
Abstract
Functional neurological symptom disorder (FND) is associated with complex specialist investigations and poor prognosis. The theoretical understanding of FND posits that functional symptoms are predisposed by both psychological factors, including attachment disturbances and childhood trauma, and biological factors such as neuroplasticity and epigenetics. Current treatment recommendations include psychological therapy, with moderate effects observed with cognitive-behavioural therapy and psychodynamic therapy modalities, however, psychological understanding is key to success. The current case report describes cognitive analytic therapy (CAT) with a 68 year-old woman presenting to services with diagnoses of FND and borderline personality disorder (BPD). The target problem for therapy was integration of fragmented self-states (dissociative and driven) pertinent to both FND and BPD. 16 session CAT was delivered, with four follow up sessions, exploring unhelpful patterns of relating with self and others, based on an unconscious repertoire of internalised patterns and procedures from early life. CAT tools were used to facilitate change; reformulation and ending letters, mapping and the therapeutic relationship. Scores on the personality structure questionnaire (PSQ) and an idiosyncratic measure of state-shifting indicated positive outcomes, sustained at 3 month follow up. This shows modest early acceptability and feasibility of CAT for working with comorbid BPD and FND, providing a validating and blame free formulation of the development and maintenance of symptoms. Additional measures would have improved the ability to comment on the effectiveness of the treatment and future research implications are discussed.
Keywords
1. Theoretical and Research Basis for Treatment
Functional Neurological Symptom Disorder
Functional Neurological symptom Disorder (FND; American Psychiatric Association, 2013) is a broad-spectrum disorder, including nonepileptic seizures, sensory symptoms, cognitive impairments, sleep disorders mimicking insomnia and parasomnia, and movement disorders such as tremors, limb weakness and dystonia (Espay et al., 2018). Other functional symptoms, such as fatigue, headaches and bowel symptoms are extremely common alongside FND (Stone et al., 2020).
FND has a high index of psychiatric comorbidity and is associated with attachment disturbances and traumatic life events (Ludwig et al., 2018; Brown & Reuber, 2016). Dissociation, including depersonalisation and derealisation, is commonly observed within FND, and is linked to a dysregulation of our nervous system typically caused by trauma and interpersonal disturbances (Moenter, 2020). Therefore, FND symptoms have been understood as an extreme dissociative state within post traumatic stress disorder (PTSD) (Fiszman et al., 2004; Gray et al., 2020), due to extreme arousal prompting neural pathways necessary for regulating emotions to cut off (Gupta, 2013). Indeed, recent practice-based evidence suggests that interventions for a primary diagnosis of PTSD can incur secondary change in FND symptoms; prolonged exposure therapy used in the treatment of PTSD symptoms in a 64 year old woman was pivotal in treating functional aphasia and paraplegia as she no longer met the diagnostic criteria for FND following intervention (Putica et al., 2022), and similarly using prolonged exposure to treat comorbid psychogenic nonepileptic seizures and PTSD symptoms in a 52 year old male caused his seizures to stop altogether, which was maintained for 2 years (Myers & Zandberg, 2018).
The current guidelines for the treatment of FND and other functional symptoms involve a multidisciplinary team approach, in which physiotherapy or rehabilitation may help to ‘retrain the brain’, as well as psychological therapy supporting adjustment and understanding of the development and perpetuating factors (Stone et al., 2020). Regarding the effectiveness of psychotherapy for FND, a recent systematic review found Cognitive Behaviour Therapy (CBT) and Psychodynamic Therapy (PDT) both show moderate improvements in mental and physical health symptoms (Gutkin et al., 2021). Although direct comparisons between the efficacy of CBT, PDT or treatment as usual could not be ascertained due to the methodological weaknesses and small number of randomised control trials undertaken. The researchers did remark that the barriers to both therapeutic interventions were dependent on how invested the patient was in a psychological narrative regarding their symptoms. Thus, introducing scope for interventions primarily targeting previous trauma, attachment or interpersonal disturbances, and PTSD symptoms, with the potential for secondary reductions in FND symptoms.
Personality Disorders
The DSM-5 stipulates that individuals who meet diagnostic criteria for a personality disorder have impairments to their identity, self-direction, empathy, intimacy, and functioning, with several categories of personality disorder existing (American Psychiatric Association, 2013). Although these diagnostic criteria enable research into the impact and treatment of personality disorders, the language and pathologising of one’s personality in this way is heavily criticised. Firstly, the categorical model of personality disorders invites questions regarding validity with overlapping symptoms and presentations such as complex PTSD (Campbell et al., 2020). Secondly, stigma and negative attitudes cloud the diagnostic category, specifically borderline/emotionally unstable presentations (BPD/EUPD; Loader, 2017). However, the diagnostic framework is relied on heavily when developing presentation specific treatments.
The Multiple self-states model (MSSM; Ryle, 1997) conceptualises the symptoms of BPD, including shifting between self-states and emotional dysregulation as methods of dissociation. The model describes levels of self-development, and was created by the founder of Cognitive Analytic Therapy (CAT). The MSSM posits that if an individual develops a restricted repertoire of relational patterns, due to inconsistent or harmful interactions with caregivers in their early years, the development of Self is negatively impacted. Thus, the Self becomes fragmented and disconnected, rather than integrated (Ryle, 1997). This limits self-reflexivity later in life, perpetuating harmful patterns without the ability to recognise and change unhelpful patterns and procedures.
Cognitive Analytic Therapy
CAT was developed as a bridge between psychoanalytic therapy and cognitive therapy, creating a relational intervention which is integrative in nature and time limited. Object relation’s theory (ORT; Ogden, 1983) influenced Ryle’s thinking as he developed CAT; understanding that relational difficulties in present day are shaped by our early relationships with important others in our lives. Therefore, CAT is built on the concept of reciprocal role procedures (RRPs), referring to relational positions that have been internalised as one interacts with others during early development; for example, abusing---hurt or nurturing---supported (Ryle & Kerr, 2020). These RRPs build a complex internal framework of relating, providing a repertoire of RRPs which are activated during interpersonal and intrapersonal interactions. This repertoire of relational procedures describes one’s identity development, with positive and coherent RRPs contributing to an integrated self, however, chaotic, negative or inconsistent RRPs create an incoherent and fragmented self (Ryle, 1997). This echoes the theoretical positions of FND, PTSD, and personality difficulties, which draw importance from early attachments and experiences with caregivers.
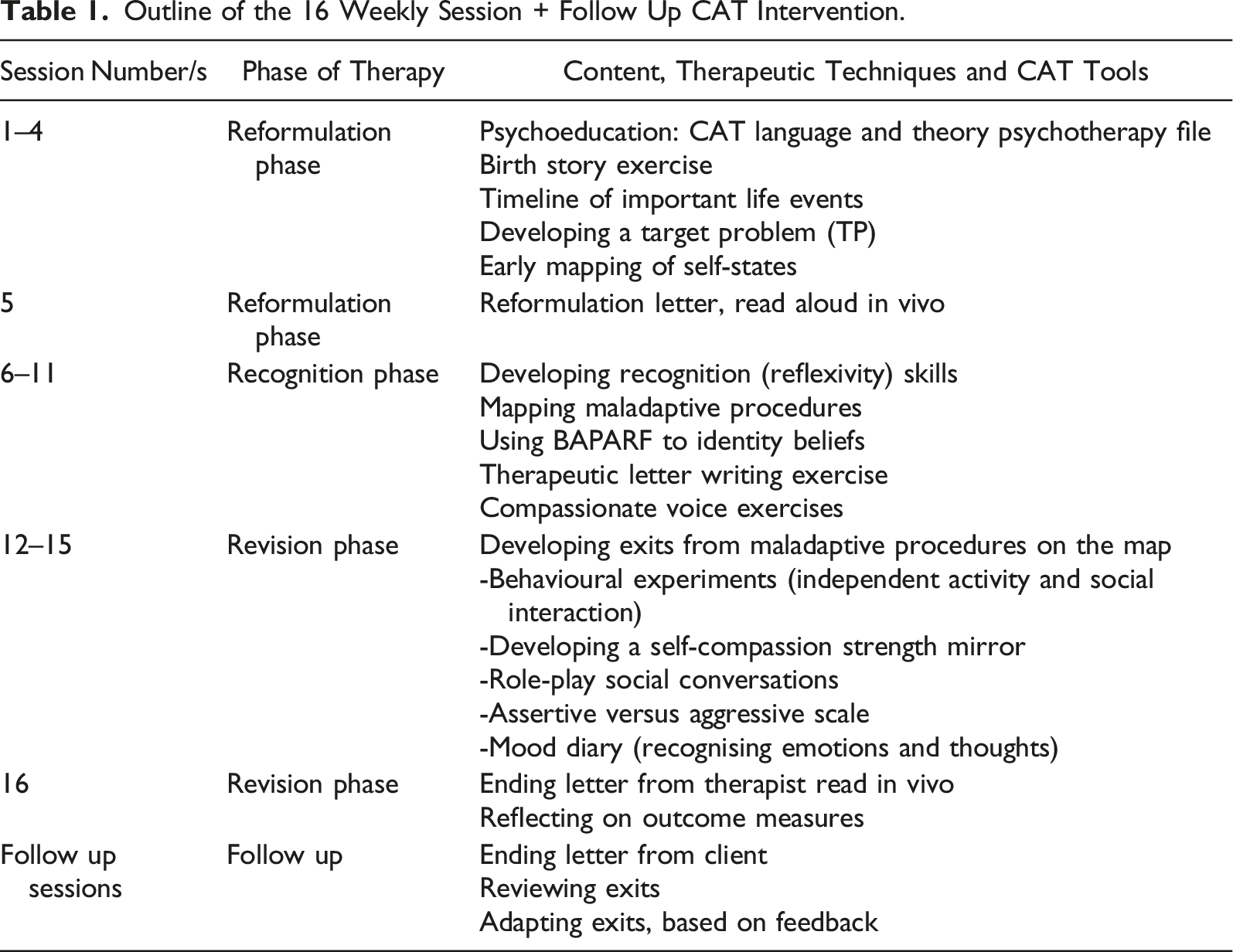
CAT is typically a 16 or 24 session intervention dependant on complexity, with follow up sessions after a period of consolidation. CAT follows the 3 R’s; the reformulation phase typically within sessions 1–4 (describing the target problem, understanding early relationships and hypothesising patterns), the recognition phase within sessions 5–12 (noticing relational patterns, mapping these out with the therapist, and developing recognition skills) and the revision phase within sessions 13–16 (identifying and consolidating exits from the unhelpful patterns identified in the recognition phase) (Ryle & Kerr, 2020). Key CAT tools include the psychotherapy file which is a questionnaire used to aid recognition of relational patterns termed traps, dilemmas and snags, sharing letters with clients in vivo (reformulation and ending letters), and visual mapping of procedures (referred to as a sequential reformulation diagram; SDR) (Ryle & Kerr, 2020).
Research into the efficacy of CAT is in its infancy and large-scale randomised control trials are lacking, however, case studies and single case experimental designs provide a wealth of insight into the flexibility and transferability of the CAT model. A review calculated a weighted effect size of d = 0.83 (95% confidence interval) from 11 CAT outcome studies (Calvert & Kellett, 2014), indicating a positive, large effect on reducing psychiatric symptoms. CAT has shown good outcomes with OCD (Kosti et al., 2008; Ameri et al., 2017), depression and anxiety (Katsigiannopoulos et al., 2008; Wakefield et al., 2021) and paranoia (Kellett & Hardy, 2014). One area that CAT has proven most useful is with individuals with personality disorders (Dasoukis et al., 2008; Livanos et al., 2008; Kellett, 2007). In addition, some practice-based evidence exists concerning the utility of CAT with physical health conditions, such as frontal brain injury (Yeates et al., 2008) and diabetes (Fosbury & Coles, 1994). Regarding the older adult population, CAT has been shown to be effective at significantly reducing symptoms of anxiety and depression in a sample of over 65s (Williams & Craven-Staines, 2017). Moreover, CAT has been used with good effect with carers of those living with dementia (Hamill & Mahony, 2011) and individuals with a diagnosis of Alzheimer’s Disease and a history of trauma (Sutton, 2003). Research demonstrating the potential for CAT with older adults is limited, therefore, this case report aims to invite further dialogue on the applicability and utility of CAT with older adults.
2. Case Introduction
Rose (pseudonym), a 68-year-old white, heterosexual cisgender female attended an older adult mental health service for assessment. Rose provided informed written consent, in which she agreed to anonymised details of her assessment, care and treatment being disseminated for the purpose of research, teaching and clinical skills training. Specific details have been changed to protect her anonymity and the content within this case report was discussed and reviewed with her prior to submission.
3. Presenting Complaints
At the time of referral, Rose was concerned about declining short-term memory, changes in attention and concertation, anxiety, and difficulties with sleep. She believed that she had dementia and had started to tell friends and family that she had Alzheimer’s Disease as a way of explaining her symptoms. These cognitive symptoms had persisted for several years, however, Rose thought they were becoming worse with age.
Rose was visibly anxious and reported feeling muddled during assessment. She described either having racing thoughts or feeling ‘cut off’ from everything within her first assessment session, making it difficult to engage in dialogue. Rose described engaging in activities such as excessive cleaning when feeling anxious to ‘keep busy’ and avoid her thoughts. Rose understood this in the context of BPD, as she found it difficult to regulate her emotions and often dissociated as a way of coping with strong feelings or memories.
Rose reported ongoing PTSD symptoms, including rumination around specific memories from childhood. These included instances in which she felt neglected and overlooked by her mother, and violent assaults perpetrated by her step-father. These ruminations occurred at night, usually involved ideas about escaping or re-imagining what she might say as an adult in those situations and disrupted her sleep. Rose also reported hypervigilance, specifically within social interactions when Rose experienced a potential threat of rejection or harm.
Rose reported a reduction in social and physical activity outside the home. Her husband stated this was his main concern as he observed his wife become increasingly isolated and noticed a reduction in her independence and confidence. Rose described avoiding social interaction due to feeling inferior compared to her peers, which prevented her from engaging in conversation or meeting new people. She described ‘cutting off’ from the world gradually as she got older, and subsequently felt lonely which triggered memories of early experiences of being different and ‘on the outside’. Relationally, Rose and her husband also reported increased conflict as he felt frustrated with her symptoms and at times struggled to understand and support Rose.
4. History
Rose reported a significant history of childhood physical, emotional and sexual abuse and experienced being removed from her family home for spells and placed into the care system. Rose’s mother reportedly experienced long episodes of depression throughout Rose’s childhood, and her stepdad was an alcoholic. Rose never met her biological father, and only found out that the man she believed to be her biological father was her stepdad when he was dying, and Rose was an adult. Rose went on to leave home as a teenager and married a man who later became violent and repeated those early experiences of abuse. Rose has no contact with her own siblings or extended family, and her parents are now deceased.
Rose’s inconsistent start understandably impacted her early education, however, in later life she returned to college to train as a social worker. This career was built on her caring and compassionate nature, however, she often found herself struggling to maintain boundaries with patient’s emotional pain which led to burn out. At this time, she had remarried and lived happily with her current husband. The couple were not able to have children, something which Rose found increasingly difficult as she aged.
Rose received episodes of inpatient and community mental health support as an adult, during which time she received working diagnoses of anxiety and depression (aged 20 on entry into adult services), PTSD (aged 32), and BPD (aged 54). Rose’s diagnosis of PTSD was historic, relevant at the time due to sleep disorder, nightmares, hypervigilance, and flashbacks. At present, Rose experienced no flashbacks or nightmares, however, disordered sleep, rumination and hypervigilance persisted as well as core beliefs about worthlessness and her identity related to traumatic events. In the last 10 years she had engaged in psychological therapy for PTSD symptoms and anxiety through CBT and recalled discussing trauma and attachment within psychodynamic and EMDR modalities in her 30s–40 s. Rose had trialled an extensive list of psychotropic medication with little positive effect.
Physical health records indicated that Rose was assessed 10 years ago for similar cognitive symptoms, with no organic cause identified at the time. During this time she had been seen by neurology and the specialist regional sleep service and given a diagnosis of functional neurological symptom disorder (FND), including functional sensory symptoms, cognitive symptoms and sleep problems. Rose’s medical records also identified many hospital assessments and stays for difficulties with her bowel and stomach, for which physical causes were continuously ruled out. She was currently accessing investigations for stomach pain, bloating and digestive difficulties through the local hospital.
5. Assessment
A full neuropsychological assessment including tests of executive functioning (DKEFS and WAIS), fluency and verbal comprehension (WAIS and DKEFS), perceptual reasoning (WAIS) and verbal and visual memory (WMS) was conducted and compared to previous testing completed several years prior. This indicated no significant change in performance, therefore alongside normal neuroimaging (MRI and DAT scans), an underlying organic cause was ruled out. Rose’s cognitive profile suggested difficulties with sustained attention and processing speed, as well as specific areas of weakness with visual and verbal memory. This is consistent with cognitive impairments associated with trauma, and comorbid depression and anxiety (Koopowitz et al., 2021).
Based on psychiatric history and a lack of cyclic patterns, a diagnosis of bipolar disorder was ruled out, and Rose was consequently diagnosed by a Consultant Psychiatrist in the team with functional cognitive symptoms as part of a complex PTSD and BPD presentation.
6. Case Conceptualisation
Rose’s symptoms were understood as comorbid BPD and PTSD, with her emotional experiences closely connected to her functional symptoms. Her early experiences of neglect and abuse caused a restricted repertoire of RRPs, as abusing---abused, controlling---controlled and neglecting---neglected became familiar. This influenced how Rose developed her sense of self and expectations of how relationships with others should look and feel. Subsequently, Rose developed different self-states that provide short term protection from painful memories and emotions, however, prevent her from being present and forming more helpful and healthy relational procedures. Rose had several protective factors too which enabled her to engage in psychological therapy; supportive husband, established links with people she used to volunteer with, she lived in a well-connected community with supportive neighbours, and had access to outdoor space and enjoyed gardening.
Rose had undergone other psychological interventions with differing efficacy in the past which had been predominantly symptom based. She requested an intervention with a focus on withdrawal from others and conflict with her husband, as well as emotional regulation. CAT was deemed appropriate following this discussion, given the important analytic components and recognition skills she wished to prioritise. CAT also provided the flexibility to adapt to cognitive symptoms as written and visual resources acted as memory prompts. During neuropsychological testing Rose’s estimated pre-morbid functioning was within the average range, therefore, any adjustments to therapy were made based on the specific cognitive areas of weakness identified within testing rather than global intellectual functioning delays which her account of disrupted schooling may have suggested.
Therefore, Rose was offered Cognitive Analytic Therapy (CAT) working with a senior clinical psychologist who was a trainee CAT practitioner at the time. The primary aim for therapy was dictated by Rose’s desire to work on integration of self-states (the busy and cut off states) and relationships with others. However, a secondary aim of therapy involved exploring FND symptoms and previous trauma.
7. Course of Treatment and Assessment of Progress
Outline of the 16 Weekly Session + Follow Up CAT Intervention.
Measures
The Hospital Anxiety and Depression Scale (HADS) was administered during Rose’s assessment as the standard screening measure used in the older adults CTT. The HADS has been deemed valid and reliable in assessing caseness for both anxiety and depression; Cronbach’s alpha for the HADS-Anxiety subscale is 0.83 and for HADS-Depression is 0.82 and high positive correlations have been detected between the HADS and measures assessing the same constructs (Bjelland et al., 2002).
The Personality Structure Questionnaire (PSQ; Pollock et al., 2001), an eight item self-report questionnaire designed for use in CAT, was used to help identify structural dissociation following Rose’s statement about fluctuating moods and presentation. This was completed pre-therapy (assessment session), mid-therapy (session 8), post-therapy (session 16) and at 3 month follow up. PSQ scores can range from 8–40; patients diagnosed with personality disorders typically score over 30 and community samples approximately 20 (Bedford et al., 2009). The PSQ has good reliability and validity and is used widely in CAT practice-based-evidence research (Pollock et al., 2001), with a Cronbach’s alpha coefficient of 0.87 (Bedford et al., 2009).
Finally, an idiographic measure of state shifting was developed during the first few sessions of therapy. Rose created a scale from −10 (describing an intense flat state) to +10 (describing an intense hyper state), with 0 denoting the ‘middle ground’ that formed the goal for therapy. Rose rated her self-state on this scale each session (session 4–16) helping to acknowledge transference and countertransference and her capacity for learning or reflecting during each session.
Reformulation Phase
The reformulation phase consisted of four sessions exploring and understanding Rose’s early childhood experiences with others and the world, and how these contributed to patterns and procedures in present day. The psychotherapy file helped Rose identify the target problem procedures (TTPs) she recognises in daily life in the form of traps (self-reinforcing patterns, e.g. social isolation trap, trying to please trap), dilemmas (restricted choices, usually two opposing options, e.g. upset feelings dilemma, approval vs. feelings/approval vs. independence dilemma) and snags (appropriate goals that are sabotaged, e.g. physical symptoms stop me from doing the things that keep me well).
Rose’s early relational experiences were plotted on a timeline which she completed for homework, incorporating positive and negative memories. This indicated which RRPs and TTPs were present, and likely internalised, to create her repertoire of relational patterns that would shape her interpersonal and intrapersonal interactions today. Moreover, a birth story exercise helped understand the contextual landscape when Rose was born. This developed a narrative about being ‘wanted’ as her mother felt isolated and unloved, therefore craved unconditional love from a baby. However, this ‘wanting’ placed responsibility on Rose from birth, resulting in neglect and abuse as having a baby that needed care and nurturing didn’t provide Rose’s mother with the reciprocal care and connection she had craved. Rose held a great deal of compassion for her mother’s position, however, was unable to connect with compassion to ‘little Rose’.
Rose identified key moments in her timeline and birth narrative that touched on early familiar RRPs; neglecting/dismissing---neglected/ignored/overlooked/forgotten, abusing/hurting---abused/victim, criticising/judging/controlling--- criticised/judged/controlled. She also identified a rescuing/protecting---rescued/protected/cared for RRP, which at times she experienced when others intervened, and the abuse stopped temporarily. Rose recalled a memory with a teacher who provided her with books and new uniform, showing her compassion and understanding.
The psychotherapy file also helped Rose to identity self-states, which the PSQ identified were highly fluctuating and unstable. Rose identified ‘zombie’; a state of being cut off which linked to the RRP of dismissing/hating/abusing---cut off/passive victim. She named this state ‘flat’ and described this as a dissociated state, in which she is “only half here” and feels numb and empty. ‘Flat’ is accompanied by nightmares, negative thoughts and depressive symptoms. Rose also identified ‘soldiering on/striving to cope’; a state in which she is driven and active as a way of avoiding affect and emotions, which linked to the powerful overwhelming---too much RRP. She named this state ‘hyper’ and noticed how her physical symptoms such as headaches, poor sleep and memory problems are worse when she is in the ‘hyper’ state, as she moves quickly and clumsily with a busy body and mind. This identification of self-states and shifting helped Rose and the therapist to simplify a confusing array of emotions and behaviours in to two versions of herself, which connected with her and brought about the target problem (TP) for therapy; I feel unable to regulate my self-states; “hyper” and “flat”, moving between them quickly, avoiding one, or being in both at once. I want to find a healthy middle ground.
The two states were written down on paper between Rose and the therapist, forming the start of her SDR, or otherwise known as a CAT map (Parkinson, 2008). The process of mapping makes procedures explicit, inviting the client to take ownership of the map.
Rose found that she was fluctuating between these two states from week to week, which influenced how easily she could concentrate and remain present in sessions. During the early sessions the therapist utilised guided imagery and progressive muscle relaxation exercises to start or close sessions, allowing Rose to focus and connect with the content and process of therapy. Moreover, the self-state scale helped Rose tune in and rate which state she was in. In fact she reported how this ability to recognise her self-state was transferable out with therapy, enabling her to monitor and adapt the emotional lens she was experiencing interactions with Self and others with. This idea was informed by Vygotsky’s concept of the zone of proximal development (ZPD; Vygotsky and Cole, 1978), which in CAT can help to understand an individual’s capacity for learning. This knowledge can help psychotherapists stretch their client’s comfort zone by introducing new learning that will challenge their understanding and invite them to leave their comfort zone, but not feel too challenged or unfamiliar that it doesn’t permeate, or they disengage. The ZPD must be assessed regularly, as this can change depending on the self-state occupied. For Rose, she was able to share information and hold conversational pace when in the hyper state, however struggled to connect with emotion. Whereas when she was in the flat state, she found it difficult to maintain concentration and conversation, was less easily able to recognise emotions, and felt numb.
In session five Rose received her reformulation letter, which summarised the procedures and states identified as familiar and linked these to early life experiences with compassion and validation. The letter prompted Rose to pause, as the therapist shared curiosity about her staying busy on an intellectual level during sessions, as a way of avoiding uncomfortable emotions. Rose was invited to start noticing state shifting and what triggered it as the therapy progressed into the recognition phase, by keeping a mood diary at home.
Recognition Phase
As Rose entered the recognition phase of therapy, the emphasis was on developing an ‘observing eye’; a CAT term to help people understand the importance of noticing when unhelpful patterns are activated and how they move through them, before one can think about change. Rose started to bring increased examples of feeling judged and criticised to therapy following a few family events she had attended. BAPARF, an acronym for Belief-Aim-Plan-Action-Result-Feedback, was used to map out a recent example when discussing the social isolation/anxiety trap (Figure 1). BAPARF was created as a tool to help understand the interaction between the outside world, internal world and emotions, based on the procedural sequence model developed by Ryle (Ryle et al., 1990). BAPARF detailing the social isolation/anxiety trap on Rose’s SDR.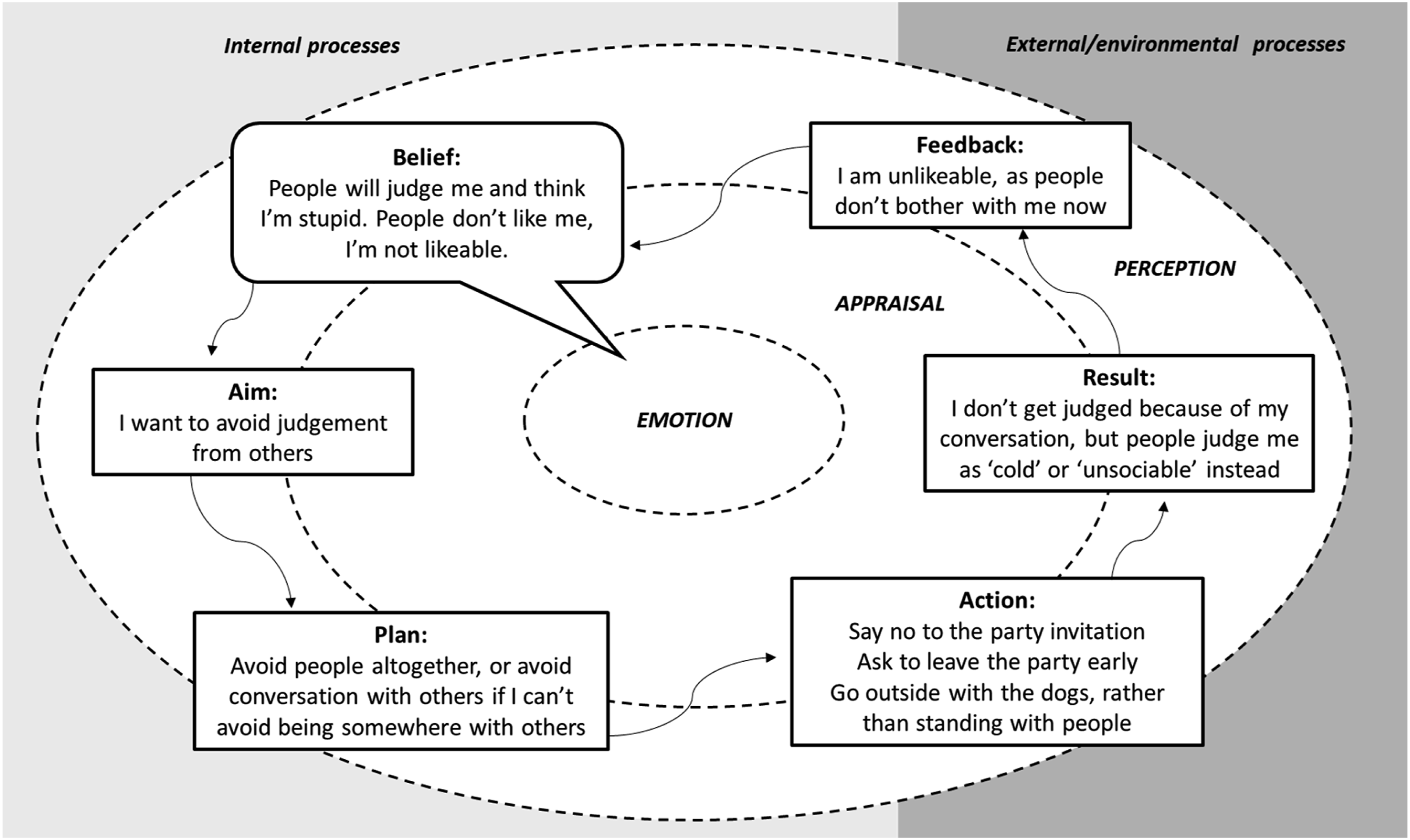
The BAPARF captured a trap which was added to the SDR (Figure 2). This maintained Rose’s fear of rejection and criticism from others. She began to understand how she was hypervigilant of criticism, judgement, and control due to her early experiences of this RRP, however, her ways of coping with this created less connection and opportunity to disprove her beliefs about self-worth and lovability and connected to the core pain of loneliness. Loneliness was something Rose experienced when in the ‘flat’ state, causing her to strive to move in to the ‘hyper’ state as loneliness could feel unbearable. The social isolation/anxiety trap.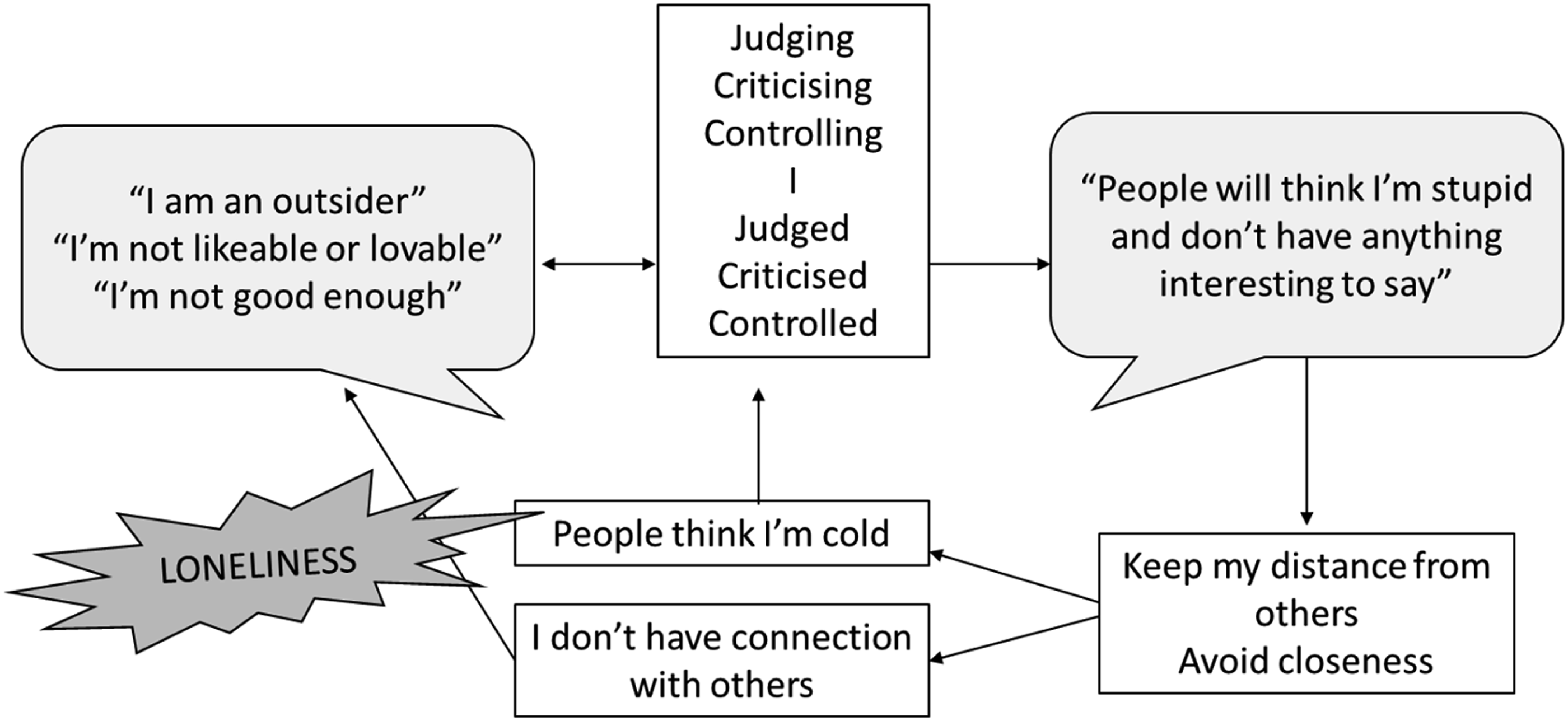
Another TPP that Rose identified as being key to keeping her in constant fluctuation between states, was the upset feelings dilemma (Figure 3). Rose experienced surges of anger, which was understood as a ‘blurting out’ of emotions. These emotions were ‘bottled up’, some for years in the case of anger towards her abusive stepfather, and some daily emotions linked to other patterns or conflict within her marriage. As she began to develop her observing eye, she noticed how ‘bottling up’ could also make her physical symptoms, such as headaches, bowel difficulties and sleep disturbances worse. Upset feelings dilemma.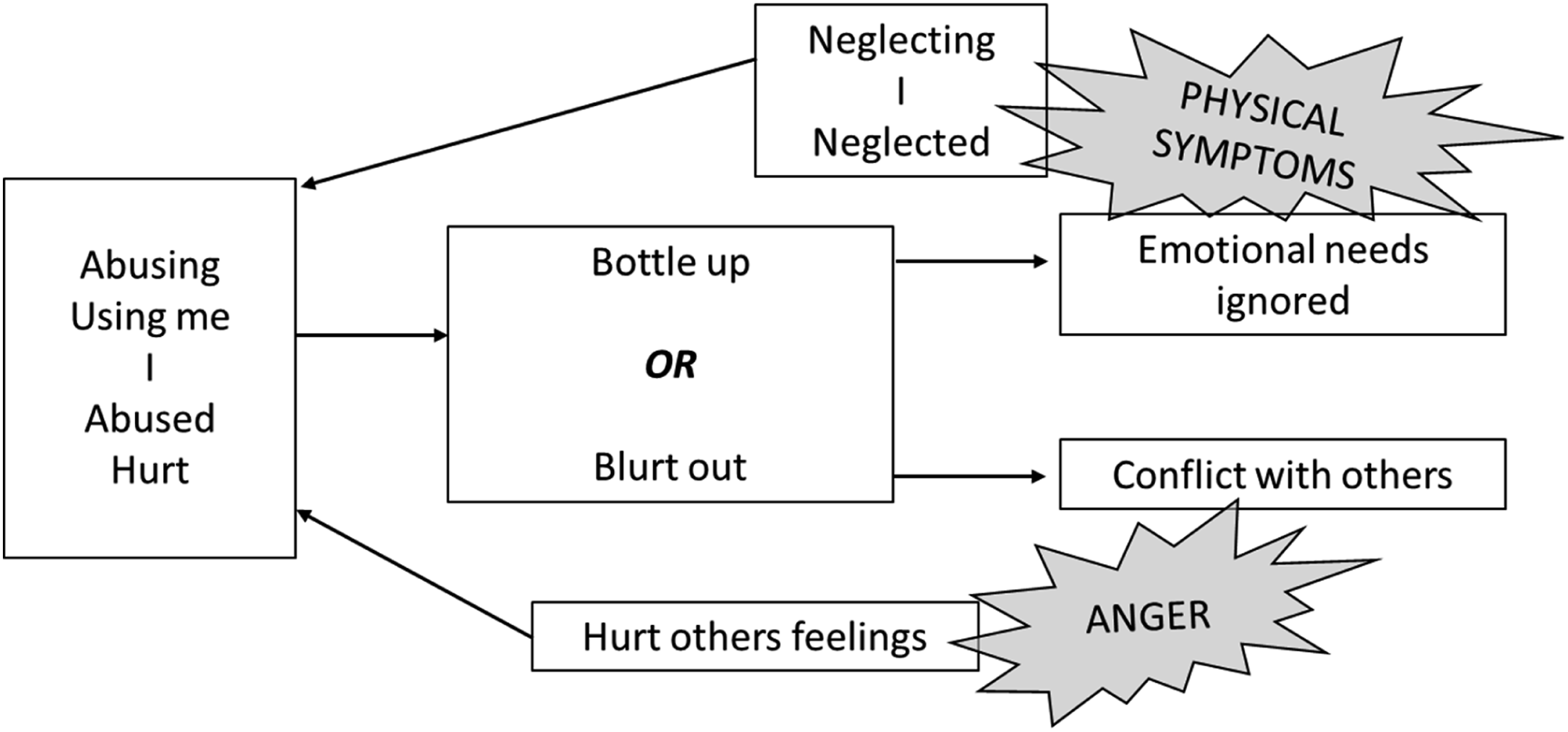
Rose was consumed by anger towards her stepfather after acknowledging the upset feelings dilemma. Rose’s stepfather died two decades ago and she never had the opportunity to confront him as an adult. This was a source of great frustration and loss. Therefore, Rose was invited her to write a therapeutic letter to her father, as part of an exercise in processing repressed and unresolved emotions associated with the abuse she experienced. Rose attended the following session with a handwritten letter. The transference and countertransference was powerful, leading to a moment of shared sadness for ‘little Rose’, before ‘adult Rose’ tore up the letter in the room and let it fall to the floor. Rose was invited to speak to ‘little Rose’ while she was held in mind in the room, from the position of a compassionate adult. Rose took this opportunity to direct kindness and love towards her younger self, in the form of an empty chair. This exercise triggered a shift away from anger and Rose’s self-state ratings appeared to reduce in intensity following this session.
At this point a half-way review was conducted and Rose reflected on her SDR and TP. She reported that it was “nice to not feel angry all the time” and was starting to approach exits from her TPPs independently as she recognised when and where she became stuck on her map. The focus of her SDR shifted to address the people pleasing and approval seeking TPP, as these linked to the loneliness uncovered earlier (Figure 4). Approval seeking/people pleasing trap.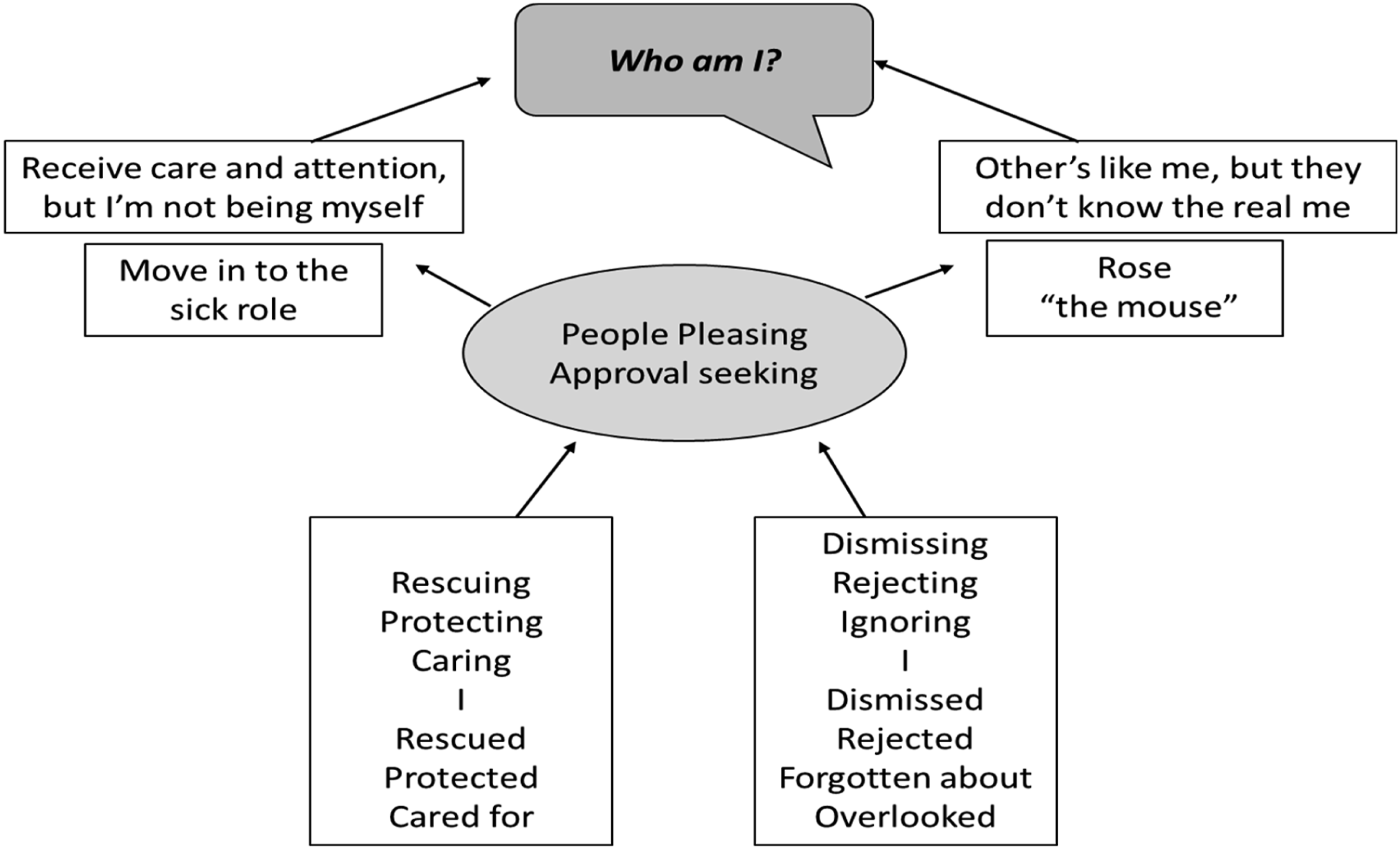
Within this TTP Rose identified how her physical symptoms can have a positive outcome socially, as being ‘poorly’ elicits care and compassion from others. Although we explicitly understood Rose’s physical symptoms as FND, and not a ‘sick role’ that was conscious, she started to unravel how having these physical symptoms contributes to her sense of self (e.g. “I am poorly”) and social interactions. Rose recalled times as a child when being physically unwell kept her safe from abuse, for example, monthly menstruation paused the sexual abuse she experienced, and having a bad case of scarlet fever increased health visitor visits which in turn reduced physical abuse during this period. This prompted a powerful realisation; care and compassion were shown in response to being poorly (rescuing/protecting---rescued/protected); a message that was internalised at a young age. Rose and the therapist used a white board in session to explore what ‘poorly Rose’ looked like in interaction with self and others (caring---cared for), and what ‘healthy Rose’ looked like (criticising/dismissing/neglecting---criticised/dismissed/neglected). This exercise led to the question “who am I without the illnesses?”. This was in Rose’s words a ‘light bulb moment’, as she recalled a recent example of telling an old friend she had Alzheimer’s Disease because she felt criticised when they joked about her forgetting their planned coffee date. This disclosure immediately elicited a compassionate response and apology from her friend, however, left Rose feeling guilty and upset that she hadn’t been her ‘true self’.
Moreover, these RRPs were linked to another strategy for approval seeking/people pleasing, involving being ‘Rose the mouse’; a version of herself that acted in a way that others expected, which she believed they preferred. For example, not sharing an alternative opinion with a previous male colleague, as he might think she was being defiant and “too much”. Rose also described dressing certain ways to communicate status and elegance, something she couldn’t afford to do as a child, which was a way of avoiding judgement from others about being ‘poor’ or uneducated. Therefore, time was spent thinking about her identity; characteristics and traits separate to physical health symptoms or the ‘mouse’. Rose completed an exercise for homework in which she was asked to reflect on her strengths, which involved identifying a compassionate ‘other’ in the form of her childhood teacher, who first invited her into a nurturing---nurtured RRP.
Revision Phase
During the final four sessions, attention shifted to finding and finalising exits to the patterns and procedures filling Rose’s SDR. Her TP described wanting to develop a middle ground, therefore, ways of being present and integration were prioritised.
Rose began “putting myself out there more” as an exit from the social isolation trap, by knocking on her neighbour’s door with baked goods and accepting their invitations to go inside and chat. Behavioural experiments were planned and conducted, detailing how Rose might feel and think as she interacted with her neighbour as well as problem solving the potential barriers. The therapist encouraged Rose to reflect on these exercises in session, and although she noticed a spike in her anxiety and a pull towards the ‘hyper state’, she was able to notice this in the moment, find her middle ground, and move away from a negative appraisal of the interaction. Ratings of anxiety regarding beliefs (not being good enough/I am stupid) were used to collect evidence and build confidence. The therapist helped Rose create a ‘self-compassionate mirror’ which documented her strengths and characteristics, acting as another exit from the social isolation trap and people please/approval seeking trap. A mirror was drawn on a large piece of paper and using the strengths and characteristics Rose had identified earlier in therapy, it was decorated with self-compassionate phrases to support Rose in entering kind self-self dialogue rather than critical dialogue, and develop confidence related to her identity.
Regarding the upset feeling’s dilemma, Rose had been practising ways of communicating her feelings with her husband during therapy as and when they came up. Therefore, the observing eye itself had become an exit, as she felt more able to calmly address her husband when she had feedback or an alternative opinion. This enabled Rose to think about “assertive, not aggressive” methods of communication to help her be ‘true Rose’ with self and others, rather than the ‘mouse’ or ‘poorly Rose’. In session role-plays supported her to practice conversations about her holidays or interests, which she then used when in social situations instead of talking about her physical symptoms. This exit provided Rose with confidence and independence, something which she later fed back was key to her moving forward towards others, and away from patterns which keep her isolated and dependent.
Rose developed a healthy island as the therapy moved toward an ending, which she called her ‘middle ground’. Healthy islands are based on the ideas of Wilde McCormick (2017) and are a place where the healthy Self resides producing a landscape of helpful, revised RRPs. In the spirit of being creative and utilising her increasing confidence, Rose was invited to make her healthy island for homework, and she chose to use her favourite holiday destination island as an outline for this and wrote on her exits and an image of a mirror as a reminder. The RRP nurturing---nurturing also featured on her healthy island, reflecting the therapeutic relationship and a move towards a more attuned and responsive self-self relationship.
Rose was provided with a goodbye letter in the final session which summarised her learning in therapy, captured how difficult her journey had been, reinforced how well she had done, and posed some hopeful curiosities for the future. The therapist encouraged a transparent dialogue about the ending, starting in the goodbye letter and continuing in the final session together, which highlighted a sense of loss as well as hope. Rose stayed present and grounded during the final session as she received the ending letter, allowing for true relational connection. The therapist reflected back to Rose how different the dialogue and connection felt as they read the ending letter, compared to the reformulation letter which was received in a different state and with an avoidance of slowing down and letting emotions come and go. In this newfound middle ground Rose was able to hear the words clearly and express emotions; the loss of ‘the old Rose’ and associated sadness for lost time and connection, but hope for ‘true Rose’.
Treatment Outcomes
Objectively, the PSQ documented a change in score over the course of the therapy which indicates a positive move toward integration of self-states (Figure 5). This change was sustained at 3 month follow up. An overall reduction of 10 points was observed from pre-therapy to the final follow up. Changes on PSQ score between pre, mid, post and follow up.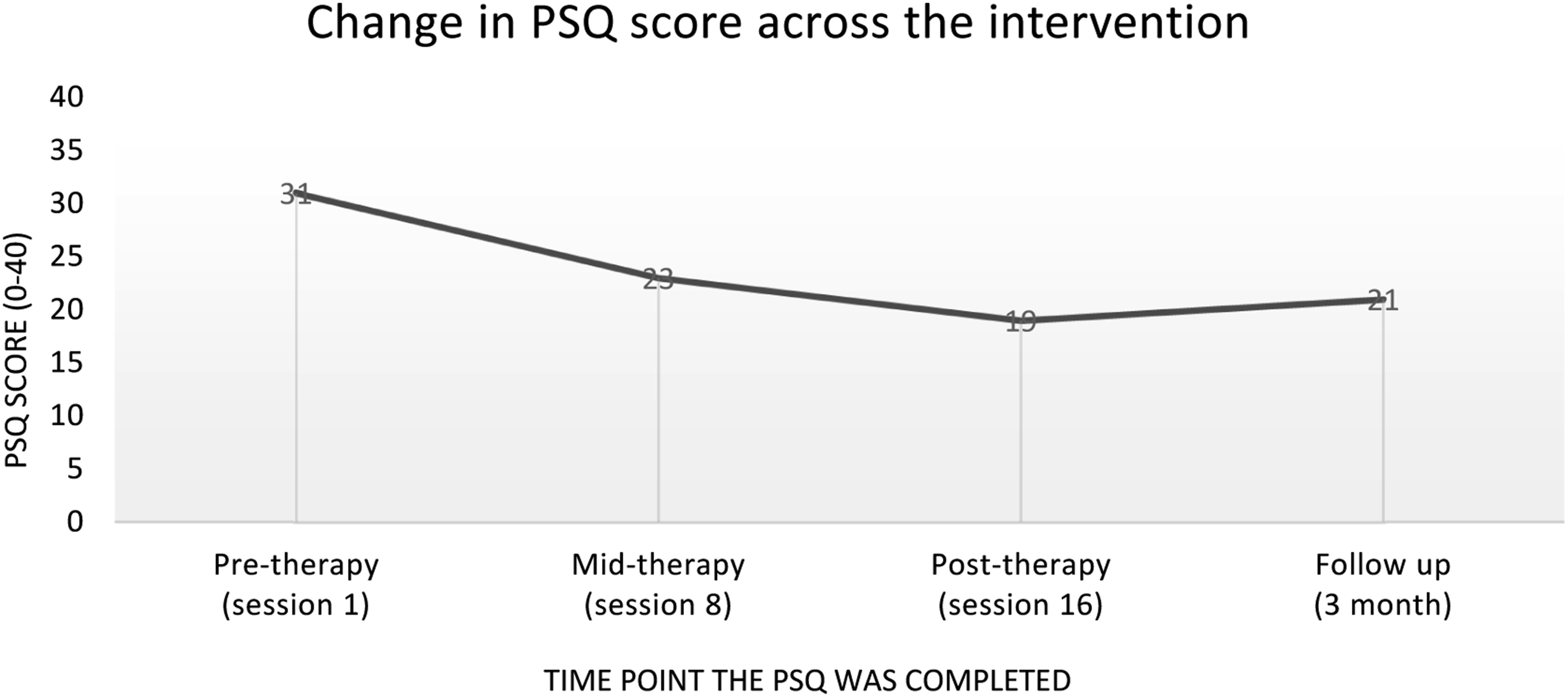
Moreover, Rose completed ratings of her self-state each session on the idiographic scale developed during the reformulation phase (−10 flat, +10 hyper). These ratings allowed transference and state shifting to be acknowledged in each session, influencing the content and process of the work. However, it also provided an overall picture (Figure 6) of how Rose’s states changed over time, with intense ratings and frequent fluctuations being observed at the beginning of therapy, and less shifting/intense ratings observed towards the end of therapy moving towards an integrated ‘middle ground’. A measure of changing self-states as therapy progresses.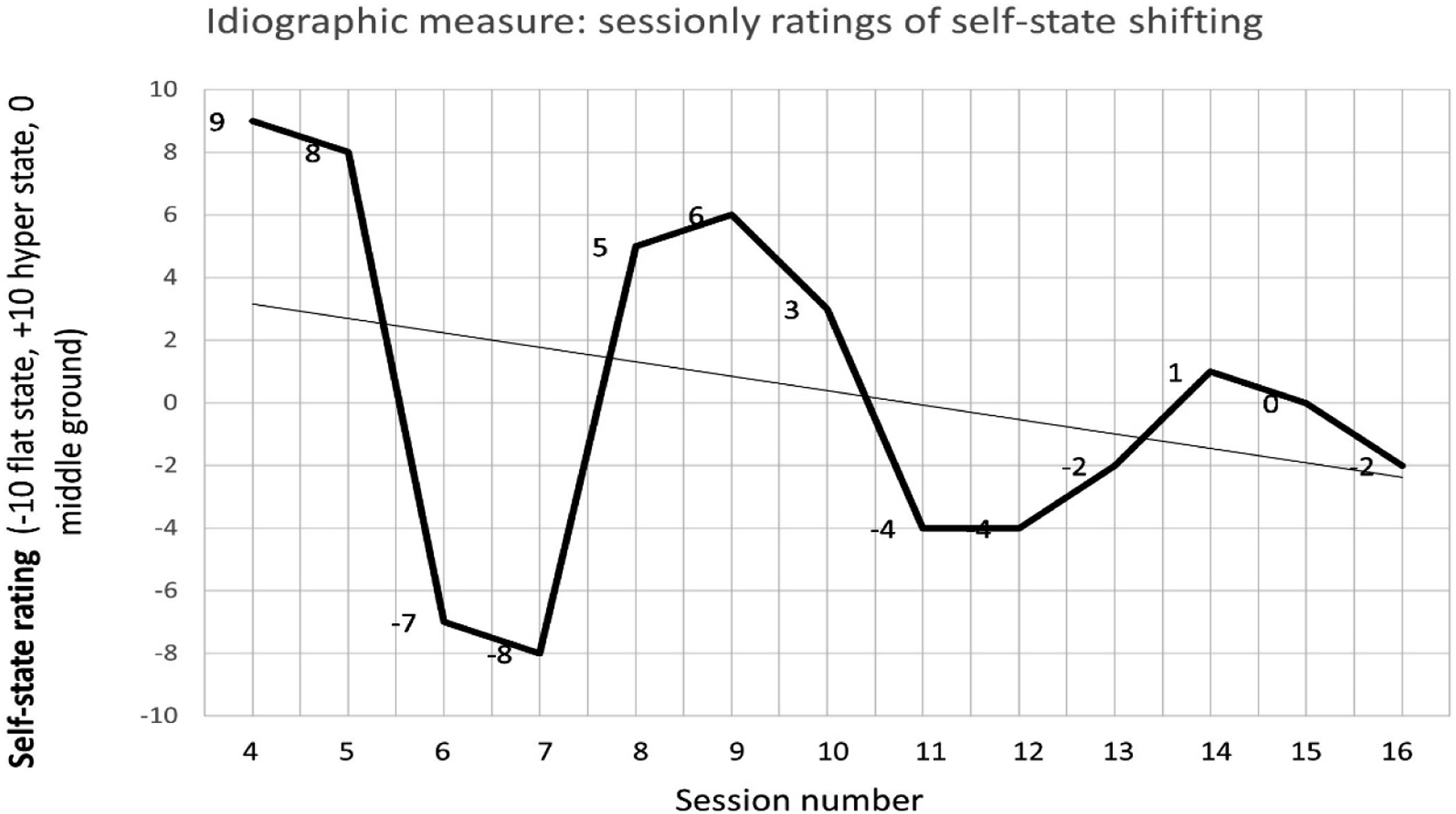
Moreover, the HADS was completed pre-CAT and post-CAT when Rose was discharged from the CTT. This showed clinically significant reductions in anxiety (pre-CAT = 17, post-CAT = 8) and depression (pre-CAT = 15, post-CAT = 5), providing some evidence of general outcomes, in addition to specific goals around emotional regulation and integration of self-states as measured by the CAT specific PSQ and idiographic measure.
8. Complicating Factors
The primary complicating factor during this therapy regarded state shifting and the impact of extreme states on Rose’s ability to engage in the content and process of therapy. This particularly applied to the ‘hyper’ state, in which Rose and the therapist were at risk of intellectualising and avoiding the emotional context in the dialogue. Through transparency of communication, the therapist was able to introduce relaxation techniques to the start and end of early sessions to facilitate grounding. The development of an idiosyncratic state measure aided Rose’s recognition and supported the therapist to pace the session; accordingly, for example, slow down and introduce pauses to connect with emotions and bodily sensations when in the hyper state or create a safe therapeutic space and relationship to allow Rose to leave the flat state and connect with uncomfortable emotions usually ignored or dismissed.
The impact of physical health symptoms, treatment and investigations often impact therapeutic work with older adult clients, as we observe increased frequency and severity of comorbid physical health complaints. In Rose’s case, she was undergoing investigations for gastrointestinal symptoms whilst therapy was ongoing, introducing some uncertainty around the difference between these and her functional symptoms, and how they should be formulated. In the end, Rose took the lead regarding what she believed were functional versus physical, following the reformulation phase and the joint understanding of longstanding physical symptoms. Moreover, flexibility was required when booking sessions to accommodate physical health appointments. This could present as a barrier for treatment; however, it did not disrupt the flow of weekly sessions for Rose given flexibility with clinic times.
9. Access and Barriers to Care
Overall, this case report highlights the acceptability and feasibility of CAT when the focus of therapy is integration in the context of FND, PTSD and personality disorder. In Rose’s case, she was offered CAT as the senior clinical psychologist in the team was completing the CAT practitioner training at that time. CAT would not necessarily be offered routinely within older adult community treatment teams in favour of NICE guidance recommended treatments, however, given Rose’s exposure to different therapeutic modalities in the past with little success and the growing evidence base for CAT with personality difficulties it was deemed appropriate. CAT provides an overarching framework in which different techniques can be drawn on to create exits and aid recognition, which was beneficial in the case of Rose as specific interventions for trauma memories were incorporated.
Memory difficulties and cognitive impairment can complicate delivery of CAT due to the pace and amount of information communicated within letters. Therefore, session summaries were utilised, letters kept as brief as possible, and the map was created visually on large A3 paper which Rose took home each week as a memory aid. These adaptations did not detract from the delivery of CAT, and from a therapist point of view felt in keeping with the collaborative and flexible nature of CAT.
10. Follow Up
Rose attended all four of her follow up sessions. She brought a goodbye letter to the first follow up session, 1 month after the ending session. Rose wrote how she found herself “feeling sorry for the person I WAS and so grateful and thankful for the help you have given me into understanding why I was the way I was…and how you have helped me to be the person I am becoming. The ME that I might have been had I not had the upbringing I had”. In dialogue with Rose, this feedback captured the integration of states achieved and growing awareness of self-self interactions.
The follow ups also provided space for Rose to offer examples of her exits, for example, dealing with a sarcastic comment on a WhatsApp group by responding calmly, changing the conversation topic and reminding herself that she’s not being criticised personally. She had also been to the supermarket by herself to buy some flowers, feeling more confident to go out in public and communicate with others. Rose also noted that her memory and concentration had been better in recent weeks, which removed power from the ‘physical symptoms’ snag, allowing her to use her exits without the complication of becoming muddled when entering shops or paying for items.
Rose’s sleep however remained poor, and although she reported fewer incidences of lying awake with racing thoughts or replaying memories from the past, she still woke frequently during the night and would get up and start her day hours before her husband. One thing that she had noticed had changed was the critical internal dialogue or frustration regarding waking through the night, as she allowed herself to nap through the day.
11. Treatment Implications of the Case
This case report provides early evidence for the possible utility of CAT when working with functional symptoms, in addition to PTSD symptoms and personality difficulties. The non-blaming position of CAT connects the significance of early experiences of relating to how we unconsciously relate interpersonally and intrapersonally as an adult. This was shown to be effective when exploring and validating psychogenic causes for physical symptoms.
Rose’s focus on physical symptoms in the early phase of therapy required careful thought and consideration. Complimenting the treatment guidance for FND, the reformulation phase in CAT allows for a gentle and validating acknowledgement of the link between psychological and physical pain. Therefore, CAT feels particularly helpful when understanding functional symptoms and it provides the flexibility to focus on relational issues pertinent to the client, rather than specifically targeting a reduction in functional symptoms.
Integration of self-states facilitates the fragmented parts of one’s identity, including psychosomatic responses and dissociative parts, which was pertinent in the case of Rose. The change in PSQ score indicated a significant increase in integration as therapy progressed and Rose moved away from a score indicative of a personality disorder diagnosis. Large improvements were observed on items regarding ‘my sense of self is always the same’, ‘my mood and sense of self seldom changes’ and ‘I never lose control’. Interestingly, the largest change was observed within the first half of therapy suggesting the reformulation and the early recognition phase had the biggest impact on integration, Rose’s mood and sense of self. Moreover, this change was sustained at 3 month follow up. A two-point increase was observed in the final session score, which although remained in a non-clinical range may indicate a possible effect of the therapy ending. Although the idiosyncratic measure of state-shifting was only completed for 12 sessions (spanning session 4–16), the trend line demonstrates a move toward less frequent and less severe shifts in state. Rose’s ratings of state severity moved away from the extremes and towards zero, which indicated her middle ground (an integrated state in which she was present and connected to self and others). These two outcome measures provide a sound sense of the impact of CAT, however, daily intensive measures could have been utilised to map a more robust trend line. Despite Rose reporting a reduction in memory and concentration problems, using more general measures of functional symptoms would have allowed for a more objective assessment of whether CAT has a secondary positive effect on functional symptoms.
Feedback from Rose during follow up highlighted the impact of the reformulation letter and goodbye letter, “serving as a reminder of what [the therapist] and the therapy meant to me”. Letter writing is a key tool in CAT used to develop shared understanding and summarise learning, but also to reflect on the therapeutic relationship (Ryle & Kerr, 2020). The therapeutic relationship is used as an explicit tool in CAT, with transparency regarding transference, countertransference, enactments of RRPs and TPPs, and ruptures being imperative. Therefore, the relationship allows for improved recognition, playfulness, modelling and practicing new or unfamiliar RRPs. This unique element of CAT appeared to help in Rose’s understanding of herself, and in her own words allowed her to ‘’grow up’’ during therapy, finding her adult self and leaving her child self behind with compassion.
This initial exploration of the acceptability and feasibility of CAT for functional symptoms and personality difficulties provides some future direction for practice-based research and larger trials. It would be interesting to examine the utility of CAT for this population on a larger scale; as a transdiagnostic intervention focussing on integration, with secondary gains in functional symptoms. Within this future research, measures exploring the impact of the therapeutic relationship and specific CAT tools would be beneficial given the impact of these in this case.
12. Recommendations to Clinicians and Students
Clinicians and students working with individuals with FND or other functional/psychogenic symptoms may benefit from using a collaborative CAT informed formulation, with the aim of understanding any patterns and procedures associated with the development of maintenance of symptoms. It is also important to be mindful of the difference between FND and factitious physical symptoms, to ensure one does not fall into the societal trap in which these symptoms are stigmatised and exist within a blaming culture. Functional symptoms are understood as unconscious manifestations with both psychological and biological predisposing factors; therefore, psychological therapy may not always be the most appropriate course of action or fit with the individuals understanding of their symptoms. Identifying goals and other primary focuses (e.g., integrating states or improving relationships) may be a helpful way to intervene, with a possible secondary impact on functional symptoms.
When working within the framework of CAT, idiosyncratic measures based on the individuals TP, TPPs or RRPs can prove extremely beneficial for monitoring progress, aiding recognition and improving the delivery or focus of sessions. This was the case for Rose, and ongoing monitoring supported the therapeutic relationship as her ZPD was continuously assessed to tailor therapy to her current needs and state, and ultimately became a change mechanism related to integration. Moreover, this case highlights the need for therapist confidence in identifying and sharing transference and countertransference, to prevent colluding or getting stuck in a problematic procedure.
Footnotes
Acknowledgments
The author would like to thank Rose (pseudonym) for consenting to the dissemination and interpretation of her CAT therapy. Rose wanted to contribute to clinical learning and developments that might support others in a similar position to her, therefore, I hope this case report has the desired impact and enables that for her.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.