
Abstract
Post-traumatic stress disorder (PTSD) and alcohol use disorder (AUD) are common among university students in South Africa. Despite the prevalence of common mental disorders such as PTSD and AUD, access to mental health services, especially evidence-supported trauma-focused treatments, remains limited in South African university settings. We aimed to evaluate the effectiveness, feasibility, acceptability, and appropriateness of massed prolonged exposure therapy (PE) for comorbid PTSD and AUD in a South African university setting. A single clinical case (N = 1) was screened using the PTSD Diagnostic Scale for DSM-5 (pre-intervention = 62; post-intervention = 17), clinically assessed at baseline using the Clinicians-Administered PTSD Scale for DSM-5 (pre-intervention = 60; post-intervention = 8), and the Alcohol Use Disorder Identification Test (pre-intervention = 11; post-intervention = 6). During treatment, assessment was measured by the PTSD Checklist for DSM-5 (Session 1 = 56 to Session 10 = 20). Moreover, massed PE was experienced and perceived as feasible, appropriate, and acceptable by the case participant. We discuss the effectiveness and utility of massed PE as an evidence-based treatment for PTSD and AUD, and the utility of accelerated treatments in university settings in South Africa.
Theoretical and Research Basis for Treatment
University students in South Africa have an increased conditional risk of developing post-traumatic stress disorder (PTSD) due to increased trauma exposure to sexual assault, robbery, and other forms of violence and trauma exposure (Padmanabhanunni, 2020). The prevalence of PTSD among South African university students is estimated at 21.0% (N = 28, 268), making PTSD one of the more prevalent mental disorders among university students in South Africa (Bantjes, Kessler, Hunt, et al., 2023).
Cross-sectional studies have found that 90% (N = 1,337) of South African university students have experienced at least one traumatic event, with suicide or homicide of a close person or family member, witnessing harm to another, and life-threatening situations being the most common (McGowan & Kagee, 2013). These traumatic experiences increase the risk of developing PTSD and comorbid alcohol use disorder (AUD) (Smith et al., 2016), especially in a population that has a high prevalence of alcohol use (Blows & Isaacs, 2022).
Comorbid conditions, such as AUD, are prevalent among university students with PTSD in South Africa, which can further complicate their recovery (Blows & Isaacs, 2022; Peltzer & Pengpid, 2015). Studies have shown that up to 33.4% (N = 6000) of university students in South Africa engage in hazardous drinking behaviour (Young & De Klerk, 2008), and alcohol use is often used as a coping mechanism to manage the symptoms of PTSD (Read et al., 2014). Alcohol use among university students is also associated with consequences, such as unsafe sex, absenteeism, and academic failure (Blows & Isaacs, 2022; Htet et al., 2020).
Several studies have reported high rates of comorbidity between PTSD and AUD. One study found that (N = 800) those students who engage in alcohol use reported elevated PTSD symptoms and that hazardous drinking was associated with a higher likelihood of having elevated PTSD symptoms, compared to non-drinking university students (Peltzer & Pengpid, 2015). Pengpid et al. (2013) found that (N = 722), 21.1% of university students (N = 152) tested positive for the AUDIT with a score of 8 or more, which is associated with harmful and hazardous drinking. Despite the high prevalence of PTSD and AUD among university students in South Africa, access to and research on the effectiveness of TFTs within universities and broader South Africa are limited (Booysen et al., 2020a, 2021).
Prolonged exposure therapy is a first-line treatment for PTSD (McLean & Foa, 2024; McLean & Goetter, 2024). Research on the acceptability of PE in culturally and ethno-racially diverse settings has received continuous attention over the last few decades (Garcia et al., 2023). Since the late 1980s, empirical evidence has been accrued to support the effectiveness and acceptability of PE across various trauma types, populations, ethno-racial groups, and cultures in various countries such as the US, Poland, Russia, South Africa, and Japan, among others (Feske, 2008; McLean & Foa, 2024). To this end, research on PE for PTSD has not only prioritised effectiveness but is also continuously investigating the feasibility and acceptability of PE in diverse settings and populations (Garcia et al., 2023).
Considering the high comorbidity of PTSD, the robustness of PE has been evaluated to ameliorate, among others, symptoms of comorbid conditions such as substance use disorders (van Minnen et al., 2012). Despite initial concerns regarding the contraindication of PE for PTSD and substance use disorders (i.e., alcohol use), Pierce et al. (2020) found that PE, in the context of SUDs, does not worsen substance use, which makes PE an effective but also acceptable and appropriate treatment in this population. Furthermore, an integrated version of PE for co-occurring substance use, known as COPE, is an effective and feasible treatment for persons with comorbid PTSD and Substance Use Disorders (SUDs) (Back et al., 2015). Back et al. (2019) found that participants attended between 8-15 sessions and had greater improvement in the COPE condition compared to relapse prevention, even at 6-month follow-up.
In recent years, accelerated formats of PE have been developed to increase the reach, feasibility, and acceptability of the treatment among various patient populations and settings (Blount et al., 2014; Dell et al., 2023; Foa et al., 2018; Peterson et al., 2023). Massed PE is a treatment approach for PTSD that involves repeated exposure to trauma-related stimuli over a more-or-less 10-day period, in contrast to Standard PE, in which therapy duration lasts between 8 and 15 weeks (Htet et al., 2020). During the sessions, patients engage in imaginal exposure, where they recount and vividly describe the trauma memory, and in vivo exposure, which is when a patient confronts safe situations that they have been avoiding. The goal of MASSED PE is to help patients learn to confront and manage the learnt fear associated with the memory of the traumatic experience, and to reduce PTSD symptoms within a shorter period of time (Htet et al., 2020).
Universities contribute to the general mental healthcare of students, addressing issues ranging from stress and anxiety to depression and PTSD (Banjtes et al., 2023a). These centres typically offer a variety of services, including individual therapy, group therapy, workshops, and crisis intervention (Bonar, 2015). Despite the broad range of services offered, mental health services often struggle with resource limitations, thus impacting their ability to serve the student population effectively (Banjtes et al., 2023a). The demand for mental health services in university settings has significantly increased over the years, placing a considerable burden on counselling centres (Bantjes, Kessler, Lochner, et al., 2023; Watkins et al., 2012). Many centres are under-resourced and face challenges in meeting this growing demand, resulting in long waiting lists and limited session availability.
Despite the increasing need for effective mental health interventions, many university counselling centres continue to rely on therapy modalities that have inferior or unvalidated treatments may not be the most effective for specific conditions, such as PTSD (Abrams, 2022). The goal of MASSED PE therapy is to deliver the same amount of exposure therapy more rapidly, with the hope that this will reduce drop-out and still improve outcomes for PTSD and comorbidities, such as AUD. This is especially useful in low-resource settings where SPE, that is 3-6 months, is not feasible. With a high prevalence of trauma exposure, PTSD, and alcohol use among university students in South Africa, as well as limited access to effective TFTs, it is crucial to investigate the effectiveness and feasibility of MASSED PE in the treatment of comorbid PTSD and AUD among university students.
We aimed to investigate whether massed-prolonged exposure (MASSED PE) therapy is an effective, feasible, and acceptable treatment for PTSD and comorbid alcohol use in a single case participant. The proposed study will be guided by the following research hypothesis and questions: (a) massed prolonged exposure therapy will improve symptoms of PTSD and alcohol use disorder among a university student at a community psychology clinic, (b) Does a university-going student perceive and experience massed-prolonged exposure as a feasible, acceptable, and appropriate therapy for PTSD and AUD?
Case Introduction
To protect the privacy of the patient, a pseudonym is used. Amy was a 23-year-old female who lost both her parents during childhood, suffered neglect and multiple sexual assaults as an adolescent. At the time of the intervention, she was a graduate student in the humanities and resided off-campus.
Presenting Complaints
Amy was sexually assaulted by a stranger in 2017 while she was at a music festival with her friends. She reported that two incidents of sexual assault occurred on the same night of the festival. The first incident was when she went to the public restroom at the festival and a stranger forced himself onto her. He pushed her to the ground, attempting to sexually assault her, but abandoned the assault as she resisted. The second incident that night was when Amy was unable to locate her friend group at the festival. She reported that a stranger indicated that he knew where her friends were and that he would take her to where the group was. After leaving the crowded area with him, he pushed her down a hill and attempted to rape her, but again did not proceed. Amy reported that a rape kit test was conducted and revealed traces of semen, but that she was not penetrated.
After these traumatic events at age 17, Amy reported having lived with signs and symptoms reflective of PTSD. Notably, she reported significant avoidance of specific places and situations that reminded her of the music festival. Amy reported that she would often social and crowded spaces (i.e., bars and pubs) because they reminded her of the festival night. She indicated that she would spend time only with friends if it were in a space that felt safe to her, such as her home. Amy also experienced intrusive symptoms, marked by distressing memories and physiological reactions, triggered by cues associated with the trauma. She reported that she often experienced nightmares associated with the music festival, which often impacted her quality of sleep. In addition, Amy had changes in her mood and cognition, reflecting the pervasive nature of the trauma’s impact on her emotional and cognitive well-being. For instance, Amy had a negative bias in terms of her interpretation of the traumatic events that had occurred in her life, which were centred on feelings of shame and guilt. She believed that the sexual assault was her fault because she was drinking alcohol, and that perhaps it would not have happened if she had been more responsible.
Arousal and reactivity symptoms were also evident. Amy described being uncomfortable and startled when people walked behind her. She reported that one evening, she was walking home, and the university security was patrolling behind her on a bicycle to get home safely. However, she indicated that this brought about significant distress and worry, even though she knew he was ensuring her safety. Her hypervigilance and reactivity underscored her increased and persistent awareness of threats and danger. Amy also reported an increased use of alcohol, despite its harmful consequences. The alcohol use was framed as a means of coping, albeit it is maladaptive.
History
Amy’s childhood was marked by early adverse and traumatic experiences; she lost both her parents when she was a child. As a result, Amy and her sister had to enter social services and were placed with adoptive parents. Amy indicated that she had an older brother; however, he was not responsible, nor willing to take care of her and her sister. Amy indicated that her adoptive parents did not provide a caring and supportive environment, and she would often be subject to verbal and emotional abuse.
Moreover, she reported that the adoptive parents failed to provide them with the necessities for living, such as food and clothing. For Amy, the transition and trauma of no longer living with her biological parents and being placed in foster care with adoptive parents were difficult. She reported, however, that she felt guilty at times because when she left for high school, she decided to live in the school accommodation, leaving her sister behind. It was during high school, at the age of 17, when Amy was sexually assaulted. After this traumatic event, Amy reported that she was able to complete high school and pursue a degree in sociology.
She indicated that she often had many existential questions about the adversity and traumas in her life, such as losing both her parents and being a victim of sexual assault. Yet she reported that her education became a beacon of hope and the idea of creating her own independent life. However, since the traumatic event, she has struggled to integrate what has happened and has never received any trauma-focused psychotherapy for her PTSD.
Assessment
An initial screening assessment was conducted via an online advert that contained a link to a Google Form that consisted of a demographic questionnaire and the PTSD Diagnostic Scale for DSM-5 (Foa et al., 2016). The PDS-5 assisted in ascertaining a history of traumatic exposure and clinically significant symptoms. Once eligibility was determined that the participant had clinically significant symptoms, a structured clinical interview was conducted using the Clinician-Administered PTSD Scale for DSM-5 (CAPS-5; Weathers et al., 2018). The following measures were used to collect treatment outcome data to measure PTSD, alcohol use, and the feasibility and acceptability of massed PE:
PTSD Diagnostic Scale for DSM-5 (PDS-5)
The PDS-5 (Foa et al., 2016) is a self-report measure for PTSD symptoms with twenty items. It has demonstrated excellent internal consistency (α .95), good test-retest reliability (r = .90), and good convergent and discriminant validity with other PTSD measures, such as the PTSD Checklist— Specific Version and the PTSD Symptom Scale—Interview Version for DSM–5, as well as with measures of depression and anxiety (Foa et al., 2016).
Clinician-Administered PTSD Scale for DSM-5 (CAPS-5)
The CAPS-5 (Weathers et al., 2018) is a structured diagnostic interview for PTSD symptoms, with a 5-point ordinal scale to rate symptoms in the past month. Total scores range from 0 to 80, with higher scores indicating more severe symptoms. The CAPS-5 has demonstrated high internal consistency (α = .88) and good reliability and validity (Weathers et al., 2018).
Alcohol Use Disorder Identification Test (AUDIT)
The AUDIT questionnaire (Saunders et al., 1993) is a 10-item tool that detects hazardous and harmful alcohol use in primary healthcare settings. Scores range from 0 to 40; a score of 8 or more indicates hazardous or harmful alcohol use, while a score of less than 8 indicates non-hazardous consumption.
Post-Traumatic Stress Disorder Checklist for DSM-5 (PCL-5)
The PCL-5 (Weathers et al., 2013) is a 20-item self-report measure that assesses the 20 DSM-5 symptoms of PTSD. The PCL-5 has a variety of purposes, including (a) Monitoring symptom change during and after treatment; (b) screening individuals for PTSD, and (c) making a provisional PTSD diagnosis. The PCL-5 test scores demonstrate good internal consistency (α = .96), test-retest reliability (r = .84), and convergent and discriminant validity (Bovin et al., 2016).
Implementation Measures
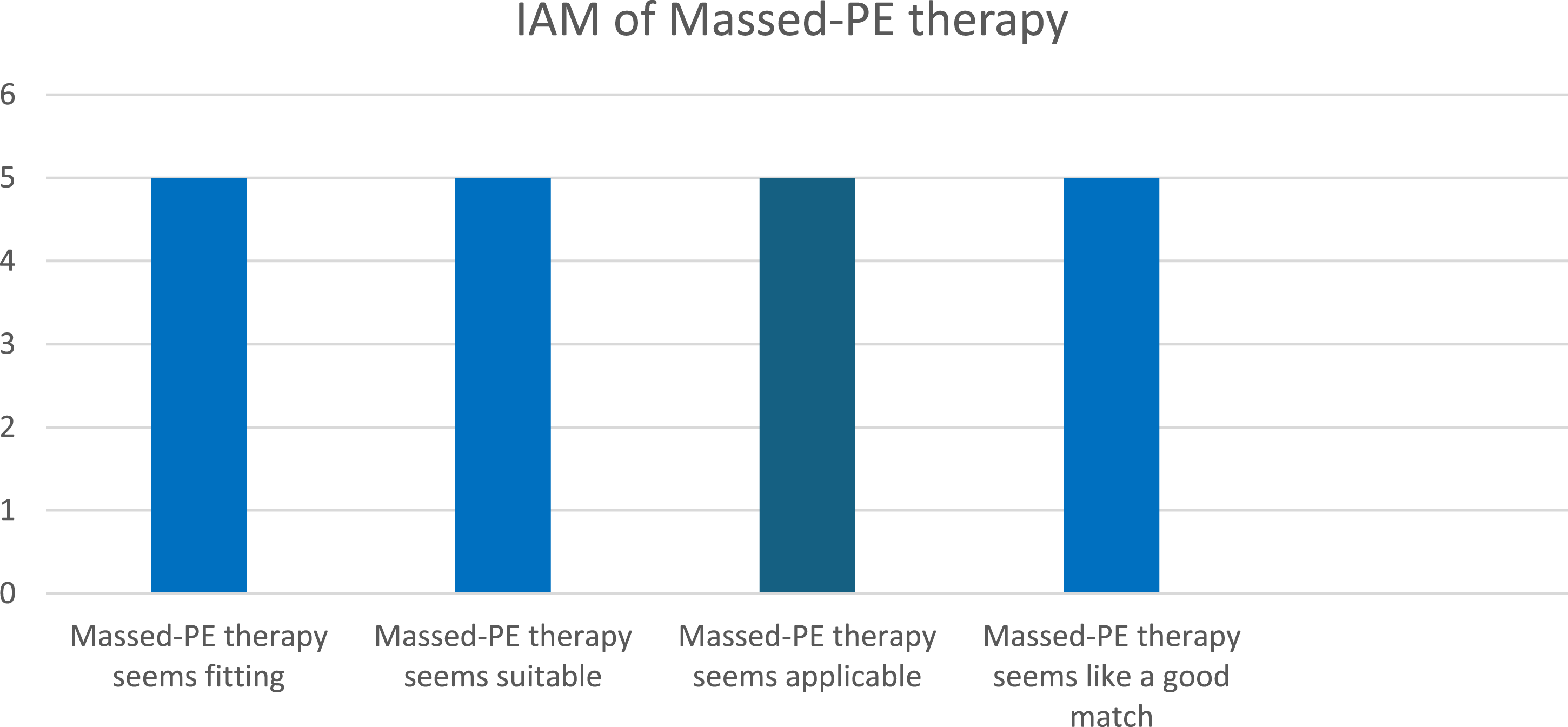
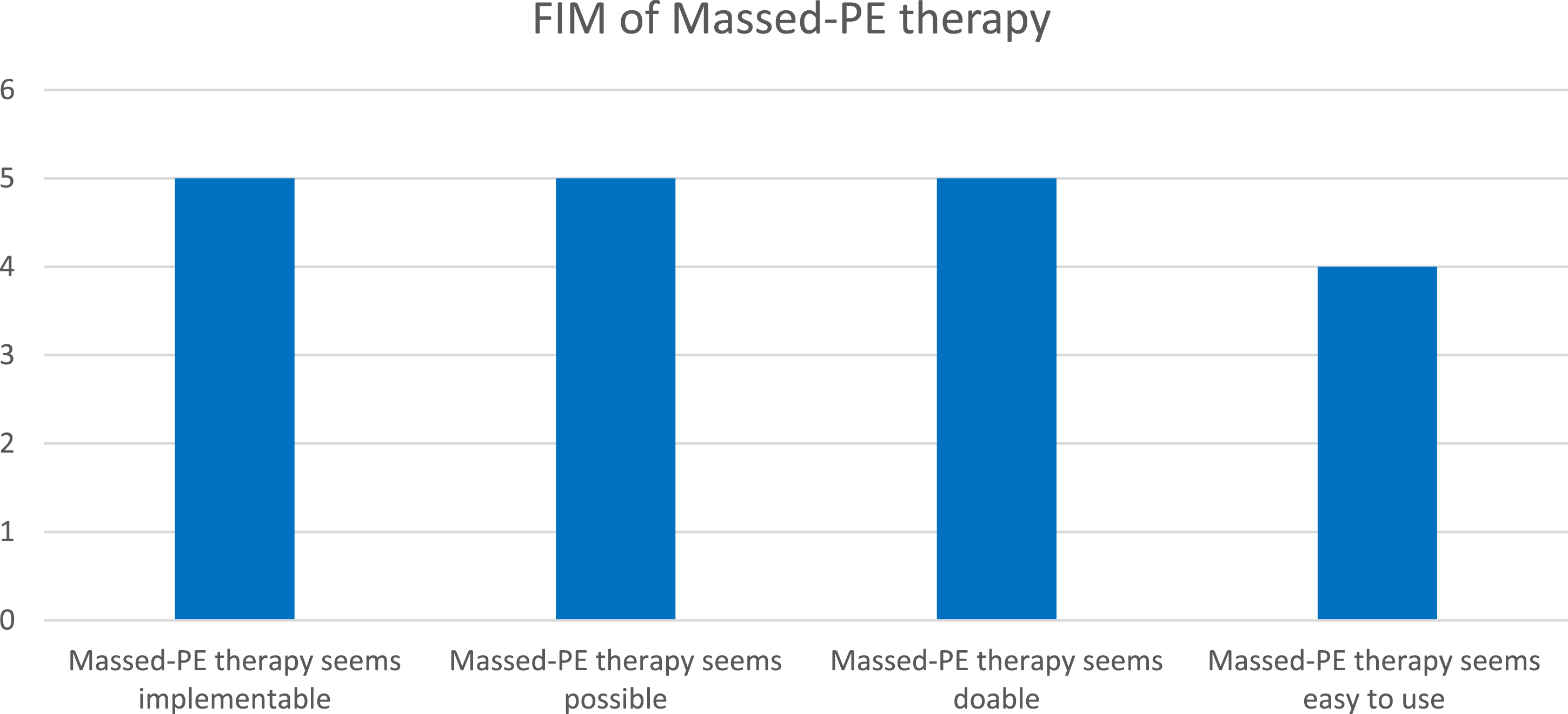
The implementation measures are made up of three sub-measures, namely, the Acceptability of Intervention Measure (AIM), the Intervention Appropriateness Measure (IAM), and the Feasibility of Intervention Measure (FIM). Each measure consists of four questions with five categories to be selected, ranging from 1 (Completely disagree), 2 (Disagree), 3 (Neither agree nor disagree), 4 (Agree), and 5 (Strongly agree). For example, participants could report whether they agree or disagree with whether the intervention is acceptable, appropriate, or feasible.
Case Conceptualisation
Emotion processing theory (EPT) delineates the aetiology, maintenance, and amelioration of emotional structures which underpin PTSD (Brown et al., 2019; Foa & Kozak, 1986). EPT posits that traumatic events can result in the development of emotional structures such as fear, which is embedded in a cognitive network which is encoded with information about the stimuli, responses, and meaning of the responses and stimuli associated with a specific traumatic event (Brown et al., 2019). For instance, a female survivor of sexual assault by an unknown male in a restroom at her place of work can develop an emotional structure, such as fear, which has distorted associative learning about stimuli and responses. A restroom at work (Unconditioned Stimulus; US) is now perceived as a dangerous place due to the association with the sexual assault (Conditioned Stimulus) and the restroom (US). The emotional structure now includes a CS (i.e., restrooms, men, work environment, etc.), the US (i.e., sexual assault), and CR (i.e., fear, avoidance, shame, guilt, blame, and anger). The stimuli and responses are associated with new, and usually erroneous, meanings, such as “I am weak”, “I am not safe anywhere”, and “all men are dangerous”.
To ameliorate emotional structures, activation of such emotion structures is required via exposure procedures such as imaginal and in vivo exposure. Activation of emotional structure allows for the processing of cognitions and emotions, such as fear and erroneous cognitions (“all men are dangerous”), to enable the encoding of competing information (i.e., not all men are dangerous, or my work environment is not a completely dangerous place) (Brown et al., 2019; Foa et al., 2019). Amy’s trauma of sexual assault resulted in the onset of a psychopathological emotional structure that developed in erroneous cognitions and avoidance (Rauch & Foa, 2006). After the sexual assault, she had become afraid of being in crowded spaces, at festivals or concerts and avoided conversations with men. Amy avoided memories about the sexual assault, as well as thinking or speaking thereof. Moreover, she avoided external reminders, such as not drinking certain alcoholic beverages, avoiding bars and conversations with men. Yet, Amy’s alcohol use, which is a maladaptive means of coping with her PTSD symptoms, can also be conceptualised as a means of avoidance to cope with symptoms such as intrusions and negative emotions, such as fear and shame. Furthermore, one could speculate that her alcohol use was also a safety behaviour, meaning that she could only engage in specific tasks or situations when using alcohol. Her alcohol use, fundamentally, is part of avoidance, which perpetuates her PTSD symptoms.
To modify these erroneous elements contained in the emotional structure, the fear structure had to be activated by using exposure techniques, such as imaginal exposure and in vivo exposure (Foa et al., 2019). According to EPT, it is deemed advantageous for clients to present with an increased level of emotional and physiological reactivity when engaging emotional structures, as it is indicative of an activation of the broader cognitive network. During the imaginal exposure, Amy displayed an increased level of discomfort when recounting the trauma memory, which was measured by her subjective units of discomfort (SUDs). A crucial aspect of PE is not only the engagement of the emotions associated with the trauma memory, but the processing of these emotions and cognitions (Foa et al., 2019). Processing was facilitated after imaginal exposure was conducted, and at times, increased levels of emotions, which might have been over-engagement, were managed in a supportive manner.
Importantly, Amy started processing her underlying beliefs about herself and the world. Initially, she believed that she was fundamentally unsafe and that the world was a dangerous place. Through exposure and emotion processing, Amy started to process these beliefs. She began to see that not all men are dangerous and that crowded spaces can be safe. These shifts in her cognitions were crucial in reducing her avoidance behaviours and in increasing her engagement with previously feared situations. EPT accounts for these changes in beliefs, which are essential for the therapeutic process.
Amy’s ability to process her trauma emotionally and cognitively led to a more adaptive and realistic understanding of herself and her environment, contributing significantly to her overall improvement. Amy reported that Massed-PE provided her with the language for what she was experiencing and explained symptoms, such as her avoidance habit. Moreover, she was able to identify cognitive distortions and negative beliefs to benefit from her quality of life moving forward, which the client found liberating. Massed-PE was chosen as a modality due to Amy’s diagnosis of PTSD and her limited time left on campus. Amy’s treatment occurred during the latter part of the academic year, and she was scheduled to leave town soon after the completion of her examinations and treatment.
Course of Treatment and Assessment of Progress
The treatment consisted of ten massed PE sessions, which were between 60 and 90 minutes long over a two-week period. We chose a two-week period to stay within the format of intensive treatments, although it can be over three weeks or more. Yet more importantly, the two-week period aligned with the availability of Amy as she had planned to leave town after the completion of treatment; therefore, the briefest format was chosen in the study. Sessions were audiotaped for Amy to listen to at home as part of the homework. In session 1, Amy received an overview of the treatment plan and a general explanation of Massed-PE at the first session. Thereafter, she was asked questions about the trauma, using the Trauma Interview to obtain information about it. The Trauma Interview is a standard PE trauma interview, and the PE Manual contains information about the PE trauma interview. The session concluded with an introduction to breathing retraining, a general coping skill to be used in everyday life. Amy was given homework, which consisted of reading the rationale for the treatment, listening to the session’s audio recording, and engaging in daily breathing retraining exercises.
In session two, the homework was checked, and if she had any difficulty practising the breathing retraining. A discussion about the common reaction was conducted, and to ground the discussion in Amy’s traumatic experiences, she was invited to link the relevant trauma reactions to her experience of PTSD. Amy was then given the rationale for in vivo exposure and encouraged to ask questions. A hierarchy of activities and situations that she was actively avoiding was then created. The session ended by encouraging Amy to engage in the in vivo activity before the next session and to practice her breathing retraining.
The third session began with a homework review. The rationale for imaginal exposure was explained to Amy, who then spent 45 to 60 minutes engaging in her initial imaginal exposure of her index trauma. While doing this, the participant received support through regular “check-ins” and encouragement and was asked to rate their level of SUDs during the imaginal exposure. After imaginal exposure, emotional processing for 15 to 20 minutes was conducted. Amy was then given homework again, this time consisting of daily listening to the audio recording of the imaginal exposure and continuing with in vivo exposure.
The intermediate sessions proceeded in essentially the same manner, yet systematic progress toward hotspots was encouraged and initiated as Amy habituated across sessions. Amy’s treatment progress was continuously reviewed via SUDs and PCL-5 scores. As the sessions came to an end, the importance of continuing to apply everything she had learnt was encouraged. Before termination, relapse prevention discussions were encouraged. As in the baseline phase, the post-intervention measures were administered at the last session.
Treatment and Implementation Outcomes
At the time of the intake, Amy met the criteria for PTSD, which were based on the CAPS-5 and PDS-5. The participant’s total CAPS-5 symptoms severity score was 60 at baseline and a score of 8 at post-intervention (Figure 1). Participants CAPS-5 Scores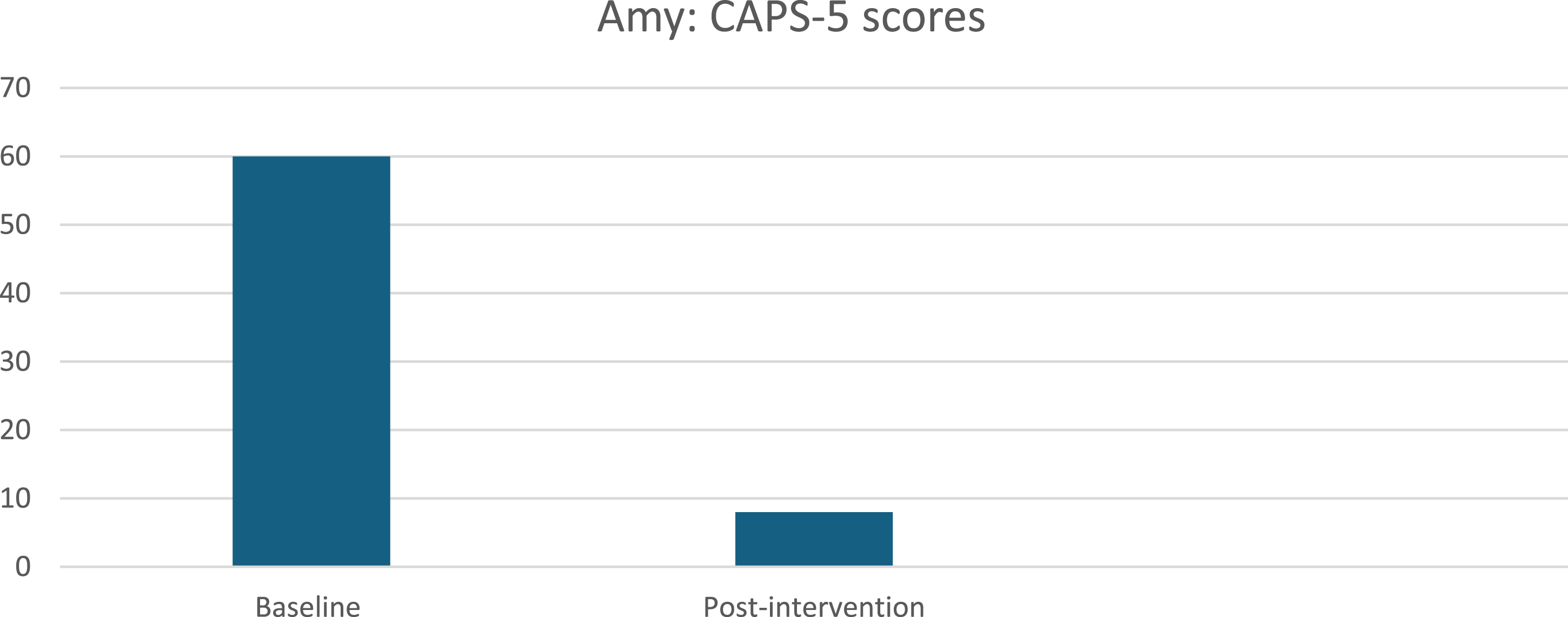
Amy’s PTSD symptoms on the PDS-5 were also significant. At baseline, Amy had a total score of 62, while the clinical cut-off score is 28. At post-intervention, she had a PTSD severity score of 17, suggesting a sub-clinical diagnosis. Figures 2 and 3 below illustrate the participant’s PDS-5 and AUDIT scores at baseline and post-intervention. It is important to note that the PDS-5, unlike the CAPS-5, which is a clinician-administered assessment, is a self-report measure. Despite the inherent differences in administration, the self-report results from the PDS-5 were in line with the CAPS-5. This consistency between the two measures strengthens the reliability of the findings, indicating that the reductions in PTSD symptoms observed in Amy indicate a reliable, genuine change in her symptomatology. Amy presented with hazardous and harmful drinking as indicated by the results of her AUDIT score. At baseline, she presented with a total score of 11 and a total score of 6 at post-intervention. Participant’s PDS-5 Scores Participant’s AUDIT Scores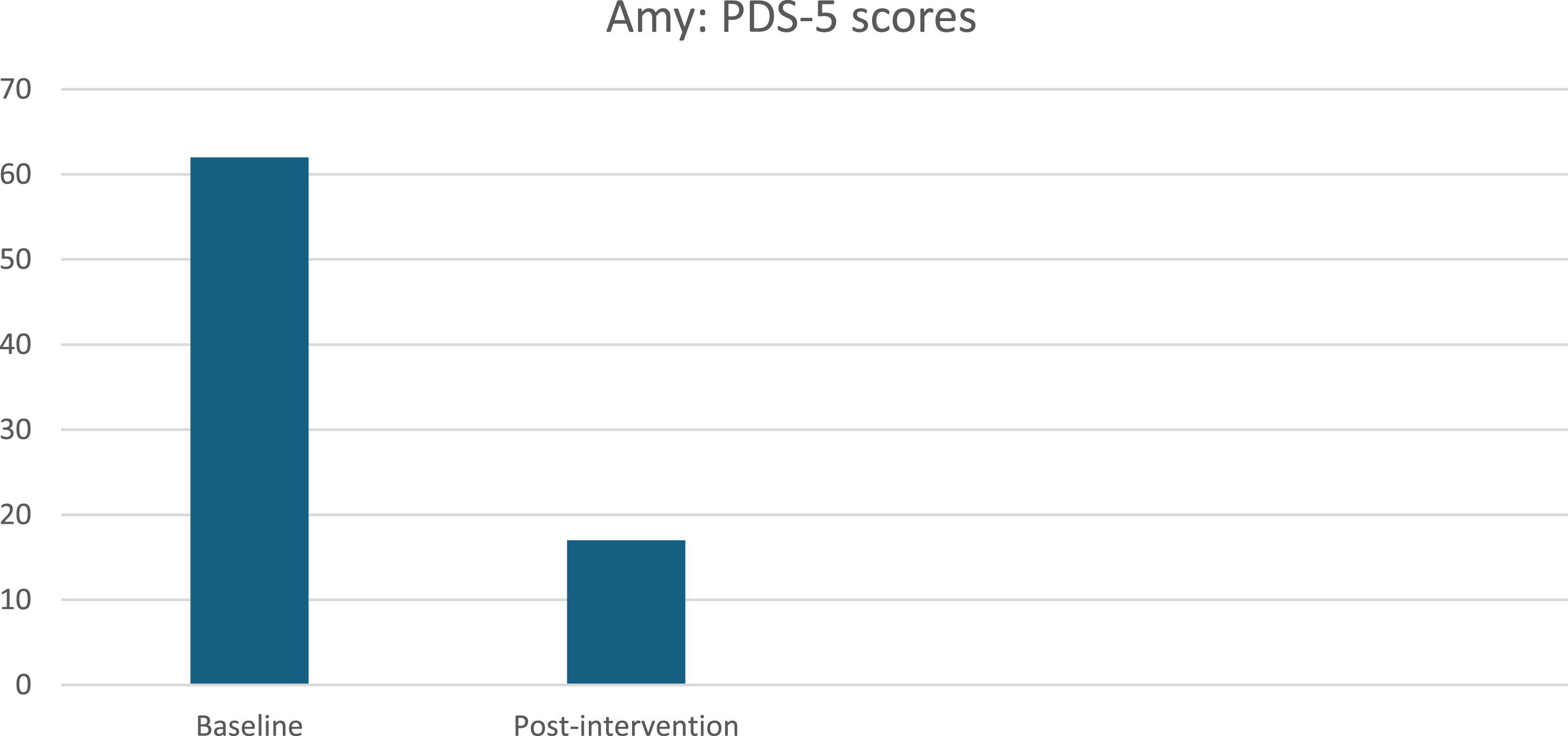
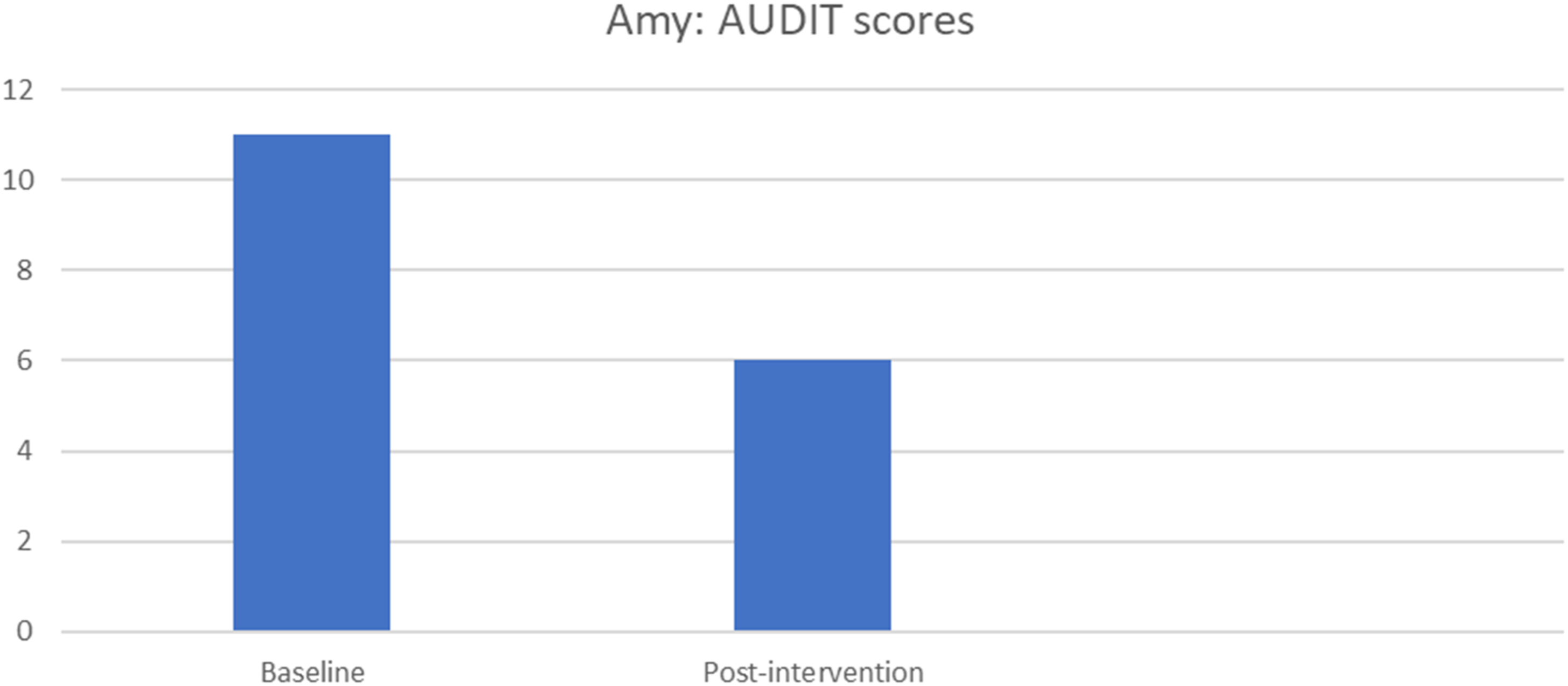
Figure 4 below illustrates Amy’s PCL-5 scores during the intervention across ten sessions. In session one, Amy had a total score of 56, and the clinical cut-off score is 31-33, which indicates a provisional PTSD diagnosis. The participant’s scores decreased over sessions, indicating good treatment outcomes with some fluctuation, due to imaginal exposure and external stressors. At the final session, the participant had a total score of 20. Participants’ PCL-5 Scores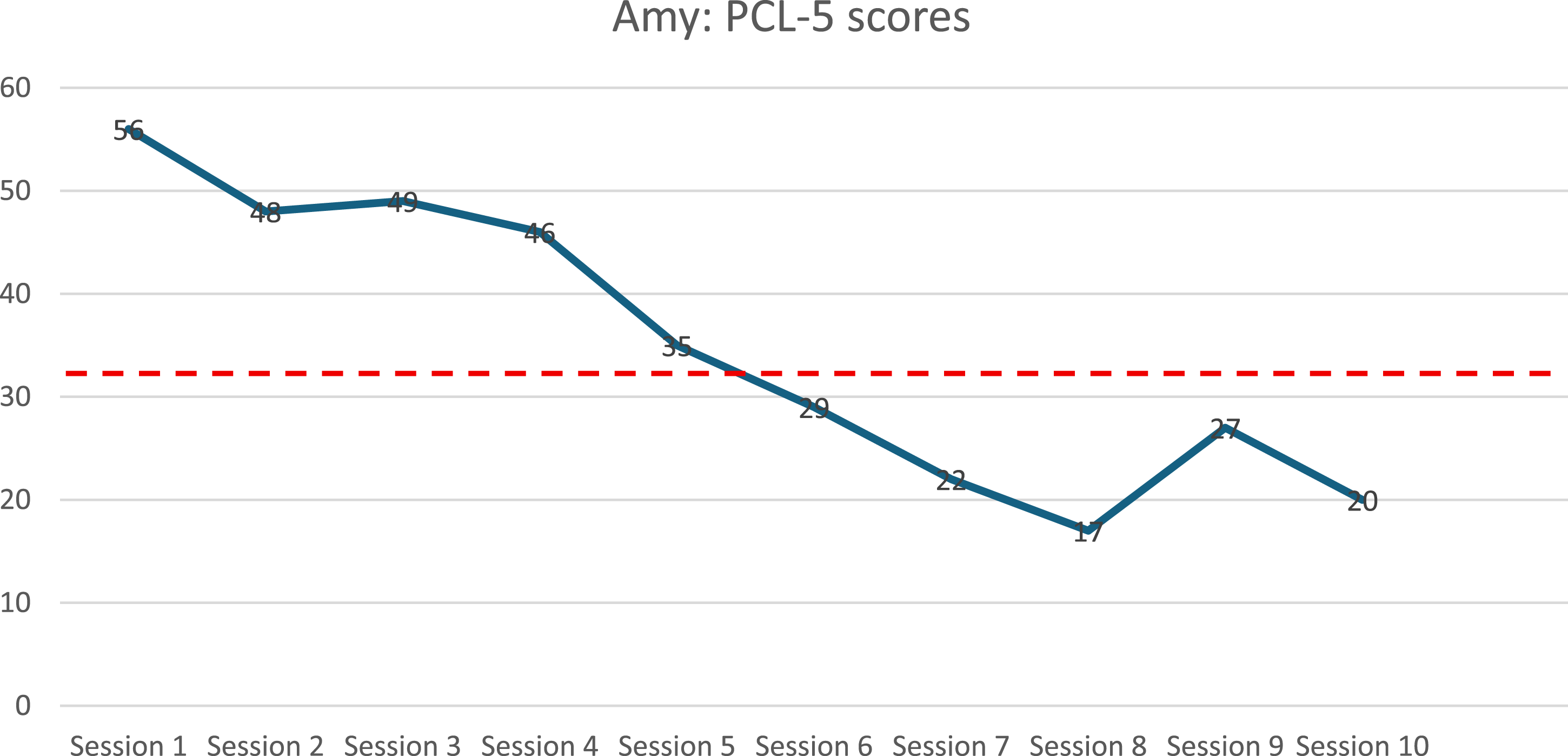
In Figures 1–4, we can see a decrease in Amy’s overall symptomatology on the various assessment measures. In terms of PTSD symptoms, a clear decrease is observed from baseline to post-intervention, as indicated by the CAPS-5, PDS-5 and PCL-5. Moreover, there is also an improvement in terms of alcohol use. Amy presented with hazardous and harmful drinking at baseline, and at post-intervention, her score had decreased, as illustrated by her AUDIT scores in Figure 3.
According to Booysen & Kagee (2020a, 2020b, 2023), research on PE and its feasibility within the South African context is limited. As mentioned, one of the aims of the study is to determine whether university students perceive Massed-PE as a feasible therapy for PTSD and AUD. To determine the feasibility of Massed-PE therapy, Amy completed implementation measures at post-intervention. Implementation measures consisted of three subscales, namely, the Acceptability of Intervention Measure (AIM), Intervention Appropriateness Measure (IAM), and Feasibility of Intervention Measure (FIM) (Weiner et al., 2017). Amy answered questions related to the acceptability, appropriateness, and feasibility of Massed-PE by rating these according to four options: “Completely disagree”; “Disagree”; “Neither agree nor disagree”; “Agree”, or “Completely agree”.
In terms of the AIM of Massed-PE, the participant seemed to deem it an acceptable intervention measure, with the most common response being “Agree” (Figure 5). Thus, it seems that overall, Amy considered Massed-PE to be an acceptable intervention measure, which indicates that a massed or condensed format of trauma-focused therapy, for her, was acceptable. In Figure 6, Amy also indicated that all the responses were “Completely agree”, indicating that she found the intervention to be appropriate. Lastly, in Figure 7, Amy was also requested to answer questions relating to the feasibility of Massed-PE, with most answers indicating “Completely agree”. Thus, in terms of feasibility, Amy was satisfied with Massed-PE as an intervention. Acceptability of Intervention Measure (AIM) Intervention Appropriateness Measure (IAM) Feasibility of Intervention Measure (FIM)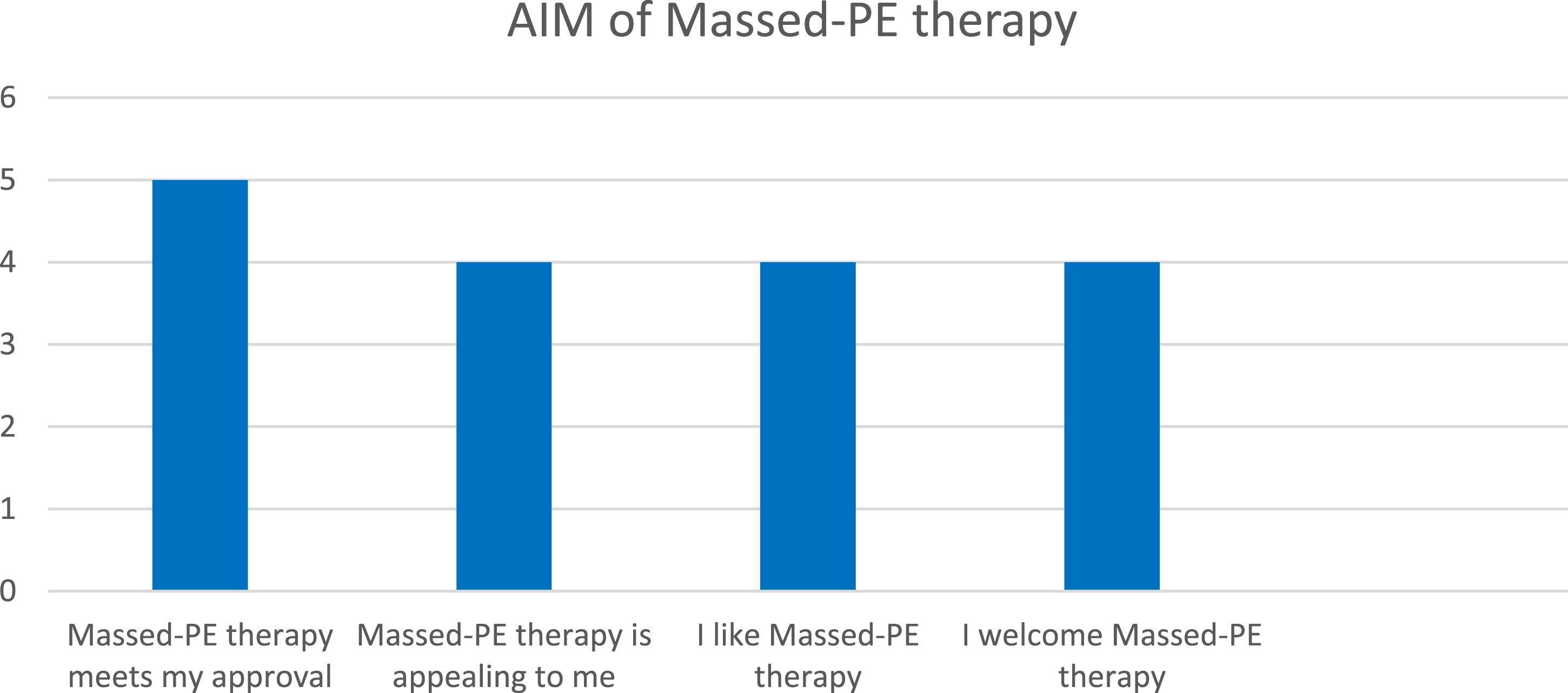
Complicating Factors
The participant had problems with transportation throughout the intervention, which raises the question about the feasibility of in-person massed PE, which requires the participant to attend sessions for consecutive days over a two-week period. The lack of public transport and prevalent socio-economic challenges underscore the importance of considering the contextual realities and structural limitations when delivering PE for PTSD (Booysen, 2024). This scenario underscores broader barriers to mental health services, generally, but also specifically in a university student setting (Bantjes, Kessler, Hunt, et al., 2023).
Access and Barriers to Care
Compared to the complicating factors in the aforementioned section, no significant access or barriers to care were reported or observed during the treatment of Amy.
Follow-Up
Amy was assessed immediately after the completion of the 10-day intervention to ascertain whether symptom improvement occurred from pre-to post-treatment. A further follow-up (i.e., 12-week follow-up) was not feasible due to Amy not being available in town.
Treatment Implications of the Case
We observed a marked improvement in PTSD symptoms on the CAPS-5 (60 to 8), PDS-5 (62 to 17), and PCL-5 (56 to 20) over a ten-day period. Similarly, AUDIT outcome scores indicated a significant reduction in risky drinking behaviours, moving from hazardous and harmful drinking levels (baseline = 11) to below the threshold for such categorisation (post-intervention = 6). The study provides preliminary empirical evidence demonstrating the effectiveness of massed PE in reducing symptoms of PTSD and comorbid alcohol use in a university setting in South Africa. Moreover, these findings are in line with similar larger-scale clinical trials and smaller sample intervention studies on the efficacy and effectiveness of massed PE for PTSD (Bonar, 2015; Coffey et al., 2016; Peterson et al., 2023; Sherrill et al., 2022; Zwetzig et al., 2022).
Zwetzig et al. (2022) found that massed PE reduced symptoms in two firefighters, suggesting the potential for similar positive outcomes in other population groups (Zwetzig et al., 2022). In a study by Bonar (2015), two participants at a university counselling centre received PE therapy over ten sessions. The results by Bonar (2015) showed that the first participant’s PCL-5 was initially quite high, 66 at baseline. During the intervention, the participant’s reduction of PCL-5 scores resulted in a final score of 24. The second participant’s PCL-5 score at pre-intervention was 46, resulting in a final score of 23 post-intervention. The second participant had spikes in their PCL-5 scores during intervention; however, as mentioned, this is to be expected with the introduction of imaginal exposure, which may exacerbate PTSD symptoms (Bonar, 2015). In a larger clinical trial, Peterson et al. (2023) found that massed PE was effective for combat-related PTSD, concluding that PE can be adapted into compressed treatment formats that effectively reduce PTSD symptoms (Peterson et al., 2023). According to Peterson et al. (2023), 61% of participants (N = 234) achieved clinically significant reductions in PTSD symptoms, and 74% had self-reported PTSD symptom reductions at the 1-month follow-up assessment.
Further, Coffey et al. (2016) assert that while valuable advances have been made toward the treatment of comorbid PTSD and substance use (See Back et al., 2019), additional research examining the efficacy of PE in comorbid substance use populations is still scarce, specifically examining Massed-PE for PTSD and comorbid AUD. A secondary outcome of the study was to evaluate whether massed PE can also improve comorbid disorders such as AUD in a university student. Coffey et al. (2016) implemented a modified PE protocol, consisting of 9-12, 60-min sessions for individuals with PTSD and comorbid substance use. At post-intervention, participants achieved 85.7%-97.9% days’ abstinence at follow-up (Coffey et al., 2016). Baker et al. (2011), in a clinical case study, found that 12 sessions of PE in a male participant with abortion-related PTSD and alcohol use dependence had good outcomes on the Impact Events Scale-Revised scale from pre-to post-treatment (46 to 6), and maintained abstinence from alcohol and illicit drug use three months after treatment. Doerfler and Twigden (2022) found that PE had positive outcomes in a Latino male with a polysubstance history and homelessness. At the end of 16 sessions, had a significant improvement for PTSD from pre-to-post on PCL (72 to 3), and similar for depression on the Beck Depression Inventory (BDI) (30 to 3). These outcomes were maintained at a 1-year follow-up for both PTSD (PCL = 3) and depression (BDI = 2).
Our study also highlights the importance of reconsidering treatment formats in university settings from the traditional once-a-week model of individual or group formats, to a variety of formats such as accelerated treatments for PTSD in university settings. Bonar (2015) argues that clinical staff at university counselling centres are often advised to work within a brief therapy model, focusing on containment and support. However, students with PTSD symptoms require more specialised treatment, given the nature of their symptoms (Bonar, 2015). Notwithstanding the complexity of treating PTSD and the workload of university counselling centres, the integration of brief and intense treatments such as massed PE may provide novel treatment formats, among others, that can offset some of the barriers to efficiency in counselling centres.
Moreover, one of the critical advantages of MASSED PE therapy is its potential for rapid symptom reduction (Dell et al., 2023), particularly the low rates of dropout, with that of the MASSED PE group (4.8%), 3.5 times less than the standard PE format (16.9%). This advantage is particularly valuable in the context of university counselling centres, which often struggle with resource limitations and where the demand for mental health services has significantly increased over the years, placing a considerable burden on counselling centres (Pedrelli et al., 2015; Watkins et al., 2012). Given that universities are responsible for developing suitable interventions (Bonar, 2015), massed PE is an evidence-based treatment worth considering in university mental health services for students with PTSD and comorbid AUD. Furthermore, research should also consider the balance between workload in counselling centres, as intensive treatment may not reduce the burden of workload but may increase efficiency in client access and completion of treatment. Yet further consideration may be needed to better understand how other workload and organisation factors may impact the overall mental health services of counselling centres.
This study also evaluated massed PE’s acceptability, appropriateness and feasibility through the participants’ experience and perception of the intervention. Utilising implementation measures, the findings suggest that Amy experienced and perceived massed PE as feasible, acceptable, and appropriate. This positive reception underscores the potential of massed PE for broader application in clinical settings targeting PTSD and comorbid AUD among university students. Sherrill et al. (2022) assessed participants’ perceptions post-intervention through a written survey that utilised open-ended questions. Their study revealed a predominantly positive reaction (51.27%) towards massed PE, highlighting benefits that resonate with the therapy’s underlying rationale; the structured approach minimises distractions and avoidance, while rapid improvements boost motivation and engagement (Sherrill et al., 2022). According to Sherrill et al. (2022), although participants noted short-term discomfort and a high demand for their time and effort, these aspects were anticipated based on the clinical theory underpinning PE and its massed delivery format. Hence, these findings corroborate the notion that despite its challenges, the intensity of Massed-PE is both appreciated and beneficial from the participant’s perspective (Sherrill et al., 2022).
Our results contribute to the growing literature on intensive trauma-focused psychotherapies by offering new insights into the application of MASSED PE within a university setting. By demonstrating the preliminary effectiveness and acceptability of Massed-PE for PTSD and comorbid AUD, this study lays the groundwork for future research to explore its implementation and potential impact across similar settings.
Recommendations to Clinicians and Students
In South African society, including university settings, trauma exposure and PTSD are highly prevalent among university students (Bantjes, Kessler, Lochner, et al., 2023). Accelerated formats of treatment provide an opportunity to mitigate several implementation (i.e., lengthy treatment processes) and treatment limitations (i.e., dropout). University students are considered a crucial factor in the socio-economic development of a nation, which requires that university students have access to the necessary academic but also psychological services to increase the likelihood of academic completion and quality of life. Our case study provides an initial step toward further research and the possible adoption of massed interventions for PTSD among university students. Furthermore, university mental health services can benefit from providing not only a range of treatment modalities but also a variety of treatment formats, such as spaced and massed treatments for PTSD. Considering the increased utility of internet-based access to PE in university settings, massed PE can be implemented on online platforms, too (Booysen & Slabbert, 2025). Furthermore, the implementation of COPE, which was not part of the current study, in an accelerated format can also be considered to further increase effective treatment of PTSD and AUD among university students in South African universities.
Notwithstanding the promise of accelerated treatment formats such as Massed-PE, the feasibility of implementing PE (spaced or massed) within the given resources still faces barriers ranging from a lack of training, supervision, and certification in PE to broader systemic and structural barriers such as increased levels of poverty and mental health literacy, which prevent persons from accessing care in South Africa (Booysen et al., 2024). In our study, Massed-PE had good feasibility, acceptability, and appropriateness due to the scale and size of the university setting, which is a small town-university, which made attending sessions easier compared to larger institutions or cities. Amy was a graduate student and had adequate mental health literacy to seek treatment, yet the same cannot be inferred about the broader social context, which may be a notable barrier to seeking treatment for PTSD. Lastly, due to the novelty of accelerated treatments such as MASSED-PE in South Africa and other LMICs, the concept of intensive treatments can be the most notable barrier among clinicians and clients to seeking and adopting accelerated treatments.
Notwithstanding the notable systemic barriers to treatment for PTSD, the study suggests that MASSED-PE is an effective and acceptable treatment for PTSD in a university context, which can be a catalyst towards more effective and efficient care for students living with PTSD.
Footnotes
Acknowledgements
We thank “Amy” for participating in this study and for the financial support of the National Research Foundation (ZA).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the National Research Foundation (ZA) Grant.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.