
Abstract
We aimed to develop and test the reliability and validity of a foot care self-management assessment tool for older Japanese patients with diabetes. In this cross-sectional observational study, which was carried out according to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines, additional items were developed and selected to reflect older Japanese patients’ needs a thorough investigation with experts in diabetes and geriatrics. A total of 200 older patients with diabetes in a foot care outpatient clinic were included in the study to finalize the scale items and verify the scale's reliability and validity. A factor analysis yielded a 4-factor, 9-item scale. Factors 1 to 4 were “skin condition” (3 items), “nail clipping” (2 items), “attention to wounds” (2 items), and “relationships with others” (2 items). The Cronbach's α coefficients for the 4 factors were .852, .900, .820, and .571, respectively. The overall scale was 0.797, indicating good internal consistency. Spearman's correlation coefficients for each of the 4 factors with the scale's total score showed good stability; all correlations were significant. In Japan's super-aged society, it is important to focus on foot care practices among older adults and to promote good foot care practices among early older adults so that they can practice self-care at home. Therefore, a scale for comprehensively evaluating foot care in elderly patients with diabetes is needed. The Foot Care Scale for Older Diabetics could be useful as a tool for assessing the ability to self-manage foot care in older Japanese patients with diabetes.
Introduction
Diabetic foot disease is a complication of diabetes mellitus. It is defined as infection, ulceration, or destruction of tissues of the foot of a person with currently or previously diagnosed diabetes mellitus, usually accompanied by neuropathy and/or peripheral arterial disease in the lower extremity. 1 According to a previous study, diabetic foot disease affects the instrumental activities of daily living (IADLs) and activities of daily living (ADLs) of patients. Foot amputation for a diabetic foot lesion has been associated with a reduced quality of life 2 and has become a common problem in a super-aged society. 3 The most important factors for the occurrence of foot ulcers are peripheral neuropathy, minor trauma, and foot deformities, but most ulcers can be prevented through foot care self-management. 1 In addition, foot ulcer occurrence in patients with diabetes mellitus is associated with mortality. 4
Health education programs on foot care have improved foot lesions and ulcers among patients. 4 However, a study by Ahmad Sharoni et al 5 found that patients with diabetes did not perform foot self-care thoroughly; particularly, men failed to regularly check their feet, walked barefoot, had poor hygiene, and trimmed their toenails inappropriately. Moreover, with age, there is a decline in the ability to perform ADLs and IADLs, a decline in the ability to see and hear, and a decline in the sense of touch; thus, foot self-care is difficult to perform.
Several studies have reported tools for the assessment of foot care self-management in older patients with diabetes, including the Nottingham Assessment of Functional Foot Care Questionnaire created more than 10 years ago by Rossaneis et al 6 and the Diabetes Foot Self-Care Behavior Scale by Lincoln et al 7 and Chin and Huang. 8 The scales reported in Japan include the Dietary Management of Diabetes Self-Efficacy Scale (DMDSE) by Daitoku et al 9 and the Japanese version of the Foot Care Confidence Scale (JFCCS) by Yasukata. 10 The JFCCS was originally developed overseas, and a Japanese version was created and tested for reliability and validity in a sample of Japanese participants. The JFCCS is suitable for patients with diabetes but not suitable for comprehensively assessing elderly people. Thus, in a super-aged society such as Japan, a tool for comprehensively evaluating foot care in elderly people, especially those with diabetes, is necessary.
The abovementioned foot care scales are not for a comprehensive foot care evaluation in older adults, especially those who are at risk of developing chronic disease due to aging. Thus, we aimed to create an appropriate scale for older Japanese patients with diabetes. Furthermore, the reliability and validity of such a scale, the Foot Care Scale for Older Diabetics (FCS-OD), were tested.
Since self-care in older adults requires skills and abilities learned by modeling behaviors, they can be measured independently. Thus, in this study, “the ability of older patients with diabetes to self-manage their foot care” was measured. To identify the skills needed for foot care self-management, we searched for nursing articles and original papers (dissertations) in the Igaku Chuo Zasshi (ICHUSHI), Japan's bibliographic database of biomedical journals, using the keyword “foot care” to find relevant documents from the past 10 years (January 2006 to December 2017).
Materials and Methods
During the article search, we searched for articles in which “self-management” was mentioned. Additionally, we held meetings with experts to identify items needed for the scale. The experts included geriatric nurses, certified diabetes educators, diabetologists, pharmacists, nutritionists, physical therapists, and experts in scale development. Similar ideas were grouped together, and the “codes” for behaviors to be turned into question items were carefully selected. Together, we checked the items of the JFCCS sequentially and omitted any items similar to those in the short version. Finally, we used 11 out of the 12 items of the JFCCS. 10
A Likert-type scale was considered the best way to ask respondents about the extent of their self-management skills by having them rate to what extent a statement about a self-management skill applied to them. These ratings were scored according to the strength and direction (eg, strongly/somewhat, agree/disagree, and neutral) of the rating; a total score was calculated. A 5-point scale was used with scores from 1 to 5, where 1 = very untrue of me, 2 = somewhat untrue of me, 3 = neutral, 4 = somewhat true of me, and 5 = very true of me.
The research team held meetings to ensure the validity of question items by examining (1) whether each item actually reflected the foot care self-management skill of older patients with diabetes; (2) whether the items covered all the foot care self-management skills that an older patient with diabetes should have; (3) whether the scale was valid for clinical use; (4) whether the item was expressed in easy language for a patient to answer; and (5) whether there were any question items that would be difficult for a patient to answer. In 1 of the research team meetings, it was decided that 1 of the JFCCS items, “I can protect my feet,” should be eliminated because there were other items on protecting the feet; therefore, we used 11 of the 12 JFCCS items.
Since our scale was a patient-reported outcome measure (PROM), we followed the recommendations of the International Consensus-based Standards for the Selection of Health Measurement Instruments Risk of Bias Checklist; specifically, the PROM development (Box 1) recommendations for PROM design (Box 1a). 11
Data were collected from April 2019 to October 2020 using a draft version of the self-administered questionnaire. Patients consenting to participate in the study were provided with the questionnaire to complete it on-site. The questionnaires were collected directly from the participants when they finished filling them. It took ∼10 min to complete the questionnaire. Other data were also collected from each participant's medical record: age, sex, hemoglobin A1c (HbA1c) levels, and diabetes history.
As our study's objective was to develop a scale, the sample size was determined by the number of responses needed to perform a valid factor analysis. According to COSMIN, 12 when performing factor analysis, the number of question items should be at least 3 to 4 times the number of factors to be extracted, and the sample size should be ∼5 to 10 times the number of question items. Therefore, the target sample size for our study was 200.
Patients who were at least 65 years old, had regular clinic visits for outpatient foot care for at least 1 year, and had the approval to participate by their physician, were considered eligible for this study.
However, patients were not able to participate if they met any of the following criteria:
The patient was deemed ineligible for the study by the principal or responsible researcher. The patient had a serious life-threatening illness. The patient suffered from a severe decline in cognitive function. The patient had severe sensory disorders. The patient could not understand the questionnaire.
All statistical analyses were performed using SPSS version 25.0 (Advanced.AI Corp., Japan). Correlations between variables were calculated using Spearman's correlation coefficient. For construct validity, a principal component analysis was performed. Cronbach's α coefficient was utilized to examine the scale's reliability. Additionally, to investigate the intrarater and interrater reliability, the kappa coefficient was calculated for 20 participants. A P value of <.05 was considered statistically significant.
To verify the internal consistency of the FCS-OD, correlations were calculated between each of the factors and the Cronbach's α coefficient for each factor and for the overall scale.
This study was designed to comply with the Declaration of Helsinki and the Ethical Guidelines for Medical Research Using Human Subjects (Ministry of Education, Culture, Sports, Science and Technology & Ministry of Health, Labour and Welfare, Notification No. 3, 2014) and to protect patient privacy. The study was approved by the ethics and conflicts of interest committee of the National Center for Geriatrics and Gerontology (approval no. 1243, May 27, 2019). Written informed consent was obtained voluntarily from each participant after providing them with a written explanation approved by the ethics committee and a thorough oral explanation. This study was carried out according to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines.
Results
The number of participants in this study was 200. The mean age of the participants was 78.3 ± 6.5 years, and the mean HbA1c level was 7.5% ± 1.1%. The descriptive statistics for the resulting scores by items are presented in Table 1. The mean scores ranged from 2.03 to 4.06. The lowest score was for item no. 4 “I know how to massage my feet,” and the highest was for item no. 19 “I have interactions with my family daily.” We checked whether any item was subjected to a floor effect or ceiling effect in case it needed to be excluded from the overall correlational analysis. However, we decided to keep item no. 19 because interaction with family is important to older adults.
Descriptive Statistics for the 30-Item Foot Care Scale (N = 200).
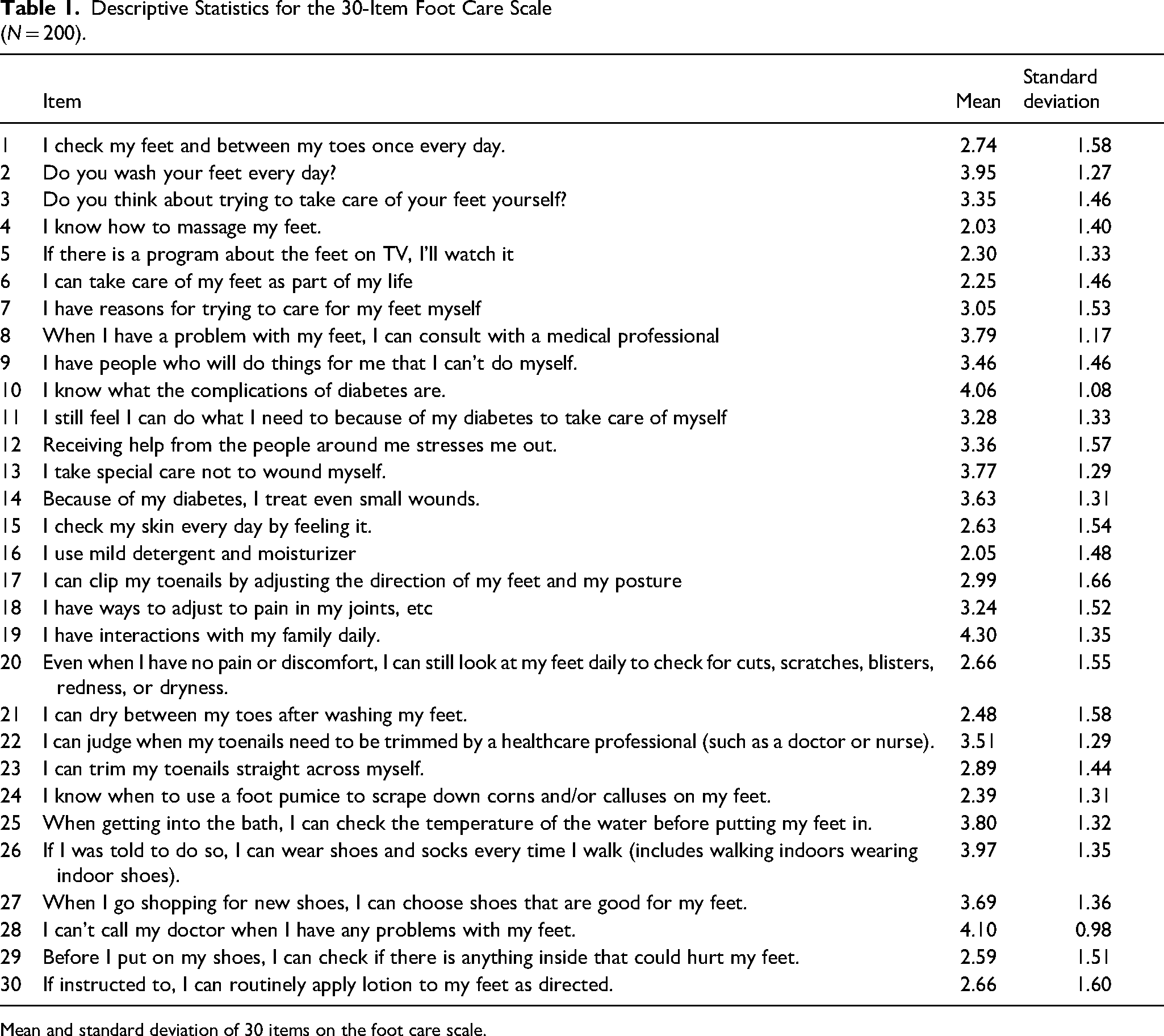
Mean and standard deviation of 30 items on the foot care scale.
To verify construct validity, a principal component analysis was performed with promax rotation. Based on the results of eigenvalues and scree plots, the number of factors was increased from 3 to 4, and by excluding items spanning multiple factors with a factor loading of <0.8, the analysis yielded a 4-factor 9-item model. The final factor pattern and factor correlations after promax rotation are presented in Table 2.
Foot Care Scale for Older Diabetics (Short Version for Screening).
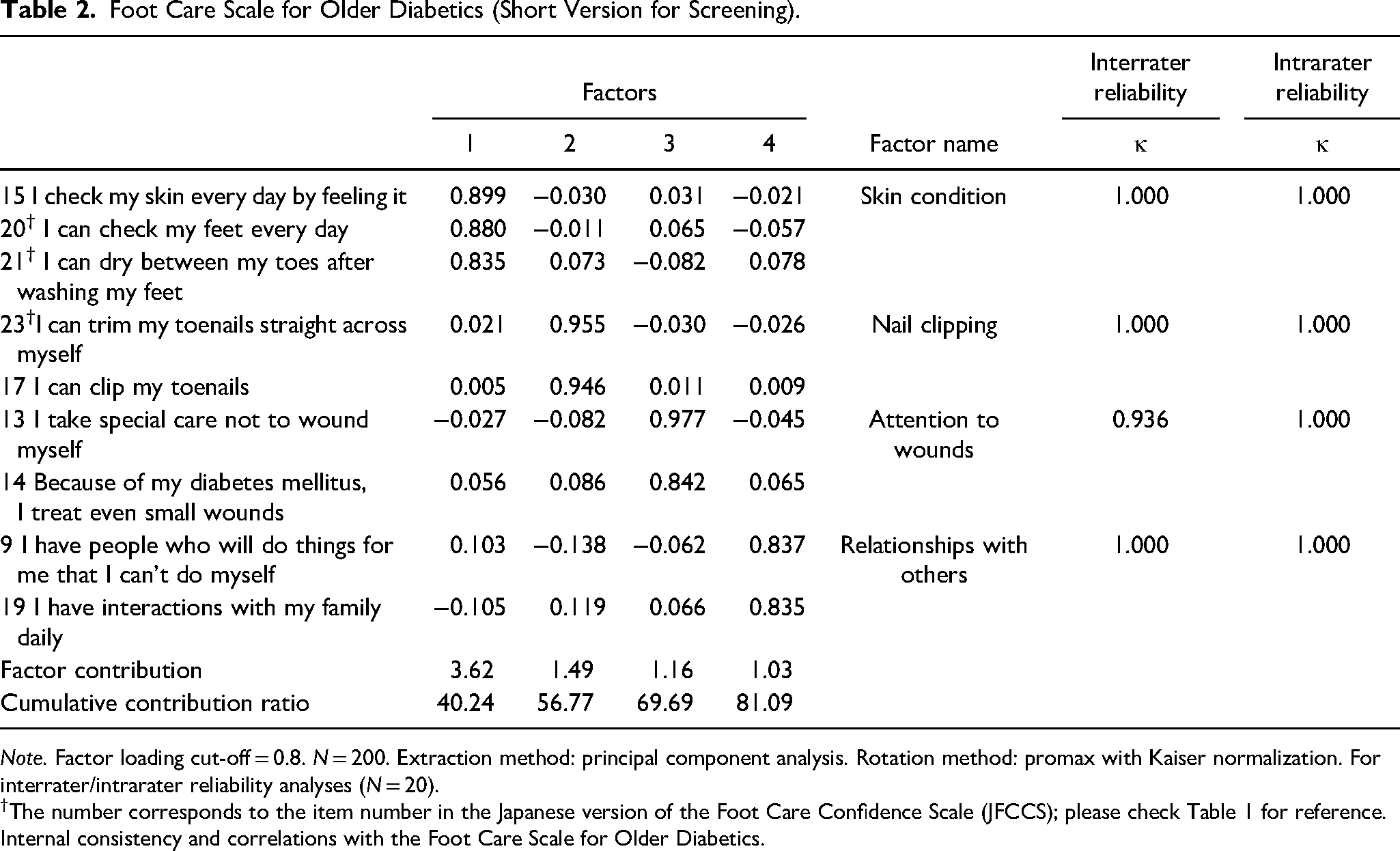
Note. Factor loading cut-off = 0.8. N = 200. Extraction method: principal component analysis. Rotation method: promax with Kaiser normalization. For interrater/intrarater reliability analyses (N = 20).
The number corresponds to the item number in the Japanese version of the Foot Care Confidence Scale (JFCCS); please check Table 1 for reference. Internal consistency and correlations with the Foot Care Scale for Older Diabetics.
We named factor 1 “skin condition” as it was composed of 3 items related to skincare of the feet: “I check my skin every day by feeling it,” “I can check my feet every day,” and “I can dry between my toes after washing my feet.” We named factor 2 “nail clipping” because it was composed of 2 items related to toenail clipping: “I can trim my toenails straight across myself” and “I can clip my toenails (by adjusting the direction of my feet and my posture).”
We named factor 3 “attention to wounds” because it was composed of 2 items related to being careful about wound prevention: “I take special care not to wound myself” and “because of my diabetes, I treat even small wounds.” Factor 4 was composed of 2 items: “I have interactions with my family daily” and “I have people who will do things for me that I cannot do myself.” Therefore, we named this factor “relationships with others.” The correlations between the total scale scores for the FCS-OD and JFCCS-11 items were calculated. The JFCCS questionnaire was also provided to all patients, and the results were compared with those of the FCS-OD scale. Although there are 3 items from the JFCCS in the FCS-OD, there was a strong significant correlation of 0.824 (P < .001).
Similarly, we developed a long version of the scale, the FCS-ODL, with 6 factors and 22 items (Table 3). The short version can be used as a simple evaluation and the long version as a detailed assessment. We named Factor 1 “skin condition” because it comprised 9 items similar in content to those for factor 1 of the FCS-OD. Similarly, factors 2 and 3 were assigned the same names as those in the FCS-OD. Factor 4 consisted of 2 items: “If told to, I can wear socks every time I walk” and “I can check the bathwater temperature before putting my feet in,” and we named it “attention to feet.” Factor 5 was named the same as factor 4 in the FCS-OD, ie, “relationships with others.” We named factor 6 “self-efficacy” because it consisted of 2 items: “Receiving help from the people around me stresses me out” and “I still feel I can (do what I need to because of my diabetes to) take care of myself.” When the correlations were calculated between the total scores for the FCS-ODL items and JFCCS-11 items, although 8 of the JFCCS items were part of the FCS-ODL, the correlation coefficient was significant and even higher at 0.898 (P < .001).
Foot Care Scale for Older Diabetics (Long Version for Assessment).
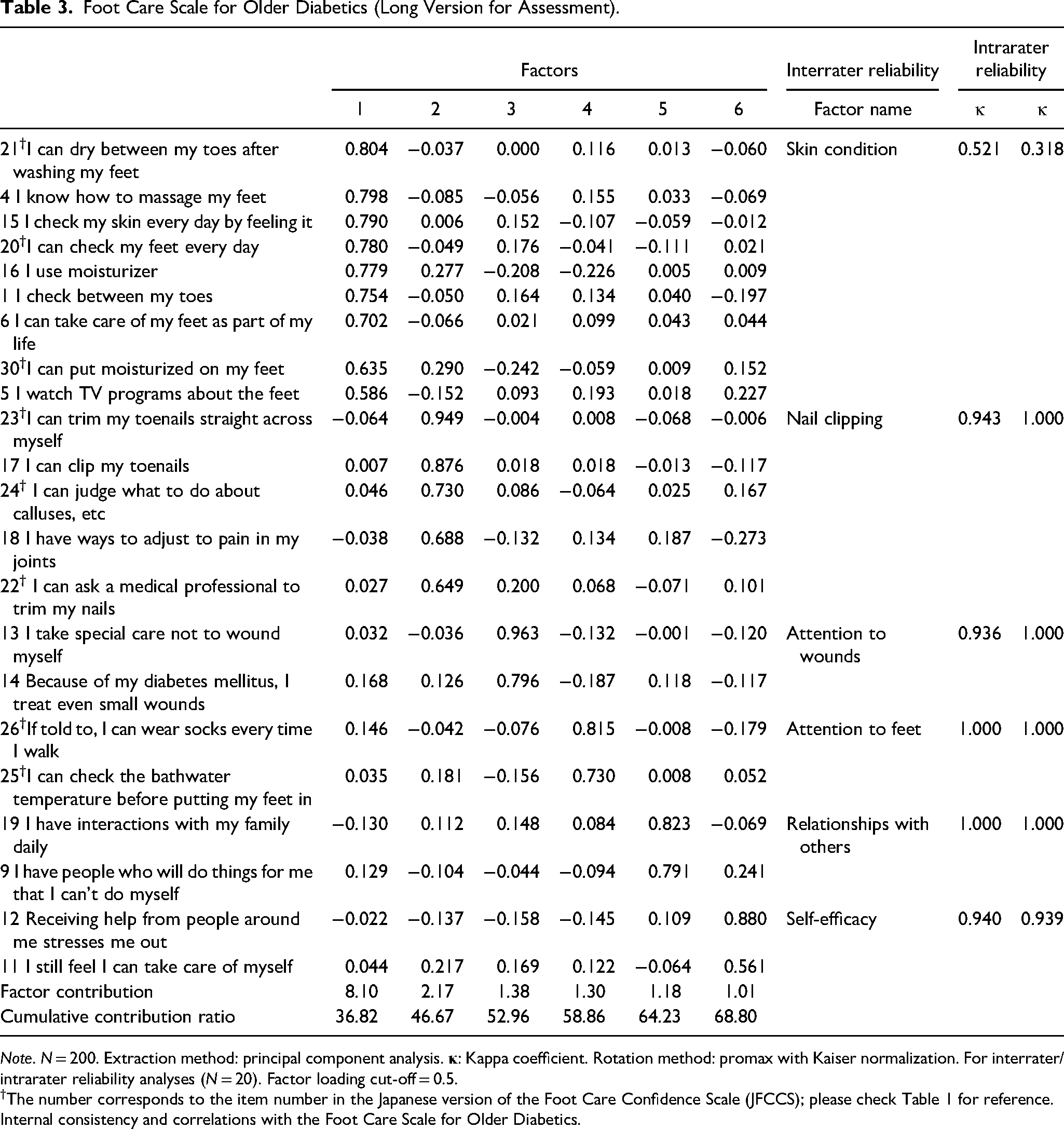
Note. N = 200. Extraction method: principal component analysis.
The number corresponds to the item number in the Japanese version of the Foot Care Confidence Scale (JFCCS); please check Table 1 for reference. Internal consistency and correlations with the Foot Care Scale for Older Diabetics.
Overall, the scale showed good internal consistency. Spearman's correlation coefficients for the 4 items of the JFCCS scale were 0.843, 0.833, 0.640, and 0.571, respectively, which showed high stability, and that for the total score of the scale was 0.824, also showing high stability. Similarly, to verify the internal consistency of the FCS-ODL, correlations were calculated between each factor and the Cronbach's α coefficients. Overall, the FCS-ODL showed a high consistency of .797. For the JFCCS, the correlation was .898, indicating good stability. The significance level for all the correlations was P < .01 (2-tailed).
For the short version, high values of the kappa coefficients showed good intra- and interrater reliabilities (Table 4). For the long version, both intra- and interrater reliabilities for factor 1, which consisted of many more items, were lower than those for the short version. However, for factors 2 and 6, the kappa coefficients were similarly high.
Reliability of the Foot Care Scale for Older Diabetics.
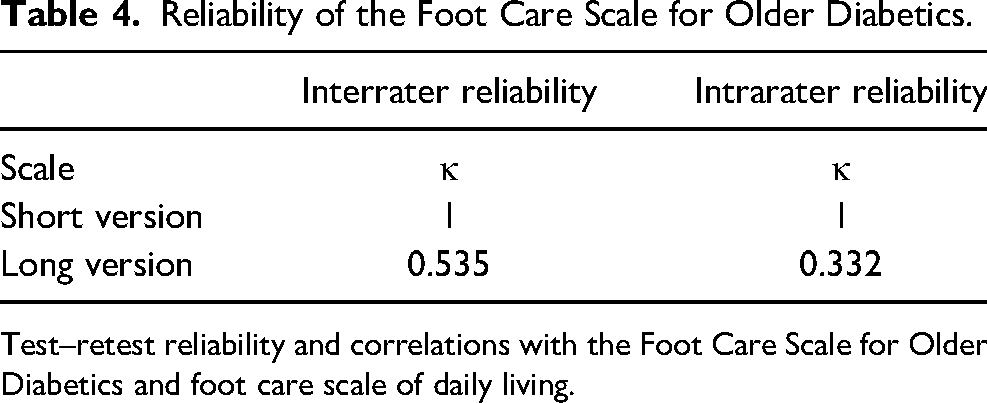
Test–retest reliability and correlations with the Foot Care Scale for Older Diabetics and foot care scale of daily living.
Discussion
The validity and reliability of the evaluation scale were assessed by examining the items of the JFCCS scale used in the United States and other items together. The validity and reliability of the content of the scale were decided by consensus with experts in diabetes and geriatrics as well as elderly patients with diabetes before the scale was translated to Japanese. Significant correlations were found between the validated JFCCS items and the FCS-OD total score (3 out of 9 items were from the JFCCS) (P < .001). The new scale had 9 items, which is less than the 12 items of the JFCCS. Thus, the evaluation could be completed in a shorter time without compromising the quality of the results.
Until now, self-care behavior measures for patients with diabetes have focused mainly on measuring treatment-related effects of changes in diet and exercise.8,13–15 Thus, self-care assessments take time, and we were unable to find a scale for specifically assessing self-care related to the standard prescribed practice of foot care in older patients with diabetes. Additionally, in Japan's super-aged society, it is important to focus on foot care practices among older adults and cultivate good foot care practices in early older adulthood so that they can take care of themselves at home. In our study, we investigated the validity and reliability of 2 versions of an assessment scale that combined items from the JFCCS, which originated from the United States, with additional items specific to the elderly population; these were determined through discussions with Japanese healthcare experts in diabetes and gerontology and with older patients with diabetes to ensure that the scale would be easy for them to use.
Strong correlations between the total scores for the FCS-OD and JFCCS confirmed the scale's validity (P < .001). Given that the 9-item FCS-OD contains 3 items from the 12-item JFCCS and incorporates items specific to older adults, it could be used for a better evaluation of the elderly population, could be conducted in a shorter time, and could be less of a burden for patients to complete. Treating elderly patients with diabetes, especially the late-stage elderly, is often challenging because they have decreased ADLs, cognitive decline, depression and mental problems, and lack of family support. Therefore, the treatment of elderly patients with diabetes requires a different approach from that of young patients. It has been reported that the comprehensive-geriatric–geriatric (evaluates ADLs, cognitive function, psychological state, family support, quality of life, etc) and the need for assessment (comprehensive geriatric assessment, CGA) are useful tools for these patients. In addition, these assessment tools can also be used when evaluating diabetes treatment. 16 The FCS-OD covers items necessary for CGA such as functional status, social assessment, quality of life, etc, in addition to diabetes-related items. It can be evaluated in a shorter time than CGA.
Regarding the scale's construct validity, previous studies have noted the importance of the following factors: “skin condition” and “nail clipping.” They were included in the JFCCS. “Attention to wounds” was included in the Instrument of Diabetes Self-Care Agency, 17 and the need for “self-efficacy” of patients with diabetes in the DMDSE. 9 Regarding “relationships” with others needed by older patients with diabetes, studies have shown that the ability to perform self-care increased with the support of friends and family.18,19 Thus, the findings that these factors were components of self-care for older patients with diabetes in our study were similar to those of previous studies.
Regarding the reliability of the FCS-OD, Cronbach's α coefficients for the scale's 4 factors and for the overall scale demonstrated good overall internal consistency. This version of the scale has only 9 items; therefore, it can easily be used by health care staff for interviewing patients in a short period of time. Meanwhile, the standard 36-item short-form survey has been used to measure comprehensive health. From this, a scale that can measure 2 summary scores of “physical health” and “mental health” and which consists of 12 items was developed, known as the SF-12. Decreasing the number of items on a scale could help lower the burden on patients. In the long version of the scale we developed, 9 items are used to evaluate the skin condition in detail, and in the short version, 3 items are used for screening. Similarly, nail clippers are assessed with 5 items in the long version and screened with 2 items in the short version. Prior literature can fully evaluate “skin condition” and “nail clippers” included in the scale. Furthermore, the scale was tailored so that items necessary for assessing patients with diabetes, such as “consideration to the foot” and “self-efficacy,” were included.
It could be easily used to screen older patients with diabetes, to determine how well they are able to self-manage their foot care. Not only can it be used for predicting how much foot care a patient can self-manage, but it can also provide basic information on the patient's psychological state and on the environment in which they live. Additionally, if an older patient with diabetes is unable to care for their feet themselves or if a patient's scores are low for a factor, a plan can be made to adjust their living environment or to provide the instructions or support needed to enable the patient to perform their foot care themselves. Whatever the case may be, given that good self-care of the feet should be an ongoing behavior, the scale would need to be used for periodic monitoring.
For the long version, although the 22-item FCS-ODL is much longer than the 10-item JFCCS, the Cronbach's alpha of .879 was higher than that for the short version. Thus, although it may take a bit longer to administer, it provides a more comprehensive assessment because it incorporates more factors that an older person may have trouble with. According to previous studies, there are 9 important factors for assessing the skin of the foot. Thus, the condition of the skin in diabetic foot disease needs to be thoroughly investigated, especially in elderly people. Aside from the 8 items of the JFCCS that were included in the long version, other items for assessing elderly people with diabetes have been added. The FCS-ODL version would be more suitable for an assessment requiring a more detailed evaluation. Thus, the short version, the FCS-OD, can be used when time is an issue, as in clinical practice, and the FCS-ODL can be used when a detailed evaluation is desired.
The sample size used in our study was limited to patients from a single outpatient clinic. In the future, studies need to be conducted using a more diverse and extensive population. Additionally, the scale needs more verification through studies conducted in actual clinical practice by medical professionals rather than researchers. Another limitation was that, although the scale was created following international standards, we were unable to record and transcribe the interviews used in the coding of data for developing preliminary survey items.
In this study, we developed and tested the reliability and validity of a foot care self-management assessment tool for older Japanese patients with diabetes. We found that the FCS-OD can be useful in assessing how Japanese patients with diabetes self-manage foot care at home. Moreover, the scale can be used to comprehensively evaluate foot care in older adults. However, it was not possible to evaluate current protocols for foot care using this scale. Therefore, further study is necessary to evaluate the effectiveness of current guidelines and interventions in foot care as well as the presence of conditions such as foot lesions in elderly patients with diabetes.
Footnotes
Acknowledgments
Authors’ Contributions
SS-M, MO, YA, KA, ST, and TT contributed to the conception and design of this study. SS-M, MO, KA, and KM performed the statistical analysis and drafted the manuscript. HT and HA critically reviewed the manuscript and supervised the whole study process. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research Grant for Longevity Sciences from the Ministry of Health, Labour and Welfare of Japan (grant number 30-25).
Ethical Approval
This study was conducted with the approval of the Ethics and Conflicts of Interest Committee of the National Center for Geriatrics and Gerontology (approval no. 1243, May 27, 2019).