
Abstract
Rates of post-traumatic stress (PTS) are greater among transgender and non-binary (TGNB) youth compared to their cisgender peers. This disparity has been linked to increased experiences of trauma among TGNB youth, including greater exposure to child abuse, discrimination, hate crimes, and familial and peer bullying and rejection. Few studies to date have examined the use of trauma-focused interventions with TGNB youth. Narrative Exposure Therapy (NET) has been identified as a potentially impactful treatment for PTS for communities who experience oppression and human rights violations given its social justice-oriented “testimonial” approach and focus on meaning-making around traumatic experiences. While narrative-based approaches are often considered “best practice” for trauma interventions, youth may present with comorbid conditions that present barriers or often preclude them from receiving trauma treatment, such as selective mutism (SM). In this case series, we describe the use of NET for treating PTS symptoms in two transgender youth with comorbid SM, as well as adaptations to support their engagement and progress in treatment. Treatment progress was observed in reduction of PTS symptoms, increase in self-reported resilience and positive well-being, and full remission of SM, with treatment gains observed 6-months post-discharge. From these cases, we identified that (1) NET is a brief treatment that can address PTS and SM symptoms among TGNB youth; (2) NET is able to be adapted to enhance engagement in a narrative-based, trauma-focused therapy for youth with PTS and SM; and (3) NET can also increase self-perceived resilience and a sense of positive well-being for TGNB youth.
Keywords
1 Theoretical and Research Basis for Treatment
Transgender and non-binary (TGNB) youth experience significant disparities in mental health outcomes, including higher rates of depression, anxiety, and suicidality compared to their cisgender peers (Delozier et al., 2020; Lefevor et al., 2019). These disparities have been linked to higher rates of familial and social rejection, experiences of stigma and discrimination, including bullying at school (Aparicio-García et al., 2018), and identity invalidation from others (Johnson et al., 2020). TGNB people are at higher risk for post-traumatic stress (PTS) due to higher rates of trauma, including societal discrimination and living in hostile, non-affirming, and invalidating social environments (i.e., those with anti-transgender laws and policies; Barr et al., 2022). Rates of post-traumatic stress disorder (PTSD) among TGNB individuals are estimated between 17.5% and 45% (Reisner et al., 2016), higher than rates in the general non-veteran population, which are estimated around 6.1% for lifetime prevalence (Schein et al., 2021).
PTSD is characterized as a mental health condition arising from direct or indirect (i.e., witnessing or learning about) exposure to actual or threatened death, serious injury, or other major stressors (American Psychiatric Association [APA], 2013). The diagnosis requires the presence of at least one type of intrusive symptom, such as nightmares or flashbacks. It also requires the presence of persistent avoidance of stimuli associated with the trauma, including avoidance of external reminders, such as places or people, or avoidance of any trauma-related thoughts or feelings related to the traumatic event. A diagnosis of PTSD also requires at least two symptoms of negative alterations in cognition and mood, which include overly negative thoughts and assumptions about oneself or the world, exaggerated blame of self or others related to the trauma, decreased interest in activities, feeling isolated, or negative affect. Finally, individuals also need to report alterations in arousal and reactivity that began or worsened after the traumatic event, which can include irritability or aggression, hypervigilance, difficulty concentrating, sleep disturbance, heightened startle reaction, or risky or destructive behavior. These symptoms must be present for at least 1 month and cause clinically significant distress and functional impairment (i.e., difficulties at school, work, or social activities; APA, 2013).
There is growing awareness that the sociopolitical and historical contexts of trauma experiences have a major influence on the expression of PTSD (Katsounari, 2015). For instance, Barr et al. (2022) recently identified that exposure to anti-transgender bias and higher levels of non-affirmation were associated with greater PTSD severity, even after controlling for exposure to other traumas. This finding suggests these specific gender minority status-related stressors may be potentially traumatic and/or induce a trauma response for TGNB individuals. Thus, it is imperative to account for and integrate such potentially traumatic social experiences into the conceptualization of PTS symptoms for marginalized communities.
For TGNB youth with trauma, experiencing greater barriers to accessing mental health services poses an additional risk for worse mental health outcomes (e.g., Warwick & Shumer, 2023). While most trauma-focused interventions require at least some verbal processing and engagement, for youth with communication challenges associated with comorbid anxiety, modifications and accommodations are much needed to support their capacity to engage in trauma-focused treatment. The result of which may also have a positive impact on their overall anxiety, mental health, and well-being. Selective mutism (SM) is a mental health condition characterized by total absence of speech in specific situations while present in other situations (e.g., absence of speech at school versus home settings). These symptoms must be present for at least 1 month and interfere with academic or occupational achievement and/or social functioning (APA, 2013; Vogel et al., 2022). SM generally presents during childhood and is relatively rare with international studies estimating prevalence between 0.18 and 1.9%, though these estimates are posited to be influenced by immigration status and bilingualism (Viana et al., 2009).
While a systematic review of the literature identified significantly greater prevalence of anxiety disorders among transgender individuals compared to cisgender individuals, with higher rates particularly among transgender men (Millet et al., 2017), there are no current estimates regarding SM in this population. Still, in their review, Millet et al. (2017) found that social phobia was one of the most common disorders among transgender men and women, which, along with social anxiety disorder, has been associated with SM (Muris & Ollendick, 2021). Current research posits that the underlying etiology for the emergence of SM in childhood is anxiety, and social anxiety in particular, with one study finding that 80% of youth with SM also met criteria for at least one other anxiety disorder (Driessen et al., 2020). There is evidence to suggest that symptoms of SM may arise primarily as a means of anxiety avoidance in social situations (Diliberto & Kearney, 2018). In fact, SM behaviors may function to reduce social anxiety through reduction of anxiety-inducing actions (e.g., speaking, social engagement), and thus may be negatively reinforced through avoiding opportunities for social exchanges. While some youth may developmentally progress out of this diagnosis, SM may persist into adulthood in the presence of chronic anxiety and lack of intervention.
In general, traumatic experiences have not been found to be a common etiological cause for SM. However, it is noted that trauma may exacerbate the mental health of an individual with a greater predisposition or vulnerability due to existing social anxiety, which may manifest as SM. More specifically, within the posttraumatic stress theory, SM may present as a coping mechanism for youth who have experienced trauma and avoidance symptoms (Wong, 2010). Prior research has found the use of behavioral and exposure-based strategies to be effective in addressing anxiety and improving communication in youth with SM (Wong, 2010), though few studies have examined such approaches for comorbid SM and PTSD. While treatment for clients with PTSD who are selectively mute can be challenging due to the co-morbidity of limited verbal communication skills and anxiety, the use of coaching and shaping interventions may reduce such barriers (Conn & Coyne, 2014). The use of modifications to augment treatment engagement and processing can also be delivered via telehealth, which may further reduce barriers to treatment access, particularly for youth who live in service area “deserts” and/or lack familial support to access in-person mental health treatment.
Few studies to date have sought to identify specific interventions to support trauma-focused work with TGNB individuals that incorporate a focus on gender-based discrimination and other minority stress (Julian et al., 2023; Lange, 2020), such as non-affirmation and internalized transphobia (Hendricks & Testa, 2012), as sources for traumatic stress. Narrative Exposure Therapy (NET), a brief, trauma-focused treatment, has been identified as an empowering intervention given its “testimonial” approach, acknowledgement of human rights violations, and focus on contextualization of trauma in a non-pathologizing and non-stigmatizing frame (Schauer et al., 2011; Wright et al., 2020). Within the NET framework, PTSD symptoms are conceptualized as resulting from fear that is activated by any cues specific to or generalized from a traumatic experience. These cues, labeled “hot” memories, consist of sensory information, maladaptive cognitions, and emotions associated with the traumatic event(s). The contextual information or facts about the experience are considered “cold” memories that are not fear-activating like “hot” memories. NET aims to integrate “hot” and “cold” memories to provide context to the traumatic event and decrease sensory activation using multiple oral and written exposure activities where clients process these events in chronological order. Through this process, clients revise the meaning associated with each traumatic experience, understand their experience within their socio-political-historical context, and reflect on their personal resilience (Schauer et al., 2011).
A growing literature has identified NET as a social justice-oriented, client-centered approach to addressing trauma among historically marginalized and minoritized communities. Though research on NET with TGNB communities is lacking (e.g., Lange, 2020), prior research has examined the use of NET with other marginalized populations, such as refugees and Native American/Indigenous communities, and communities impacted by multiple traumatic events (Bedard-Gilligan et al., 2022; Gwozdziewycz & Mehl-Madrona, 2013). Such populations, including TGNB individuals, who have experienced chronic trauma are often also victims or witnesses of human rights violations, which makes a social justice-oriented intervention well-aligned with the needs and goals for their treatment (Diab et al., 2018). Several randomized controlled trials have shown NET to be effective at reducing trauma-related symptoms among ethnically and racially diverse populations (Robjant & Fazel, 2010) and chronically traumatized youth (Fazel et al., 2020). In general, studies have highlighted the ability to culturally adapt NET to meet the needs of diverse clients, though details on these adaptations are limited (Wright et al., 2020). Increasing exploration of the use of NET via telehealth has appeared promising (Olavarrieta & Benuto, 2022). However, in general, clinical research with TGNB youth has remained scant particularly in the context of the ongoing COVID-19 pandemic and challenges with accessing mental health services among TGNB individuals (Kidd et al., 2021).
In this article, we present two case studies to demonstrate strategies to adapt NET with TGNB individuals experiencing PTSD symptoms with comorbid SM for telehealth and in-person settings. We also contribute to the paucity of literature documenting the efficacy of NET with TGNB individuals (Julian et al., 2023; Lange, 2020). These clients were seen within a pilot program, the Trans Community Trauma Treatment Center (TCTTC), in a gender health clinic embedded within a large tertiary care pediatric medical setting in the Southwestern United States. The purpose of the TCTTC is to provide timely, evidence-based intervention to a population of young people that have a high rate of exposure to complex trauma, many of whom are also disproportionately unable to access mental health services due to being uninsured, under-insured, or of lower income status. These clients were initially screened during an interdisciplinary clinic visit using the Primary Care Post-Traumatic Stress Disorder Screen for the Diagnostic and Statistical Manual of Mental Disorders (Prins et al., 2016) and scored at least 3 out of 5 on the screener, indicating high likelihood of meeting criteria for PTSD. The clients in this case series were given standardized measures at baseline, discharge, and 6-month follow-up. All names have been changed and any significant identifiers have been altered or removed for confidentiality. In this case series, the term ‘Latiné’ is used in place of Latinx to honor the Spanish language and gender inclusivity (Celis Carbajal, 2020).
2 Case Introduction
Hector (pronouns: he/him) is an 18-year-old Latiné (i.e., identifies as Mexican-American) adolescent living with his mother and three siblings in Palmdale, California. Hector identifies as transmasculine, though he reports that his mother and family members continue to use incorrect pronouns and struggle with accepting his gender identity. He has difficulty speaking and feeling comfortable using his voice, so he often communicates via writing. Hector has two supportive friends online and is completing high school online. He has trouble discussing weight gain and his medical transition with medical providers, which is a source of stress and contributes to barriers to accessing care. Hector participated in NET via telehealth and in-person.
Erik (pronouns: he/him) is a 14-year-old, transmasculine, Latiné (i.e., identifies as Afro-Latino) adolescent living with his mother and father in Simi Valley, California. He has a few supportive friends and has built meaningful relationships with online gamers. He participated in NET both via telehealth and in-person. He shared that he was not comfortable looking at himself on camera and was not happy with the sound of his voice resulting in SM in social contexts and healthcare appointments. Erik generally utilized the telehealth chat box for communicating when participating in appointments virtually.
3 Presenting Complaints
During intake, Hector was assessed using the UCLA-PTSD Reaction Index for DSM-5, which indicated that he met all criteria for PTSD with a dissociative subtype. Hector reported having nightmares of his parents fighting, trouble falling asleep, and waking up for school. He reported feeling anxious and on guard most days. Hector shared that he felt detached from others and at school. Hector presented with significant anxiety and excessive worry that he had been experiencing for over 6 months, which occurred across various settings. Hector was constantly picking at his skin to cope with anxiety. Hector shared that he was sometimes verbal at home but did not speak in all other social contexts. He also reported significant anxiety about his body image and weight gain, which impacted his self-esteem. These stressors were seen to be contributing to difficulty with making decisions and concentrating at school. His SM and skin picking were conceptualized as arising from his history of chronic childhood trauma, ongoing trauma-related symptoms, and general anxiety.
During Erik’s intake assessment, the UCLA-PTSD Reaction Index for DSM-5 indicated that Erik met three criterion for PTSD and at least one dissociative symptom. Erik had been experiencing anxiety for the past 12 months and experienced uncontrollable trembling and eye movements when faced with stressful situations. He reported difficulty finding the motivation to leave his room and with sleep for the past 2 months. He reported that he found it difficult to connect with others and was losing interest in school. Erik reported losing joy in activities he enjoyed over the past 6 months. He shared that he had isolated himself from family members for 2 weeks. At intake, Erik did not speak to his parents, at his medical visits, or in social gatherings, which he reported began around age 13. His SM and mood symptoms (i.e., anxiety and depression) were conceptualized as associated with his trauma-related symptoms.
4 History
Hector was born in Los Angeles, California, and moved to Palmdale, California, around 4 years of age. From ages 4 through 10, he experienced anxiety due to his parents arguing and yelling. He spent much of the time trying to avoid his parents’ arguments with each other. Around age 12, Hector had a traumatic drowning experience, which resulted in needing to go to urgent care. Hector experienced isolation from his family at the age of 13 as he was beginning to explore his gender identity. Hector came out as transgender to his family and was rejected by certain family members. The rejection from his family during his “coming out” experience led to symptoms of anxiety, depression, and isolation. He could connect with two friends at school, which helped him feel less isolated. During adolescence, Hector witnessed community violence and a shooting in his neighborhood. He lost most of his support system at age 16 and experienced emotional abuse from his partner and from a religious church member. Hector also reported experiencing gender discrimination, contributing to feelings of isolation and becoming selectively mute. Hector reported difficulty with trusting others due to his past trauma.
Erik was born in Los Angeles, California, and lived with his parents in Simi Valley, California. He reported that his parents were generally supportive. Erik experienced bullying starting at the age of 6. He stated that the bullying was severe and caused him to isolate himself from others. He found support in his animal companions and would prefer them over others at school due to the bullying he was experiencing. At the age of 9, Erik experienced the death of his pet, which he struggled to cope with. Erik had a hard time creating attachments with others. At 13, he was in a severe car crash that caused recurring nightmares. He was uncomfortable talking about the crash because it involved his mom and witnessing her injury. Erik also experienced gender discrimination by peers in school and with some family members. He shared that he experienced bullying for his masculine gender expression. He shared that this is when he isolated himself from his peers and was scared to interact with others for fear of discrimination. Erik reported that he didn’t speak often with others but spoke softly with short responses when he was not understood. For example, Erik wrote that he answers questionnaires with a low voice at the dentist or medical visits if needed.
Both Hector’s and Erik’s parents reported that they had a prior history of anxiety from childhood. Hector’s mother shared that he began experiencing anxiety when around others at the age of 12. He became increasingly worried and fearful of social interaction beyond his room. At 13, Hector expressed his masculine identity but faced bullying from peers, the church pastor, and family members. This led to feelings of isolation and anxiety. Hector’s mother stated that he had not spoken at home, with his family members, or in most social situations since he was 15. Erik’s mother shared that his anxiety started at a young age, around middle school, and into high school. She stated that he had not spoken at home or school for 3 months before intake, since age 13.
5 Assessment
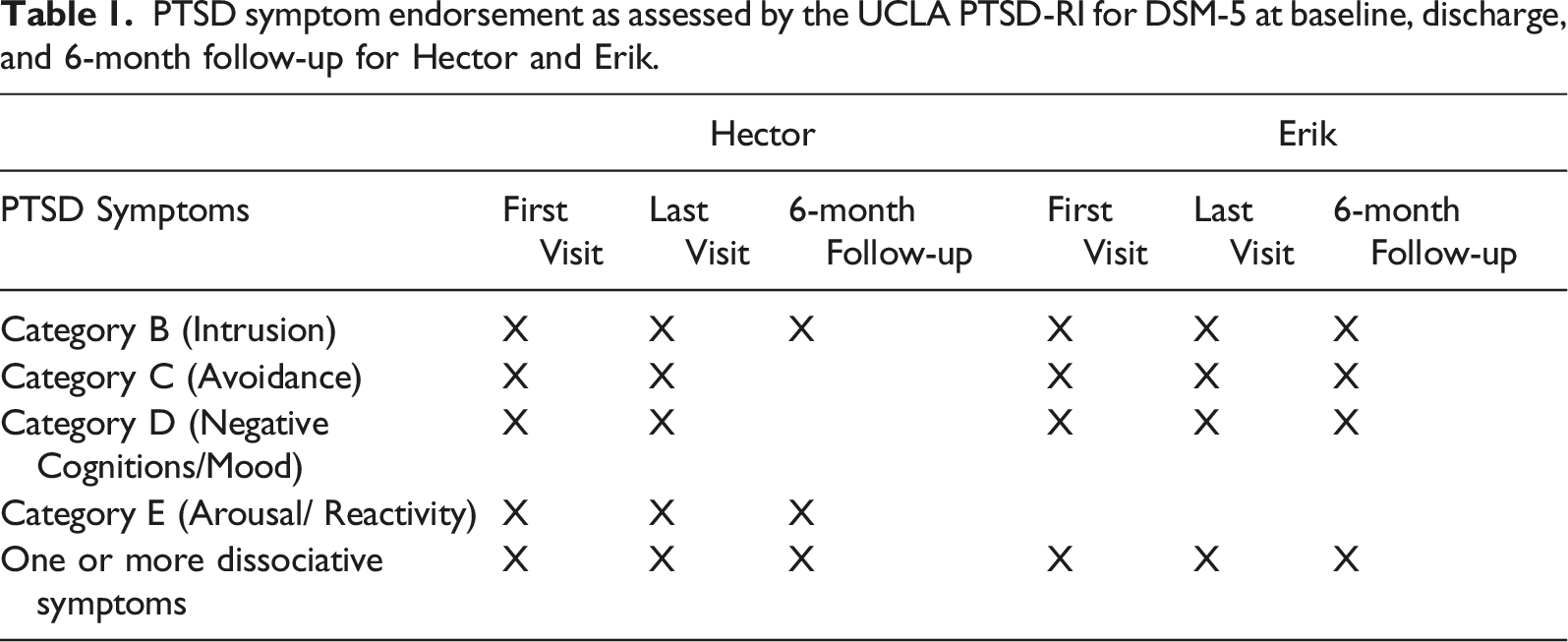
Both clients completed self-report measures at the beginning of therapy, immediately at discharge, and at 6-months post-discharge. To assess symptoms of PTSD, the Post-Traumatic Stress Disorder Reaction Index for DSM-5 (PTSD-RI-5; Doric et al., 2019), a widely utilized and validated measure for screening and assessing children and adolescents for symptoms of PTSD, was administered. Within our clinic, we modified the PTSD-RI-5 based on feedback from clinicians with expertise in TGNB mental health and members of the community. Two additional items reflecting gender-based traumatic experiences (i.e., institutional gender discrimination, interpersonal gender discrimination) were developed and included (Julian et al., 2023). Clients were asked to rate the frequency of their symptoms in the past 30 days keeping in mind their most traumatic event (0 = none of the days, 5 = almost every day). Items are combined into four categories of PTSD criteria: Intrusion, Avoidance, Negative Cognitions/Mood, and Arousal/Reactivity. Clients are also asked three additional items to assess for dissociative symptoms. At intake, Hector experienced symptoms across all four categories and dissociative symptoms, meeting the criteria for PTSD. Erik endorsed Intrusion, Avoidance, Negative Cognitions/Mood, and dissociative symptoms, though he did not meet full criteria for PTSD.
To assess for resilience and psychological well-being, clients completed two additional measures. The Connor-Davidson Resilience Scale (CD-RISC-25; Connor & Davidson, 2003) is a 25-item measure that assesses capacities associated with psychological resilience. Individuals self-assess their ability to cope with stressful situations and traumatic events. Total scores range from 0 to 100 with higher scores reflecting greater psychological resilience (Davidson, 2018). The Flourishing Scale, an 8-item tool used to assess psychological well-being, including self-perceptions of self-esteem, relationships, purpose, and hope for the future (Diener et al., 2009), was also administered. Scoring is based on a 7-point Likert scale (i.e., 1 = strongly disagree, 7 = strongly agree), with a range of 8–56. Higher scores indicate greater psychological well-being.
6 Case Conceptualization
The clinician conceptualized these cases from a trauma-informed biopsychosocial framework, which acknowledges that each youth likely had a greater genetic vulnerability for greater anxiety or emotion dysregulation, exacerbated by experiences of different kinds of traumatic experiences, including invalidating and interpersonal rejection. In addition, the clinician conceptualized SM as facets of both clients’ ongoing trauma and anxiety symptoms, and that the exposure inherent in NET may be a useful therapeutic approach for the clients’ comorbid PTS symptoms and SM.
Hector experienced several traumatic events, including gender discrimination, a traumatic drowning experience, witnessing gang violence, and witnessing his parents fighting. At intake, Hector was selectively mute and struggled to communicate about his trauma. NET was utilized as an intervention for Hector as NET is culturally responsive and flexibly uses narratives to process trauma and reduce PTS symptoms. NET allowed Hector to revisit multiple traumatic events chronologically and process them one at a time. Hector was encouraged to write his narratives to describe and process the traumatic events using his own words. Hector was unaware that some of his life events were as traumatic and impactful as they were. NET supported Hector in identifying and labeling traumatic events he was unaware of. Hector felt empowered to share his traumatic experiences through NET.
Erik had experienced chronic gender discrimination, bullying, and a traumatic car crash. At intake, Erik did not feel comfortable talking with others and did not want to use his voice to share his life events. NET provided space for Erik to write down his life events and share his emotional responses with written words and images. When Erik would feel stress or anxiety, his body would tremble, he would make little eye contact, and he had panic attacks. NET supported Erik in identifying his traumatic events, engaging in exposure within a safe, supportive environment, and feeling grounded and empowered in sharing his narratives. The clinician would often use clarifying questions to understand Erik’s responses when he spoke with a low tone or when he wrote down a word that was not written clearly, which helped to increase or shape his verbal communication. Erik was able to share the traumatic event with a supportive family member to reduce feelings of fear, worry, and guilt. Erik was also supported in building his confidence to talk to his gender health provider and advocate for his needs.
7 Course of Treatment and Assessment of Progress
NET begins with psychoeducation about PTSD and an orientation to the structure of NET: creating the lifeline (i.e., timeline of life events associated with trauma or resiliency), developing trauma narratives, and identifying “future flowers” (i.e., hopes and aspirations for the future). In the first activity (i.e., creating a lifeline), clients are asked to draw out or create a visual representation of their life since birth using rope or string, with symbolic items like stones and flowers used to mark key events or memories in their life. Clients identify traumatic memories, or “stones” (e.g., abuse, loss), on their lifeline and moments of resiliency or support, or “flowers” (e.g., meeting a good friend). These “stones,” or traumatic events, are processed using a narrative approach where clients are guided verbally or through written means in sharing their traumatic memories. Habituation, or gradual reduction in physiological arousal in response to the traumatic memory, is achieved through repeated exposure to the narrative either by the clinician reading the narrative to the client and/or the client re-reading aloud. Within this process, clients are encouraged to engage in reflection and meaning-making to support them in reducing the emotionality of their memories and developing new cognitions and beliefs about their experiences. For instance, a client may initially report feeling hot, shaky, and light-headed when first sharing their narrative. After subsequent exposures and processing, clients may report only feeling fidgety and having less anxiety during the reading. Clients who initially report feeling guilt or shame when sharing their narrative may, after processing, report having shifted thoughts and beliefs such as, “It wasn’t really my fault” or “I wasn’t the only person responsible.” After all stones have been processed, the clinician and client close the intervention with “future flowers,” which is an exercise focused on supporting the client to reflect on their NET process, explore hopes for the future, and consider new perceptions of their self and experiences within the context of healing (Schauer et al., 2011). To accommodate the additional barriers associated with SM, the clinician provided writing/drawing supplies, such as colored pencils, pens, a flip-page notebook, and paint. Clients were also encouraged to use the telehealth chat box and paint application during virtual sessions. For example, during sessions, Hector would begin by writing his narrative and then the clinician would read it out loud to ensure understanding. Hector also utilized pictures and symbols to depict his emotions and memories.
Part of creating gender-affirming, culturally responsive spaces for trauma-focused work, includes reflecting on clinicians’ own intersecting identities and lived experiences. The clinician working with Hector and Erik identified as genderqueer, brown, first-generation Latiné (i.e., Mexican-American), and had personally experienced and worked in several care systems. The clinician disclosed their genderqueer identity to build a space where Erik and Hector could feel less anxious and more comfortable when sharing their gender identity or trans experience. Integrating a gender-affirming approach included using asserted names and pronouns and supporting clients in processing their memories within their current gender identity to reduce gender dysphoria. This adaptation also helped to reduce the burden of reliving past traumatic events using their name assigned at birth, gender, and pronouns. Further, the clinician actively worked with both clients to process the role of machismo within Latiné culture to support them in feeling comfortable and safe to talk about their emotions and past trauma. Integrating such cultural contexts within a gender-affirming approach can be beneficial in promoting ancestral and intergenerational healing among Latino men (Delgado-Romero et al., 2022).
Hector: Sessions 1–2
Hector participated in-person during COVID-19 restrictions, such that masks were worn throughout the treatment. The clinician guided Hector in completing a lifeline with pen and paper. Hector and his clinician worked to illustrate positive and negative events in his life. Hector identified four traumatic events to process throughout treatment. Hector prioritized discussing childhood trauma, gender discrimination, the emotional loss of a partner, and negative religious experiences. Hector expressed feelings of relief when processing life events. After Hector shared his traumatic experiences or “stones,” the clinician helped him practice grounding exercises at the end of each session to support regulation following exposure and habituation.
Sessions 3–4
During these sessions, Hector and his clinician focused his narrative exposures on experiences of discrimination. Hector narrated memories of mistreatment and favoritism, describing the environment of these traumatic events. The clinician supported Hector in labeling triggers, such as yelling. Hector and his clinician wrote down feelings about gender discrimination. The clinician listened to Hector’s narrative about his family misgendering him. They also explored a hospital-based memory where providers misgendered him. The clinician reflected on Hector’s feelings of not being seen or heard by his family. Hector identified that his limited verbal communication stemmed from being misgendered. Hector also explored how childhood trauma and generational trauma had impacted him. Hector reported feeling more at ease after sharing past family trauma. During the session, Hector would draw on his hands and the clinician followed up on what the drawings meant to him.
Session 5–6
The next sessions focused on processing grief and the loss of Hector’s relationship with his partner. Hector wrote details of the relationship and events as part of his narrative exposure, which the clinician then read back to him. Hector and his clinician reflected on emotional abuse from his partner. The clinician validated Hector’s feelings of abandonment. At this time, Hector began to decrease communication and had greater difficulty writing down his feelings. Hector could not process the event at the end of the fifth session and wrote that he would like to move on. He and the clinician practiced grounding skills and processed physical feelings that started to appear. Hector identified wanting to move on to his next “stone.” In the next session, the clinician supported Hector in processing his experiences related to his religious upbringing and the associated traumatic events. The clinician validated Hector’s experience with forceful religious practices and gender discrimination in religious institutions. Hector wrote down detailed experiences of his memories during this time and processed his feelings associated with the clinician. At this time, Hector stated that he was comfortable ending NET soon.
Sessions 7–8
In the final two sessions, Hector identified the most salient traumatic events in his life and processed the most intensive memories with support from the clinician. In these sessions, Hector appeared happier compared to the previous two sessions. He did not engage in any drawing during these sessions. Hector and the clinician developed a care plan for future traumatic events should they occur. Hector engaged in “future flowers” and described his hopes and dreams to be open and express his gender identity. He explored options for how to express happiness for others and himself. He reframed negative thoughts about himself to be more positive and focused on self-love. Hector was observed to be able to name complicated feelings and events and demonstrated decreased negative emotional responses to them. Hector shared that he hoped to build healthier relationships and break the cycle of isolation. He shared that he learned a lot from NET and found support from his clinician. Hector ended his treatment after sharing the emotional abuse he received from his ex-girlfriend. The clinician asked Hector if he would like to process his abuse in a future session, but the client stated that he had shared and processed all his traumatic events and was ready to end treatment. The clinician validated Hector’s decision, autonomy, control of his narrative, and determination to finish treatment.
In assessing for outcomes at discharge, Hector continued to meet the criteria for PTSD per his score on the UCLA PTSD-RI. This may have been associated with the potentially premature termination of NET and the limited processing of some of his stones. Still, he reported a notable increase in his resilience score at discharge (i.e., increased from 24–42). There was no observed change in his score on the flourishing scale. At discharge, he no longer met the criteria for SM as he was observed to be able to verbally communicate and advocate for himself with his providers, both in NET and during medical appointments.
Erik: Session 1
In the first in-person session, Erik was primarily non-verbal. The clinician provided psychoeducation about the process of NET. Erik’s anxiety caused him to shake and become quiet at the beginning of the session. He exhibited little eye contact and looked down for most of the session. The clinician guided Erik in learning a breathing exercise to alleviate his anxiety symptom (i.e., shaking). In addition, the clinician acknowledged and encouraged Erik’s efforts to acquire new coping skills, including utilizing art to express his emotions. The clinician provided Erik with large pieces of paper, markers, and colored pencils to write down his past traumatic events and enjoyable memories as part of his lifeline activity. The clinician read back the life events that Erik wrote down. Erik and the clinician agreed to focus on four traumatic events that Erik experienced: the loss of his emotional support animals, early childhood bullying, gender discrimination, and a car crash. Erik drew pictures of his traumatic events and memories. Erik would draw his cat if he started to feel negative feelings. The clinician would ask questions to confirm responses, and then Erik would answer softly or write down his response. The clinician guided Erik through a grounding exercise at the end of the session. Erik ended the first session by showing pictures of his emotional support cat.
Session 2
Erik initially participated in this session using the chat box in the telehealth platform. He felt uncomfortable seeing himself on camera and had it off after the initial welcome. Erik then gradually moved to unmute his microphone and would share out loud in a soft, low-pitched voice. During his session, Erik struggled to answer open-ended questions about his emotional state, often giving brief responses like “ok” or “I don’t know.” However, he responded well to close-ended questions (e.g., “are you feeling anxious right now?”), indicating that he was comfortable with providing brief answers. The clinician noticed this pattern and adjusted their approach, checking in with Erik at the beginning of each session onward to ask if he was willing to share his thoughts. When Erik expressed hesitation or anxiety, the clinician would follow-up with more specific questions or allow him extra time to process his thoughts. For example, Erik might sketch his cat to indicate that he needed more time to reflect before answering a question. The clinician read the responses from the chat box for clarification and to encourage communication. Erik used the drawing application or chat box to communicate whenever he felt anxious. For example, Erik wrote that he would sketch his cat “Milo” to represent his anxious feelings when they would come up. The clinician would clarify with Erik and ask him if he was feeling anxious or to share any emotions using the chat box or drawing feature. The clinician utilized the telehealth drawing application, and Erik drew symbols and words that described the bullying he experienced. Erik shared that people would make fun of his gender expression. He began to feel anxious while sharing and started to draw fast with scribbles. Erik typed the details of people who would bully him while also providing detailed descriptions of the day, time, and type of environment. Erik shared that his peers would gaslight his feelings, leave him out of social events, and call him “crazy.” He shared that his fear of being judged stemmed from being bullied. Erik did not remember much of his interactions with peers and shared that writing his memories down was helpful. The clinician supported Erik with grounding exercises and doing a body scan to help him feel calmer at the end of the session. Erik drew his pet cat and shared that drawing animals helped ground him after sharing traumatic events. Erik and the clinician agreed that adding drawings of Erik’s favorite animals to help ground him would be beneficial.
Session 3
Erik appeared anxious and was nonverbal primarily at the beginning of the session, which was in-person. At the beginning of the session, he was shaking and avoided eye contact. The clinician would follow-up and clarify Erik’s responses when the clinician could not hear Erik’s low voice. The clinician asked Erik how he felt about processing a new “stone” during the session. Erik took several minutes to respond but wrote that he was open to sharing his trauma around the loss of emotional support animals. Erik stated that he values his emotional support animals as friends. The clinician guided Erik in an art activity to express emotion and feelings around the sudden loss of his emotional support animals and witnessing the loss. Erik wrote that remembering the images of his pet passing retriggers him and makes him shake. Erik’s eye movement was rapid when writing down his narrative. The clinician asked clarifying questions about the trauma event to elicit both “hot” and “cold” memories to integrate them. Erik wrote that remembering specific details of memory strengthens his appreciation for his current emotional support animal. The clinician supported Erik in drawing symbols that grounded him and helped him to calm down after the session.
Session 4
Erik did not speak at the beginning of the session. The clinician asked questions about the traumatic car crash Erik experienced. Erik wrote down specific details and drew pictures of the car crash. Erik later shared a short story that he wrote related to the crash. Erik shared that this day was an important part of his life because it was also when he felt a connection with his mother. Erik shared that when the crash happened, he was conscious and seeing his mother beside him caused him to experience self-blame. While Erik shared the crash details, he remembered memories that felt good and provided clear details of the day following the car crash. The clinician read back Erik’s narrative as part of the habituation process. The clinician validated Erik’s feelings of sadness, shock, and worry. Erik identified happy events before the car crash and reported greater habituation to this narrative by the end of session.
Session 5
In this session, Erik was observed to engage in some eye contact and was able to share small phrases aloud. He shared that he has two supportive friends online and that he was able to share his narratives with them while feeling safe. Erik wrote that he was grateful to process life events with someone without judgment. He also shared his car crash narrative with his mother. Erik wrote that it was his first time sharing his feelings of sadness and loss. At this point, Erik identified that he was ready to discontinue treatment as he had shared around his major “stones” and was experiencing less shame and guilt.
In assessing outcomes at discharge, Erik continued not to meet the full criteria for PTSD, though he continued to report symptoms in the areas of intrusion, avoidance, negative cognitions/mood, and dissociation. While he reported a decrease in resilience (i.e., 41 to 28), he reported an increase in his score on the flourishing scale (i.e., 21–35). Erik was also observed to no longer meet the criteria for SM as he was observed to be verbally communicative across a range of settings (e.g., in therapy, with medical providers, with family and friends).
Of note, Hector and Erik received support from their families during and after treatment. As part of their treatment, they were encouraged to share their personal stories with others if they felt comfortable doing so. Erik chose to share part of his story with his mother, while Hector shared his narratives with both a friend and his mother. This sharing of narratives may have contributed to symptom improvement. In addition to these services, Erik and Hector received gender-affirming medical care, which may have further improved their symptoms. Neither Hector nor Erik was actively receiving other therapy services while engaged in NET treatment.
8 Complicating Factors
While telehealth was available during the COVID-19 pandemic, Erik and Hector did not have private spaces to share or type responses via the telehealth platform. Hector did not have access to headphones to protect his privacy while around other family members. Hector agreed to participate in NET in-person but would commute about 116 miles roundtrip, totaling 3 hours. Erik’s commute was 70 miles roundtrip with a total commute time of 2 hours. Erik and Hector would mostly arrive tired from the commute. Due to the long commute, the clinician would offer water or a snack before each session. Hector’s treatment with NET started at the beginning of the COVID-19 pandemic. The clinician took multiple precautions, including using two plexiglass barriers, wearing masks and gloves, setting up a two-way screen, and deploying an air filter to reduce the risk of COVID-19 transmission during in-person appointments. However, when Erik opted for telehealth, it became challenging to fully perceive nuances in body language and facial expressions while processing trauma.
9 Access and Barriers of Care
The primary barrier to care for both clients was their SM during treatment. In addition, Erik and Hector had difficulties accessing mental health care in their area which was considered gender-affirming, trauma-focused, and flexible regarding their communication challenges. During COVID-19 and Los Angeles’ stay-at-home order, Hector was referred for NET, which presented additional unique barriers. Hector lacked privacy at home and was unable to access video applications, so his parents assisted him with transportation to the appointment. The clinician needed additional time to prepare and sanitize their equipment before and after the appointment.
Erik participated in NET both through telehealth and in-person at the clinic. Erik could not make it into his lifeline session in person. He used the telehealth platform with his camera off and used the chat box feature. NET often uses physical objects in building a lifeline. Erik could not physically participate in this activity, which was a barrier to creating the lifeline as intended by the developers. The clinician asked Erik to utilize the draw feature on the telehealth platform and images or symbols that represent his memories to create his lifeline visually.
10 Follow-Up
As part of the clinic protocol, the clinician conducted a 6-month follow-up with Hector to assess for symptoms of PTSD, resiliency, positive well-being, and any functional improvement. Hector reported that symptoms dramatically decreased by his 6-month follow-up visit; more specifically, while Hector had continued to meet all criteria for PTSD at discharge from NET, 6 months later, he only met two of the four criteria (i.e., intrusive symptoms, arousal). In addition, Hector’s resiliency and flourishing scores continued to increase post-discharge. More specifically, his resiliency follow-up score was 30% higher compared to baseline and 12% higher compared to discharge, suggesting improved ability or resources to cope with stressful events. His flourishing follow-up score was unchanged from baseline to discharge, and approximately 7% higher from discharge to follow-up. The clinician also observed continued improvement in Hector’s functional communication, such that he had experienced a full remission of his SM symptoms and was able to verbally communicate across all domains of his life. At the follow-up evaluation, Hector communicated verbally in a soft tone. His mother told the clinician that he talks more often than he used to but still speaks with a low voice. Hector mentioned that he prefers not to speak louder and feels uncomfortable with the sound of his voice. Additionally, it was concluded that Hector didn’t meet the criteria for SM. Moreover, Hector’s mother mentioned that he had been more sociable lately and wanted to participate in more activities with friends.
PTSD symptom endorsement as assessed by the UCLA PTSD-RI for DSM-5 at baseline, discharge, and 6-month follow-up for Hector and Erik.
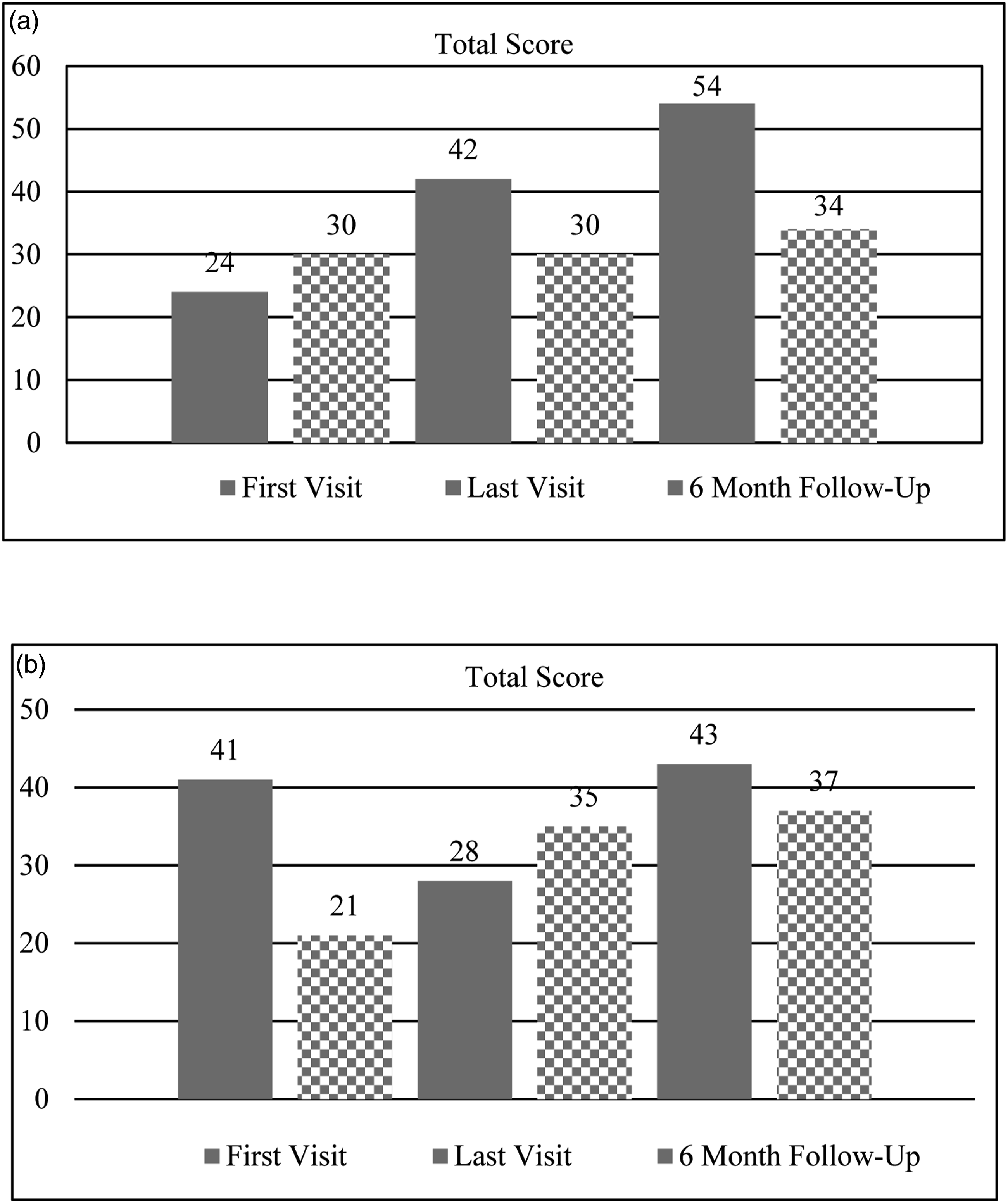
Total Scores for Connor-Davidson Resilience Scale (solid) and Flourishing Scale (checkered) at baseline, discharge, and 6-month follow-up for Hector (a) and Erik (b).
11 Treatment Implications
One of the major treatment implications is the demonstration of the use of NET with two transgender youth presenting with PTS symptoms and SM. While research has documented the effectiveness of NET in reducing trauma-related symptoms for many vulnerable populations, most studies have focused on refugees and displaced persons from non-Western countries (Lely et al., 2019). However, a few studies have begun to apply this intervention to TGNB populations who are disproportionately impacted by trauma (e.g., Julian et al., 2023; Lange, 2020). This case series demonstrates key considerations and modifications for narrative-based treatment to facilitate crucial trauma-focused healing, specifically for TGNB youth. Moreover, as demonstrated in these case studies, talk-based, trauma-focused treatment is possible with TGNB youth who present with SM. For these youth, the flexible use of telehealth and other written modalities, which facilitated shaping and gradual exposure, lead to an unexpected remission of SM symptoms alongside reduction in trauma symptomatology.
There were several limitations in these case studies. Both clients elected to participate in NET either wholly or partially in-person, which was an asset to their treatment, especially as treatment was provided in the context of the ongoing COVID-19 pandemic. Thus, we were unable to determine whether these modifications would be as effective if delivered fully via telehealth. Though additional work is needed to evaluate these modifications via telehealth, existing guidelines and case research support the adaptation of NET for online delivery (Kaltenbach et al., 2021; Olavarrieta & Benuto, 2022). Moreover, outside of outcome data collected, there was limited information on additional supports and resources that were available during this time which may have impacted the clients’ progress and maintenance of treatment gains following NET. For one client, there was not a significant change in his PTSD symptoms immediately at discharge. It may be that additional sessions would be beneficial to observe a decrease in PTSD symptoms. However, it appeared that a potential reduction in anxiety vis a vis treatment led to significant improvement in SM, which may also be associated with his increase in self-perceived resiliency and well-being.
In addition, both clients presented in this case series identified as transmasculine, though the clinic in which these clients were seen serves youth and young adults across the gender-diverse spectrum, including transfeminine, non-binary, and genderqueer individuals. At the time, only transmasculine clients had presented with comorbid SM and PTSD symptoms. This may be aligned with prior research indicating greater prevalence of anxiety, and social anxiety specifically, among transmasculine individuals (Millet et al., 2017), which may increase likelihood of SM especially among those with higher anxiety and potentially with trauma exposure (Vogel et al., 2022; Wong, 2010). In general, modifications related to the intervention are further detailed in another publication (Julian et al., 2023) and are tailored based on the client’s gender identity and experiences of gender-based trauma. Prior research highlights the importance of considering the nuanced experiences of different gender minority identities (e.g., Lefevor et al., 2019). Thus, modifications to address the unique stressors experienced by individuals of different gender-diverse identities, including messages around transphobia and gender-based trauma, particularly for transfeminine and non-binary individuals should be addressed. This remains an area for future research and intervention development.
These case studies contribute to growing support for the use of NET with TGNB youth to address trauma-related symptoms, while also identifying additional modifications and accommodations to support youth with gender-based trauma and with SM. The clinic in which these youth accessed care aims to identify the necessary modifications to be able to more adequately and fully address the range of trauma experiences reported by youth, including gender-based invalidation, discrimination, and abuse. Future research is needed to further understand the relationship between such trauma experiences and SM, as well as explore how these modifications support the reduction of PTSD symptoms for TGNB youth.
12 Recommendations to Clinicians and Students
Research has shown that NET is effective in reducing PTSD symptoms, particularly among marginalized and minoritized communities, as the narrative-focused, testimonial approach is posited to be less stigmatizing and more empowering (Wright et al., 2020). This is one of the first case studies to report on the use of NET with TGNB youth, building upon prior research which has explored its use with older TGNB population (Lange, 2020). In addition, both TGNB youth presented with SM, a diagnosis that would often be identified as a barrier or exclusionary criteria for engaging in trauma-focused treatment due to the challenges with verbal communication and high levels of anxiety. However, as observed, Hector and Erik’s experiences in NET demonstrates the potential for significant improvement in a range of mental health symptoms, potentially rooted in the impact of childhood trauma. The use of NET is recommended with TGNB youth to include specific focus on gender-based trauma experiences, which are rarely and explicitly included in trauma-focused treatment. While more recent models of TGNB care encourage clinicians to identify and address these experiences as leading to internalized negative core beliefs and ongoing minority stressors (i.e., Matsuno & Israel, 2018), few interventions to date have explored the explicit identification and processing of gender-based trauma, including microaggressions, invalidation, and hate crimes. Despite limited research, these case studies highlight the importance of explicitly naming and addressing these experiences when treating trauma in the TGNB community. Doing so acknowledges and empowers gender-diverse youth to voice and heal from such traumatic experiences and is grounded in a social justice approach.
Further, it is recommended that clinicians work to address any biases that may create barriers to engaging in trauma-focused treatment with TGNB youth with SM. As noted, challenges with communication may preclude clinicians from attempting to engage in trauma treatment without first trying to increase functional communication. This case series demonstrates that it is possible to address both simultaneously. In fact, addressing one of the sources of anxiety (i.e., trauma symptoms) may over time also lead to the reduction in SM symptoms, as observed by the clinician. At the end of treatment, though focused interventions targeting SM were not employed, the clinician observed remission of SM symptoms with continued remission 6-months after treatment was discontinued. This case series highlights the potential for therapeutic effectiveness of NET in reducing PTSD symptoms and increasing resilience and psychosocial functioning in TGNB youth with SM using a gender-affirming, flexible, and supportive approach.
Footnotes
Acknowledgments
The authors would like to thank the youth who allowed us to share their experiences and the team in the Trans Community Trauma Treatment Center at Children’s Hospital Los Angeles for their support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Substance Use and Mental Health Administration grant (1H79SM082875).