
Abstract
Emergency and critical care personnel face a heightened risk of occupational trauma exposure. Practitioners lack clear guidance on how to support individuals who are off work with work-related posttraumatic stress disorder (PTSD), particularly those receiving treatment in the context of a claim with a workers’ compensation board. While trauma-focused psychotherapies are recommended as first-line interventions for PTSD, there is an ongoing discourse about how to address the increased functional impairments of individuals who are off work, and how to best support individuals struggling with in-vivo exposures and return to work. This article utilizes case studies involving an intensive care unit nurse and an emergency dispatcher, to demonstrate how occupational therapists can collaborate with psychotherapists to address functional impairment following workplace trauma to support clients in their mental health recovery and return to the workplace. Beyond the traditional focus on non-trauma-related treatment domains, occupational therapists are uniquely positioned to address trauma-focused aspects of therapy. Strengthening the partnership between occupational therapists and psychotherapists has the potential to improve treatment outcomes, promote work reintegration, and provide comprehensive and holistic care that addresses the clients’ full spectrum of needs.
Keywords
1 Theoretical and Research Basis for Treatment
Posttraumatic stress disorder (PTSD) is a mental health condition that can manifest after exposure to a traumatic stressor involving actual or threatened death, serious injury, or sexual violence. Trauma exposure can occur through directly experiencing the event, witnessing it happening to someone else, learning that it has occurred to a close person, or through repeated or extreme indirect exposure to traumatic events in the course of professional duties (American Psychiatric Association, 2022). It is estimated that about 4% of the world’s general population have PTSD (Koenen et al., 2017). Emergency and critical care workers face a particularly high likelihood of trauma exposure due to the nature of their work, leading to an elevated susceptibility to work-related PTSD. For example, in a survey among various first responder groups, participants reported having responded to an average of 11 different types of potentially traumatic events, including disasters, fires, serious accidents, deaths, and physical and sexual assaults (Carleton et al., 2019), and 23% screened positive for current PTSD (Carleton et al., 2018). Similarly, among intensive care nurses about 18% exhibited positive PTSD screening results (Cho & Kang, 2017). These prevalence statistics highlight the need to explore unique treatment considerations for these groups.
Evidence-based clinical practice guidelines recommend trauma-focused psychotherapies as first-line interventions for PTSD (Hamblen et al., 2019), including prolonged exposure (Foa et al., 2019), cognitive processing therapy (Resick et al., 2016), cognitive therapy for PTSD (Ehlers et al., 2005), and eye movement desensitization and reprocessing (EMDR; Shapiro, 2018). The interventions differ in various ways in their theoretical models, specific treatment components, and assumed mechanisms of change, but there is also a high degree of overlap between them. The central idea of their underlying models is that there is something special about the way the traumatic event is represented in memory, and that failure to process the experience in an appropriate way will result in involuntary reexperiencing of the trauma, excessive emotional responses to current trauma reminders, persistent negative feelings and cognitions, and maladaptive coping and avoidance behaviours.
Typical components of evidence-based PTSD treatment protocols are psychoeducation, coping skills building, trauma processing, and in-vivo exposure to feared and avoided situations. Traditionally, these interventions are provided by a psychotherapist (e.g., psychologist or counsellor). However, there is an ongoing discourse about their limitations that requires attention in order to advance therapy development. Notably, trauma survivors tend to present with extensive functional impairments in interpersonal and occupational domains, reduced personal satisfaction and poor quality of life (Bryant et al., 2023). Thus, criticism has been directed at the existing interventions’ narrow focus on symptom reduction, overlooking how clients can regain purpose, connection, enjoyment, and a sense of self beyond the mental health problems (Yehuda & Hoge, 2016). Also, while it is recommended that clients complete in-vivo exposures to feared and avoided situations between sessions (e.g., Foa et al., 2019), there is little guidance on how therapists can assist individuals who struggle with exposure assignments. Finally, individuals who are off work due to occupational trauma exposure face some unique challenges. For example, a key symptom of PTSD involves intense emotional reactions to, and avoidance of, reminders of the traumatic event. This can make it especially difficult for them to return to the work environment. Extended time away from work may lead to increased functional impairments and avoidance due to the lack of structure, routine, purpose and social interactions, and decreased necessity to leave the house. Consistent with this, studies have shown that unemployment following a traumatic event predicted persistence of PTSD symptoms (Nandi et al., 2004), and that re-employment was associated with subsequent mental health improvement (Hoare & Machin, 2010). However, most treatment manuals lack directives on facilitating the return-to-work process for individuals with work-related PTSD (Torchalla & Strehlau, 2018).
The current article proposes that these shortcomings can be addressed by using an interdisciplinary approach to treatment, where occupational therapists play a unique role in the client’s recovery, due to their specific skills and focus on function and occupation. In the mental health realm, occupational therapy focuses on treating the repercussions of mental illness as they impact the ability to complete daily activities, by assisting clients with restoring function in self-care, productivity and leisure (Kirsh et al., 2019). In a review of the literature, Edgelow and Cramm noted a lack of formalized occupational therapy guidelines for individuals with PTSD, and proposed that occupational therapists contribute to treatment by providing education, establishing routine, structure and activity, and teaching self-regulation techniques (Edgelow & Cramm, 2020). We suggest that by collaborating with psychotherapists, occupational therapists can address trauma-focused aspects of the intervention as well, thus contributing to more comprehensive and holistic treatment. Occupational therapists can support individuals with PTSD in finding purpose, enjoyment, and connection by using value- and strength-based interventions to eliminate barriers towards engagement in meaningful, pleasurable and productive occupations. In addition, they are unique in their ability to conduct treatment outside of the clinical setting, such as in clients’ homes, workplaces, and communities; thus, supporting individuals who struggle to complete in-vivo exposures independently. Lastly, occupational therapists are experts in the realm of return to work and can identify return-to-work barriers, provide interventions to improve return-to-work readiness, facilitate return-to-work planning, and support individuals during a return-to-work attempt. The current paper utilizes two case studies to demonstrate how occupational therapists and psychotherapists can effectively collaborate to support clients with work-related PTSD in their mental health recovery and return to work.
Interdisciplinary Treatment
The article describes the treatment of two injured workers, a nurse working in the intensive care unit (ICU) and an emergency dispatcher (John and Montana, both names are pseudonyms), who had been diagnosed with work-related PTSD and been referred to an interdisciplinary trauma recovery program by the workers’ compensation board. In this program, each client works with a team consisting of an occupational therapist and a psychologist, who collaborate to set treatment goals with the client, share resources and responsibilities, make recommendations, and provide comprehensive trauma-focused therapy by working on different aspects of the recovery. The treatment is time-limited (about 12–16 weeks long) but intensive with two occupational therapy and two psychology sessions per week. Following treatment, clients participate in a gradual return-to-work plan, or are discharged with recommendations for work-related restrictions to move forward with vocational rehabilitation or further treatment.
At the beginning of the program, both clinicians will complete an assessment using interviews and psychometric scales, to determine the client’s current state and needs. During the interviews, the occupational therapist focuses on identifying the client’s functional limitations through review of treatment goals and occupational performance issues, whereas the psychologist focuses on identifying mental health symptoms and risk factors. An initial joint session will be held where the team members review the treatment plan and treatment options with the client, explain their roles, and address any questions and concerns the client might have. Although subsequent sessions will usually be held separately, joint meetings are offered at the request of the client or when deemed helpful by the therapists; to review progress, discuss concerns or troubleshoot any barriers that arise. The clinicians continue to maintain close communication throughout treatment while performing discrete yet complementary roles. While both team members provide psychoeducation, they vary in their foci; while the psychologist explains common reactions to trauma from a neurophysiological understanding, the occupational therapist reviews the functional limitations associated with trauma-related symptoms. The psychologist introduces coping skills during office-based sessions, while the occupational therapist supports the integration of these skills through practice with the client during community outings. For the remainder of the program, the psychologist will focus primarily on trauma processing, whereas the occupational therapist works with the client on re-engaging in leisure, social and productive activities before progressing to in-vivo exposure to feared and avoided situations. Collaboration between the clinicians occurs through formal discussion during weekly case conferences as well as informal conversations between sessions. During these consultations it is not uncommon for either provider to request the other’s support emphasizing a particular education component, reinforcing the importance of a treatment recommendation, or addressing functional or psychological concerns identified within sessions. This supports client progress by ensuring that they receive cohesive messaging and integrated treatment throughout their program. The collaboration also ensures that each provider maintains within their scope of practice, by eliciting the support of the other team member when required.
Return to work is primarily addressed by the occupational therapist, who may accompany the client to the workplace, create a gradual return-to-work (GRTW) plan with the client, communicate with the employer, and meet with the client throughout their GRTW. However, the decision to initiate return-to-work planning is made in consultation with the psychologist. In addition to informing return-to-work readiness, consultation with the psychologist can assist the occupational therapist with identifying appropriate work duties and overcoming return-to-work barriers. This could include reviewing coping skills and communication strategies, challenging unhelpful beliefs, normalizing anticipatory anxiety, processing difficult or unforeseen circumstances, and managing setbacks. Upon conclusion of the GRTW plan, the team will work together to determine work-related restrictions based on a review of the client’s self-report and psychometric testing (as ascertained by the psychologist) and objective information and functional abilities (as ascertained by the occupational therapist through observation and collection of collateral information).
2 Case Introduction
John is a white male who worked as the lead nurse in the intensive care unit. He had been exposed to many deaths and other difficult events during his career. He was most distressed by working with an indigenous pregnant woman, who was determined to be brain-dead after a drug overdose when she started having a spontaneous abortion. Both the woman and the baby did not survive the delivery.
Montana is a white female who worked as an emergency dispatcher. She had been exposed to numerous challenging calls during her career, but was most distressed by a recent call from a woman who was raped.
3 Presenting Complaints
John
At the time of his intake, John had been off work for five months. He reported having frequent intrusive memories of various work events, and feeling emotionally distraught and having physical reactions when confronted with work-related reminders. He avoided talking or thinking about work and engaging with anything work-related. He endorsed sleep problems, increased irritability and anxiety, feeling jumpy, on edge and easily startled, and having difficulty concentrating. He felt emotionally labile and avoided engaging with emotionally intense events (e.g., sad movies). He spent his days doing chores and puttering around the house, but often felt fatigued and overwhelmed and sometimes found himself “spaced out” for hours. He did not like being around people and had withdrawn from previously enjoyed activities. John endorsed passive thoughts of death (e.g., “I wish I wouldn’t wake up in the morning”) nearly every day. He denied having active suicidal ideation or having ever made a suicide attempt in his life.
Montana
At the time of her intake, Montana had been off work for seven months. She kept picturing the rape in her imagination, and replaying the call in her mind to identify what she could have done differently to help the victim. She had nightmares of the call and reported feeling unsafe, irritable, and constantly on guard. She had strong physical reactions when confronted with anything that reminded her of work, and had isolated herself socially. She did not go out unless she had to, avoided situations she perceived as distressing such as busy environments or being in crowds, and had discontinued activities she used to enjoy. She felt easily overwhelmed by everyday tasks and reported daily alcohol consumption.
4 History
John
John noted that in addition to experiencing specific traumatic events with patients that accumulated over time, the opioid epidemic and the COVID-19 pandemic had presented chronic stressors in previous years, in terms of workload, understaffing, and fear amongst staff of acquiring COVID-19. Over time, this left him with increasing exhaustion and a sense of having nothing left to give. John began experiencing suicidal ideation about three years ago, although he felt that he had been supressing symptoms for longer. In the following years, he became increasingly symptomatic and had greater difficulty functioning at work and at home. His doctor prescribed him antidepressants and he participated in several sessions with the employee assistance program, supportive counselling with a community counsellor, and EMDR with a psychologist. However, his symptoms and suicidal thoughts intensified over time, and he realized he could not continue working.
Montana
Montana shared that the rape she had to dispatch had striking similarities with a rape that she had suffered herself years ago. It also activated her memories of extensive experiences of childhood sexual abuse. For most of her life, she had tried to avoid memories, thoughts, and feelings related to her own abuse, and she had never received any therapy. Despite her history, she had been functional and had worked throughout her adult life.
5 Assessment
PTSD symptoms were assessed using the PTSD Checklist for DSM-5 (PCL-5; Weathers et al., 2013), a self-report measure assessing symptom severity on 20 items, using a 5-point scale. This results in a summary score between 0 and 80. A cut-off score of 31–33 points is indicative of a probable PTSD diagnosis. Studies identifying the reliable change index for the PCL-5 suggest that a change in scores between 9 and 12 points reflects reliable and clinically significant change (i.e., not due to measurement error) over time (Blanchard et al., 2023).
Depressive symptoms were assessed using the Patient Health Questionnaire (PHQ-9; Kroenke & Spitzer, 2002), a self-report measure assessing the severity of depression on 9 items using a 4-point scale. This results in a summary score between 0 and 27, reflecting minimal, mild, moderate, moderately-severe, and severe symptomatology. A cut-off score of >9 is recommended for detecting clinically significant depression. Studies identifying the reliable change index for the PHQ-9 suggest that a change of 5 points reflects reliable and clinically significant change (McMillan et al., 2010).
The Inventory of Psychosocial Functioning (IPF; Bovin et al., 2018) is an 80-item measure to assess difficulties in functioning in seven life domains (romantic relationship, family, work, friendship/socializing, parenting, education, and self-care) using a 7-point scale. The responses yield an index of functioning from 0–100 for each domain, reflecting no (0–10), mild (11–30), moderate (31–50), severe (51–80), and extreme (81–100) impairment.
John’s Assessment Measures.
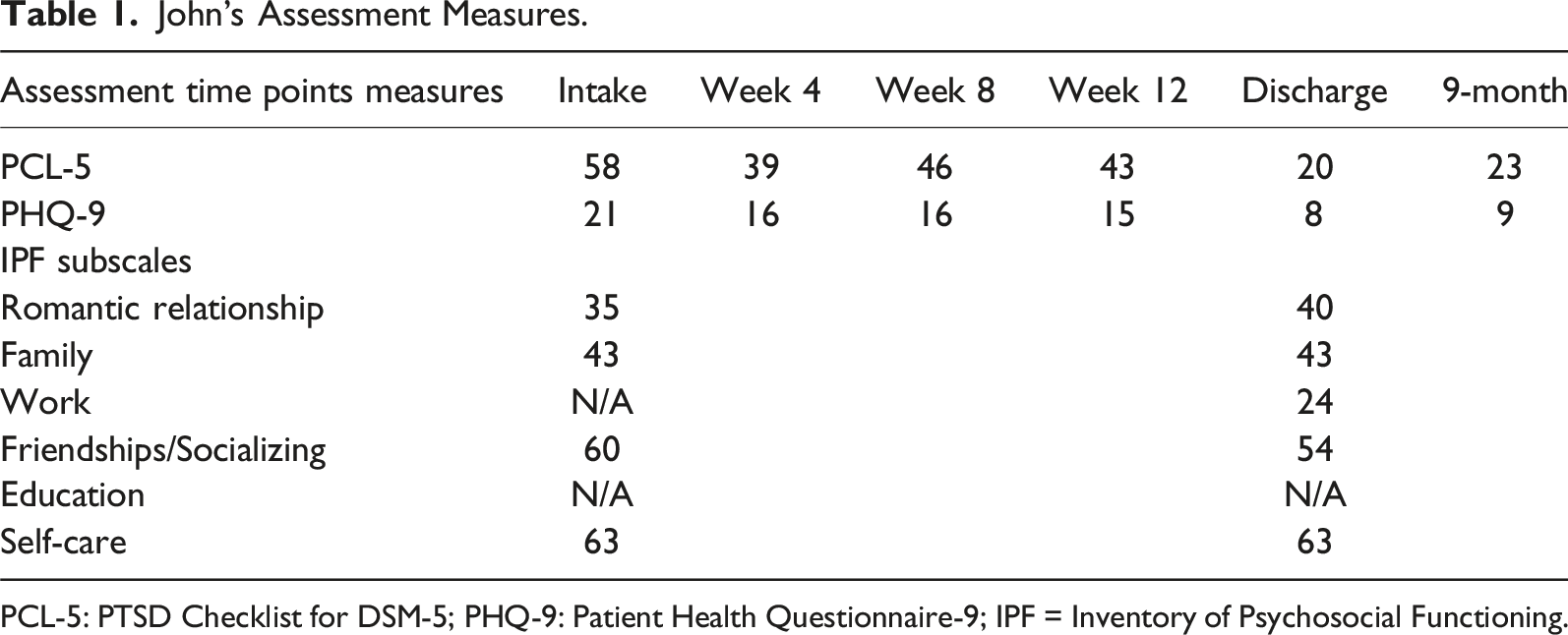
PCL-5: PTSD Checklist for DSM-5; PHQ-9: Patient Health Questionnaire-9; IPF = Inventory of Psychosocial Functioning.
Montana’s Assessment Measures.
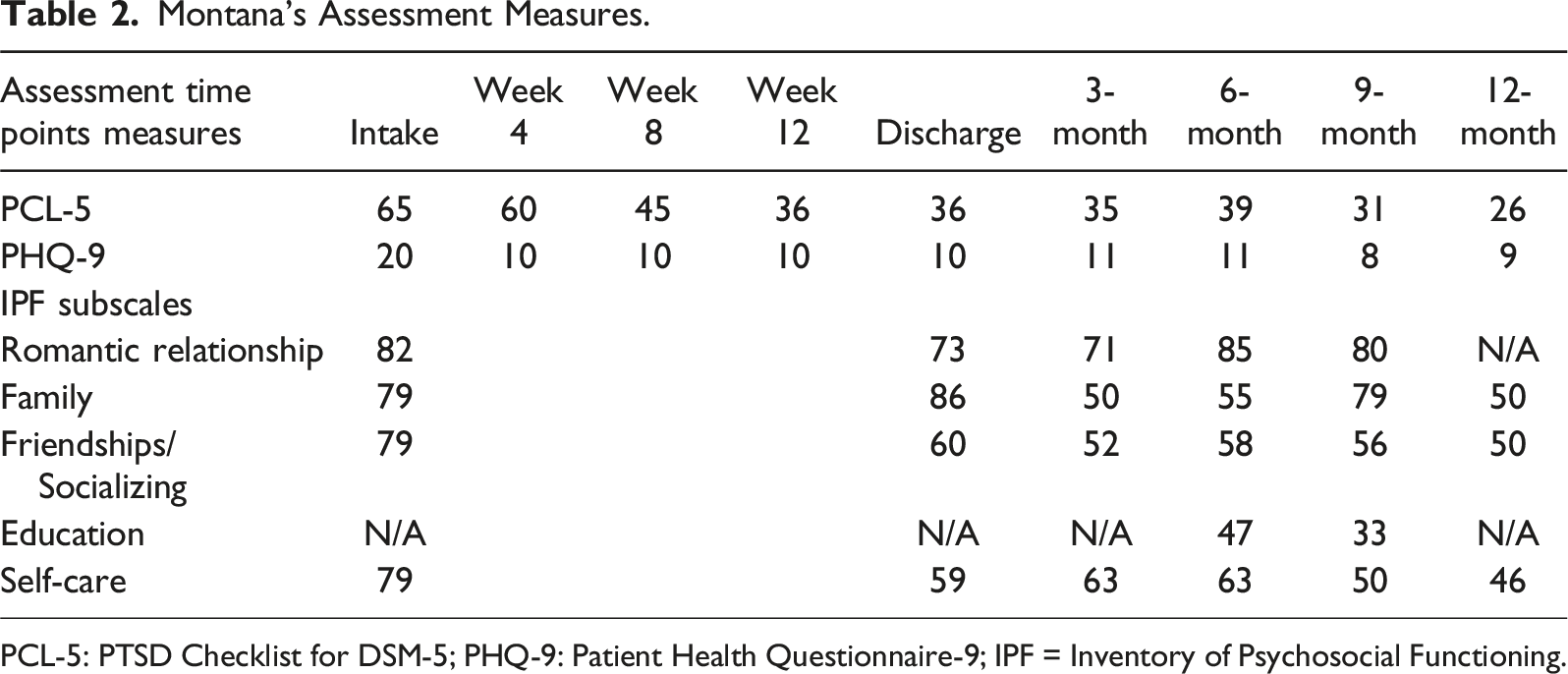
PCL-5: PTSD Checklist for DSM-5; PHQ-9: Patient Health Questionnaire-9; IPF = Inventory of Psychosocial Functioning.
6 Case Conceptualization
John’s Case Conceptualization
A shared decision making approach is recommended for PTSD treatment, where clients and clinicians review evidence-based treatments together to determine which intervention best meets the client’s needs and preferences (Hamblen et al., 2019). John chose the Prolonged Exposure (PE) protocol. PE includes psychoeducation, breathing retraining, in-vivo exposure, and imaginal exposure and processing. In-vivo exposure involves creating a hierarchy of feared and avoided but realistically safe situations, and approaching them gradually without escaping or using safety behaviours. During imaginal exposure, the individual revisits the trauma memory in their imagination and describes it aloud repeatedly, in detail and for prolonged periods of time to the therapist. Processing involves discussing the person’s trauma-related thoughts and feelings. The sessions are audio-recorded, and clients listen to the recordings between sessions. A Subjective Units of Distress Scale is used during exposures, in which the individual rates their current level of distress on a scale from 0 to 100. According to the PE protocol, most sessions are spent with completing imaginal exposure and processing, whereas in-vivo exposures are assigned to the client as homework activities. This protocol lends itself well to interdisciplinary collaboration; within the program, imaginal exposure and processing is delivered by the psychologist, while in-vivo exposure is delivered by the occupational therapist as a means of improving client functioning.
The foundation of PE is emotional processing theory (Rauch & Foa, 2006), and John’s symptoms can be understood within this framework. The theory posits that fear is represented in memory as a cognitive structure (the “fear structure”) which includes information about fear-related stimuli, the person’s responses to the stimuli, and the meaning associated with the stimuli and responses. The fear structure can be adaptive and can trigger appropriate responses, such as preparing equipment and engaging in interventions in case of a cardiac arrest. Due to cumulative unprocessed traumatic work events, John’s fear structure included numerous distressing representations of sensory stimuli such as the sight of patients dying, the smell of blood, and the sound of family members crying; representations of his responses such as rapid heartbeat, sweating and muscle tension; and associated meanings such as the sight of any patient as a sign of ‘impending suffering and death’ and the meaning of his physiological sensations as ‘I am afraid and incompetent’. His fear structure became more problematic when his responses began to interfere with his daily functioning (e.g., having a freeze response during patient care, or having intense reactions in safe day-to-day situations such as watching a sad movie), and later resulted in avoidance of work-related stimuli, which in turn maintained his negative feelings and beliefs and other PTSD symptoms. Although emotional processing theory was initially developed for fear-based trauma, the core concept of a memory structure that involves maladaptive associations between stimuli, responses, and meanings and promotes avoidance when activated can be applied to any type of emotion. In John’s case, the distressing stimuli (e.g., patients dying) became erroneously associated with meanings such as “I failed the patient and their family” and “I can’t bear their suffering.” These meaning elements evoked feelings of guilt, shame and sadness that promoted cognitive and behavioural avoidance, which in turn maintained his negative feelings and beliefs. The avoidance was initially specific to hospital-related memories and places, but generalized over time (e.g., avoidance of social or community events where conversations could potentially lead to work-related topics). In PE for non-fear related emotions, imaginal and in-vivo exposure serve the same purpose of processing the traumatic experience by activating the memory structure and integrating new information. Such information may include new experiences with allowing difficult feelings (e.g., I can handle sad feelings; the sadness passes if I do not avoid it), or altered interpretation of an event (e.g., Their death was not my fault) after placing it in its context. Consistent with this case conceptualization, research has shown that PE can effectively ameliorate a wide range of trauma-related emotional sequelae, including guilt, shame, anger, sadness, moral injury, and emotion dysregulation (Ragsdale et al., 2020).
Montana’s Case Conceptualization
Montana chose EMDR for trauma processing, and in-vivo exposure to address her avoidance behaviours. EMDR consists of eight phases, including history taking and treatment planning; preparation (psychoeducation and coping skills building); assessment (identifying aspects of the trauma memory required for desensitization); desensitization; installation; body scan; closure; and re-evaluation. During desensitization, the individual focuses on disturbing aspects of the memory (the trauma-related image, negative belief, emotions and body sensations), while simultaneously engaging in “bilateral stimulation” which most commonly involves tracking the therapist’s hand with their eyes as it moves back and forth across their visual field. It is assumed that this facilitates integration of adaptive information into the trauma memory. Clients briefly report on their experience in between sets of bilateral stimulation. This procedure is repeated until the memory no longer generates distress. During installation, a more adaptive belief about the self is linked to the newly resolved memory. During the body scan, the individual holds the positive belief and what remains of the trauma memory in their mind, as they scan their body for sensations. The closure phase ends each session with a reflection on insights and application of coping techniques. Re-evaluation is used to identify changes that have occurred in the client’s life and memory. EMDR addresses avoidance behaviours by inquiring about them during re-evaluation and by targeting “present triggers” (e.g., avoided situations) during desensitization, but there is little guidance on how therapists can assist individuals who continue to avoid situations and activities. However, the protocol lends itself well to interdisciplinary collaboration; trauma processing is delivered by the psychologist following the EMDR manual, and an in-vivo exposure component to feared and avoided situations and present triggers was added to be delivered by the occupational therapist.
The foundational framework for EMDR is the adaptive information processing model (Solomon & Shapiro, 2008). It posits that the brain has an inherent ability to process disturbing experiences and integrate them into adaptive memory networks. When distressing events are too overwhelming and not adequately processed, they become stored in a state-specific form, “frozen” in time and in their own neural networks, and unable to connect with other memory networks that hold more adaptive information. The unprocessed memories carry a high emotional charge and can be triggered by a variety of stimuli in the present, resulting in maladaptive emotional, cognitive and behavioural responses and PTSD symptoms. During history taking and treatment planning, Montana reported memories of being sexually and physically assaulted by her ex-partner and being sexually abused by several males throughout her childhood and adolescence. She noted that nobody had supported her at the time and she had never talked about the abuse with anyone. She was ashamed and disgusted with herself, reported feeling worthless and permanently damaged, and never felt totally safe. Working as an emergency responder kept these feelings at bay, and gave her a sense of control and a sense that she could prevent or ameliorate bad things happening to others. However, her past memories continued to play in her mind vividly like movies that could not be stopped once they had started. For most of her life she had been able to push them away, but the rape she had to dispatch was too similar to her personal experiences and activated her memory network related to the abuse. From an EMDR-informed perspective, Montana’s symptoms stemmed from unprocessed experiences of extensive childhood sexual abuse; however, she felt that addressing them directly would be overwhelming and she chose the call as the target for desensitization.
7 Course of Treatment and Assessment of Progress
John’s Treatment and Progress
Reactivation
Both clinicians provided education and coping skills training. When the occupational therapist reviewed John’s activity levels, he reported reduced socialization, limited engagement in enjoyable activity and exercise, and frequent procrastination of chores. Fatigue, reduced interest, low motivation, and avoidance were identified as barriers towards increased engagement. John struggled with creating a list of previously enjoyed activities at home, and with adhering to his goal of doing something enjoyable and meaningful every day. Thus, the list was created within a session, and the occupational therapist utilized education, goal setting, and activity planning to support him with follow-through, until he maintained his activity and goal planner independently. He also reported reduced engagement in productive chores and projects, and described a frequent state of overwhelm regarding his large to-do list. The occupational therapist supported John with creating a system of organization and prioritization, which was developed within session and subsequently maintained by John independently.
Trauma processing
focused on John’s experiences with the indigenous pregnant woman. He had disturbing memories of the woman dying and her brother holding the dead baby, and believed that he had failed to save the patient’s life and had let her family down. He struggled with feelings of guilt, sadness, grief, helplessness and moral distress, and had strong urges to cry which he tried to suppress. During imaginal exposures, the psychologist prompted him to include increasing levels of detail into the narrative, in order to get in touch with painful emotions, place the event in context, and identify new information that was incompatible with the unhelpful and inaccurate meaning he had attached to the event. John readily engaged in imaginal exposures, but initially struggled with tolerating the intervention. During this time, the psychologist consulted frequently with the occupational therapist who actively supported John with progressing through trauma processing. After completing multiple imaginal exposures, the images were no longer intrusive, his emotional and physical reactions attenuated, and he no longer had nightmares. During processing, after reviewing the variety of factors that had led to the outcome, discussing what John and his staff had done for the patient and her family, and exploring what else could have been done, he experienced a significant decrease in guilt and self-blame, and realized that all family members had been supporting each other and had not needed more staff involvement. He also recognized that he tended to take on his patients’ and their families’ suffering, and strategies for maintaining his compassion while retaining a sense of the self-other boundary were discussed. John frequently ruminated about the health inequities that indigenous communities face. In acknowledging his anger and sadness as understandable reactions given the racial injustice prevalent in society and his own values related to ethical practices, he moved towards acceptance of these moral-driven emotions, and reflected on what he could do to address these issues (e.g., promote a supportive culture on the unit, discuss racial health inequities and their moral and ethical challenges during staff meetings).
In-Vivo Exposure
Concurrently, the occupational therapist reviewed the rationale for in-vivo exposure, and created a hierarchy of triggering and avoided situations with John. He reported limited difficulty with typical community stressors (e.g., crowded environments), and as such, exposures focused on work-related avoidance. This included environments (his hospital and medical ward), activities (accessing his work email, interacting with colleagues), and job duties (e.g., holding staff meetings). John had not returned to the workplace since the start of the claim, and the occupational therapist met him across the street from his workplace, to assess his tolerance prior to initiating an exposure to the workplace. Upon arrival, he reported feelings of sadness but demonstrated good emotional regulation and symptom tolerance. Upon entering the hospital lobby, John reported fear of encountering colleagues and a desire to leave. The occupational therapist supported him in creating responses for likely interactions and encouraged the use of learned techniques to cope with anxiety. John was approached by two colleagues who expressed interest in how he was doing. He experienced significant discomfort following the exchange, and the occupational therapist pointed out unhelpful thinking patterns and encouraged him to focus on the facts of the conversation, in which his colleagues stated that they were happy to see him and missed him. When considering this, John reported a strong desire to return to work. A second workplace exposure was completed the following week, which progressed to spending time at the lobby on the intensive care unit floor. John reported moderate discomfort in this location which decreased with time. Subsequently, he completed workplace exposures independently. He also completed exposures to meeting with his manager, participating in online staff meetings, and visiting his ward. Each exposure was subsequently reviewed in session to support knowledge acquisition. The occupational therapist provided support for planning the progression of exposures, consulted with the employer to arrange exposures, and supported John in working through ongoing difficulties with avoidance.
Return-to-Work Support
As treatment progressed, John reported strong motivation to return to work. However, he feared that he had lost practical skills and was concerned regarding his ability to tolerate exposure to intense emotions (e.g., grieving families). As such, John and the team brainstormed ideas to increase his confidence and preparedness, such as spending time with colleagues, reviewing workplace protocols and procedures, and completing online learning modules. After 12 weeks in treatment, John reported an improvement of his PTSD and depressive symptomatology although his scores remained in the clinically significant range. Despite this, John and the team believed that he was ready to initiate a GRTW. The psychologist supported him in creating a relapse prevention plan. The occupational therapist spent time with him addressing return-to-work concerns, by completing a strength assessment, discussing strategies to employ his strengths at work and soliciting feedback, providing education regarding the mental health continuum, and creating a wellness plan to identify mental health indicators and actions for maintaining wellbeing. A 12-week GRTW plan was collaboratively created, in which John gradually increased his work hours and duties. The occupational therapist met with him weekly throughout his GRTW, and the psychologist met with him at the beginning and the end of the GRTW. John progressed through his GRTW with limited difficulty. He reported some initial avoidance of specific duties (e.g., patient rounds), but was able to confront these situations after the occupational therapist reviewed education regarding the importance of challenging avoidance. As John neared the end of his GRTW, he reported excellent improvement of his well-being in the workplace but expressed fear regarding his ability to maintain his progress post-discharge. The occupational therapist reviewed the importance of maintaining work-life-balance, prioritizing restorative activity, and following his relapse prevention plan. At the end of his GRTW, John demonstrated the ability to perform full duties. The occupational therapist liaised with the employer who expressed full confidence regarding his return-to-work readiness.
Montana’s Treatment and Progress
Reactivation
Both clinicians provided education and coping skills training at the beginning of the program. Because Montana no longer engaged in previously enjoyed activities and hobbies, the occupational therapist supported her in identifying her values and strengths, creating activity goals, pre-scheduling activities on a weekly planner, and problem-solving barriers to increase follow-through. She gradually increased her engagement in meaningful activities, including socializing, riding her motorbike, journalling, organizing her home, going to church and jazz cafes, and going on walks and hikes. Sessions focusing on pacing and grading activities aided her in re-engaging in regular household chores. The occupational therapist also monitored her alcohol use in collaboration with the psychologist, and over time Montana implemented a healthy diet that involved minimal alcohol consumption.
Trauma Processing
Montana was anxious but motivated to initiate trauma processing. During the preparation phase, the psychologist taught her skills for shifting from a state of distress to a state of calm, observing her inner experiences mindfully without engaging with them, and maintaining dual attention on both past memories and the present moment. The target image was based on information she had obtained during the call-taking. She rated her associated distress (0–10) at a 9. Her negative cognition was that she is worthless and a failure. She identified her desired positive cognition as being valuable and worthy, and rated its current validity at a 2 (on the validity of cognition scale where 1 means a belief feels “completely false” and 7 means it feels “completely true”). The reminder of the program was used for desensitization. Associations that emerged during desensitization were primarily related to Montana’s childhood abuse experiences. She was quite emotional during these sessions but over time her ability to tolerate the memories improved. At the end of the program, she rated her SUDS for the work event at a 3/10, and the validity of her positive cognition as a 6/7. Montana identified the cessation of intrusive memories and nightmares as the most positive outcome of her therapy. In addition, she reported having an improved ability to cope; reduced feelings of guilt, shame and disgust; having a healthier perspective of her life experiences; and feeling no longer overwhelmed by memories and feelings.
In-vivo exposure
After Montana had increased her engagement in meaningful activity, the occupational therapist proceeded to planning in-vivo exposure to feared and avoided situations. An in-vivo exposure hierarchy was created with Montana, which included general situations she found stressful (e.g., crowded locations), as well as work-related reminders. She readily engaged in several community exposures accompanied by the occupational therapist, including going to a large supermarket and a busy mall. When first initiating these exposures, Montana reported and demonstrated hypervigilance, an increased startle response, rapid heartbeat and breathing, sweating, restlessness, nausea, and difficulties concentrating. However, with repetition and through the use of coping skills, these symptoms began to reduce. Over time, she reported reduced avoidance and distress in the community, and feeling more comfortable in louder environments and more confident in social settings. Subsequently, she completed various community exposures independently and treatment progressed to work-related exposures, commencing with going through her work bag and viewing her workplace neighbourhood and building on google maps. She required much support from the occupational therapist before she felt ready to progress to the surrounding area of her workplace. Five exposures to the workplace neighbourhood were then completed. They commenced three blocks away from the building and progressed to being outside the fence of her workplace. All of them were accompanied by the occupational therapist as Montana did not feel able to go on her own. She exhibited ongoing fear and physiological symptoms of distress, difficulty using coping skills independently without prompting, and difficulty walking closer to her workplace building without significant encouragement by the occupational therapist. The occupational therapist regularly evaluated Montana’s distress, supported her in using coping skills, and aided her in challenging unhelpful thoughts and safety behaviours. During in-clinic sessions, the occupational therapist used motivational interventions such as reviewing progress with Montana, discussing the pros and cons of returning versus not returning to the pre-injury position, and aligning exposures with her life goals. Concurrently, the psychologist spent some time reviewing exposure exercises with Montana and practicing additional coping skills. However, although Montana participated in all scheduled exposure sessions, she ultimately felt unable to enter her workplace building.
Return-to-Work Support
Despite multiple exposures to the surrounding area of her workplace, Montana continued to report significant guardedness, emotional distress and concerns about relapsing when talking about the possibility of returning to her pre-incident position or entering her worksite. She had also begun to report high anticipatory anxiety prior to exposures in which she started to feel unsafe driving to the location, as well as difficulties engaging in her daily activities both prior to and after completing exposures. She continued to present with considerable symptomatology during exposures close to the workplace building which did not improve over time. She felt unable to progress with completing any exposures to the interior of her workplace building despite the team’s joined support. Her scores on the psychometric scales improved gradually over time but remained in the clinically significant range at the end of the program (Table 2). In a joint decision-making process with the team, Montana and her case manager at the workers’ compensation board, it was decided to discontinue workplace in-vivo exposures and GRTW planning due to risk of decompensation. It was recommended that she be restricted from an emergency call-taking environment, including active call-taking and dispatch work as well as indirect exposure (e.g., through reports or desk work on an operations floor). Based on her difficulty progressing to exposures into the workplace building, it was also recommended that she be restricted from returning to her pre-injury work location. With these restrictions in place, she felt ready to move on to vocational rehabilitation.
8 Complicating Factors
John
John reported having passive suicidal ideation nearly every day, and navigating trauma processing in the context of suicidality was addressed throughout the program. Because it is typically the trauma-focused treatment components that result in the greatest amount of symptom reduction and because trauma-focused interventions have evidence of both reducing PTSD symptoms and suicidal ideation (Rozek et al., 2022), the team followed clinical practice recommendations for treating PTSD in the context of suicidality, which advise that trauma processing can be initiated without delay for clients who report suicidal ideation without recent intent, plan or behaviours (Holliday et al., 2021), which was the case for John. The imaginal exposure protocol was delivered without modifications and John’s ideations were assessed by the psychologist on a regular basis; they continued to improve over time, and in his third treatment block he no longer reported experiencing these thoughts.
John was highly motivated to participate in therapy, but initially reported difficulty tolerating trauma processing. As the lead nurse, he was used to focusing his attention outwards on his patients and staff, but not on his inner experiences. He was able to recount factual information with little prompting but struggled with accessing, describing and reflecting on his feelings, thoughts, and body sensations. He found the emerging emotions uncomfortable and needed to learn to cope with them in a way that allowed their natural flow to take place. He described feeling exhausted and depressed after these sessions, expressed concerns regarding the treatment’s effectiveness and his ability to engage in trauma processing, and questioned if he should continue with the therapy. He struggled to pace his psychology homework and reported feeling hopeless and like a failure. During this time, the occupational therapist supported him by normalizing symptoms, providing education and encouragement to support treatment engagement, and setting time constraints for homework and planning a restorative activity for afterwards. These sessions often took place immediately following psychology visits and the occupational therapist encouraged engagement in restful activity within session.
Montana
At intake, Montana reported daily alcohol consumption in the evenings, but was motivated to reduce her drinking. During phase 1 of EMDR, her alcohol use was assessed and she kept an alcohol tracking sheet for much of her time in the program. For treatment planning, the team considered evidence suggesting that trauma-focused psychotherapies can be used safely and effectively in individuals with concurrent alcohol use problems (Taylor et al., 2017). Recommendations for the use of EMDR with individuals with substance abuse propose that substance use should be addressed in most phases of the EMDR protocol, and that desensitization can be initiated in clients with minimal or no withdrawal symptoms (Brown et al., 2016). As such, psychoeducation included a discussion of the relationship between PTSD and alcohol use. Using the daily schedule, the occupational therapist worked with her on planning alternative activities to drinking in the evening. Coping skills building included strategies to cope with drinking urges. Relapse prevention planning addressed both PTSD and alcohol. Montana consistently reduced her alcohol consumption without experiencing signs of withdrawal or a worsening of her PTSD or depressive symptoms.
9 Access and Barriers to Care
Psychological workplace injuries such as PTSD can be difficult to navigate, and the time it takes for the workers compensation board to investigate and make a decision on a claim can significantly slow down the worker’s access to care. However, a presumptive clause had recently been added to the Workers Compensation Act, for workers in occupations who are frequently exposed to traumatic events. The list of eligible occupations includes nurses like John and emergency dispatchers like Montana. The presumption provides that if a worker develops a disorder that is recognized as a condition that may arise from trauma exposure, it is presumed to have been due to their work, and there is no longer a need to prove that it is work-related. This fast-tracks the claims process and provides workers faster access to treatment, such as referral to specialized trauma recovery programs. The workers compensation board has contracted multiple clinics to deliver these services, including the current clinic to which both John and Montana were referred to. Following discharge from the program, John returned to his pre-injury job. He subsequently participated in several post-discharge follow-up sessions with the team which were funded by the workers compensation board. In contrast, Montana transitioned to vocational rehabilitation. The psychologist continued to meet with her biweekly throughout this process, which was also funded by the workers compensation board.
10 Follow-Up
John’s psychometric scores are presented in Table 1. At intake, they indicated significant PTSD symptoms, severe depressive symptomatology, and significant functional impairment. His scores slowly improved over time. Three follow-up sessions were completed (including one psychometric reassessment); at all time points John was still at work and feeling well. Using the reliable change score of 10–12 points, his responses on the PCL-5 suggested reliable improvement from intake (58 points) to his 4-week reassessment (39 points). His scores showed no significant change at the 8- and 12-week reassessment and remained above the cut-off for a probable PTSD diagnosis. At the end of his GRTW, his score suggested another reliable improvement compared to his pre-GRTW score which was maintained at the follow-up reassessment; both scores were below the cut-off for a probable PTSD diagnosis (20 and 23 points, respectively). The same pattern was observed for the PHQ-9: Using the reliable change score of 5 points, his responses suggested reliable improvement from intake (21 points, severe depression) to his first 4-week reassessment (16 points, moderately-severe depression). His scores showed no significant change at the 8- and 12-week reassessment and remained in the clinically significant range. At the end of his GRTW, his score suggested another reliable improvement compared to his pre-GRTW score, which was maintained at the follow-up reassessment; both scores were in the non-clinical range and reflected mild depression (8 and 9 points, respectively). At discharge, his IPF scores indicated good functioning at work (mild impairments) but some ongoing impairments in other areas of his life.
Montana was enrolled in a computer skills course as part of her vocational rehabilitation, and early sessions with the psychologist focused on supporting her to meet course demands. Once she felt confident managing her workload, trauma processing following EMDR protocol was resumed, focusing on her own abuse experiences, which led to further symptom improvement. She ultimately enrolled in a diploma program. Her psychometric scores continued to improve during the vocational rehabilitation process (Table 2). Her responses on the PCL-5 suggested reliable improvement after 8 weeks of treatment, but no further significant improvement over the course of her treatment and early follow-up reassessments. However, they continued to decrease slowly and were below the cut-off for a probable PTSD diagnosis at both her 9-month and 12-months follow up (31 and 26 points, respectively). A similar pattern was observed for the PHQ-9: Her responses suggested reliable improvement from intake (20 points, severe depression) to the 8-week reassessment (10 points, moderate depression). There was no further significant change during treatment and the early follow-up reassessments; however, her scores subsequently improved slightly and were in the non-clinical range at both the 9- and 12-month reassessment (8 and 9 points, respectively) and reflected mild depression. Her final IPF scores indicated some improvement of her functioning over time, although suggested ongoing impairments in all life domains measured.
11 Treatment Implications
Intensive PTSD treatments have gained increasing empirical support for reducing trauma-related symptoms (Sciarrino et al., 2020). Through two case studies, this report delineates the use of intensive treatment through interdisciplinary collaboration between occupational therapists and psychologists, to deliver both trauma-focused therapy and return-to-work support for individuals with work-related PTSD. Edgelow and Cramm (2020) proposed in their Occupational Therapy Trauma Intervention Framework that occupational therapists contribute to treatment by working on non-trauma-focused domains, establishing routine, structure and activity, providing education, and teaching self-regulation techniques. Our case studies extend this perspective, underscoring the pivotal role occupational therapists play in trauma-focused aspects of treatment. This insight is crucial given the greater efficacy of trauma-focused compared to non-trauma-focused psychotherapies (Lewis et al., 2020a).
In both case studies, occupational therapists supported and implemented trauma-focused interventions in various ways. Montana, with a significant trauma history, exhibited extensive avoidance and safety behaviours and doubted her ability to challenge these patterns. The occupational therapist’s in-person support during her confrontation of avoided situations significantly reduced overwhelm, enhanced self-efficacy, and facilitated the independent completion of exposures, thereby increasing treatment adherence. Meeting clients outside clinical settings uniquely enables occupational therapists to identify safety behaviours and translate coping skills into everyday life more effectively than their psychotherapist counterparts. Furthermore, it provides the opportunity of an objective assessment of a client’s progress with in-vivo exposures (in addition to clients’ subjective self-report).
John, facing barriers such as reduced energy and motivation, found motivation and accountability through the occupational therapist’s in-person support, aiding in completing in-vivo exposures. The occupational therapist also collaborated with John to address symptoms of low mood through pacing and motivational interventions. This reduced the burden on the psychologist, which allowed them to fully focus on trauma processing. Finally, John struggled to tolerate his imaginal exposures. This experience is well documented in other PTSD studies and has been related to treatment dropout (Lewis et al., 2020b). However, with the support of his occupational therapist, John was able to continue his engagement in trauma processing throughout treatment.
Besides trauma-focused treatment, occupational therapists supported clients in community reintegration and envisioning a positive future. Both John and Montana, experiencing a loss of enjoyment, purpose and connection, regained these through goal-setting aligned with their values and re-engagement in meaningful activities. In addition to supporting improved mood, re-engaging in these activities made the trauma-focused aspects of treatment more manageable, and contributed in itself to changing trauma-related appraisals of permanent damage (e.g. “My life is over”) and feelings of hopelessness.
The report also emphasizes the crucial post-treatment role of occupational therapists in supporting injured workers’ next steps. For instance, John’s occupational therapist formulated a trauma-informed GRTW plan, which allowed for continued gradual exposure to trauma-reminders and avoided situations. This approach allowed for a successful and durable return to work by ensuring John was provided with the just-right challenge and necessary supports as he returned to the workforce. When workers are deemed unable to return to pre-injury work, as was the case for Montana, work-related restrictions are often determined by the psychotherapist in isolation. However, by observing the clients during work-related exposures, the occupational therapist can provide valuable information to determine return-to-work readiness and inform restrictions and limitations. The collaborative dynamic between occupational therapists and psychotherapists not only aids in assessing clients’ progress but also plays a vital role in charting a sustainable path forward for injured workers.
12 Recommendations for Clinicians and Students
Our article demonstrates the value of occupational therapist and psychotherapist collaboration in providing evidence-based trauma-focused treatment, adding to previous works considering the role of occupational therapists in the treatment of PTSD (Edgelow et al., 2019; Torchalla et al., 2019). Unfortunately, lack of knowledge and misconceptions among health professionals towards occupational therapy (e.g., Wan Yunus et al., 2022) may act as barriers to interdisciplinary collaboration. This is demonstrated by a recent study on the opinions of allied health professionals, in which only 42% of participants recognized occupational therapists as having a role in mental health (Alotaibi et al., 2018). Therefore, it is recommended that occupational therapists actively engage in efforts to promote their profession. This can be done through provision of both formal and informal education, publication in interdisciplinary journals, participation in interdisciplinary networking events and conferences, and informal discussions with members of allied healthcare disciplines.
Our case studies also highlight the potential for occupational therapists to expand their practice by incorporating trauma-focused, exposure-based interventions into their treatment repertoire. Occupational therapists can play a key role in graded exposure to trauma-related reminders and avoided situations, and addressing cognitive, emotional and behavioural return-to-work barriers early on. By doing so, occupational therapists can move beyond traditional rehabilitation and play a more proactive role in their clients’ mental health recovery. Occupational therapists interested in the provision of trauma-focused therapy should participate in professional development courses in related treatment modalities following graduation (e.g., a prolonged exposure course). Having an advanced skillset in evidence-based treatment is expected to not only improve treatment outcome, but also help occupational therapists to earn trust from their psychotherapist partners, thus facilitating collaboration between team members.
It is our clinical experience that outside of an explicitly interdisciplinary program, it is often suggested that occupational therapists should begin treatment only after psychotherapy treatment is nearly completed. This approach is led by an incorrect narrowing of the occupational therapy scope of practice to include return-to-work efforts alone, and a lack of understanding regarding the occupational therapist’s ability to provide trauma-focused treatment. We recommend that psychotherapists actively seek occupational therapists as partners in treatment planning for work-related PTSD cases, and that both clinicians collaborate by providing treatment simultaneously, as outlined in the above case studies. Shared treatment models, joint training programs, and interdisciplinary case consultations could strengthen the integration of these disciplines. Professional organizations and training institutions should incorporate education on interdisciplinary PTSD treatment within both psychotherapy and occupational therapy curricula. Students from both disciplines will benefit from learning these interventions and exploring and practicing their integration as part of their clinical training. Interdisciplinary collaboration is further supported by strategies aimed to foster a sense of familiarity between professionals. Clinics with interdisciplinary teams can create opportunities for informal interdisciplinary communication by hosting joint social events for practitioners, and creating opportunities for connection through the provision of shared office spaces.
While the benefits of interdisciplinary collaboration between allied health members and occupational therapists is well studied in areas such as chronic pain rehabilitation (Elbers et al., 2022), there is limited current research considering occupational therapy-psychotherapy collaboration in mental health. Future research should further investigate the efficacy of interdisciplinary approaches for work-related PTSD, and professional networks should foster collaboration between these fields. Strengthening this partnership has the potential to improve treatment outcomes, promote work reintegration, and ultimately enhance the quality of care for individuals with work-related PTSD by providing holistic, functional and psychologically informed care that addresses the clients’ full spectrum of needs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.