
Abstract
The prevalence of Obsessive-compulsive disorder (OCD) among older adults varies between .5% and 4.5%. OCD typically develops at a young age, and many clinicians consider the chances of successful treatment in older adults to be minimal based on the chronicity of their symptoms. To date, no randomized controlled trial have been conducted on the effectiveness of treatments for OCD in older adults. This case study describes a high intensive cognitive behavioral therapy (CBT) provided to a 72-year-old man with OCD. This CBT program includes psychoeducation, exposure and response prevention, and cognitive therapy. The treatment was provided by a team of 5 therapists over one week. The patient’s score on the Yale Brown Obsessive-Compulsive Scale decreased from 31 at the start of the treatment to 2 by the end of treatment, which is below the recommended cut-off for a clinical diagnosis. Secondary depressive symptoms, as assessed with the Inventory of Depressive Symptomatology Self-Report, decreased from 57 at the start of treatment, to 1 by the end of treatment, which indicates the absence of depressive symptoms. The treatment gains were maintained with persistent remission until the 18-month follow-up. This study highlights an effective high intensive CBT program for older adults with OCD and challenges the false assumptions that (a) psychological interventions are ineffective for older adults and (b) existing treatments are unsuited for older adults. Future research should investigate the effects of this program in large sample with sufficient power.
1 Theoretical and Research Basis for the Treatment
The current and lifetime prevalence of obsessive-compulsive disorder (OCD) among older adults varies between .59% and 4.5% (Grenier et al., 2019; Kirmizioglu et al., 2009; Klenfeldt et al., 2014; Pulular et al., 2013). This indicates that OCD is, together with generalized anxiety disorder and specific phobias, one of the most common anxiety-related disorders among older adults (Kirmizioglu et al., 2009). However, anxiety disorders and OCD are often missed or ignored in older adults (Bryant et al., 2008). Importantly, OCD has a negative impact on patients’ social functioning, family life, and activities in daily living (Porensky et al., 2009). These negative effects of OCD are greater than those of other anxiety disorders (Grenier et al., 2009). OCD most commonly develops between the ages of 20 and 30 years. Only 17.6% of older adults with OCD develop symptoms after age 60 (Grenier et al., 2009). This indicates that most older adults have a long duration of the illness, which likely negatively effects their treatment outcome (Grant et al., 2007). However, little is known about treatment options for older adults (Jazi & Asghar-Ali, 2020), and clinicians often adhere to the guidelines for adults aged 18–65 years.
The most studied and most successful treatment for adults aged 18–65 years with OCD is cognitive behavioral therapy (CBT), including exposure and response prevention (ERP; Rosa-Alcázar et al., 2008). ERP includes two components. First, patients gradually expose themselves to experiences that provoke their anxiety. Second, patients are instructed to suppress their compulsions and safety behaviors after having exposure therapy (i.e., response prevention; McGuire et al., 2015). Because it has been used successfully with younger adults, ERP is the first treatment choice for older adults. However, the use of ERP in older adults has not been well researched. For example, there has been no randomized controlled trial (RCT) of ERP in older adults with OCD (Hendriks et al., 2021). Only a few case studies have reported successful outcomes with weekly CBT, weekly CBT in combination with medication, and frequent CBT sessions in a clinical setting (Hendriks et al., 2008; Jazi & Asghar-Ali, 2020; Price & Salsman, 2010).
However, the effectiveness of ERP in older adults with a longstanding illness remains unanswered. Possibly, older adults have more residual symptoms after ERP treatment than younger adults (Carmin & Wiegartz, 2000). Even though ERP is the most studied and most successful treatment for adults aged 18–65 years (Foa et al., 2005), a significant proportion of individuals (i.e., 30–50%) do not benefit sufficiently from CBT, including ERP (Abramowitz, 2006; Kathmann et al., 2022). A lack of sufficient progress in treatment might be related to the severity of the patient’s symptoms or the presence of a comorbid personality disorder (Kathmann et al., 2022). Another possibility is that the CBT was not performed optimally (i.e., the treatment was not intensive enough, or the patient exhibited too much avoidance or too many safety behaviors during the ERP). Because not every patient benefits from CBT (including ERP), it is important to optimize current treatments.
One way in which CBT/ERP treatments could be optimized is through the use of an intensive treatment. In an intensive treatment, patients receive multiple sessions of therapist-guided ERP within a short period of time (i.e., one or two weeks) instead of weekly sessions across several months. During therapist-guided ERP, the therapist might notice subtle signs of avoidance or safety behaviors, of which the patient might be unaware. In addition, the therapist can assess the patient’s harm expectations, thereby allowing greater symptom reduction than self-guided ERP (Voderholzer et al., 2020). There are also other substantial benefits of an intensive treatment. First, our clinical routine outcome monitoring (ROM) data and a study of Pittig et al. (2021) found lower dropout rates (between 2.2% and 5.7%) for intensive treatments compared to those of other OCD treatments (between 10 and 15%; Pittig et al., 2021; Ong et al., 2016). Second, intensive treatments can overcome the stagnation observed in earlier treatments. This may be particularly relevant for older people with therapy-resistant symptoms. Third, intensive treatments result in faster responses to treatment. This, in turn, results in a shorter duration of the illness and a faster increase in the patient’s quality of life, thereby providing substantial public-health benefits (Pittig et al., 2021).
Intensive treatment programs have been evaluated for posttraumatic stress disorder (PTSD; Hendriks et al., 2018), anxiety disorders (Pittig et al., 2021), and OCD (Havnen et al., 2014). However, the studies did not focus specifically on older adults, for whom intensive treatment programs are often considered too burdensome. Moreover, the intensive treatment for OCD, which was evaluated among younger adults, was delivered in a group setting (Havnen et al., 2014). The present case study is, therefore, the first description of an individual high-intensive CBT/ERP treatment program for an older adult, who was diagnosed with OCD.
2 Case Introduction
A 72-year-old, married, white man was seen at a specialty center for the treatment of anxiety, OCD, and PTSD. His pseudonym is Max, which was chosen to maintain anonymity. Max was referred by his psychiatrist for a second opinion after having experienced treatment stagnation for two years. During the screening interview, Max indicated that he was suffering from symptoms of severe anxiety, which despite his request had not been addressed during his previous treatment. Specific anamnestic questions and a semi-structured interview (i.e., M.I.N.I.-5-NL; Overbeek et al., 1999) confirmed a diagnosis of OCD. When the OCD symptoms intensified, the patient also reported more severe depressive symptoms.
3 Presenting Complaints
During the diagnostic phase at our treatment center, Max mentioned that he had had symptoms of OCD since the age of 35. He also reported that his symptoms started while he was at work. Specifically, he declined to help with the installation of windows because he feared that they could fall out of their frames.
After a while, these symptoms decreased, but other fears emerged. For instance, whenever he heard a siren, he was afraid that he might have hurt someone. At the age of 46, Max feared hitting others while he was driving a car. As a result, he has not driven a car for 26 years. Because Max lived in a rural area, he was highly dependent on his wife for his mobility.
Max reported that his OCD symptoms had been present in a mild form since his young adulthood, but his symptoms had intensified during the last two years, without a clear explanation. He also mentioned that while often confined to his home during the COVID-19 pandemic, his symptoms intensified. During the diagnostic phase, Max’s most common obsession was his fear of hurting others or otherwise causing accidents. Max did not report a specific scenario, but a more generalized fear of hurting others. A prominent theme was a fear of going through a red traffic light and causing an accident, causing Max to avoid both driving a car and riding a bicycle. He also avoided walking alone and made sure that he would not encounter a traffic light on his route. Another prominent obsession was the fear of having a household fire. As a result, Max engaged in various checking behaviors, such as repeatedly checking whether doors and windows were locked and checking household appliances before leaving the house and before nightfall.
Although Max reported engaging in checking behaviors before leaving his home, his OCD symptoms were most prominent outside the house. He experienced anticipation anxiety (e.g., the fear of causing an accident that would cause harm to others), and he would ruminate about an experience for 15 minutes after he returned home. Max also actively listened for sirens and felt reassured when he had not heard one. Max’s anticipation anxiety was the greatest hinder because he felt like going outside was unsafe. He, therefore, avoided social activities and stopped doing volunteer work.
As a consequence of his avoidance, Max felt as if his world was getting smaller. He never wanted to hurt himself or to end his life, but he did describe his life as unsatisfying. He reported that when the OCD symptoms worsened, so did his depressed mood (e.g., guilt feelings). Max stated that his goal for the current therapy was to reduce his anxiety, avoidance, and compulsions to a level that it did not hamper his daily life anymore. Specifically, he indicated that he wanted to be a good father and grandfather again, by which he meant that he wanted to be able to help with chores and spend time with his grandchildren (e.g., playing soccer and biking).
4 History
Max grew up in an emotionally supportive family that included his mother, father, and brother. Max’s mother died when he was 15 years old. He described his mother as supportive, caring, and responsible. He mentioned that his father was unable to assume parenting responsibilities after his wife’s death. Accordingly, Max and his brother lived with other family members from whom they felt little emotional support. Max reported that the death of his mother and the subsequent changes in his life were traumatic at the time, but they did not negatively affect the rest of his life.
Max described his experiences in school as normal until he learned about his mother’s illness. Thereafter, he did not perform as well as previously, but he was able to finish high school. He had several friends, and no disruptive events occurred during puberty and early adolescence. Max is now married and has a son and a daughter and two grandchildren.
Max completed vocational training and then started his own decorating business, which he maintained despite suffering from OCD and related fears. In fact, he was able to continue until he retired at the age of 65. This was possible because he relinquished the driving responsibilities to an employee or his wife. Max also delegated work assignments for which he would be responsible if something went wrong to other employees.
Max reported two episodes of hypomanic dysregulation after he had started taking antidepressant medication. The first incident was in 1996 when he was taking clomipramine. He described this as a period where he was extremely hyperactive, and he thought that he could fly. Consequently, a psychiatrist advised Max to stop taking clomipramine and that he would not be allowed to obtain the medication again. Thereafter, Max’s symptoms abated without experiencing withdrawal symptoms. The second incident occurred in 2007 after Max started taking venlafaxine. Again, Max’s symptoms immediately decreased when he stopped taking the medication.
During the diagnostic phase of his treatment at our center, Max was taking venlafaxine, olanzapine, and Depakene (the latter because he was suspected of having a bipolar II disorder after hypomanic dysregulation on clomipramine and venlafaxine). Max indicated that he had not perceived a therapeutic effect from these medications. Instead, they seemed to intensify his fears and depressed mood. Max did not agree with the diagnosis of a bipolar II disorder, especially because his symptoms immediately abated when he stopped taking the antidepressant medication.
With regard to his psychiatric history, Max had received several psychological treatments, starting in 1996 (approximately 13 years after he developed his first symptoms). Although Max had consistently reported symptoms of OCD (e.g., his fear of causing an accident) since the age of 35, his treatment had been focused primarily on depressive symptoms (e.g., feeling sad or guilty about possibly hurting others). His therapists considered the OCD related symptoms to be beneficial (e.g., it is helpful to be cautious at work in order to prevent accidents) and, therefore, did not consider it to be a disorder. From the age of 48, Max’s treatment had included antidepressant medication, psychotherapy, creative therapy, Eye Movement Desensitization and Reprocessing (EMDR), and cognitive therapy, which included some ERP. In 1998, 2007, and 2018, Max had three relapses and received treatment in specialized mental health care. His relapse in 2018 was so serious that Max underwent two inpatient treatments, which were followed by day treatment. During his inpatient treatment, Max was medicated with venlafaxine (112.5 mg a day), but in view of his hypomanic episodes in the past, the medication was combined with olanzapine (10 mg a day) and Depakene. The goal was to prevent another hypomanic episode and to stabilize Max’s mood. The dose of Depakene was gradually increased to 500 mg, twice a day. The inpatient treatment also included EMDR for Max’s anxiety-related symptoms and CBT for his depressive symptoms. Moreover, Max was able to reduce some compulsions and avoidance through the use of CBT and ERP oriented treatment. For example, Max was able to take a bike ride with his therapist and then alone. In addition, he was also able to lock the door again, which was something he previously outsourced to his wife. This treatment, however, consisted only for a minor part of CBT/ERP, and it was secondary to the treatment for depression. Consequently, Max’s obsessions returned.
Max indicated that the previous treatments were not targeted at his primary goal (i.e., to reduce his recurring fears and anxiety). He believed that both professionals and laypeople had misunderstood his complaints. They labeled him as depressed, whereas he mainly experienced fear.
5 Assessment
As part of the standard clinical care, we confirmed the diagnosis of OCS according to the DSM-V (American Psychiatric Association, 2013) by using the M.I.N.I.-5-NL (Overbeek et al., 1999). The M.I.N.I.-5-NL is a semi structured interview to assess DSM diagnoses in a systematic way.
The Yale Brown Obsessive-Compulsive Scale (Y-BOCS; Goodman et al., 1989) was also administered by the therapist to assess the severity of Max’s OCD symptoms. His score on the Y-BOCS was 31 at the start of the treatment, which indicated severe OCD.
As a part of routine outcome monitoring (ROM), the Inventory of Depressive Symptomatology Self-Report (IDS-SR; Rush et al., 1996) and the Outcome Questionnaire (OQ-45; Lambert et al., 2006) were also administered at baseline, halfway through the treatment (i.e., after two weeks), and at the end of the treatment (i.e., six weeks after the start of the intensive CBT/ERP treatment). The IDS-SR assesses the severity of depressive symptoms in the past seven days. Even though Max did not meet the criteria for a depressive disorder according to the M.I.N.I.-5-NL (Overbeek et al., 1999), his score on the IDS-SR at the start of the treatment was 57, which is indicative of very severe depressive symptomatology. The OQ-45 is a self-report questionnaire widely used in outcome research to assess psychological problems and how people function in their daily life. Max’s score on the OQ-45 at the start of the treatment was 111, which indicated severe symptoms, which were disruptive of daily life.
6 Case Conceptualization
Max is a 72-year-old, married man with OCD. His symptoms have been present in a mild form since young adulthood. A possible life event that increased Max’s susceptibility to developing OCD is the loss of his mother at a young age, followed by placement in a unprotective environment (Fontenelle & Hasler, 2008). Max’s symptoms had increased during the last two years without a clear reason and further increased during the COVID-19 pandemic. His symptoms included obsessions (e.g., fear of hurting others or causing accidents and a fear of a household fire) and compulsions, including checking behaviors (observing sirens, checking household appliances). He also experienced anticipation anxiety and avoidance. Max’s compulsions served to maintain his OCD symptoms through negative reinforcement: engaging in compulsions (e.g., checking) brought relief from the distress that accompanied the obsessions (e.g., a fear of a fire or of hurting others; Abramovitch & McKay, 2016; Salkovskis et al., 1998). Because checking behaviors are effective in bringing about short-term anxiety relief, Max’s relied on checking behaviors to relieve his distress in the long term (Salkovskis et al., 1998).
Max’s avoidance behavior (e.g., not driving a car; his wife has driven the car for 26 years, not leaving the house alone, not going to social events) also maintained his OCD symptoms. Although avoidance is not necessarily considered a compulsion, it did serve the same maladaptive function of negative reinforcement in that it prevented Max from learning that his obsessions were unfounded (Abramowitz, 2006; Salkovskis et al., 1998).
Finally, family accommodation was a maintaining factor for Max’ symptoms in that his wife had assumed responsibility for many of the tasks that Max ordinarily would have performed, even though his wife mentioned that she was often not aware that she was taking over Max’s tasks. Similar to Max’s avoidance behaviors, family accommodation served the maladaptive function of negative reinforcement as it allowed Max to mentally and/or physically avoid fear-eliciting stimuli and situations, thereby reducing his anxiety and distress. This in turn, reinforced the idea that certain situations should be avoided (Kagan et al., 2017). Altogether the maladaptive behaviors maintained and possibly increased Max’s long-term distress.
Max’s goal for the therapy was to reduce his anxiety, avoidance, and compulsions to a to a level that they no longer interfered with his daily life. Max’s therapist explained to him that his OCD symptoms were being maintained through self-reinforcing mechanisms and, therefore, CBT (including ERP) was the chosen treatment. Because previous exposure-based treatments had not been successful, the goal was to optimize CBT through a high intensive CBT/ERP treatment over the course of one week, instead of the usual weekly sessions across several months. We discussed Max’s desire to break through his avoidance, and we judged him to be sufficiently motivated to participate in a high-intensive CBT/ERP treatment. In addition, Max was sufficiently vital to break through his avoidance behavior and had a good support system, including his partner and children. Altogether, we expected that the high intensive CBT/ERP treatment would result in a rapid treatment response.
7 Course of Treatment and Assessment of Progress
In accordance with the patient’s goal to reduce his anxiety, the treatment was focused on his OCD symptoms rather than his secondary depressive symptoms. We proposed a high-intensive CBT/ERP treatment for four days across one week (i.e., Thursday, Friday, Monday, Tuesday), followed by weekly, 90-min exposure booster sessions for four weeks. The treatment was an intensive form of individual CBT consisting of psychoeducation (i.e., in behavioral models of OCD, and explain how the treatment is linked to these models), exposure and response prevention (ERP), and CBT. The main focus, however, was on ERP. The ERP followed the inhibitory learning model (Craske et al., 2014). Significant others (e.g., Max’s wife) were also involved in the treatment and received psychoeducation on the importance of resisting family accommodation (Kagan et al., 2017). This treatment program is generally provided by a team of five therapists and is spread over the course of one week, instead of weekly sessions spread over a number of months. Given that the patient mentioned several side-effects (e.g., an affective flattening) since he started taking the medication but without any reduction in his anxiety, obsessions, or depression, we decided to evaluate the treatment after four weeks and to taper the medications if the intensive CBT/ERP treatment had a positive outcome.
Preparation Day
Before the high-intensive CBT/ERP began, the patient was invited for a session to prepare for the treatment. During the session, Max was very tense and indicated that it had been very difficult for him to leave his house. Thereafter, the therapist and Max thoroughly assessed his obsessions, compulsions, and triggers. Max reported that his anxiety was often elicited by encountering others (e.g., during a walk) and by operating household appliances (e.g., the television set or coffee machine). The internal cues that provoked Max’s anxiety included fearful expectations that he would cause harm to others by being negligent. During this session, the therapist also assessed Max’s harm expectancies. The patient reported that if he did not perform his rituals, he or other people would encounter a disaster or an accident (e.g., there would be a car accident or the house would burn down).
The therapist and Max also thoroughly assessed Max’s avoidance behavior, safety behavior, the short-term and long-term consequences of the avoidance and safety behaviors, and the goals of the therapy. Examples of Max’s avoidance behavior included not going to the playground with his grandchildren, not going outside, not driving a car, and not walking alone. Examples of his safety behavior included returning to check whether he had caused an accident and his going for a walk only with others. These examples of avoidance and safety behavior were provoked by the fearful expectation of causing harm to others. Max mentioned that his avoidance and safety behaviors resulted in a short-term reduction in his anxiety, but they intensified his symptoms in the long term. During the preparatory session, the therapist also provided psychoeducation, including behavioral models of OCD and how the treatment was linked to these models (see Section 6. For the case conceptualization). The therapist explained to the patient that he needed to confront his anxiety instead of avoid it. To this end, the therapist and the patient created a practice list whereby exposure assignments were written next to Max’s avoidance and safety behavior (e.g., going for a walk alone, going to the playground with his grandchildren). This list could be used during his exposure sessions.
Explanation of Treatment Day 1 Till 4
The first of the four intensive exposure days consisted of one 90-min session to devise an exposure plan for the coming day and to provide the patient with some additional psychoeducation. To devise the exposure plan, the therapist and Max used his practice list, from the preparatory session. Then, three guided-exposure, 90-min sessions followed. The exposure sessions might include different locations (e.g., at home, in the city, at the treatment center) aiming to conduct the guided exposure in a setting where the patient was suffering the most from his OCD symptoms. The exposures were designed to maximally violate harm expectancies and following the inhibitory learning model (Craske et al., 2014). The other three days followed a similar program: the days started with one session of 90 minutes in which to devise an exposure plan and were followed by three exposure sessions. During days Two, Three, and Four, the exposure sessions from the previous day were also evaluated. At the end of each exposure day and on the weekend, the patient was instructed to practice additional exposure assignments while alone.
Day 1 (Thursday)
During the first session on Day 1, Max indicated that he had already started to reduce his avoidance in that he had started to bike again. Together with the therapist, Max came up with an exposure plan for his first exposure day. They decided to proceed with biking and walking both with the therapist and alone.
During the guided exposure sessions (Sessions 2, 3, and 4), Max and his therapist actively sought out traffic lights and crowded places in order to activate and test Max’s intrusions (e.g., I fear that I will walk up to this woman and push her). Max concluded, however, that there wasn’t even enough time to hurt someone because people bike by very fast. He that his fear was unrealistic, and his fear that something had happened had already been abated. This exposure was repeated in different places, both with the therapist and alone. Max confirmed that practicing alone was difficult, but his harm expectancy became less credible because he repeatedly realized that he had not hurt someone. Next, Max and the therapist practiced biking. Prior to the exposure, Max feared that he would suddenly cut someone off, but when he started biking on a route without traffic lights, this was no longer a problem. Therefore, the therapist and Max sought out traffic lights in order to activate additional intrusions (e.g., I will bike through a red light and cause an accident). Max well understood the rationale for the exposure, and he was very motivated to participate. His homework assignment for the evening was to further walk alone in his neighborhood.
Day 2 (Friday)
Max’s wife was present for the first session on Day Two. The day started with an evaluation of the exposures on Day One. Max said that he learned a lot. Specifically, he was able to cope with his anxiety and confront his intrusions without acting on them. He learned that it takes a lot of time to execute a fear-inducing scenario (e.g., pushing someone) and that he did not act on his intrusions. As a result, his intrusions became less realistic. Max also mentioned that the session went so well that he thought he needed no further practice. The therapist, therefore, provided some additional psychoeducation about the rationale for the treatment and the importance of rehearsal (see also Craske et al., 2014; Craske et al., 2022). The therapist also explained how Max’s family accommodation was a maintaining factor for Max’ his OCD symptoms and explained that it was important that his wife would stop with accommodation by giving reassurance or taking over tasks (See also; Kagan et al., 2017). The therapist, Max, and Max’s wife concluded that she would continue driving the car, because Max first had to take driving lessons. They agreed, however, that all other forms of accommodation should stop. Moreover, they discussed the importance of involving their grandchildren in a later phase of the treatment. Finally, they devised an exposure plan for the day at Max’s home.
When the therapist arrived at Max’s home for Sessions Two and Three, Max was assigned the task of going to a supermarket to buy lunch. He practiced while biking and going through traffic lights. While Max was out of the house, the therapist chatted with Max’s wife who mentioned that she was very satisfied with Max’s treatment. She mentioned the long treatment history of Max and mentioned that they did not feel heard for a long time. The therapist also discussed that his wife had to leave after they had lunch, so that Max could practice on his own as well. When Max arrived home, the exposure therapy continued with holding a bottle of chlorine and operating some household appliances. Some examples included using a hairdryer and putting it on the bed (with the feared consequence of fire) and leaving the coffee machine on. At first, Max did not want to do these exposures as he thought that it would be a waste of energy and money. After repeating the rationale for the ERP treatment, Max admitted that he had been making an excuse, and he continued with the exposure.
The last exposure session of the day (session 4) involved Max being home alone for an hour with the coffee machine on, a bottle of chlorine open, and the hairdryer on his bed. During the exposure, Max was required to leave his house twice without checking the appliances. He was also not allowed to check when he arrived back home. When the therapist returned, Max mentioned that the exposure went well and he had learned that the coffee machine turns itself off and that the hairdryer does not cause a fire. In the end, the therapist and Max together devised exposure exercises for Max to practice during the weekend. They included walking and biking, visiting Max’s grandchildren, pouring them a drink, and repeating day’s exercises.
Day 3 (Monday)
The first session of the day started with an evaluation of the exposures from Day Two (Friday) and the homework exercises. Max indicated that they gone very well; he had done all of the exercises without any difficulty; and he had not avoided anything. He felt as if he now had the tools for dealing with his fears. His wife also mentioned that everything had gone well during the weekend. The therapist and Max came up with a new exposure plan for the day and agreed that Max would first practice alone walking and biking and repeating the exercises from the previous day. For the next sessions, the therapist would visit Max at home for additional guided exposure.
When the therapist arrived at Max’s home, Max again mentioned that everything was going well, but also that he had experienced severe relapses in the past and he was still afraid of relapse. The therapist therefore explained more about relapse prevention and again explained the importance of rehearsal (Craske et al., 2014, 2022). Max also said that he no longer avoided things, nor did he experience anxiety. When the therapist, however, probed more deeply, Max admitted that even though things were going well, he still experienced some fears and some anxiety. He also explained that it was very difficult for him when his wife was not at home because he was afraid that something bad would happen to her. The therapist and Max decided, therefore, to practice the guided exposure while his wife was elsewhere. The exposure consisted of using the bicycle carrier on the highway and on bumpy roads, without using unnecessary safety precautions such as checking buttons/bands, checking the mirrors and stopping multiple times to see check whether the bicycle carrier was still firmly attached. Max learned that nothing happened when he used his bicycle carrier in this manner. There were, however, also situations for which it would be difficult or impossible to develop in vivo exposures, for example, Max’s fear that his wife would not come home again or would die. Therefore, the therapist conducted an imaginary exposure that represented Max’s distressing thoughts or situations (Foa, 2010), and Max also wrote his own disaster scenario. His homework assignment was to reread his disaster scenario and to bike on an unfamiliar road.
Day 4 (Tuesday)
During the first session of the final intensive exposure, Max mentioned that he realized that his anticipation anxiety was greater than his actual anxiety during an exposure. He knew that he had to confront his anxiety rather than avoid it, and he also knew how to deal with his anxiety.
During the guided exposure sessions (sessions 2 and 3), Max practiced walking and using public restrooms to actively provoke the unwanted intrusions. Max indicated that the intrusions no longer arose spontaneously while he was walking or biking. He learned to walk toward people and to think “I’m going to hurt you” without experiencing fear. He knew that he was not going to hurt anyone or act on his intrusions, so he now realized that his harm expectancy was unrealistic. Nevertheless, Max stated that he was genuinely afraid of relapse. The therapist, therefore, reiterated the importance of rehearsal for relapse prevention.
During the fourth session that day, the therapist helped Max to devise an exposure plan for Max to use until his first booster session (e.g., visiting his grandchildren and pouring them a drink, going to the playground with his grandchildren, biking, encountering traffic lights). Max’s assignment was to practice the exposure assignments alone during the following week. In addition, the therapist and Max together created a practice jar with written exposure exercises for Max to practice each day.
Explanation of Booster Session 1–4
During the booster sessions, the therapist discussed the homework assignments. The therapist specifically checked whether Max avoided certain assignments and whether he completed them by using safety behaviors. The therapist and Max also discussed additional exposure assignments to practice alone during the coming week. This procedure was repeated each week until the fourth weekly booster session had been reached. During the booster sessions, Max along with the therapist worked on a plan for preventing relapse. Approximately one week after the last booster session, an evaluation was undertaken.
Booster Session 1
During Booster Session 1, Max reported that he had practiced diligently during the previous week, and he did not report any avoidance or safety behaviors. He had learned to accept certain risks in life, but he was still afraid that he would relapse. The therapist, therefore, reiterated the importance of rehearsal, and started to work on Max’s relapse prevention plan. They also discussed that Max should continue doing the exposure exercises as homework. The remaining time of the session was used to repeat some of the exposure exercises.
Booster Session 2
During Booster Session 2, Max and his wife reported that Max was doing very well. Max, in fact, was now involved in more activities, such as biking, and Max had completely relinquished his avoidance and safety behaviors. Using his bicycle carrier still caused Max the most distress, so Max decided to keep practicing this as homework. A prominent theme in the session was relapse and relapse prevention.
Booster Session 3
At the time of Booster Session 3, Max was still doing well. He mentioned that he might wanted to take driving lessons again. He no longer experienced aggressive intrusions, and he also wanted to become involved in more activities with his grandchildren, although this was a bit difficult due to the busy schedules of both his children and grandchildren. Max described himself as feeling 100% better than when he started treatment. He thought that this was due to the high-intensive CBT/ERP therapy, because he never had the feeling that his medication was effective in ameliorating his OCD symptoms. Accordingly and consistent with Max’s request, we started tapering his medication use in close consultation with Max’s his psychiatrist.
Booster Session 4
At Booster Session 4, Max was still doing well. He was continuing to taper his medication, and a consultation with his psychiatrist had been arranged for the same week. He was still using his practice jar to practice the exposure exercises and mentioned that these exercises were becoming easier for him. He continued to abstain from his avoidance and safety behaviors completely. Max was, however, still afraid of relapsing. During the session, relapse was discussed extensively, and the therapist and Max together completed Max’s relapse prevention plan. It was agreed that Max would continue practicing. His treatment would be evaluated in three weeks.
Assessment of Max’s Progress
Max’s OCD and depressive symptoms were assessed at several points during the treatment (i.e., after the first four intensive exposure days, at the end of the treatment, and at the three, six, twelve, and eighteen-month follow-up). Max’s score on the Y-BOCS decreased from 31 at the start of treatment, to 8 after the first four days of intensive treatment. This indicated that the OCD symptoms were already in remission (see Figure 1; Veale et al., 2021). His IDS score had decreased from 57 at the start of the treatment, to 4 after the first four days of intensive guided exposure. The latter score falls well below 13, which indicates the absence of depressive symptoms (Rush et al., 1996). Y-BOCS scores from baseline until 1.5 year follow up.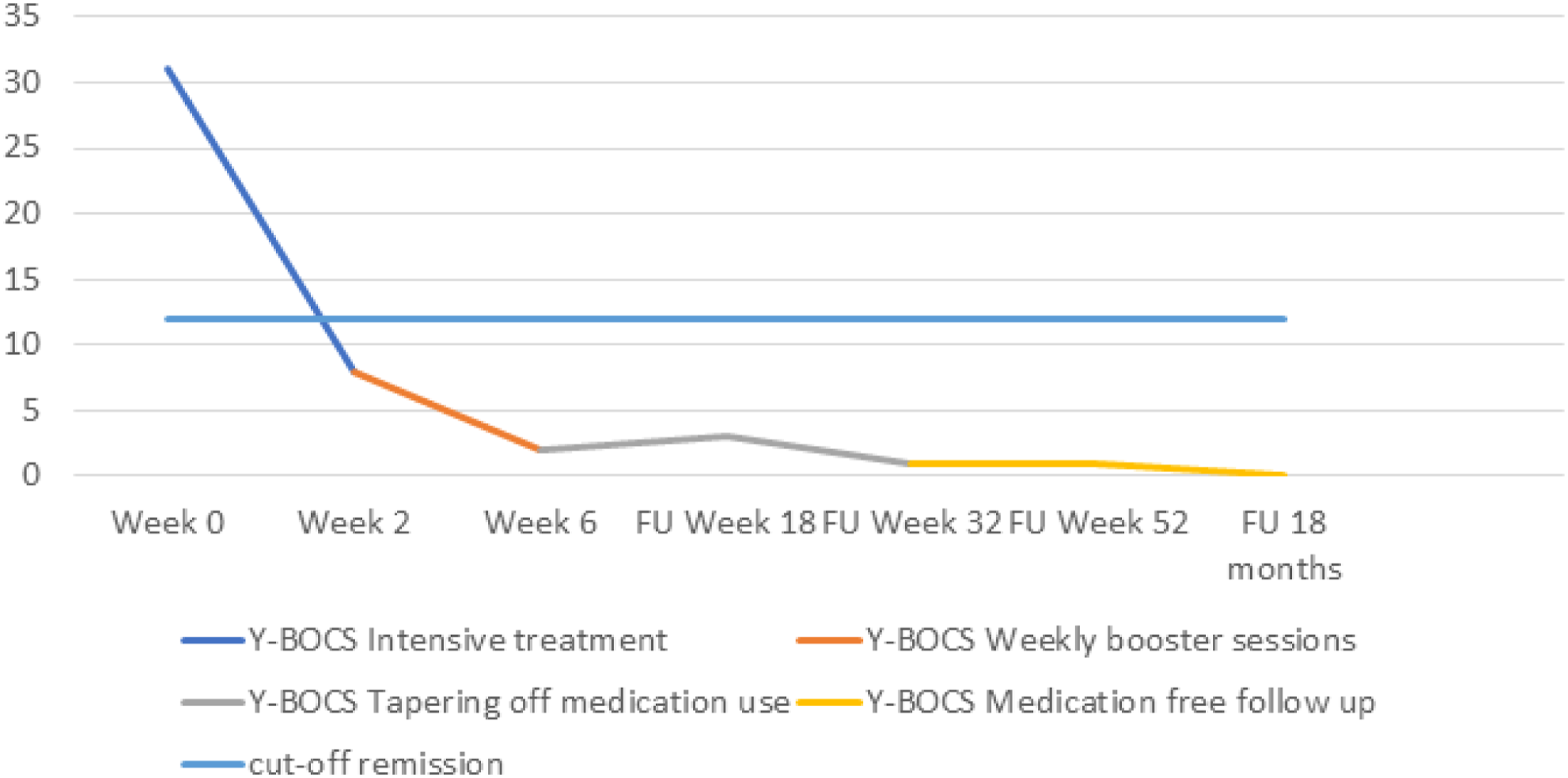
At the time of the treatment evaluation (six weeks later), there was an even larger reduction in the OCD and depressive symptoms (see Figure 1). The Y-BOCS score at the end of the treatment was 2, which falls well below the recommended cut-off of 7 for a clinical diagnosis (Fisher & Wells, 2008). The IDS-SR score at the end of the treatment was only 1.
The OQ-45 score had decreased from 111 at the start of the treatment to 30 at the time of the treatment evaluation. This was within the normal range and indicated a clinically significant decrease in disease burden (de Jong et al., 2007). Max remained motivated during the entire treatment, and he had been able to eliminate most of his avoidance and safety behaviors. His functionality had also improved, and he was, for example, able to see his grandchildren again.
8 Complicating Factors
A complicating factor in the case of this patient was the scarcity of research on OCD treatments in older adults. Most studies have evaluated weekly CBT/ERP or intensive CBT/ERP for the treatment of OCD among adults of working age (Carpenter et al., 2018; Havnen et al., 2014). Other studies in older adults focused on other mental disorders and indicated that older adults respond just as well, or even better to psychotherapy than younger adults (Chaplin et al., 2015; Cuijpers et al., 2020; Segal et al., 2018). However, except for a few case studies (e.g., Hendriks et al., 2008; Price & Salsman, 2010), there has been insufficient research on CBT/ERP in older adults with OCD (Hendriks et al., 2021). In fact, there have been no studies that have focused on the effectiveness of a high-intensive CBT treatment for OCD in older adults. In view of the positive effects of intensive CBT programs in the younger population (Havnen et al., 2014; Hendriks et al., 2018; Pittig et al., 2021), we decided to expand the treatment to include an older adult.
Another complicating factor was Max’s medication use and his hypomanic episodes in the past. At the time of the diagnostic phase, Max used Venlafaxine, Depakene (Valproic acid), and Olanzapine. He reported several side effects, such as sedation and concentration problems, while also reporting no therapeutic benefit of these medications. He also reported two hypomanic episodes in the past after having taken antidepressant medication for which he was previously diagnosed with a bipolar II disorder. This was the reason why Depakene and olanzapine had been prescribed. However, Max mentioned that his hypomanic symptoms immediately decreased when he stopped using the antidepressant medication. He also mentioned that he had never experienced other (hypo)manic episodes in the past. According to the DSM-IV-TR (American Psychiatric Association; APA, 2000), Max’s symptoms were not sufficient for diagnosing him with a bipolar disorder. However, such a decision is more nuanced in the DSM-5 (APA, 2013), and some studies strongly argue that patients who experience antidepressant-induced hypomania are truly bipolar (Chun & Dunner, 2004). According to the DSM-5 (APA, 2013), a hypomanic episode that emerges while a patient is taking antidepressant medication and which persists beyond the physiological effect of the treatment, is sufficient evidence for a hypomanic episode and thus a bipolar II disorder. Max’s symptoms immediately decreased after he stopped taking the antidepressant medication; therefore, the episode did not persist beyond the physiological effect of the antidepressant medication. Moreover, the depressive symptoms decreased after the first four days of exposure treatment and paralleled the reduction in the OCD symptoms. This suggested that the depressive symptoms were secondary. We discussed this at length within the treatment team. We concluded that this information, together with the fact that Max never reported further (hypo)manic episodes in the past, confirmed that there was insufficient grounds for a bipolar II diagnosis. It was, moreover, clear to the patient, his wife, and his psychiatrist that his hypomanic episodes had been medication induced. Max himself also felt like his medication was not useful in decreasing his OCD symptoms. Hence, Max started tapering his medication use in close consultation with his psychiatrist.
A final complicating factor was that the high-intensive CBT/ERP treatment took place during the COVID-19 pandemic. Because of Max’s age, he was at greater risk of severe disease following a COVID-19 infection than younger people (Chen et al., 2021). We discussed at length how we could carry out the treatment with Max in a safe manner. We adhered to the national guidelines for the prevention of COVID-19 infections. This included among other things staying at home and obtaining a test when the therapist showed potential signs of being infected his or himself. We also maintained a 1.5-m distance from the patient or wore a face mask when maintaining the minimum distance was not possible.
9 Access and Barriers to Care
The greatest barrier to the care would have been having stereotypical ideas about older adults. Examples include the belief that older adults are too old to change, or that older adults benefit less from psychological interventions than adults of working age (Kessler & Blachetta, 2020; Laidlaw & Baikie, 2007). Therapists regularly strive to maintain a supportive attitude in their work with older adults. They strive for a harmonious therapeutic relationship by adopting a cautious and less confrontational style (Boschann et al., 2022). In the case of OCD, this tendency not to confront the patient with his or her anxiety might lead to the erroneous assumption that exposure treatments, and especially an intensive CBT/ERP based treatment, would be too burdensome for older adults. It is, therefore, regularly assumed that available treatments would not be suitable for older adults (Boschann et al., 2022; Chew-Graham et al., 2012). Consequently, older adults are two-to-three times less likely to be referred for psychological treatment than younger adults (Mackenzie et al., 2012; Pettit et al., 2017).
Additionally, anxiety disorders are often missed or ignored in older adults (Bryant et al., 2008). When an individual is diagnosed with a comorbid depressive disorder, the symptoms related to anxiety are often seen as secondary, and the treatment is usually targeted at the depressive symptoms (Schoevers et al., 2008), which had also been the case with Max. Thus, his OCD symptoms had remained untreated for a long time. These diagnostic problems complicated Max’s referral to an appropriate treatment.
10 Follow-Up
As stated previously, Max’s OCD symptoms were assessed at the three-, six-, twelve-, and eighteen-month follow-up. Three months after treatment had ended, Max’s score on the Y-BOCS was 3. Max also discontinued his medication at three-month follow-up.
At the six-month follow-up, Max’s score on the Y-BOCS was 1. This was well within the normal range and shows that Max had continued to progress after the treatment had ended (Fisher & Wells, 2008). At the 12-month follow-up, Max’s score on the Y-BOCS was still just 1. His follow-up scores were lower than at pretreatment and also lower than they were at the initial evaluation (see Figure 1). At the 18-month follow-up, Max’s score on the Y-BOCS was 0. By then, Max indicated that he was free of the obsessions, compulsions, and avoidance behaviors.
11 Treatment Implications of the Case
There has been very little research on OCD treatments for older adults (i.e., Hendriks et al., 2008; Price & Salsman, 2010), and there has been no evaluation of a high-intensive CBT/ERP treatment for older adults. The present case study is the first description of an individual high-intensive CBT/ERP treatment for an older adult with OCD. Results from both the treatment and the follow-up indicate that the treatment was effective, with the patient’s OCD symptoms already in remission the first four days of the treatment. These positive results are consistent with prior research that investigated this intensive treatment in adolescents (Eenink et al., 2019), and they add to the limited research on OCD in older adults. Even though we cannot generalize these results to the population of older adults, this case study illustrates that a high-intensive individual CBT/ERP treatment based on psychoeducation, ERP, and CBT is highly effective in an older adult.
This study also shows that CBT/ERP can be effectively applied in a team-setting with therapist rotation. This has previously been investigated only in the case of PTSD (Van Minnen et al., 2018). By implementing the high-intensive CBT/ERP therapy by a team of five therapists, patients can acquire new associations in a variety of therapeutic contexts, and this would appear to strengthen their learning experiences (Craske et al., 2014, 2022). The present study lends further support to Van Minnen et al.’s (2018) finding that alternating therapists during treatment for OCD serves to augment the effectiveness of the treatment.
Previous case studies on OCD in older adults have reported successful CBT/ERP treatment responses; however, this might have been due to the low severity of the OCD and a short duration of the illness (e.g., Price & Salsman, 2010). The present study confirms that a high-intensive CBT/ERP treatment is effective for a severe case of OCD that included significant functional impairment and multiple episodes of inpatient treatment, even though the illness was of long duration (more than 35 years). Illness duration does thus not form a barrier for treatment success in a high-intensive CBT/ERP treatment for OCD. In a similar way, our study illustrates that age does not have to be a barrier for treatment success. Even though stereotypical beliefs about older adults (See Boschann et al., 2022; Chew-Graham et al., 2012) are common, the present study suggests that there is no basis for these beliefs. Finally, this study illustrates that a high-intensive CBT treatment is capable of breaking through stagnation arising from previous treatments, yielding a rapid treatment response (Pittig et al., 2021).
This case study serves as a preliminary step for research on intensive treatments for older adults. In view of the positive effects of the treatment for a 72-year-old adult with OCD, larger samples should be used to investigate the effects of intensive CBT treatments for older adults with OCD. In addition, it would be fruitful to evaluate the effects of intensive CBT/ERP treatments for other anxiety-related disorders, such as panic disorder, social anxiety disorder, and PTSD. Inasmuch as earlier studies with younger populations have yielded positive results (Hendriks et al., 2018; Pittig et al., 2021), it would be fruitful to extend these studies to include older adults. This is especially relevant, given that it is to be expected that anxiety and anxiety-related disorders become increasingly prevalent among older adults (He et al., 2016).
12 Recommendations to Clinicians and Students
The case study presented here confirms the successful application of a high-intensive CBT treatment. We recommend that therapists who see clients needing relief from OCD become trained in CBT and ERP. To become skilled in delivering intensive treatments, we recommend pursuing an intensive training program, readings the relevant theories, obtaining regular supervision, and regular team meetings throughout the treatments. A thorough understanding of the rationale for exposure therapy is needed to help motivate the patient to eliminate avoidance and safety behaviors. On top of regular team meetings, we also recommend short meetings between the therapist who starts the intensive exposure day (i.e., session one) and the therapist who performs the guided exposure sessions (i.e., session two, three, and four).
Our center is specialized in the treatment of anxiety, OCD, and PTSD. In our experience, we noticed that the high-intensive CBT treatments work best if patients are familiar with exposure techniques. The decision to initiate an intensive CBT treatment should always be made in consultation with the patient and an experienced psychologist or psychiatrist. When a patient is referred to us without having had a previous treatment or without prior experience with exposure, we usually recommend a protocol-based OCD treatment for the patient to become familiar with the basic principles of exposure. If a regular, protocol-based treatment is insufficiently effective, it is possible to intensify the CBT treatment (e.g., using stepped care; Bower & Gilbody, 2005). Intensive treatments have been promising, but for many patients a regular protocol-based CBT treatment is sufficient (Foa et al., 2005). We, therefore, recommend that clinicians thoroughly review each patient’s treatment history before discussing treatment options and follow a stepped care procedure (Bower & Gilbody, 2005).
Additionally, we recommend clinicians to actively reflect on their work with older adults (see Lilienfeld & Basterfield, 2020). Many clinicians assume that existing treatments are not suitable for older adults (see also 9; access and barriers to care), and this negatively impacts their clinical decision-making. For example, a therapist might assume that an exposure-based treatment would be too burdensome for older adults or that older adults would not benefit from having an ERP treatment (Boschann et al., 2022; Chew-Graham et al., 2012). The present case study confirms that old adults can, in fact, benefit from CBT with a main focus on ERP. Through reflection and experience (Lilienfeld & Basterfield, 2020), clinicians might overcome their biases regarding older adults. Based on our experience, therapists should not hesitate to use evidence-based treatments in older adults.
As stated, intensive treatments have been shown to be effective with the younger people (Eenink et al., 2019; Havnen et al., 2014). Through the present case study, we have also demonstrated the effectiveness of a high-intensive CBT/ERP treatment in an older adult and we preliminarily expand these findings to the older population. We therefore carefully argue that therapists can learn similar treatment approaches that generalize across the population, rather than having to learn multiple treatments for people of differing ages. Although the results of this initial case study are promising, it is unknown whether the results can be generalized to other older adults with OCD. Therefore, it is even more important to use high-intensive guided CBT/ERP only after intensive training, consideration of treatment history, careful case conceptualization, and after consulting with other clinicians, - which is a standard step we take at our expertise center. Hopefully, future studies will confirm that intensive CBT is indeed effective for a wide range of older adults with OCD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.