
Abstract
In the present study, the efficiency of two formulations of maggot therapy: free-range larvae on the wounds and larvae in a special bag (larval-bag), was compared for healing diabetic ulcers with Wagner 2 diabetic ulcer. This study was conducted as a parallel randomized clinical trial. Out of 281 patients with Wagner grade 2 diabetic ulcers referred to the wound clinic, 54 patients who met the inclusion criteria were randomly assigned to intervention groups. The disinfected larvae of Lucilia sericata were put on the wounds with 2 methods, free-range larvae and larval-bag. Follow up was done at every 48 h interval until the full appearance of granulated tissues. The main measures were wound bed preparation, removing of necrotic tissues, appearing of granulated tissues, and removing of bacterial infections in the wounds. Statistical analysis based on the Kaplan–Meier curve and the Wilcoxon (Breslow) test showed a significant reduction in wound healing time by using free-range larvae in comparison with larval-bag (P = .03). The median time to debridement was 4 days in the free-range larval group (95% confidence interval: 3-9 days) while it was 9 days in the larval-bag group (95% confidence interval: 5-16 days). Debridement rate (proportion of removed necrotic tissue surfaces) at any time in the free-ranged larvae group was 1.78 times that of the bagged larvae group (95% confidence interval 1.01-3.15, P = .036). There was no significant difference between free-range larval use and larval-bag in the acceptability of maggot therapy by patients (P = .48). It can be concluded that both of two formulations of the larval therapy (free-range larvae and larval-bag) could be recommended for cleaning out and bed preparation of diabetic ulcers. However, using free-range larvae is hardly recommended on the wounds which are eligible to use.
Introduction
Diabetic foot ulcers are the most common complication of diabetes and a significant cause of morbidity and mortality in the world. 1 It is estimated that, annually, foot ulcers develop in 9.1 million to 26.1 million people with diabetes worldwide, and almost 20% of mediocre or intense diabetic foot infections lead to some levels of amputation.2,3 With the high prevalence of diabetes in Iran, it is estimated that more than 4.6 million people will be diagnosed with the diabetes in 2030, of which more than 20% will lead to amputation. 4 The estimated total economic burden of diabetic foot ulcers in the United States is more than 5 costliest cancers (breast, colorectal, lung, prostate, and leukemia), which costing a total of $79 billion in 2017. 5
There are different methods for the treatment of chronic diabetic wounds that the choice of a suitable method is one of the most important methods of diabetic wound management. 6 Debridement is the removal of necrotic and senescent tissues from a wound which is considered the first and the most important therapeutic step leading to wound closure and a decrease in the possibility of limb amputation in patients with diabetic foot ulcers. 7 Debridement using larval therapy is one of the oldest method of wound healing that has been used for the several hundred years. 8 Maggot debridement therapy (MDT) is a type of optional myiasis under controlled conditions that uses freshly emerged and sterile larvae of the common green-bottle fly, Phaenicia (Lucilia) sericata. 9
Although it is not fully understood how the maggots work, however, different mechanisms of wound healing by maggots were suggested which includes: wound debridement activity, antimicrobial activity “wound disinfection” and growth promoting activity “wound healing”. MDT is achieved through maggots’ secretion of proteolytic enzymes that liquefy the necrotic tissues and then feed on such tissues (wound debridement activity), wound disinfection (antimicrobial) activity, and growth-promoting (wound healing) activity. 10 Various studies have been performed on the healing of chronic wounds using maggot therapy.10,11 With the advent of antibiotic-resistant bacteria, larval therapy has received more attention from physicians and treatment staff and in 2004 the Food and Drug Administration (FDA) approved maggots as a medical device.12,13
Maggot's debridement has been suggested to work by mechanical and biochemical techniques. Mechanical debridement is caused by the specific mandibles or “mouth hooks” of the maggots and their rough body which both scratch the necrotic tissue. Furthermore, maggots produce excretions and secretion that possess proteolytic enzymes that can dissolve the dead and/or infected matrix on the wound bed. 14 In MDT, maggots are applied mostly by free release of larvae on the wound which make possible direct contact of larvae with the wound surface. It sometimes uses by means of larval-bag, in which larvae are allowed to act chemically on the wounds (indirect contact). In the dressing for free-range larvae, maggots are applied directly to the wound for 2 days and allowed to roam freely over the surface seeking out areas of necrotic tissue but due to which, maggots can escape out from the wound site, while in larval-bag dressing, the maggots are enclosed in a net pouch containing a piece of hydrophilic polyurethane foam, which is placed directly upon the wound surface, so that maggots cannot escape dressing.15,16 Controlled studies demonstrate the efficacy and safety of maggot therapy, however, in larval therapy using larval-bags, the mechanical mechanism of larvae for debridement of the wound is limited. 14 Use of maggots in the bag (larval-bag) may increase the range of wounds which are not permitted for usage of free-range larvae such as burning ulcers in which the free-range larval-use may be extremely painful, the wounds which are placed near main blood vessels or near the internal body cavities as well as the wounds near the main spinal cord. In practice, the use and renewal of larval-bag is simple.
So far, few studies have compared larval therapy using free-range larvae and larval-bags. Studies performed using larvae in bags are generally in the form of case reports or studies with small sample size. In most studies, the time of necrosis tissue removal between these two methods has not been investigated. This study was conducted as a parallel randomized clinical trial (RCT) for comparing the efficacy of removal of necrotic tissues in patients with Wagner 2 diabetic ulcers between the free-range larval method and the larval-bag.
Methods
Clinical Phase
Trial Design
This study has been designed as a parallel RCT with allocation ratio 1:1. Randomization has considered as a key element for the work. According to the random sequence created, participants were divided equally into 2 intervention groups which were received free-range larvae or larvae in bag as 2 kinds of interventions for comparing the results. Both of the groups were received standard of care measures including sharp debridement, antibiotic therapy, and food regimen schedule for diabetic patients.
Participants
The diabetic ulcer patients included in the study were aged above 20 years and were diagnosed with diabetes type 1 or 2, and had one or more ulcers and from February 2016 to January 2017 referred at the clinic of Academic Center for Education, Culture and Research (ACECR) of Tehran University of Medical Sciences (TUMS). Participants gave written informed consent.
Eligible participants had diabetic ulcers (assessed as an ankle brachial pressure index ≥0.6) with at least 25% of the wound covered by slough or necrotic tissue (larval therapy would not normally be used on wounds with less coverage). If a patient had multiple ulcers, the largest eligible ulcer was selected as the reference lesion. Patients were excluded if they were pregnant or lactating, were allergic to maggot, had grossly edematous legs, or were taking anticoagulants. Out of 281 patients referred to the wound clinic, 54 patients who met the inclusion criteria were randomly assigned into two intervention groups (Figure 1). In order to randomly assign participants into 2 study groups, the balanced block randomization method was used in this study. Out of a maximum of 6 forms for blocks with a size of 4, including 2 participants from each group, using the RANDBETWEEN command in Excel, 14 blocks were randomly selected and a random sequence was created.
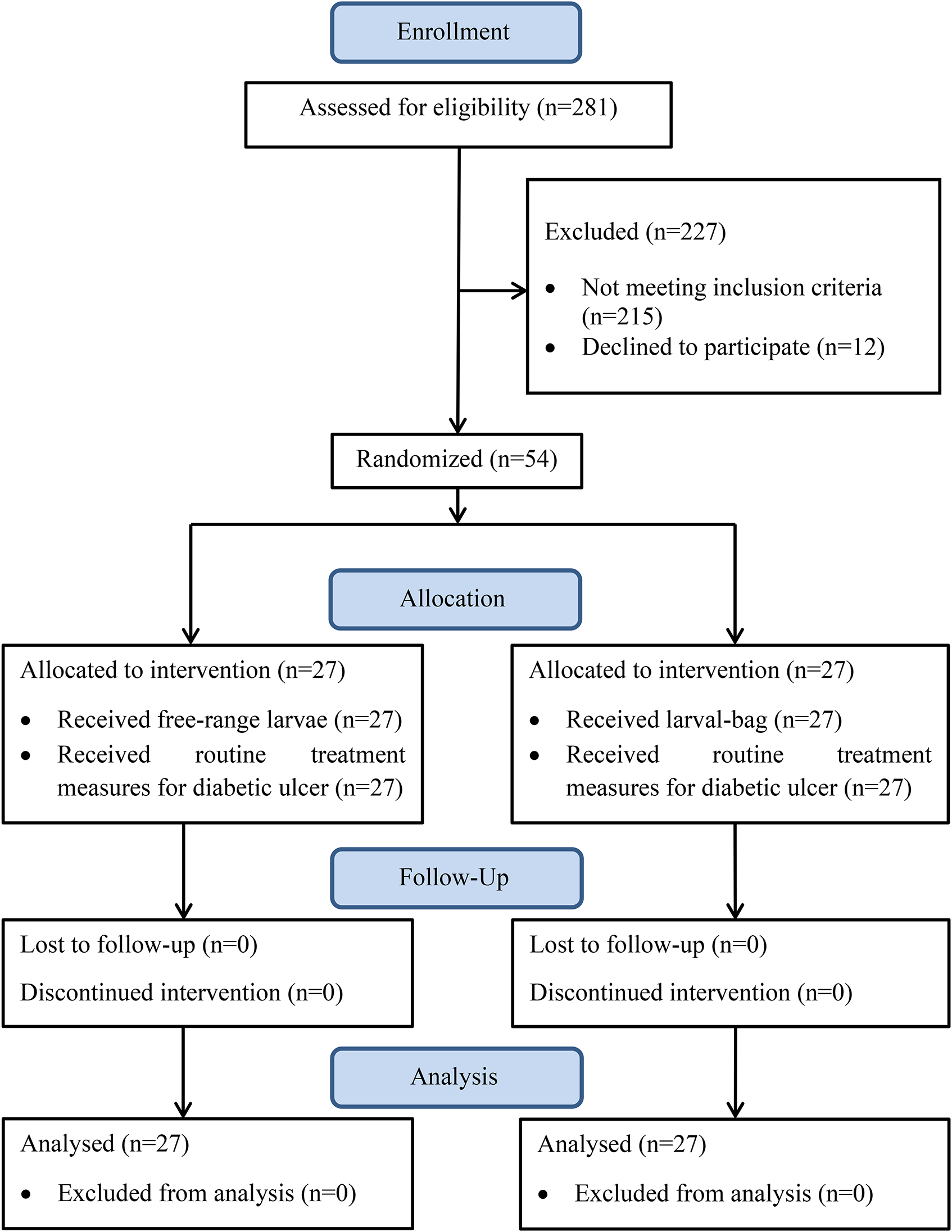
Flow of participants through the trial.
Interventions
In this study, for patients who met the inclusion criteria, after obtaining informed consent, larval therapy was performed by applying a cage-like dressing on the wound and sterile larvae of L. sericata were placed on the wound in 2 methods, free-range larvae or in the larval-bag for 48 h in a Tandem. Maggot applications and the first few dressing changes were performed by the physician or a trained technician and 7 to 10 larvae were placed per square centimeter of wound. After the first week or so of treatment, family members were sufficiently trained to perform the dressing changes themselves, but the maggot applications were always performed by professionals. After 48 h, the dressing was opened by a trained technician and the larvae are removed from the wound. The wound was washed with distilled water and the larval healing process continues until the necrotic tissue is removed. Zinc oxide or silver sulfadiazine was applied to the peripheral skin to protect the skin from irritation or maceration from the proteolytic wound drainage and maggot secretions.
Outcomes
Reducing the necrotic tissue surfaces has mentioned as primary outcome of the trial. Appearing of granulated tissues has mentioned as secondary outcome for this study.
Outcome Assessment
Before the start and after the end of each larval therapy round, length, width, and finally the area of necrotic and granular tissue in each wound were calculated using digital images by MATLAB software. 17 For more accuracy, the measurements for each wound were repeated 3 times in MATLAB software and the average of 3 measurements was entered in Stata software. All photos were taken with a digital camera and a common index after the wound was thoroughly washed. Data were collected using a checklist including demographic variables (age, sex, duration of ulcer, duration of diabetes), wound characteristics (necrotic tissue area, granular tissue area, and total wound area) and patient and medical staff satisfaction during the intervention. The time to complete removal of necrotic tissue and wound healing (debridement time) was considered as primary outcome and endpoint.
Sample Size
Based on the previous study, the healing rate of diabetic wounds for free-range larvae was 80%. 18 The minimum differences between 2 groups for showing the statistical difference has mentioned at least 40%. The sample size with 95% confidence interval (CI) and a power of 80%, has calculated as 24 wounds in each group. For preventing any unpredictable failure in completing the trial process, 3 wounds have added to the sample size of each group. So, the sample size for each group has mentioned 27 wounds.
Randomization
The balanced block randomization method was used for random arranging of the included patients into 2 study groups. Out of a maximum of 6 forms for blocks with a size of 4, including 2 participants from each group, using the RANDBETWEEN command in Excel (Microsoft, Redmond, WA, USA), 14 blocks were randomly selected and a random sequence was created.
Blinding
Due to nature of the larval therapy in both formulations, free-range larvae and larvae in bag, the blinding was not possible for this study.
Statistical Analysis
Continuous variables were described using mean (± standard deviation), and frequencies with percentages for categorical data. Baseline characteristics of participants were comprised using independent t-test for continuous variables and Chi-square test for categorical variables, between 2 groups.
In order to compare the differences between the 2 study groups in the time to debridement of ulcer, we used the Kaplan–Meier survival curve. Identified between-group differences were tested using the log-rank and Wilcoxon (Breslow) tests. Cox regression was used to calculate hazard ratios and 95% CIs. The proportionality assumption for the Cox model was evaluated with a test based on the Schoenfeld residuals.
Data were analyzed using Stata® (StataCorp. 2009, Stata Statistical Software: Release 11: StataCorp LP) and for all comparisons a P value of <.05 was considered statistically significant.
Entomological Phase
Preparing of Disinfected Maggot
For this study, L. sericata flies were rear in the insectarium of Tehran University of Medical Sciences with temperature conditions of 25 ± 2 °C and a humidity of 60 ± 5%. Adult flies fed with 10% glucose and chicken liver was used for spawning. Chicken liver was also used to feed the larvae. The eggs were washed with 70% ethanol solution and chloramine for disinfecting. 19 The disinfected eggs were transferred to sterile filter to flask and left 1 night in clean area hatching and preparing sterile first instar larvae for use as free-range larvae. For preparing suitable larvae for larval-bag, the previously disinfected larvae of first instars were put on sterile medium to be grown to young disinfected second instar and transferred to the sterile bags which are made of polyvinyl alcohol.
Results
Between February 2016 and January 2017, 281 patients with diabetic ulcers referred to the clinic of ACECR of TUMS. Fifty-four patients who met the inclusion criteria were randomly assigned into 2 intervention groups (free-range larvae and larval-bag) equally (27 patients for each group) to treatment. In this study, 29 (53.7%) patients were male and 25 (46.3%) were female. As detailed in Table 1, the mean age of the patients was 59.0± 12.7 years old and their mean wound size was 7.25 ± 1.7 cm2. Before the intervention, the mean areas of necrotic and granulated tissue of wounds were 6.6 ± 1.8 and 0.9 ± 0.6 cm2, respectively. The mean history of diabetes in the subjects was 14.9 ± 8.0 years with an average of 12.2 ± 3.7 months were suffering from diabetic ulcers. Figure 1 shows the flow of participants through the trial and Table 1 summaries their baseline characteristics. Gender distribution, mean age, wound duration, disease duration, and area of necrotic and granular tissue of wounds were not significantly different between the 2 groups in the baseline (P > .05).
Preliminary characteristics of patients before the intervention (baseline characteristics).
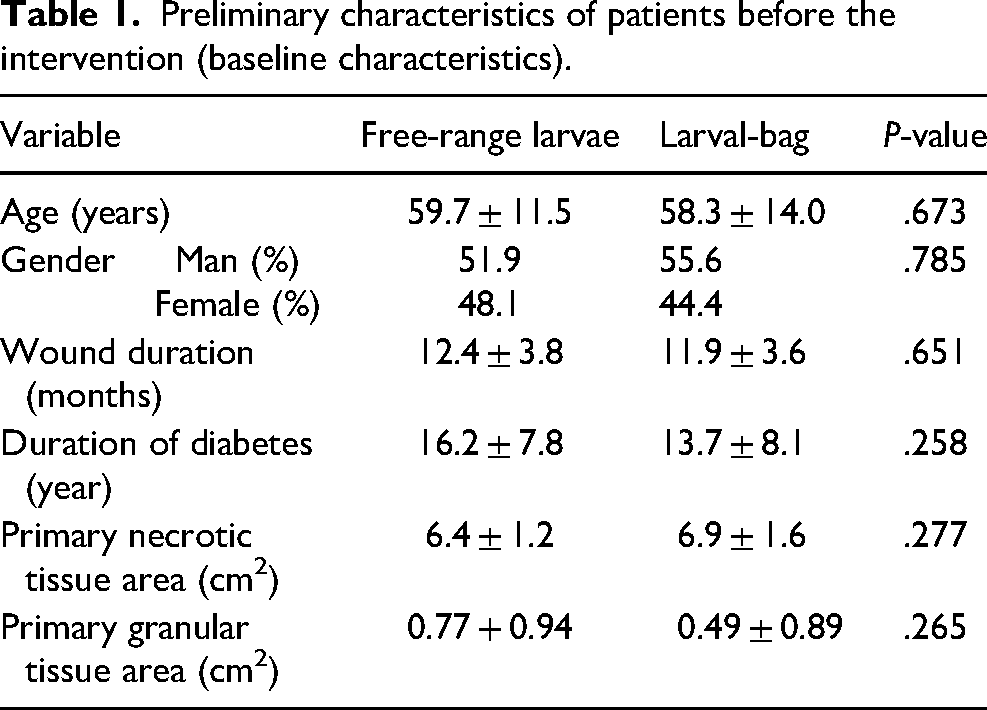
Figure 2 shows a comparison of wound healing time (debridement time) in the 2 groups using free-range larvae and larval-bag using the Kaplan–Meier curve. The results of log-rank (P = .04) and Wilcoxon (Breslow) (P = .03) tests showed that wound healing was significantly different between the 2 study groups and wound healing time was shorter in the free-range larval group. Also, the median time to debridement was 4 days in the free-range larval group (95% CI 3-9 days) and in the larval-bag group was 9 days (95% CI 5-16 days).
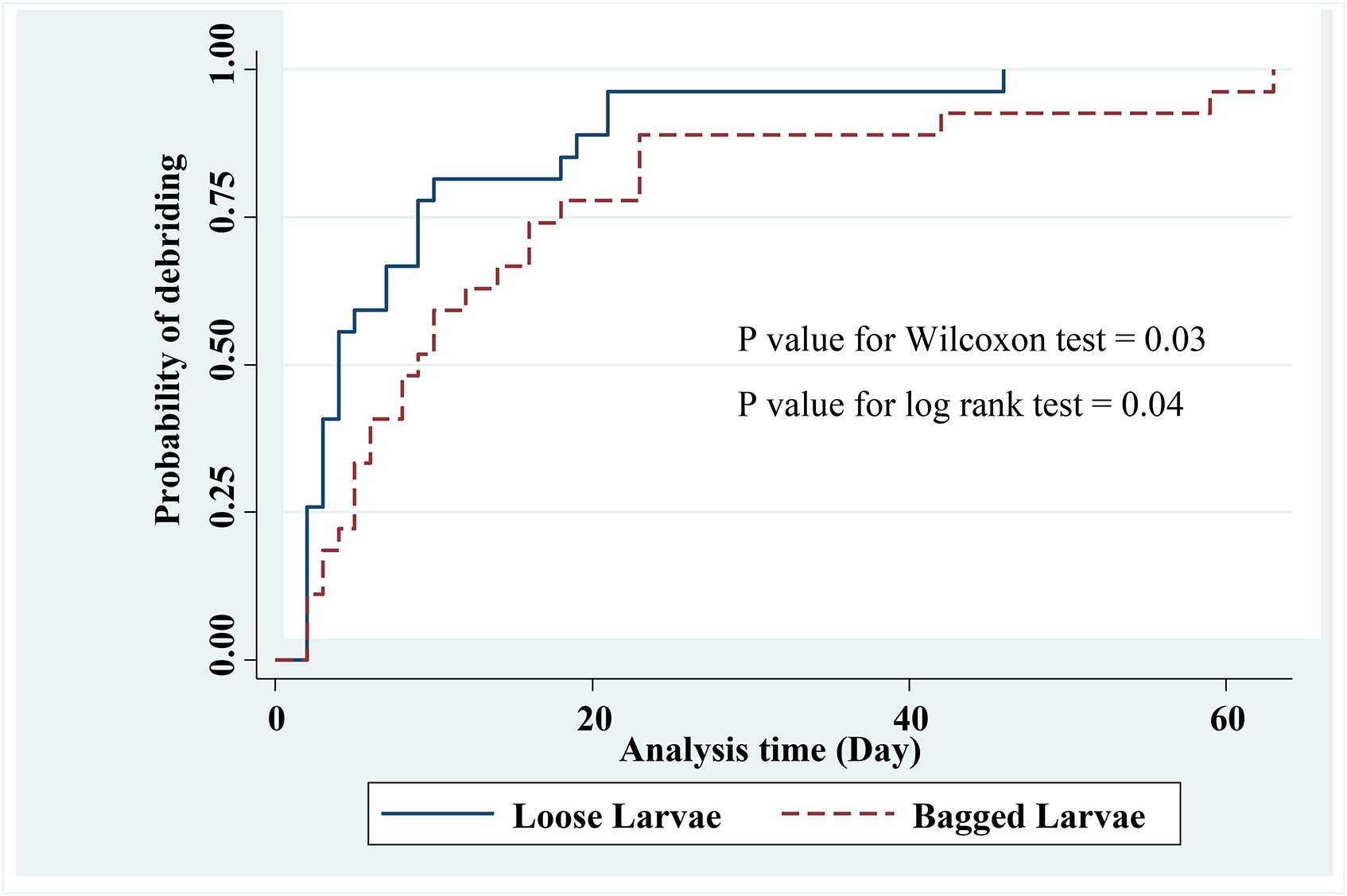
Kaplan–Meier plot of time to compare debridement duration of ulcer using loose larvae and bagged larvae.
The rate of debridement at any time in loose group was 1.78 times that of the bagged larvae group (95% CI 1.01-3.15, P = .036). According to the Schoenfeld residuals test, proportionality assumption was confirmed for type of intervention (P = .61). Therefore, using Cox regression, the hazard ratio in the free-range larval group compared to the larval-bag group was 1.86 (95% CI 1.05-3.31). This indicates the probability of wound healing and necrotic tissue removing in the free-range larval group is 1.86 fold faster time than the larval-bag group (P = .033).
In this study, the level of satisfaction of patients and medical staff was evaluated using 2 methods: free-range larvae and larval-bag (Figures 3 and 4). There was no significant difference between patients’ satisfaction with the methods of free-range larvae and larval-bag (P = .48). Patients’ satisfaction with larval therapy using free-range larvae and larval-bag larvae was 85.2% and 77.8%, respectively. Also, there was no significant difference between the satisfaction of the medical staff for treatment using free-range larvae and larval-bag (P = .09). The satisfaction of the medical staff with MDT using free-range larvae and larval-bags was 96.3% and 81.5%, respectively.

Diabetic ulcers healing of 2 patients (1 and 2) treated with free-range larvae of L. sericata: (a) before maggot therapy, (b) during maggot therapy, and (c) after maggot therapy (original photos). Neither harm nor side effect was observed during and after treatment.

Diabetic ulcers healing of 3 patients (1, 2, and 3) treated using made larval-bag with L. sericata larvae: (a) before maggot therapy, (b) during maggot therapy, and (c) after maggot therapy (original photos). Neither harm nor side effect was observed during and after treatment.
Discussion
The larvae of L. sericata are used commonly in tow methods of maggot therapy, free-range larvae in wound and larval-bags (the alive larvae in bag). Use of larval-bag seems to be easier practically in comparing with free-range larvae on the wounds. Either releasing larvae to the wound or removing them from the wounds makes somewhat limitations in clinics for free-range larvae. On the other hand, the free-range larvae method allows employing full potential of larval activities both mechanical and chemical. Due to this reason, some small limitations of free-range larval use could be ignored.
One of the most important issues in process of maggot therapy is to know how many times it should be used for the wounds. In the study of Steenvoorde in treatment of 54 wounds with maggots of L. sericata, the average larval therapy has estimated as 2.4 times in average for significant reduction in necrotic tissues. 20 The duration needed for debridement is another important matter in the process of maggot therapy. This duration has estimated as 14 days in average in the study of Dumville. 21 In the present study average duration for treatment of the cases with free maggots was 4 days which was 1.86 better than larval-bag. The reduction in efficiency was due to the restriction of the larvae from physical contact with the wound surface. Average time duration in the use of larval-bag was 9 days in a study which was done by Steenvoorde et al 2007. 22 Dumville used larval-bag for treatment of 86 cases and estimated time for debridement as 28 days. However, they did not observe significant difference between 2 methods of larval use, free-range larvae and larval-bag. 21 In the present study, the median time duration for debridement of wounds was 9 days. Average rate of wound healing in the larval-bag method was 1.76 less than free-range larval use.
Patient acceptability for the maggot therapy trials may influence the results. There are various factors which can affect the level of acceptability for the larval therapy. Patient acceptability for maggot therapy was about 75% in the conducted study by Spilsbury by means of 2 questionnaires for 35 patients 23 and it was found some of the factors affecting patient acceptability were duration of treatment, type of alternative therapy, ideas of relatives and disgusting view of larvae in the wounds. The latest factor, disgusting view of larvae in the wounds, was the most effective in the change of mind of the patients. 23 In the similar study which has been done by Sherman, more than 95% of the medical staff and 90% of the patients were satisfied with maggot therapy. 24 In the present study, the degree of acceptability of both of medical staff and patients from larval-bag was higher than free-range larvae. The patients were clearly followed the ideas of medical staffs.
Conclusions
It can be concluded that using of free-range larvae is hardly recommended on the wounds which are eligible to use. Otherwise, use of larvae in bag is more accepted with the patients and medical staff which can be recommended to use for wide variety of the wounds. The larvae in bag gain from all chemical mechanisms of the larvae in the maggot therapy process.
Footnotes
Acknowledgments
The authors wish to thank all personals of 3 cooperating divisions of Tehran University of Medical Sciences, including wound clinic of ACECR, Department of Medial Entomology, and Department of Medical Pathology.
Data Availability
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project has supported financially by the Tehran University of Medical Sciences with the research code of 96-01-27-34029.
Ethical Approval
This study was approved in Committee of Ethics in Medical Research of Tehran University of Medical Sciences with code of IR.TUMS.SPH.REC.1395.1533 and registered in website of Iranian Randomized Clinical Trial (IRCT) with the code of IRCT2017053134272n1. For maggot therapy on the diabetic foot ulcer of patients, all work was conducted in accordance with the Declaration of Helsinki (1964).