS, and SB collected data for the trial. FR wrote the statistical analysis plan for the evaluation presented in this paper, JvN and TB supervised this. FR and JvN performed the statistical analyses. FR, JvN and WadS verified the underlying data. FR wrote the manuscript and all other authors read, commented and edited the manuscript for intellectual content. All authors approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The DIATEMP trial was funded by the Netherlands Organization for Health Research and Development (ZonMw, project nr. 837002508), with 10% matching funded by the Dutch Society for Podiatrists (NVvP) and Dutch Branch Organization for Pedicures (ProVoet). The funders had no influence on study design, data collection, management, analysis, and interpretation, the writing of the report, or the decision to submit for publication, and had no authority over any of these activities.
Supplemental Material
Supplemental material for this article is available online.
Appendix A
Self-care was assessed by asking participants seven questions, based on a commonly used questionnaire by Dutch podiatrists, regarding their foot-related self-care behavior:
Do you inspect your feet for abnormalities daily? Do you inspect the inside of your shoes for abnormalities daily? Do you sometimes walk on bare feet, socks or flip flops? Do you moisture the dry skin of your feet with emollient ointment? Do you, or someone else, cut your toe nails straight? Do you wash your feet daily? In case of any (suspected) foot problems, do you call your health care provider immediately?
Every answer with a “Yes’ was scored as one point (with the exception of question 3, where “no” was scored as 1 point). The accumulated score indicated someone’s self-care for prevention, ranging from 0 (worst) to 7 (best).