
Abstract
When clinicians address dangerous behavior via remote telehealth consultation, it may be especially important to ensure remote implementers can apply behavioral interventions in a manner that keeps recipients and implementers safe while still achieving effective outcomes. We present the case of a 13-year-old autistic adolescent with limited communication skills, living in South India, whose dangerous behavior was escalating and becoming more pervasive during the pandemic quarantine, putting himself and his family at risk. In this study, we evaluated the effects of an enhanced choice model of skill-based treatment—informed by a practical functional assessment of dangerous behavior. We systematically replicated and extended procedures that have been shown to address dangerous behavior while avoiding difficult situations that place the individual and others at risk. The intervention yielded elimination of dangerous and associated non-dangerous behavior and socially valid acquisition of multiple alternative behaviors. We report multiple strategies to overcome barriers unique to remotely addressing dangerous behavior and discuss implications for the safe, telehealth application of behavior analysis in research and practice.
1 Theoretical and Research Basis for Treatment
Skill-based treatment refers to a distinct set of behavioral intervention procedures, often informed by a specific practical functional assessment process, to address dangerous and challenging behavior (Hanley et al., 2014; Jessel et al., 2018, 2022). Following identification of a context that reliably evokes dangerous behavior or associated non-dangerous behaviors (e.g., precursor responses) and a highly reinforcing context that momentarily eliminates challenging behavior when instituted, skill-based treatment involves using differential reinforcement with some form of extinction, and various prompting procedures, to teach a comprehensive repertoire of social skills (e.g., self-advocacy, communication, coping with disappointment, cooperation with instructions from others). Layman et al. (2023) recently meta-analyzed 111 intervention outcomes associated with this specific intervention approach and revealed that skill-based treatments developed from practical functional assessment processes have nearly 100% success rate in eliminating dangerous behavior across myriad contexts and participant demographic profiles.
Rajaraman, Hanley, Gover, Staubitz, et al. (2022) described an extension of skill-based treatment procedures termed the enhanced choice model that successfully eliminated socially mediated, dangerous and non-dangerous challenging behavior of five children who were causing harm to themselves and others and who were all highly resistant to physical management from adults. Unique features of the enhanced choice model included: (a) providing ongoing options for individuals to choose to engage with intervention or not (with alternative options to either hang out with preferred activities or to terminate the appointment for the day); (b) incorporating multiple choice-making opportunities across intervention phases; (c) sharing detailed information before and after each session and opportunity for the individual to debrief, ask questions, and request changes to procedures; and (d) avoiding any physical guidance procedures as consequences to challenging behavior or noncooperation.
Two chief aims in extending skill-based treatment to incorporate enhanced choice procedures were to (1) promote safety during the intervention process by minimizing dangerous behavioral episodes and (2) increase the autonomy of recipients during effective interventions by arranging continuous opportunities for them to give and withdraw assent and influence procedures. The former aim was achieved in Rajaraman, Hanley, Gover, Staubitz, et al. (2022) as well as in replications by Metras et al. (2023) and Staubitz et al. (2022) in that dangerous and non-dangerous challenging behavior of nine child participants (across both studies) was not only eliminated, but rarely occurred during the intervention process. The latter aim also appears to have been achieved in all three studies in that participants chose to engage with the potentially challenging intervention context, despite having continuous options to hang out or leave, in approximately 80% or greater of opportunities. Similar procedures were also recently applied and were successful in addressing the food selectivity of three autistic children and one autistic adolescent who exhibited challenging behavior during mealtime contexts (Gover et al., 2023, 2024).
Thus far, enhanced choice model procedures have appeared to be efficacious (Metras et al., 2023; Staubitz et al., 2022) and socially valid (Rajaraman, Hanley, Gover, Staubitz, et al., 2022) when applied with children with developmentally appropriate language skills, and when implemented, in person, by either board-certified behavior analysts® (BCBA) or graduate student interns closely supervised by BCBAs. The emerging literature shows promise that behavioral interventions grounded in principles of behavior analysis can be applied to address dangerous behavior in a manner that keeps everyone safe throughout every part of the process while simultaneously respecting the autonomy of individuals served. However, replications and extensions are needed to understand boundaries of effectiveness and applicability.
2 Case Introduction
In the present study, we aimed to systematically replicate and extend the enhanced choice model of skill-based treatment in three distinct ways. First, we served an autistic adolescent (13 years old) with underdeveloped language skills (i.e., he communicated in 1–3-word phrases). Second, the parent of the adolescent conducted all analysis and intervention sessions. Third, all consultation of the process was conducted remotely, via telehealth, across two continents. Our primary question was whether we could conduct a socially meaningful intervention for dangerous behavior without observing dangerous behavior when providing telehealth consultation to a mother who had no professional support in her geographic area, and who along with her husband had been attempting to manage dangerous behavior in their home largely by themselves.
Sachin (pseudonym) was a 13-year-old autistic young man living in Chennai, Tamil Nadu, India. He communicated using 1–3-word sentences and gestures and appeared capable of following one-to three-step instructions (e.g., “get a tumbler and milk so I can make your tea”). He lived with his biological mother, Janani (pseudonym), and father. At the time the study commenced, the state of Tamil Nadu was in an indefinite and strict lockdown to prevent the spread of the Coronavirus.
The study’s procedures were approved by the institutional review board at the first author’s academic institution. Every element of the study, from initial intake and assessment to intervention planning, implementation, and evaluation, was conducted via remote telehealth consultation using HIPAA compliant video conferencing software. The first author (hereafter referred to as the analyst) provided all consultation to the family. Both parties (analyst and family) accessed the video call via a laptop with Internet connection.
3 Presenting Complaints
Sachin was referred for behavioral services by his mother, Janani, due to increasingly dangerous behavior that was occurring in the home as the pandemic lockdown endured. Janani reported that patterns of dangerous behavior (specifically, aggression toward Janani, head-directed self-injurious behavior, and property destruction) were spreading across more activities and contexts throughout the day and sometimes late into the night. Strategies that previously seemed successful in mitigating escalation to dangerous episodes were no longer effective. Sachin began engaging in multiple, often extended episodes of dangerous behavior and meltdowns each day. The immediate risk of harm posed by the aggression (e.g., scratching, hair-pulling, choking), self-injury (e.g., persistent slaps to the face), and property destruction (e.g., throwing heavy objects) to Sachin and his parents was imminently concerning unto itself. However, Sachin’s mother was further concerned that he would not be invited to return to school when it reopened due to how pervasive his dangerous behavior had become. Moreover, his family reported that he seemed deeply unhappy much of the time, and they feared that continued bouts of dangerous behavior would damage their relationship and may preclude the development of future relationships with peers and other community members.
4 History
In childhood, Sachin had a history of engaging in several topographies of dangerous behavior, including aggression, property destruction, self-injury, and extended meltdowns. However, according to parental reports, there was a two-to three-year window of time (when Sachin was approximately ages 9–12), prior to the pandemic and therefore prior to the onset of this study, during which Sachin’s episodes of dangerous behavior were infrequent and less of a concern. Janani reported that, during the period of lower-rate dangerous behavior, both parents were able to detect Sachin’s signs of agitation or discomfort and were typically successful in meeting his unmet need or otherwise redirecting Sachin to activities or spaces that served to calm him, thereby preventing escalation to dangerous episodes. During this period, Sachin was regularly attending school and engaged in many activities in and outside of the house, including daily bike rides, walks to local supermarkets and malls, and trips to the park and beach. All of Sachin’s activities, including school, were abruptly and indefinitely suspended upon initiation of the pandemic quarantine. Sachin’s school system provided limited virtual learning opportunities during the pandemic. To supplement this, Janani attempted to regularly have Sachin sit with her and engage in diverse academic tasks and physical education activities. According to Janani, it was shortly after the abrupt changes brought about by the lockdown that Sachin’s behavioral presentation changed dramatically and began posing seemingly intractable, imminent safety risks.
Janani had obtained a board certified, assistant behavior analyst (BCaBA) credential after receiving her son’s autism diagnosis. Janani emailed the analyst seeking assistance with dangerous behavior exhibited in the home. Despite behavior-analytic didactic and practical training, Janani did not (a) have experience assessing and intervening upon dangerous behavior, (b) have accessible professional support in her geographic region, or (c) feel comfortable conducting behavior analytic procedures with her son without support. In spite of these barriers, Janani was willing to serve as implementer of a behavior analytic process to address her son’s dangerous behavior in the home, provided there was support from the analyst.
5 Assessment
Open-Ended Caregiver Interview
We conducted a Practical Functional Assessment (Jessel, 2022; Whelan et al., 2021), comprised of an open-ended functional assessment interview (Hanley, 2012) and interview-informed synthesized contingency analysis (IISCA; Brown, 2021; Hanley et al., 2014; Rajaraman & Hanley, 2020), to understand the variables influencing Sachin’s dangerous and associated non-dangerous behavior and to develop a motivating yet safe context in which to teach skills. An additional purpose of the interview was to ascertain Janani’s goals for Sachin with respect to behavioral intervention, as well as her and her family’s personal and cultural preferences and sensitivities that the analyst could consider in the development of intervention procedures and objectives. Janani served as the informant during the interview and the implementer of the IISCA. Janani was fluent in several languages, including Tamil and English. The analyst was fluent in English, could fully understand and comprehend spoken Tamil, and was able to speak a blend of Tamil and English at a conversational level (colloquially referred to as Tanglish). Therefore, correspondence between Janani and analyst routinely involved blended Tamil and English (see Sivaraman & Fahmie (2020) and Tsami et al. (2019) for some discussion on the importance of common language to consumers of telehealth services).
Sachin’s Response Definitions and Measurement.
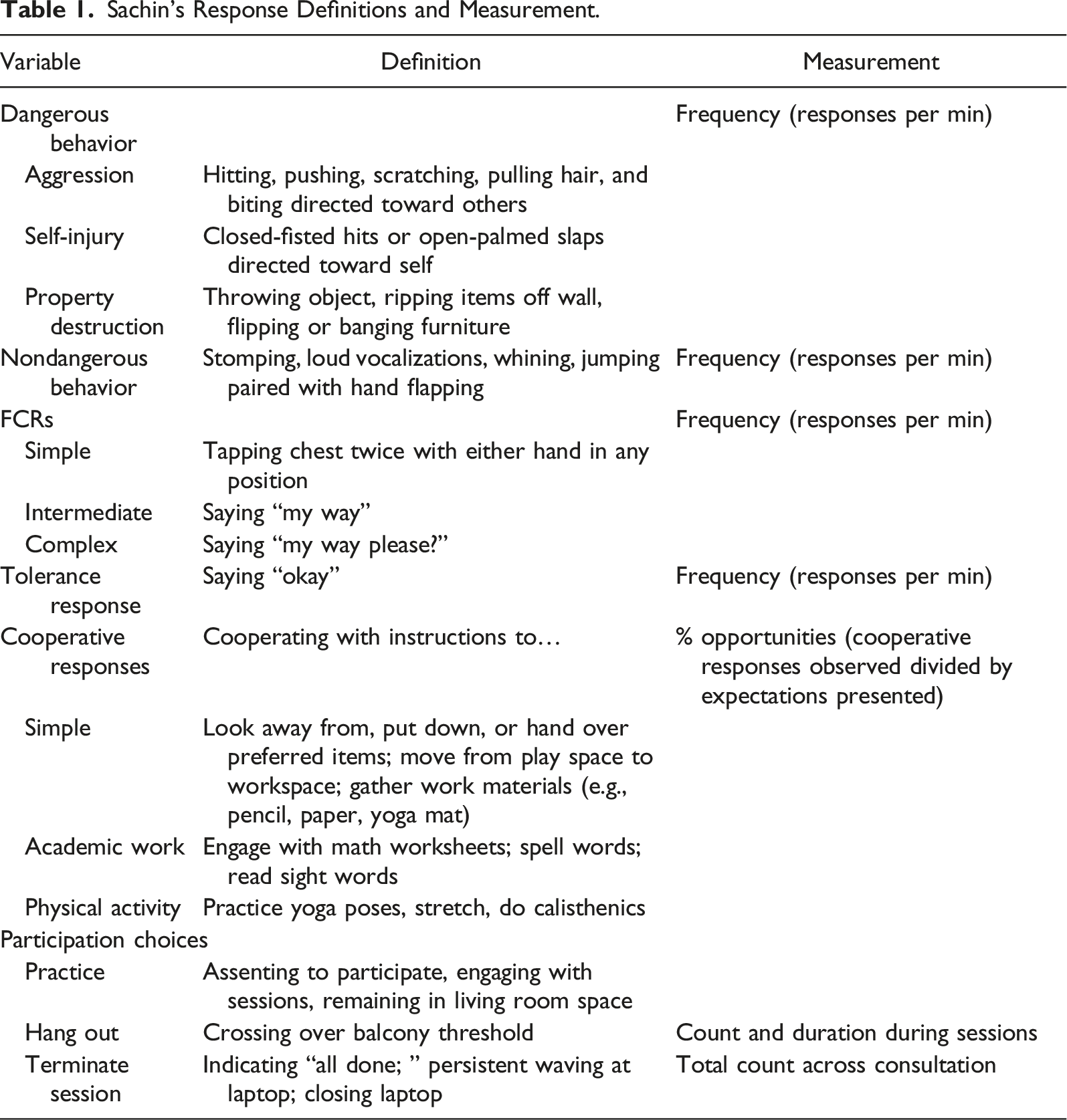
Janani reported that her goals for Sachin were closely linked to her current challenges. She wanted Sachin to be able to (a) communicate when he was upset instead of defaulting to challenging behavior, (b) stay safe and calm during periods when he could not have his preferred items and activities, and importantly, (c) willingly cooperate with adults when presented instructions similar to those experienced in school. Janani nominated academic contexts, involving math and reading, as well as physical activity contexts including yoga and calisthenics as areas in which she would like to see Sachin’s improved cooperation. Janani’s overall goal was for Sachin to be able to return to school and participate meaningfully and successfully with scheduled expectations therein. All reported goals were targeted during skill-based treatment.
Interview-Informed Synthesized Contingency Analysis (IISCA)
Janani implemented all conditions of the IISCA in her home with coaching from the analyst via telehealth. An IISCA is a type of functional analysis that involves arranging two conditions: one in which the suspected reinforcement contingency is absent (i.e., control) and one in which it is present (i.e., test). A unique feature of the IISCA relative to other functional analysis formats is the deliberate, proactive synthesizing of reinforcement contingencies when they are suspected to operate congruently in the natural environment, as gleaned from the interview (Slaton & Hanley, 2018). Because Janani reported multiple events that appeared to simultaneously precede and follow episodes of dangerous behavior, the IISCA seemed to be the most appropriate approach to analyzing Sachin’s behavior and serving as the basis for intervention development.
The analyst relied on behavior skills training (BST; Lloveras et al., 2022; Nylen & King, 2023) to coach Janani on implementation of the IISCA. Janani and the analyst met for 45 min prior to the analysis session to allow for virtual description of and rationale for procedures, modeling, rehearsal (with the analyst emulating child behavior over videoconference), and feedback. Due to (a) Janani’s limited access to in-person training opportunities, (b) the perceived urgency of the consultation, and (c) the fact that Janani would have live coaching from the analyst via a Bluetooth earpiece, we did not pursue formal training and mastery criteria prior to conducting the analysis. Instead, the analyst rehearsed all elements of both conditions of the analysis and answered all questions until Janani noted feeling comfortable and “ready” to conduct the analysis. The authors acknowledge that some risk could be imposed by asking a mother to implement procedures without a formal demonstration of competency; however, due to several safety considerations germane to the IISCA (described below) as well as a specific emphasis that Janani could deliver all suspected reinforcers at any time to thwart behavioral escalation, the analyst and, importantly, Janani, felt risk was sufficiently mitigated and the analysis could be conducted safely. During the first telehealth appointment that included Sachin, Janani introduced him to the analyst over the video call. The analyst and Janani described to Sachin that these calls would occur a few times a week so the analyst could help mom play with and teach Sachin new things. Sachin was asked if he would like to participate in the process and he provided initial assent with a head nod or by approximating “okay.”
During the 5-min control conditions, Janani provided Sachin with free access to all suspected reinforcers. He had uninterrupted access to his favorite toys, she honored his requests as quickly as she could, and she refrained from imposing any demands related to participating in academics or physical activity. If challenging behavior were to occur during this condition, Sachin’s mother would have attempted to comfort him, detect which reinforcers were missing from the context, and deliver them immediately (this did not happen during the control condition). During the 5-min test conditions, Sachin’s mother periodically interrupted a similar reinforcement experience by slowly imposing and progressing the EOs until Sachin engaged in any targeted topography of dangerous or associated non-dangerous behavior. For example, while Sachin was playing with his toys and interacting with Janani, she would slowly shift her body positioning by standing up as if she was about to deliver an instruction. Then, without touching his preferred toys, she would instruct him to stop playing with them. If he did not engage in any dangerous or associated non-dangerous behavior during that sequence, she would continue to progress the EO by presenting instructions until Sachin was cooperating with instructions to participate in his most challenging tasks. If at any point in that sequence he engaged in target non-dangerous or dangerous behavior, she immediately reinforced the response(s) by returning the preferred items and removing the instruction (i.e., synthesized reinforcement) for 45–60 s. This sequence repeated until 5 min elapsed.
To promote safety and prevent escalation to dangerous behavior, we included associated non-dangerous responses in the class of behaviors that would be eligible for reinforcement during the analysis (Pollack et al., 2024). This tactic has not been explicitly articulated in telehealth evaluations of functional analysis to our knowledge (Schieltz & Wacker, 2020); however, it is not without precedent in the functional analysis literature. In fact, multiple studies have demonstrated that, when caregivers report that certain non-dangerous topographies tend to precede or co-occur with dangerous topographies, they are very likely to share response class membership (e.g., Heath & Smith, 2019; Hoffman et al., 2018; Magee & Ellis, 2000; Smith & Churchill, 2002; Warner et al., 2020). That is, identifying the reinforcers for associated non-dangerous behaviors is tantamount to identifying the reinforcers for dangerous behavior. This means that the contingencies influencing dangerous behavior can be understood while only evoking and reinforcing associated non-dangerous behaviors (Rajaraman, Hanley, Gover, Staubitz et al., 2022; Warner et al., 2020), which has important safety implications for telehealth applications of functional analysis.
Procedural Integrity and Interobserver Agreement
To intermittently assist with coaching and to help Janani ensure she was implementing procedures as intended, a trained observer and data collector scored Janani’s procedural integrity across analysis and treatment sessions using the integrity checklists reported in the Appendices of Whelan et al. (2021; analysis) and Rajaraman, Hanley, Gover, Ruppel, et al. (2022; intervention). Checklists were slightly adapted to reflect in-home application, and the addition of enhanced choice procedures (described below). Procedural integrity was scored for 33% of sessions across analysis and intervention (range, 25%–50% within each phase) and was calculated by dividing the number of correctly implemented components in a session by the total number of components and multiplying by 100. Janani’s mean procedural integrity was 96% (range, 92%–100%) during the analysis and 98% (range, 96%–100%) during intervention. We note the analyst did provide live coaching during all appointments; however, most of the feedback, debrief, and discussion occurred in between sessions. Had performance errors occurred during sessions, they would have been scored and reported as integrity errors even though the analyst provided in-the-moment feedback. In other words, the above integrity scores reflect Janani’s independent performance during sessions suggesting high implementation integrity.
Undergraduate research assistants were trained to collect data on all measures reported in Table 1. To promote reliable and accurate data collection (i.e., interobserver agreement; IOA), two data collectors independently scored 33% of sessions across analysis and intervention (range, 20%–50% within each phase). Agreement was calculated by dividing each session into 10-s intervals, dividing the number of measures in agreement per interval by the number of disagreements plus agreements per interval, and multiplying the quotient by 100. For all dependent measures across analysis and intervention, mean IOA was 97% (range, 80%–100%).
6 Case Conceptualization
Results from Sachin’s functional analysis are depicted in Figure 1. During control conditions, Sachin did not engage in any targeted topography of dangerous or non-dangerous behavior. During test conditions, he reliably engaged in non-dangerous target behavior when his mother implemented the EOs. He engaged in one instance of dangerous behavior across the analysis (in session 6). Sachin’s functional analysis indicated his dangerous and non-dangerous topographies of problem behavior were indeed sensitive to escape from non-preferred tasks, access to preferred toys, and mand compliance (Rajaraman & Hanley, 2021). The results of the IISCA provided information about a contingency that was functionally related to the behaviors of concern, but it importantly revealed (a) evocative events that quickly motivated Sachin to exhibit dangerous or associated non-dangerous behavior, and (b) reinforcing events that immediately quelled behavior and ensured a safe situation. This synthesized reinforcement contingency would serve as the basis for subsequent intervention. Interview-informed synthesized contingency analysis data for Sachin’s challenging behavior.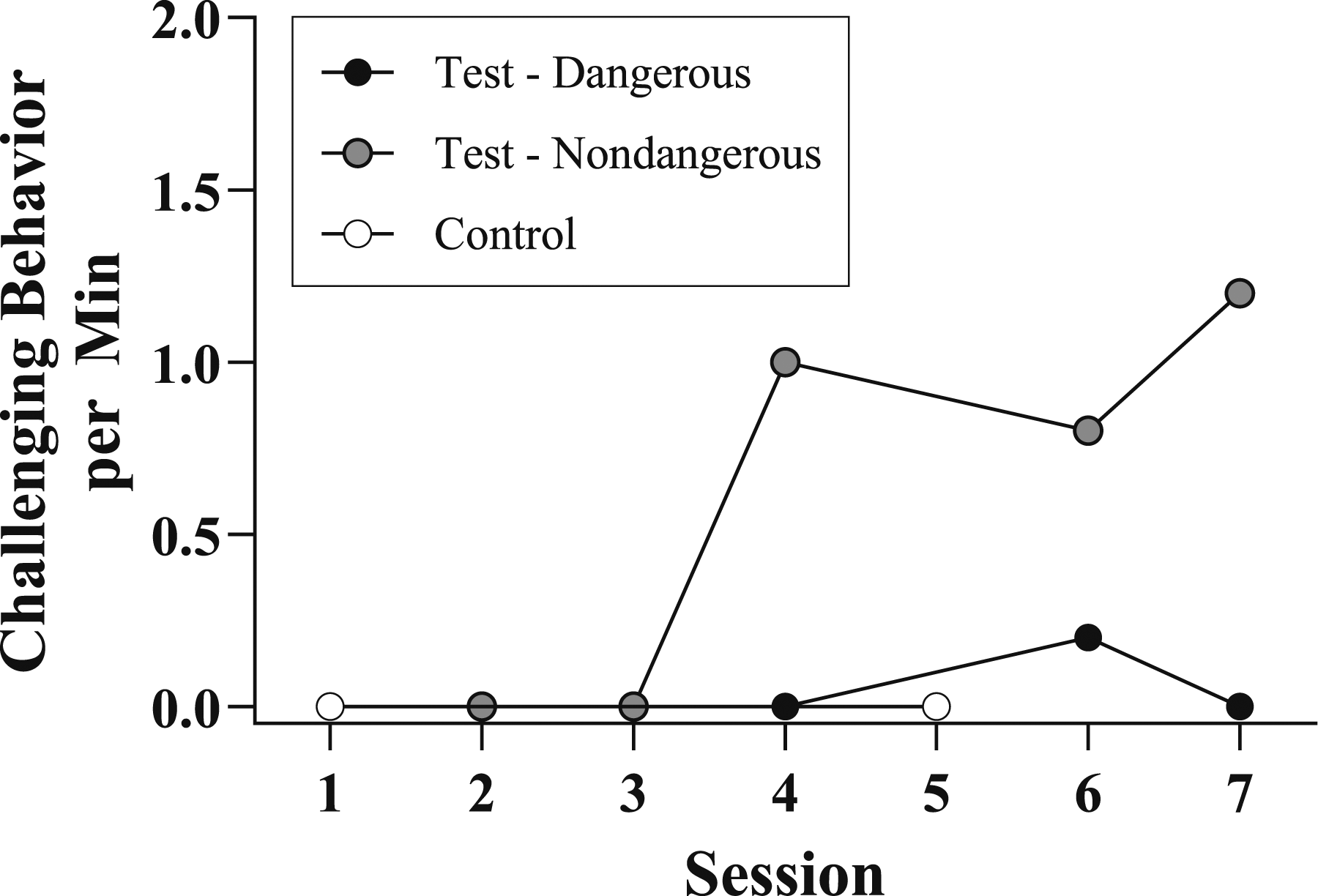
Based upon the results of the practical functional assessment process, and the skill-related goals Janani nominated, we agreed that a skill-based treatment was the proper intervention approach. Following the IISCA, Sachin’s mother implemented all phases of a skill-based treatment package within an enhanced choice model in her home with coaching from the analyst via telehealth. One-hour sessions were conducted two-to-three times per week during which the analyst communicated to Sachin’s mother and observed via video conference. Data from the test conditions of Sachin’s IISCA served as baseline data from which to evaluate the effects of the intervention.
Skill-based treatment is an intensive, focused, behavioral intervention package. It does not describe a “behavior-intervention plan” that could be immediately arranged across Sachin’s days. By contrast, skills that can effectively replace dangerous behavior are carefully introduced, taught, and differentially reinforced during planned exposure to challenging contexts. Because Janani was receiving coaching on these procedures in alignment with her aims for Sachin and herself, we implemented skill-based treatment during dedicated sessions with the analyst present. However, because Sachin’s dangerous behavior was potentially concerning around the clock, we shared some suggestions with Janani on how she might mitigate behavioral escalation during periods when we were not conducting sessions. The chief recommendation was informed by the results of the IISCA; Sachin’s dangerous behavioral episodes were likely to be mitigated, in the moment, by the immediate delivery of all possible reinforcing consequences, particularly upon early signs of agitation (i.e., associated non-dangerous behavior). The analyst reflected on this finding with Janani following the IISCA, noting that although it would not be a long-term solution, it may help keep things safe during moments of escalation across the day, while important skills were being developed during dedicated intervention sessions. In the current study, we did not report the extent to which this recommendation was adopted and efficacious for Janani’s home situation.
7 Course of Treatment and Assessment of Progress
Skill-based treatment primarily involves differential synthesized reinforcement with prompting of target skills, wherein prompts are gradually and flexibly faded to promote independent responding under authentic EO conditions. Across all phases of skill-based treatment, sessions consisted of five trials (i.e., five presentations of the synthesized reinforcement contingency). Trials increased in duration and difficulty as Sachin developed more complex skills. As such, sessions varied in duration, with the mean session duration lasting approximately 10 min (range, approx. 4 min–22 min). Skills were built in progression from communication, to coping (i.e., toleration of disappointment), to cooperation. New skill expectations were only introduced after two consecutive sessions of no dangerous behavior and consistent emission of the target skill under the proper stimulus conditions.
Similar to the IISCA, we relied on BST with in-vivo coaching to aid Janani in implementation of skill-based treatment procedures. Prior to commencing each distinct intervention phase, Janani and the analyst would meet ahead of the day’s appointment (usually by starting the videoconference 10–15 min early) so the analyst could describe, rationalize, model, allow rehearsal, provide feedback, and answer questions regarding upcoming procedures. The 5–10 min prior to each subsequent appointment consisted of a brief review of the current intervention phase, associated goals and procedures, and opportunity for Janani to ask pertinent questions. Janani continued to wear an earpiece during each appointment so the analyst could provide in-vivo positive and corrective feedback. Janani’s procedural fidelity was indeed quite high (98%) during actual implementation of skill-based treatment procedures, suggesting that in-vivo feedback was relatively sparse throughout. However, when Janani perceived challenges or had questions that required nuanced answers, they debriefed for 5–10 min following the day’s appointment.
The first phase of skill-based treatment involved functional communication training (Carr & Durand, 1985; Ghaemmaghami et al., 2021; Tiger et al., 2008), during which Sachin was taught a functional communicative response (FCR) that produced access to all the reinforcers identified in the IISCA. Similar to the test conditions of the IISCA, Sachin’s mother would instruct him to stop playing and participate in an activity. She would then provide an immediate prompt to emit a non-vocal FCR of tapping his chest twice. Emission of the FCR, either prompted or unprompted, resulted in the immediate delivery of synthesized reinforcers. Once he emitted that simple FCR in the absence of any dangerous or non-dangerous behavior, she prompted a more intermediate FCR (a vocal request, “My way”). Once he emitted the FCR, “My way,” consistently in the absence of dangerous behavior, she taught him a more complex FCR, “My way, please.”
Next, tolerance response training was initiated. The purpose of tolerance response training was to teach Sachin an adaptive response in the face of disappointment (e.g., when the FCR was denied). Once Sachin consistently emitted the complex FCR, “My way, please” in the absence of dangerous behaviors, his mother began to periodically deny his FCR and taught him the tolerance response (TR), “Okay.” Once he emitted the TR, his mother immediately provided access to his synthesized reinforcers. Denials to the FCR were intermittent and unpredictable such that Sachin could not detect when his FCR would be granted and when it would be denied. On average, FCRs were reinforced on 20% of trials and TRs were reinforced on 80% of trials.
Once Sachin was consistently emitting the complex FCR when his mother told him to stop playing and engage in an activity and emitting the TR when his FCR was denied all in the absence of non-dangerous or dangerous behavior, his mother initiated the contextually-appropriate-behavior (CAB) chaining phase of skill-based treatment. On an intermittent and unpredictable schedule, she presented instructions for Sachin to cooperate with adult-directed tasks after he emitted the TR. These tasks were selected based on the contexts that (a) evoked dangerous and non-dangerous behavior during the IISCA and (b) were nominated by Janani as important for Sachin at home and in school. Janani started by introducing simple tasks such as relinquishing his preferred tangible items and transitioning to a different space in his house. All the while, she continued to reinforce the FCR on approximately 20% of trials and the TR on approximately 20% of trials.
Once Sachin was reliably cooperating with simple instructions, Janani provided instructions related to two specific repertoires: academic instruction and physical activity. She started with academic instruction, slowly progressing to more and more instructions as he completed smaller chains without exhibiting any targeted dangerous or non-dangerous behaviors. Instructions to complete physical activities were introduced in the same way. Sachin’s mother progressed from short, simple physical tasks to longer and more challenging activities. After completing the specified number of instructions or duration of physical activities in the absence of dangerous or associated non-dangerous behavior, Sachin was provided access to synthesized reinforcers.
Unique challenges—germane to remote application and Sachin’s potential for harm when in distress—required that the intervention be guided by safety and parent-child rapport. Safety in this regard primarily referred to minimizing the occurrence of Sachin’s dangerous behavior despite repeatedly exposing him to known challenging situations. Contrary to many typical clinical settings in which several restraint-trained professionals may be available to respond to dangerous behavior during intervention, Janani would likely not be able to keep herself or Sachin safe should he have escalated to dangerous behavior.
One strategy we emphasized to promote safety during dedicated sessions was to encourage Janani to immediately reinforce any instance of dangerous behavior with all synthesized reinforcers (this never occurred during intervention). This was an important addition because skill-based treatment involves repeatedly presenting EOs known to be challenging for Sachin, which had historically evoked dangerous behavior. If Sachin displayed any associated non-dangerous behavior, Janani was encouraged to respond empathetically, keep the EO in place, and provide an additional prompt to emit the target skill (Landa et al., 2021). For example, if Sachin began whining or stomping during academic instruction, Janani would have acknowledged Sachin (e.g., “I know this is difficult; you are working hard”), kept the expectation in place (e.g., “we still need to work on math right now”), and provided an additional prompt (e.g., “you can pick up your pencil like this”). Importantly, despite encouraging the above procedure in response to associated non-dangerous behavior, the analyst stressed to Janani that terminating the trial by providing synthesized reinforcement was always an option up to her discretion to promote safety in the moment. Associated non-dangerous behavior never occurred during intervention.
A second strategy we implemented to promote safety and autonomy during dedicated sessions was that we arranged for Sachin to be able to withdraw assent to participate at any time during all analysis and subsequent intervention conditions. In other words, if Sachin indicated to his mother that he did not want to participate in the session, if he left the analysis space mid-session, or if he requested to or closed the video call on the laptop, his mother honored that choice instead of insisting on his participation. This tactic was included to promote safety and to preserve rapport given his potential for dangerous behavior (Jessel et al., 2023; Rajaraman, Austin, et al., 2022). According to Janani’s reports, if she had attempted to cajole or force Sachin to participate, he may have escalated to aggression or self-injury. Prior to the IISCA, Janani conveyed to Sachin that he could terminate video calls at any point by asking to be all done, or by closing the laptop. This occurred twice throughout the course of assessment and intervention.
The first time Sachin closed the laptop was during the first appointment, approximately 25 min into the call and prior to the initiation of any IISCA or intervention sessions. Upon debrief, Janani suggested that Sachin may have felt uncomfortable being observed by a stranger and likely felt interrupted by conversations she and the analyst were having during Sachin’s play time (i.e., mother’s attention was diverted). The team scheduled an additional call, prior to the onset of the functional analysis, in which Janani was asked to play with Sachin in his preferred manner for the duration of the call. To minimize disruptions to Sachin’s play time, Janani wore a Bluetooth earpiece, and the analyst kept his camera off during the calls (these tactics remained in place throughout the consultation). Sachin appeared more comfortable with the video call setup, as he did not request to end the call. In subsequent appointments, video calls always began with at least 5 min of uninterrupted play. Sachin terminated the appointment one additional time, during the first day of skill-based treatment, approximately 48 min into the one-hour appointment.
A third strategy to promote safety and autonomy throughout intervention was that Sachin was provided an additional opportunity to escape the intervention context (i.e., reinforcement space, academic instruction space, physical activity space) to the balcony of his apartment where no specific contingencies were programmed for any response. Sachin was free to go “hang out” on the balcony, bring toys and other preferred materials, and to invite his mother to join him. He was allowed to spend as much time out there as he liked and was not prompted to return to the intervention space. When and if Sachin chose to re-enter intervention, trials resumed. Sachin chose to hang out on the balcony on seven occasions across all intervention sessions, for a total duration of 13 min 15 s (mean duration 1 min 53 s per hang out; these sessions are denoted with the letter “H” in the sixth panel of Figure 2). Enhanced choice model of skill-based treatment evaluation for Sachin. Note. BL is baseline. FCT is functional communication training. FCR is functional communicative response. TRT is tolerance response training. CAB is contextually appropriate behavior. The H above data points in the sixth (cooperation) panel denote sessions during which Sachin elected to hangout for some period.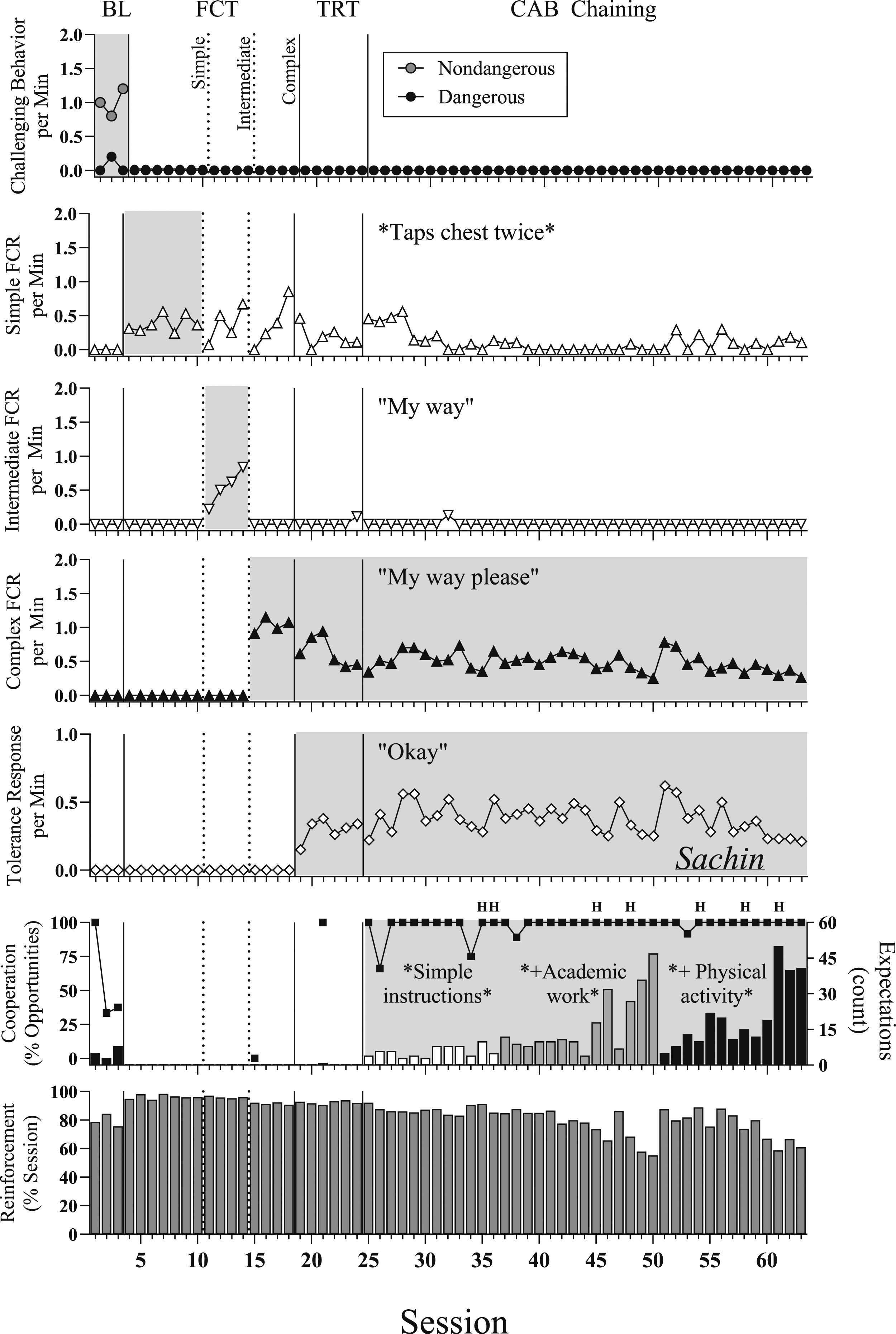
Intervention progress was assessed throughout the course of intervention by monitoring levels of dangerous and associated non-dangerous behavior, prompted and independent skills emitted, and the instances Sachin chose to “hang out” per session and across conditions. Some markers that would indicate an issue with progress would be the occurrence of high frequency dangerous or associated non-dangerous behavior, the absence of independent responding despite prompting and reinforcement being in place, and excessive appointment termination or use of the hang out space. If these markers occurred and impeded the ability to run sessions or to make meaningful progress, adjustments would have been made in collaboration with Janani and Sachin.
The internal validity of the study (i.e., the extent to which changes in behavior could reasonably be attributed to the independent variable) was evaluated via a multiple baseline across skills design. The independent variable involved differential synthesized reinforcement with prompting, as this was the contingency systematically manipulated and applied to new skills across intervention phases. Evidence of the effect of the synthesized contingency was seen when each new skillset (i.e., simple FCR, intermediate FCR, complex FCR, tolerance response, simple instructions, academics, physical activity) emerged only when it was included in the contingency requirement.
Results from Sachin’s intervention evaluation are depicted in Figure 2. Simple functional communication training resulted in the immediate elimination of dangerous and associated non-dangerous behavior. Dangerous and associated non-dangerous behavior remained at zero throughout the duration of this intervention evaluation (top panel). Sachin mastered simple FCT in seven sessions (second panel), intermediate FCT in four sessions (third panel), and complex FCT in four sessions (fourth panel). Sachin mastered the TR in six sessions (fifth panel).
Sachin learned to cooperate with simple instructions, academic work, and physical activity (sixth panel) in the absence of non-dangerous and dangerous behavior. These were the same CAB expectations that immediately evoked associated non-dangerous behavior during baseline and that Janani had reported were often met with extended episodes of dangerous behavior. Discrete academic expectations (e.g., complete this math problem, sound out this sentence, write your name) were introduced and interspersed into trials after Sachin exhibited cooperation with simple instructions. Sachin cooperated fully (100%) with 36 and 47 discrete academic tasks and simple instructions in sessions 49 and 50 respectively, after which physical activity expectations were introduced and interspersed into trials (e.g., balance on one leg, hop ten times, do a sun salutation). Skill-based treatment culminated when Sachin fully cooperated (100%) with 40 and 41 discrete CAB expectations in sessions 62 and 63, respectively. Visual inspection of the data revealed that immediate and lasting changes to the level and trend of all relevant dependent variables occurred when the independent variable was applied to each respective variable. The grey shading across panels of Figure 2 conveys the responses to which the synthesized contingency was applied. Elevated behavior in each of the grey-shaded panels suggests that the prompting and differential synthesized reinforcement was indeed responsible for the changes in all targeted behavior.
8 Complicating Factors
We encountered several technical difficulties while attempting to conduct routine behavioral intervention via telehealth. Difficulty with inconsistent and unreliable Wi-Fi meant that some scheduled sessions could not continue as planned. Moreover, given the urgent conditions under which the case consultation commenced, the authors did not have the opportunity to adequately vet videoconferencing programs and relied on Google Meet due to its institutional HIPAA compliance. One example of where the video setup fell short was that we did not have video coverage of the balcony area where Sachin occasionally chose to hang out. If Sachin left the frame of the camera to the right side (i.e., toward the balcony), we could not reliably capture his activity while off screen. We therefore only measured and reported duration of time in hangout as a corollary of Sachin’s withdrawal of assent to participate in sessions.
Furthermore, given the inclusion of enhanced choice model procedures, wherein Sachin could opt to terminate the telehealth session at any time, we had to be prepared for the possibility of a shortened session. This not only had the potential to elongate the duration of service, but also resulted in intervention planning that may have been more methodical than is typical of skill-based treatments conducted in person. Our goal was to have Janani increase her expectations in such a manner that Sachin would not opt to hang out or terminate the session; as such, we often made small, incremental increases in that which was expected of Sachin during periods of nonreinforcement.
9 Access and Barriers to Care
Janani reached out to our team because there were no suitable ABA services in her city or state in India. Janani’s reports of alienation in this regard were exacerbated by constraints imposed by the pandemic, which required that Janani and Sachin remain in their high-rise flat across most hours of each day. Said another way, Janani was essentially isolated from professionals with expertise in the assessment and intervention of dangerous behavior. As such, remote service delivery was the only viable option, and its viability depended on Sachin’s capacity to tolerate routine sessions with an ostensible stranger videoconferencing into his space. This underscores the importance of procedural modifications that ensured Sachin had the autonomy and skills to advocate for himself during the consultation, and sensitivity to such advocacy indications on the part of Janani and the analyst.
10 Follow-Up
Caregiver Social Validity Evaluation of Assessment, Intervention, and Telehealth Process.
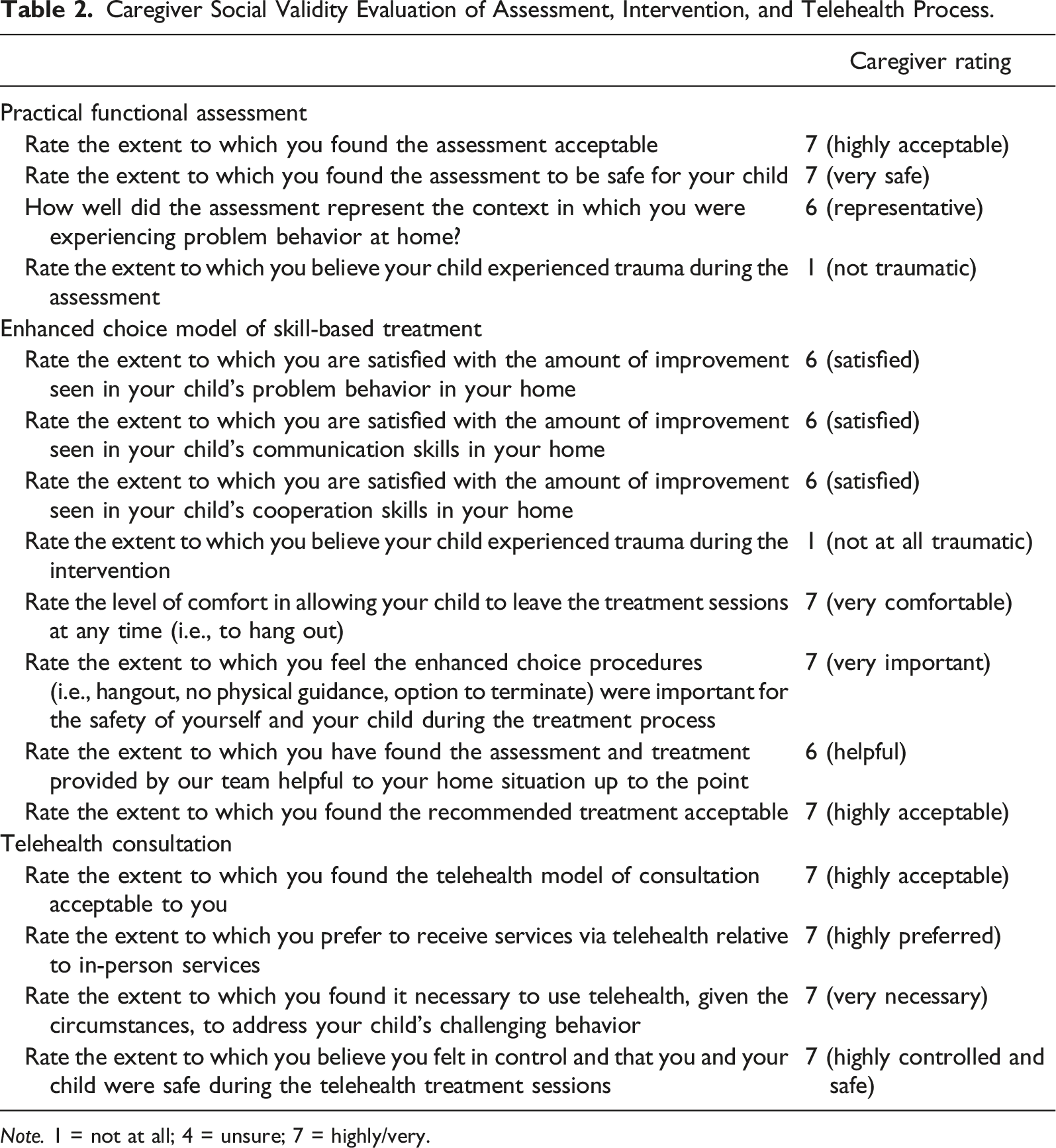
Note. 1 = not at all; 4 = unsure; 7 = highly/very.
The analyst and Janani remained in touch via WhatsApp following the consultation. Janani informed the team that Sachin was able to be successfully re-invited back to his school once the quarantine was lifted. She commented that he had several successful weeks before beginning to show some agitation in school. When asked to meet with Sachin’s teachers, Janani introduced them to the “hang out” concept, described what it might look like in his classroom (e.g., a cozy corner of the room where Sachin could escape with preferred items), and asked them to consider incorporating it. They agreed, and Janani anecdotally reported it appeared to virtually eliminate agitation in school. Although we did not conduct direct behavioral observations in Sachin’s school and cannot speak to the extent to which Sachin and Janani’s experience with telehealth consultation contributed to these reported positive effects, we argue Janani’s testimony and the school’s adoption minimally provide supplemental evidence of the social acceptability of the proposed procedures.
11 Treatment Implications of the Case
We were able to safely coach a caregiver, via telehealth, through the assessment of and intervention for dangerous behavior exhibited by their son in a manner that achieved the stated behavioral goals of the consultation while minimizing the occurrence of dangerous behavior. This study extends the existing literature on the enhanced choice model and behavioral telehealth research by demonstrating the generality of its effectiveness to the behavior of an autistic adolescent with underdeveloped language skills. Procedures and outcomes reported in this study further expand the generality of the applicability of the enhanced choice model by demonstrating that the entire assessment and intervention process can be successfully implemented in home by a parent (albeit with some background in behavior-analytic principles), with entirely remote, telehealth consultation from a trained analyst.
Furthermore, to our knowledge, this study represents one of the first demonstrations of telehealth assessment and intervention for dangerous behavior that targeted and reported the acquisition of multiple alternative skills in the presence of challenging situations that previously evoked dangerous behavior. Schieltz and Wacker (2020) conducted a review of functional assessment and function-based treatment delivered via telehealth and found a total of 18 studies. Nearly 30% of those studies did not include any intervention (i.e., functional assessment only) and most studies that did include intervention only taught a single skill, such as a communication response, without reaching more practical implementation goals (e.g., thinning reinforcement). Using the enhanced choice model and skill-based treatment, we were able to thin reinforcement and teach a host of skills that included communication responses of increasing complexity, tolerance with denials, and cooperation with instructions across personally relevant domains. In addition, the entire assessment and intervention process was reported by a caregiver to have been appropriate and helpful to their home situation.
The results of this clinical case have multiple implications for clinicians who provide behavioral services to individuals who exhibit dangerous behavior. First, it appears increasingly possible to teach multiple skills in situations demonstrated to be challenging while effectively eliminating dangerous behavior in a manner that does not seem to place individual’s and their family in harm’s way (i.e., in a manner wherein targeted dangerous behavior rarely occurs). Across all published reports of the enhanced choice model, including the current study, dangerous behavior seldom occurred despite repeated presentations of known challenging situations (Metras et al., 2023; Rajaraman, Hanley, Gover, Staubitz, et al., 2022; Staubitz et al., 2022). We attribute this benefit to the procedures of the enhanced choice model in that Sachin could choose to leave at any point if the behavioral expectations became too “stressful,” so to speak. Instead of engaging in dangerous behavior, Sachin could indicate his lack of preference for the context by immediately removing assent and choosing to enter a different context, not only free from punitive consequences, but with similar reinforcers freely available. In addition, we attempted to ensure the safety of all those involved by reinforcing early indicators of agitation or distress (i.e., associated non-dangerous behavior; Warner et al., 2020). That is, we provided reinforcers upon indications of behavioral escalation during analysis resulting in almost immediate calming and the cessation of behavior. It seems reinforcing early indicators of dangerous behavior helps thwart escalation to dangerous behavior and emotional outbursts, the occurrence of which could place the individual and those attempting to manage dangerous behavior, at risk (Heath & Smith, 2019; Smith & Churchill, 2000; Warner et al., 2020).
Another clinical implication of this study is the ability to coach caregivers through the assessment and intervention process using telehealth. This allows clinicians to serve individuals outside of areas where the majority of their clientele may live and creates a cost-effective way for caregivers to access specialists for specific intervention needs. For example, it was highly unlikely for there to be any other clinicians in the region of India where the family lived who were trained in conducting the enhanced choice model. The only options were to fly experts from out of the country or receive the services through telehealth. Although there has been success of using telehealth with ABA programming (e.g., Gerow et al., 2023; Lindgren et al., 2016), this is the first demonstration of the application of the enhanced choice model of skill-based treatment with data depicting that the entire process was virtually devoid of dangerous behavior. The fact that Janani held a BCaBA credential prior to the initiation of the study likely positively moderated implementation integrity and concomitant intervention effects, in that knowledge of behavioral principles could have helped Janani more readily pick up procedures and their underlying rationale. That said, emerging evidence suggests that individuals with no prior training or knowledge in applied behavior analysis can conduct successful skill-based treatments with intensive coaching support (Pollack et al., 2021).
12 Recommendations to Clinicians and Students
Clinicians may want to consider embracing telehealth when addressing dangerous behavior exhibited by clients who may not be readily available for in-person consultations. The COVID-19 pandemic was likely a catalyst for many ABA providers and organizations transitioning to telehealth services (Pollard et al., 2021); however, it seems the benefits of telehealth are far broader. For example, Lindgren et al. (2016) conducted a large trial comparing in-home therapy against clinic-based- and home-based telehealth. They found similar ultimate reductions in dangerous behavior and parent acceptability across all conditions but reported both telehealth models to be far less costly and likely more accessible.
Addressing dangerous behavior in a safe context (i.e., one in which dangerous behavior was unlikely) was particularly important given that the analyst was providing training from thousands of miles away. In other words, we would not have been able to provide direct behavioral support in any way if something dangerous were to happen. There is an inherent risk to safety for those who may live in rural areas without immediate access to services; however, this does not make their need for such services any less essential. It is also important to note that this behavioral intervention did not require any physical management. It would have been difficult to coach caregivers to physically manage Sachin’s challenging behavior via telehealth and would it have been physically difficult for his mother to implement alone. Janani even expressed an inability and unwillingness to do so because her son was already too strong for her, and he would likely be able to overpower her in any attempt to physically manage him.
Indeed, Schieltz and Wacker (2020, p. 1255) noted that “older individuals who engage in severe aggression that may harm others” have not been represented in behavioral telehealth research. Therefore, when the target behaviors are particularly dangerous, and when individuals have imminent potential for harm, clinicians may want to consider reinforcing associated non-dangerous behavior and adhere to the procedures of an enhanced-choice model. If these procedures are taken together, non-dangerous associated behaviors such as precursors and opting to hang out can serve as useful opportunities to re-evaluate procedures, examine their possibly aversive features, and adjust accordingly to foster positive intervention progress—with the added benefit of safety from dangerous behavior.
Footnotes
Acknowledgments
The authors would like to thank Viola Lis, Alex Harvin, Eric Neutzling, and Elaina Lee Schnelle for their assistance with data collection and preparation of the current manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.