
Abstract
The management and healing of lower extremity ulcers have always been a complex health problem because the clinical course is typically chronic, the results are often poor, and the socioeconomic impact is considerable. The healing process of foot ulcers of people with diabetes is further hindered by the concomitant presence of obstructive arterial disease, neuropathy, and foot malformation. It is frequently associated with multiresistant infections and often results in micro/macro amputations. Photodynamic therapy employs a photosensitizer activated by light of a specific wavelength able to generate reactive oxygen species, which initiate further oxidative responses locally with components of the bacteria. The experience of the treatment center for the lower extremity ulcers in 17 persons with diabetes in Acerra (Italy) with photoactivated RLP068, reported here, corroborates the results of the clinical trials and of the previous case reports. In all cases, examined photodynamic therapy with photosensitizer RLP068 and red light at 630 nm was found to reduce lesion area and inflammation and to ensure the decrease of bacterial load, hence reducing treatment times and antibiotics use, improving patient outcomes, and reducing the incidence of amputations. The simultaneous combination of photodynamic therapy with other ancillary physical-based treatments such as therapeutic magnetic resonance or Bio-Electro-Magnetic-Energy-Regulation was observed to be safe, time-saving, and able to lead to faster healing.
Introduction
The management and healing of lower extremity ulcers have always been a complex health problem because the clinical course is typically chronic,1,2 the results are often poor, and the socioeconomic impact is considerable.3,4 The healing process of foot ulcers of people with diabetes is compromised by the concomitant presence of obstructive arterial disease, neuropathy, and foot malformation5-7 and is complicated because it is associated with multiresistant infections and often results in micro/macro amputations.4,8,9 Early detection, strict glycemic control, and appropriate arterial inflow to remove from the wound and its margins combined with proper management aimed at eliminating any infection are beneficial in diabetic foot ulcers (DFU) prevention. However, it is not often sufficient to eradicate bacteria and fungi that not only hamper and delay healing but can lead to amputations or death of the patient. Treatment of DFUs is challenging and can be associated with high social burden, and alternative and/or complementary approaches are necessary to promote, support, and accelerate the healing process through the reduction or resolution of the infection and inflammation, and the induction of re-epithelialization.
Novel therapeutic interventions have been developed based on the principles of photomedicine (absorption of photons by specific chromophores) to overcome the issue of poor drug circulation in infected areas. 10 Photodynamic therapy (PDT) employs a photosensitizer activated by light of a specific wavelength. When activated, the photosensitizer takes part in generating reactive oxygen species (ROS), which initiate further oxidative responses locally with components of the bacteria, ideally without affecting the adjacent host cells. 10
RLP068 is a tetracationic Zn(II)phthalocyanine derivative activated by exposure to red light at 630-nm wavelength. The photoactivation of RLP068 results in the production of singlet oxygen and other ROS, able to affect a range of cellular targets, including cell membrane and/or wall, cytoplasm, and cellular components, resulting in a rapid, broad range, bactericidal, and fungicidal effect. 8
Clinical trials and case reports previously showed that photoactivated RPL068 is capable of inducing a dose-dependent reduction in total and pathogen microbial load in infected DFU, with a negligible systemic absorption through the wound and a dose-dependent reduction in total and pathogen microbial load.8,11-13 The experience of the treatment center for the lower extremity ulcers in 17 persons with diabetes in Acerra, Italy, is reported here.
Materials and Methods
Design and Population
The clinical experience of the lower extremity ulcers treatment Center in Acerra (Italy) is presented here. Given the retrospective nature of data collection, board approval was not required, since individual patient consent was obtained for all the procedures.
Eighteen patients presenting chronic DFU who were treated with photoactivated RLP068 for 4 weeks with 2 sessions per week between October 2019 and October 2020 were retrospectively selected and examined. Patient with ulcers of different origin (eg, venous, arterial, traumatic) were not included in this sample. Before being admitted to the lower extremity ulcers treatment center, all patients were treated with appropriate dressings and aspecific antibiotic home therapy prescribed by the general practitioner. Patients characteristics are reported in Table 1.
Patients Characteristics.
One patient lost at follow-up.
TPO2 < 30 mm Hg.
Enterococcus faecalis (1), Staphylococcus aureus (6), Staphylococcus epidermidis (8), Escherichia coli (5), Proteus mirabilis (1).
Wound Evaluation and Treatment
During the 4 weeks of treatment, lesions were clinically assessed every week for the determination of exudate, periwound skin, depth of the lesion, background color, and granulation tissue to evaluate the degree of re-epithelialization. The pain was evaluated using the visual analog scale (VAS) from 1 to 10 units. Size, pain, Tissue-Infection/Inflammation-Moisture-Edge (TIME), 14 inflammation, exudation, and re-epithelialization were assessed by patient and physician evaluation every week (Table 2).
Modifications After 8 Sessions of Photodynamic Therapy.
Abbreviation: VAS, visual analog scale.
Tissue-Infection/Inflammation-Moisture-Edge. 14
When possible, biopsy swab after edge and lesion infiltration was performed and surgical debridement was executed if deemed necessary. DFUs were treated with RLP068 twice a week in a sterile environment for 2 min and covered with a transparent dressing according to the manufacturer's instructions. Thirty minutes after the application of the photosensitizer, the lesion was irradiated for 8 min by a portable LED light device with a red light at 630 nm wavelength, providing a total energy of 60 J/cm2. All patients were treated for a total of 8 sessions.
The ulcer was then washed with saline to remove residual photosensitizers and covered with a hydro-fiber or silver hydro-fiber dressing, followed by a conventional dressing.
Results
Of the 18 patients, 7 women and 11 men, one was lost during the follow-up. All patients had type II diabetes, associated with either obstructive arterial disease (14 patients) or diabetic neuropathy (11 patients), and chronic lesion (all participants, for at least 5 months). Before the PDT, 17 of 18 lesions tested microbiologically positive at swab/biopsy (Enterococcus faecalis, Staphylococcus aureus, Staphylococcus epidermidis, Escherichia coli, Proteus mirabilis) (Table 1). Specific antibiotic therapy was prescribed against the bacteria identified at the swab/biopsy.
After the 4-week treatment, all lesions presented the disappearance of the inflammatory signs and reduction or elimination of the exudate. A significant re-epithelialization (between 50% and 80%) was highlighted in 10 out of 18 patients. Infected and large lesions were made suitable for skin grafting (Table 2). As described below, patients were treated with PDT alone or in association with another technique, based on their clinical evaluation.
Patients Treated With RLP068
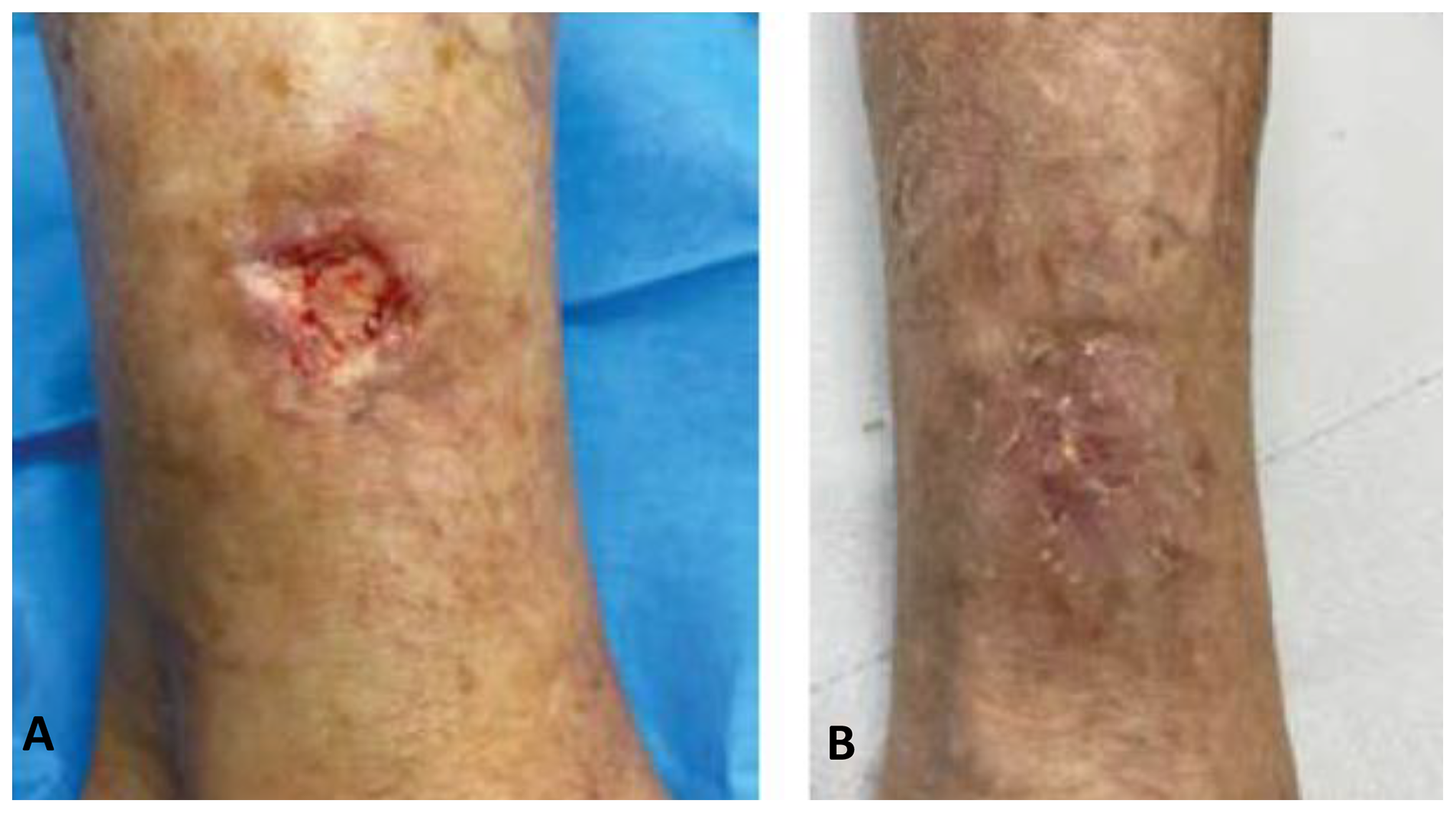
Thirteen of the patients described above were locally treated with RLP068. One example is the lesion depicted in Figure 1, before and after the 4-week treatment. A 72-year-old man presented mild obesity (body mass index, BMI 35.6), hypertension, hypercholesterolemia, and type II diabetes and showed osteomyelitis at X-ray examination. He showed a recurrent open lesion for more than 5 months positive for S aureus and at the angiography evidence was found only for collateral circulation in the leg (tissue oxygen tension, TPO2, 31 mm Hg). The ulcer underwent surgical debridement and subsequently 8 sessions of PDT with discharge of the lesion, which then permitted to start the angiogenic therapy. At the first visit, the lesion appeared infected and the patient reported pain (VAS = 6/7). After 2 PDT sessions, a marked reduction of pain (VAS = 2) and signs of local inflammation were observed.

Lesion of case 1 before (A) and after (B) 4-week photodynamic therapy (PDT).
Patients Treated With RLP068 and Autologous Skin Grafting
In 2 cases, the lesion was cured with PDT and subsequent autologous skin grafting. One example is the case of a 61-year-old man presenting mild obesity (BMI 34.9), hypertension, hypercholesterolemia, and type II diabetes and showing osteomyelitis at X-ray examination. At the angiography, multiple intermediate stenoses of the popliteal–tibial axis (TPO2 46 mm Hg) were found. The man showed an open lesion for more than 3 months that tested positive for S epidermidis and P mirabilis. The ulcer underwent surgical debridement, 8 sessions of PDT, and, subsequently, autologous skin grafting with a negative buffer for bacterial growth. Severe pain (VAS = 8) was reported at the first visit, started decreasing at the second PDT session, and was reported to be lower than 3 during the last 2 weeks of treatment. The lesion before and immediately after treatment is depicted in Figure 2. Complete healing was reached after skin grafting.

Lesion of case 2 before (A) and immediately after (B) photodynamic therapy (PDT).
Patients Treated With RLP068 and Magnetic Stimulation
In 3 of the 18 cases described above, the ulcer underwent PDT with photoactivated RLP068 and simultaneous magnetic stimulation, which include therapeutic magnetic resonance (TMR) or Bio-Electro-Magnetic-Energy-Regulation (BEMER).
A lesion before and after the 4-week treatment with PDT and TMR is depicted in Figure 3. In this case, the patient was a 73-year-old woman with hypertension, hypercholesterolemia, and type II diabetes. She presented a leg ulcer for more than 6 months that tested positive for S epidermidis and P mirabilis.
Lesion of case 3 before (A) and after (B) photodynamic therapy (PDT) and therapeutic magnetic resonance (TMR).
An occlusion of the superficial femoral artery (TPO2 61 mm Hg) was found, with good popliteal rehabilitation and a good walking perimeter. The lesion underwent surgical debridement and, subsequently, 8 sessions of PDT with concurrent TMR on the same lesion. The combination of the 2 techniques permitted to significantly decrease the pain (from VAS 6 to 0) and local signs of inflammation (about 80%) in 4 weeks.
Discussion
In the 17 cases examined here, PDT with photosensitizer RLP068 and red light at 630 nm was found to reduce lesion area and inflammation and to ensure the decrease of bacterial load. The therapy modulates the infectious process and reduces/eliminates exudate. It also lessens pain hence improving the patient's quality of life. Furthermore, no adverse events were highlighted. These results are in good agreement with the randomized, double-blind, parallel series, placebo-controlled phase IIa trial, where a reduction in total microbial load was observed, no safety issues emerged from the analysis of adverse events and systemic absorption of the photosensitized was negligible. 11
The use of PDT proved to be valuable for the antimicrobial treatment of complex patients, for example, with multiple diseases under multiple therapies, with ulcers chronically infected by drug-resistant bacteria, or in addition to other therapies in serious cases, here as in other case series.8,10,12,13
When chronic lesions are autonomously treated by the patient, living with the ulcer can become a habit that is broken only when a health care professional visit is imposed by an infection. Time and resources can be saved by using PDT, able to achieve wound healing with a limited number of ambulatory sessions (8 sessions over 4 weeks), limited professional and logistics resources for the health care system.
Finally, in diabetic ulcers, an additional value of PDT is represented by the possibility of simultaneously combining the procedure with ancillary physical-based treatments such as magnetic stimulation, such as TMR and BEMER. Both techniques use weak magnetic fields to enhance microcirculation and enable tissue oxygen perfusion. More in detail, TMR enhances skin wound healing improving the quality of the extracellular matrix, leading to a rejuvenation effect,15,16 while BEMER significantly increases vasomotion of microvessels, arteriovenous pO2 difference, number of open capillaries, arteriolar and venular flow volume, and flow rate of red blood cells. 17 TMR or BEMER were coupled to PDT in 3 of the described patients and, more specifically, in those with severe edema and/or lymphedema. Simultaneous application of PDT with therapies that last less than 30 min as TMR or BEMER can be time-saving and able to lead to faster healing. In addition, the complementarity with angiogenic therapy with stem cells taken from peripheral blood, bone marrow, or fat should be evaluated.
The main limitation of this work is represented by the inclusion of relatively small sample size and by the heterogeneity of treatment timings and associated therapies.
Conclusion
In conclusion, our experience further demonstrates that PDT using RLP068 photoactivated with a red light at 630 nm wavelength is a technological innovation capable to reduce treatment times and antibiotics use, improve patient outcomes, and, above all, avoid the extension of an injury and reduce the incidence of amputations. The technique has been satisfactorily associated with different devices as TMR and BEMER. Considering these results, evident PDT capability of decreasing DFU treatment costs should be investigated.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The publication was supported by an unrestricted grant from Molteni Farmaceutici, Italy.