
Abstract
Introduction
Amputation is defined as cutting a section or all of an extremity with surgical methods. Amputation is performed with the aim of removing tissue which has lost functionality, ensuring circulation to the remaining extremity, reducing pain of individuals, providing a functional stump in order to use prosthetics and increasing the welfare of individuals. 1 Reasons for amputation differ from country to country, but the number of amputations linked to chronic disease is increasing every year. 2 Amputations of the lower extremities are observed nearly 5 times more compared to amputations of upper extremities, with below-knee amputations comprising the majority of all amputations. 3 Though amputation appears to be a restructuring process that has the potential to improve an individual's functional independence, mobility, and quality of life, 4 it may be a traumatic experience due to negative effects. 5
The effect of amputation on individuals and the adjustment of individuals to amputation is a complicated and dynamic process. Extremity loss may significantly affect the whole life of the individual undergoing amputation. 6 The meaning and roles in life of individuals with lower limb amputation may change, while they may also experience anxiety about the future. 7 An individual losing basic physical functions may have difficulty in protecting mental health and sustaining social relationships due to problems like violent emotional reactions (anxiety, sadness, guilt, etc), disrupted body perception or destruction of self-confidence.7–9 In fact, studies stated that individuals with lower limb amputation have difficulty adjusting to life after amputation.10–11 The causes of difficulty generally comprise unwanted experiences like changed body image, anxiety, self-blame and negative perceptions of the future. 12 Finally, the amputation process may display variations linked to the meaning attributed to amputation by the individual, perception of job, family and amputation, personality traits, previous experiences, social support, mental health status and coping skills, along with the cultural and social attitudes related to disease in the environment in which the individual lives.13–15
In the literature, it was stated that individuals may have many unspoken thoughts about lower extremity amputation and they have difficulty expressing these thoughts. 16 Post-amputation individuals were stated to encounter negative experiences and think that their lives will never be the same again, 17 and they also have negative feelings such as exclusion from life.18–19 However, there are limited studies in the literature that investigate the narrative experiences of individuals who undergo lower limb amputation. In this context, we believe that the narrative experiences of individuals after lower limb amputation will guide the orthopedics and traumatology team for the rehabilitation of these individuals. Studies evaluating the narrative experiences of individuals who undergo lower limb amputation will contribute to the literature and may also benefit readers. Therefore, this study aimed to reveal the narrative experiences of individuals who underwent lower limb amputation.
Questions of Research
What is the experience of individuals undergoing lower limb amputation?
How does undergoing lower limb amputation affect the individual's narrative experiences?
Method
Study Type
This study was a qualitative study conducted using the phenomenological pattern to determine the narrative experiences of individuals with lower limb amputation. This study was conducted according to the guidelines of the COREQ checklist.
Qualitative research is particularly recommended when complex issues need to be explored and studied in depth. 20 Feelings and thoughts are more difficult to determine than other subjects because they are both long-term and not often expressed. Therefore, in this study, the qualitative research method was chosen to reveal the expressions that explain the feelings and thoughts of individuals with lower limb amputation.
Sample of the Study
The study sample comprised 13 individuals with lower limb amputation living in Kayseri province in Turkey from July-August 2021. The individuals were found and contacted using the snowball method. The study sample comprised 13 individuals, consisting of five women and eight men, who had lower limb amputation due to chronic disease (diabetes, peripheral diseases etc) and who agreed to participate in the study.
Inclusion Criteria for the Study
Individuals over the age of 18, who had lower limb amputation due to chronic disease at most 12 months ago and who agreed to participate in the study were included in the study. All individuals participated voluntarily. Individuals who had lower limb amputation revision, sensory loss and diagnosed with mental illness were not included in the study. Individuals who did not want to continue with the study were removed from the sample.
Data Collection Tools
Data collection tools consisted of two parts; a demographic information form and semi-structured interview form.
Collection of Data
Data were collected from July to August 2021. Participants were reached from the community of individuals who had amputations and were followed up at the university hospital in Kayseri, Turkey (with the help from health care providers). The interviews were conducted in quiet environments (rooms at home, garden, etc) where the researcher and participant could easily see and hear each other and communicate comfortably without any noise or distraction. Interviews lasted 40–45 minutes on average. Demographic information was collected at the beginning of the interview. The questions were asked in the same order, and when necessary, questions were used to gain additional information. Interviews were transcribed. Three participants did not consent to the use of an audio recorder so the researcher took interview notes during the interview.
Data Analysis
The demographic data was analyzed using descriptive statistics, expressed in numbers and percentages. Qualitative data audiotapes were transcribed by the researchers. A total of 193 pages of interview text served as the raw data for analysis. Findings were analyzed using content analysis. The study data were categorized by three researchers. Data was coded independently and then themes and subthemes were identified by analyzing the relationships between categories. Expert review of the analysis was obtained from two independent researchers with training and experience in qualitative research to ensure the validity of the theme and subthemes. Subsequent to this review, redundant codes were removed, related themes were regrouped, main ideas behind the statements were identified, and the themes and subthemes were finalized. All quotes are referenced with the number of the participant, gender and age (p3, Female-50; P9, Male-46 etc). The themes are illustrated in Figure 1.
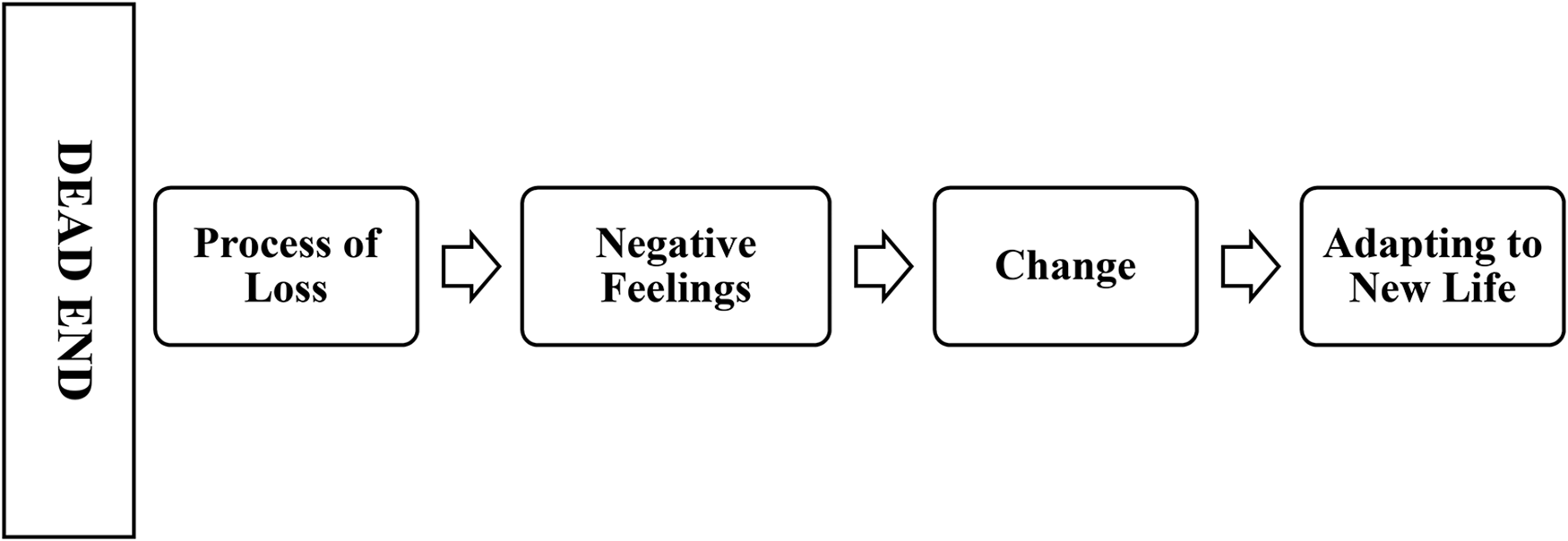
Themes emerging from the interviews.
Credibility and Trustworthiness of Qualitative Data
The methods of long interviews, member checking, and expert review were used to ensure credibility. Prior to the long interview, the participant was provided with the information required to establish secure communication with the researcher, and the interviews were conducted at the scheduled date, time, and place. At the end of the interview, the data obtained by the researcher were summarized for participants, and participants were asked to express their thoughts on their accuracy. In addition, participants were asked if they had any final thoughts that they would like to add. The additional thoughts were recorded, and the interview was terminated. During the planning stage of the study, expert opinion was sought from qualitative research experts about the interview questions and the identified themes. Thus, credibility was achieved by receiving expert opinions from the beginning to the end of the study. For validity, the interview notes and the notes about the participant statements during the interview were taken as raw data, and the statements of participants were directly included in the research report. The results obtained from the interviews conducted on this sample group are believed to be suitable for use and transferable to similar sample groups in different environments, and thus, the transferability criterion is considered to be met.
Reflexivity
The researchers’ experience was as follows; the first researcher (PhD) completed her doctorate education in psychiatric nursing. The second researcher (PhD) completed her doctorate education in surgical nursing. The third researcher (MD) is a medical doctor who completed his specialty training in the field of orthopedics and traumatology. In addition, they have scientific research experience in the field of orthopedics, mental health and qualitative research. The researcher who conducted the interviews was a psychiatric nurse who ensured effective communication with individuals and feasibility of the interviews.
Ethical Aspects of the Study
Permission was obtained from the ethics committee of University (Decree no: 2021.08.279/14.07.2021). The purpose of the research was explained to the participants individually and approval was obtained from the participants. The names of the participants were kept confidential and the statements by the participants included their number, gender and age as code instead of their real names (p3, Female-50; P9, Male-46, etc).
Results
Interview and Sample Characteristics
The mean age of the 13 individuals was 51.17 ± 8.7 years. Five of the individuals were female and eight of them were male. Of the 13 participants, nine were married and had nuclear families; all participants were literate, nine belonged to the middle-income group and five were employed.
Themes Emerging from the Interviews
The study revealed one theme and four subthemes regarding the narrative experiences of individuals with lower limb amputation. This main theme together with sub-themes were Dead End (Loss Process, Negative Feelings, Change, Adaptation to New Life). The themes and subthemes identified in the study are presented in Figure 1.
Theme 1: Dead End
Participants stated they felt they had entered a dead-end street with the decision requiring amputation linked to chronic disease. They stated that all of their experiences were connected to each other, firstly they experienced a process of loss, that very severe negative feelings and thoughts changed over time and that they adjusted to amputation of their legs along with many other changes in their lives. In this process they assessed as a dead end, feelings and thoughts were at the forefront and they emphasized that it affected their whole lives.
Process of Loss
When individuals first learned of the amputation decision they went into shock and stated they thought the doctor's decision to amputate may be wrong or that there may be another treatment method. Additionally, they denied their situation, were examined by several doctors, and cried and were sad when they were faced with the same decision each time. They emphasized that they were angry with themselves for not paying attention to their health in the past, and regretted not putting sufficient effort into their health. When the doctor said my leg needed to be cut off, it was like the world stopped and life ended. I cried for hours. The rest of my life was gone. I wanted to die so badly, I thought I couldn't live with half a leg (P3, Female, 52).
When I first heard this decision I cried a lot, I was very angry at everyone and everything, led by myself, I was only half a woman. I couldn’t get away from negative thoughts. I wished it was a nightmare and I would wake up from the dream. (P2, Female, 50)
Negative Feelings
When individuals first underwent amputation, they emphasized they were angry with the doctor explaining the decision to amputate, they regretted times they did not participate in the treatment process, they were intensely afraid that amputation would be painful, they were anxious as the process after amputation was full of uncertainty and felt intense sadness and guilt when they had difficulty with self-care after amputation. Additionally, individuals stated that pain and physiological problems experienced after amputation negatively affected their mental health. They stated they experienced shame, pain, grief, difficulty expressing themselves, stress and agitation due to these problems. I still hear the voice of the doctor saying that my leg should be amputated… I was so angry… I raised my voice to the doctor saying it must have been a mistake. (P10, Female, 51).
If I’d cared about my health and nutrition, my leg might still be in place. That's why I'm responsible for everything. This is my punishment… I can't forgive myself. Also, I don't know how to deal with it. (crying, P3, Female, 54).
It's like an earthquake… To me, undergoing amputation is like coming out of the wreckage of an earthquake with permanent damage… Leaving my leg in the hospital was a great pain for my heart, I was very anxious about what I would experience afterward (P1, Male, 59).
I felt a deep and severe pain, not only in my leg, in all my cells along with my soul… I know no matter what I do, this pain will never go away. I feel sad every time I look at my leg. I have to learn to love my leg even if only half remains (P7, 49, Female).
Change
Individuals stated there was a severe level of change in their lives after amputation, family, work and social life changed, there were role changes within family and society especially, they were stigmatized by concepts like patient, crippled, disabled, and that people around them looked at them with pity in their eyes. Sometimes they didn’t go out so no one would see the amputation (shopping, trips, visiting friends, etc) and they emphasized that they felt very alone in this situation. I no longer felt like a strong and capable father and that saddened me a lot. I am in need of care from my children. I consider myself a heavy burden rather than a father. (P11, Male, 52).
I can no longer do many of the things I used to be able to do. This is the worst! Even when I go shopping, I have to think about many factors. I can’t go swimming or I can’t actively deal with our garden. Not just the shape of my leg, my whole life changed (P5, Male, 56).
I chose not to leave the house as I didn’t want our family friends or work colleagues to pity me. After the amputation, my happy home turned into a dark prison. I can't stand people around me or people in the community looking at my leg and me with pity (P9, Male, 49).
Adapting to New Life
They stated that they had new lives after the amputation, they made efforts to adjust to the rehabilitation process in this new life, they began to get used to their amputated leg as time passed and the pain they experienced reduced. They emphasized that coping skills, social support, communicating with people like themselves with amputations and beliefs (religion) were very important during the adjustment process. Lessening of my pain was a support, even though it was part of me. Additionally, when I went to check-ups and saw people like me who were happy, it gave me hope. When I saw people with their legs cut off, I thought I wasn't alone. Maybe it was the factor that made it easier for me to adapt to this process. Talking to people like me, listening to their experiences was a good interaction (P10, Female, 51).
It's been 10 months since the amputation, I don’t know if I’m recovering with time but I feel good knowing my family will support me and I beg God to heal me. Praying is the best thing for my soul… Sometimes I do it for hours as a ritual. I am purifying my soul. Praying is a medicine for my pain and my body! (P6, Male 53).
Discussion
This was an empirical study in which the research team collected qualitative data from a particular area. In this study, 13 individuals with lower limb amputation linked to chronic disease had similar feelings and thoughts and it was determined that amputation caused significant changes in their lives.
The mourning process linked to amputation is stated not just to involve one stage, but to be a dynamic process involving complicated psychological outcomes linked to personal and social conditions of individuals undergoing amputation. 21 Studies reported that individuals with amputation experience a mourning process, do not accept their body/themselves, have different feelings like shame and anger, and that family has an important place in the mourning process.22–23 Other research found that they felt grief after amputation; however, there was also relief due to the end of pain and bad odors. 24 Similar to the literature, in this research individuals were shocked when they first learned about the decision to amputate, denied their situation and this was accompanied by negative feelings like sadness, regret and anger during the process of loss. These results, while emphasizing the universality of the process of loss, also showed that the reactions during the loss process can be individual. In other words, while experiencing loss is a universal reality, loss experiences may differ between individuals.
Individuals with amputation are stated to experience contradictory feelings about accepting their bodily loss. 25 Studies reported that individuals experienced intense negative feelings after amputation (anger, shame, worry, sadness, depression) and also experienced role changes and social isolation.26–27 A study researching psychological outcomes of limb amputations reported psychological problems, like despair, depression, irritation, anxiety, loss of self-confidence, stigmatization, isolation and powerlessness and physical disability. 28 Additionally, fear of loss of a visible section of the body was stated to cause a real feeling of fragmentation of the body. 29 Similar to the literature, the participants in this study expressed negative feelings during the amputation process. At the same time, they expressed various severe feelings, especially towards themselves. In this context, it is important to allow the expression of negative emotions and to develop skills to cope with these emotions while providing psychosocial support to individuals with amputation.
Loss of a body part strongly affects the interactions of a person with their surroundings and their feeling of belonging to their surroundings. 30 Amputation changes the lives of the individual and their families; however, it is stated that with time the individual adjusts to changing body functions and appearance. 27 A study of individuals with amputation stated that they were alienated from their limbs after amputation, bodily integrity changed and it negatively affected their sense of self. 31 In this study, individuals stated there were severe levels of change in their lives after amputation (family, working and social life) and there were role changes especially in the family and society. These findings provide insight into how they subjectively experience changes in their lives after amputation. It is considered that evaluating the changes in the lives of individuals with amputation in detail during the rehabilitation process and learning their feelings and thoughts by conducting interviews about this could reduce negative effects about amputation.
Rehabilitation and adjustment to society of individuals with extremity amputations is a long and difficult process. 32 Treatment and rehabilitation services for individuals with amputation should be run with a multidisciplinary understanding and it is reportedly important to offer psychosocial support to these individuals.33–34 The adjustment process for individuals with extremity amputation is stated to require psychosocial support to ensure acceptance and perception of body representation, and adjustment to the real body. 30 Amputation is stated to leave a person physically and psychologically vulnerable, especially after discharge from hospital, and for this reason it is necessary to offer emotional support and healthy lifestyle information to encourage independent living and limit the effect of psychological problems. 35 Additionally, family should be included in this process for individuals with lower limb amputations and family support plays a critical role. This situation increases adaptation by reducing anxiety 32 and assists in expressing negative feelings. 36 In this study, individuals emphasized they had a new life after amputation, they attempted to adjust to this new life with rehabilitation processes and social support (partner, family, close friends), communication with people like themselves with amputations and beliefs (religious practices) were very important in this process. Religious rituals like meditation, yoga, prayer and fasting in some religions are stated to have protective and ameliorating effects on mental health.37–39 A study reported that medication improved the mental health of individuals with amputation linked to chronic disease. 40 Additionally, it was stated that social interaction is associated with better physical health. 41 It is an important finding of this study that the participants stated that meeting individuals like themselves was a good interaction for them. In addition, it is thought that the use of religious practices such as praying or social supports can guide the planning of health care provided to individuals with amputation.
Limitations of the Study
Considering the features of the sample group, this study has limited capacity to mention possible differences that may occur due to characteristics related to amputations (age, sex, socio-economic and ethnic origin, amputation type or duration since amputation). Additionally, the relatively short duration since amputation (maximum 12 months) narrows the scope of the research and is thought to limit opportunities to discover later themes.
Conclusion
Individuals with lower limb amputations stated there were positive factors affecting the rehabilitation process while emphasizing negative thoughts and feelings during the amputation process. Individuals with amputation considered it was important to include coping skills, social support, communication with other amputees and beliefs in the adjustment process. The findings of this study support the available literature and also provide an idea about how the feelings, thoughts and lives of individuals are affected after limb loss. Additionally, they show that the adjustment process needs to be considered from many aspects. These results can be used in planning for training, counseling and therapeutic interviews to protect the psychosocial health of individuals with lower limb amputation. Finally, it is recommended to conduct more experimental and qualitative studies regarding the effects of lower limb amputation. In addition, long-term follow-up studies will contribute greatly to this field.
Footnotes
Author Contributions
The authors report no conflicts of interest. Author contributions Küçük Öztürk G. designed the study. Küçük Öztürk G. And Yüceler Kaçmaz H. analyzed the results. Küçük Öztürk G., Yüceler Kaçmaz H., and Öztürk Rİ. reviewed related literature, drafted the article, and have read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Financial Disclosure
No financial support has been received.
*This study was announced as a verbal announcement at the I. International Congress of Health Sciences and Multidisciplinary Approaches 2021 in Turkey.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Supplemental material
Supplemental material for this article is available online.