
Abstract
Comorbid diagnoses including autism spectrum disorder, bipolar disorder, schizophrenia, and intellectual disability can present a variety of personal barriers and challenges to interventions that promote safety and autonomy. The current case study provides an overview of a 10-week intervention that included elements of Acceptance and Commitment Therapy and contingency contracting to target psychological flexibility and aggressive behavior in a 17-year-old presenting with these comorbid diagnoses. The treatment was fully individualized to include the client’s interests in Star Wars and focused on supporting the client’s self-identified valued outcomes associated with independent living. Prior to intervention, baseline data showed high levels of aggressive behavior in both frequency and duration, and low levels of psychological flexibility and adaptive behaviors were reported. Following implementation of the combined intervention, aggressive behavior reduced significantly below baseline levels, psychological flexibility improved, and the client engaged in a greater frequency of adaptive behaviors relative to baseline. Positive outcomes were also maintained 1-month and 1-year following the intervention. Implications of this case for clinicians and staff are discussed.
1 Theoretical and Research Basis for Treatment
Empirical evidence suggests that there are increased rates of co-occurring psychological disorders in adults with autism spectrum disorder (ASD; Varcin et al., 2022). Autism as a singular diagnosis can be pervasive and result in substantial variability in life outcomes while presenting challenges to social communication, independent living, and employment opportunities. Comorbidity of psychiatric diagnosis can also increase the likelihood of negative outcomes throughout the lifespan. For example, there is a growing rate of bipolar disorder (BD) presenting in people with ASD with a higher incidence rate in males than females (Dunalska et al., 2021; Varcin et al., 2022). Other psychological disorders such as schizophrenia (SZ) may also present in autistic populations. While ASD is generally diagnosed at a younger age, SZ is more developmentally prominent in adulthood (Rapoport et al., 2009). There are similarities in symptom expression between SZ and ASD, such as atypical perception and communication, and repetitive and/or restricted interests (Cochran et al., 2013; De Crescenzo et al., 2019). While SZ often presents with delusions and/or hallucinations, related characteristics of ASD are that of anomalous emotional and social engagement. Comorbidity among ASD, BP, and SZ is complex in its diagnosis and intervention research with this population is limited. However, research has found that the quality of life for individuals with these diagnoses can be low and accompanied by deficits in neurocognitive functioning, irritability, and aggression, among other behavioral challenges (Frazier et al., 2002).
These experiences can limit access community activities, gaining and maintaining employment, and finding housing or residential placement, even when doing so represents a valued outcome for autistic individuals and their families. Kanne and Mazurek (2011), for example, examined rates of aggression in autistic children between the ages of 4 and 17 years and concluded that, of the 1380 participants, 68% engaged in aggressive behavior towards a caregiver and 49% exhibited mild to severe forms of aggression towards non-caregivers. Severe behaviors such as aggression are often predictors of lower quality and high-stress family dynamics (Hwang et al., 2015) and can lead to decreases in overall well-being (Fitzpatrick et al., 2016). In the current case, the client was diagnosed with ASD, BD, SZ, and an intellectual disability while demonstrating several behavioral symptoms evident within each of the disorders. A recent study of ASD rates found that more than one-third of autistic children were classified as having an intellectual disability (Maenner et al., 2021), which are together predictive of mental and physical health challenges (Bishop-Fitzpatrick & Rubenstein, 2019). In this case, high rates of aggressive behavior were a major barrier to the client independently accessing his community and obtaining residential placement, both of which were expressed values and interests of the client and his family.
Two intervention approaches served as the basis for the present case study: Acceptance and Commitment Therapy (ACT) and Contingency Contracting (CC). ACT is a behavior analytic approach that integrates behavior change techniques to increase psychological flexibility and well-being and reduce maladaptive, rule-governed behaviors that cause psychological distress. Psychological flexibility is defined as the “ability to contact the present moment more fully as a conscious human being and to change or persist in behavior when doing so” (Hayes et al., 2004, p. 7). Much of the research involving ACT-based approaches has occurred in randomized controlled trials (e.g., Shawyer et al., 2017). Given the uncommon expression of ASD, BP, and SZ, however, there are gaps in the literature regarding the utilization of ACT with individuals with this comorbid expression that may benefit from clinical case study research. For example, Velga-Martinez et al. (2008)bib_vm_2008bib_vm_2008 evaluated the utility of an ACT-based intervention with a 30-year-old male experiencing auditory hallucinations demonstrating the logic and effectiveness of the intervention approach. More recently, Chapman and Evans (2020) utilized an art-based ACT intervention to support an adolescent female to reduce anxiety and improve wellbeing over the course of an 8-week intervention. In both of these studies, the clinical case study format allowed for analysis of the progression of the intervention in highly idiosyncratic cases, both extended from a common approach to intervention rooted in ACT.
One streamlined approach that could provide a starting point in clinical settings providing intervention for youth is the Accept.Identify.Move curriculum (AIM; Dixon & Paliliunas, 2018). AIM includes daily lessons, practice items, and a point tracking system to reinforce positive and flexible behavior. In the current case study, we adopted and personalized 20 lessons from AIM based on the participant’s interests. The AIM point system was also adjusted to contain a contingency contract (CC). CC is a collaborative approach that establishes a written agreement between the individual and the teacher or caregiver to set up reinforcers contingent on the established behaviors and has been shown to be an effective addition to interventions with autistic populations (see Alwahbi & Hua, 2021 for comprehensive review; see Gregori et al., 2023 for clinical case study). Moreover, as noted by Wisniewski and Ben-Porath (2015), CC is a form of contingency management that “may be a highly effective and valuable intervention for patients with complex and multi-diagnostic presentations” (p. 135).
In the current case, the combined AIM+CC was developed to decrease the rate and duration of aggressive behaviors while improving reported psychological flexibility and opportunities for social experiences and transitioning to more independent living. We placed emphasis on decelerative and accelerative behavior change and gave the client opportunities to be an active member of his intervention development team in all intervention elements to promote assent, engagement and commitment to making values-based changes in behavior.
2 Case Introduction
James was a 17-year-old white male with a history of multiple treatment providers and diagnoses. While James’ Individualized Education Plan contained no reference to mental health diagnoses at the time of referral to his most recent alternative school setting, previous psychological evaluations indicated he has been involved in psychiatric treatment since age 3 years, including at least seven placements in various psychiatric treatment centers, the longest of which was 13 months. Over time and treatment providers, James had received several diagnoses including attention deficit hyperactivity disorder (ADHD), combined type, autism spectrum disorder (ASD), bipolar disorder (BP), unspecified bipolar and related disorder, disruptive behavior disorder, not otherwise specified, disruptive mood dysregulation disorder (DMDD), mild intellectual disability (ID), oppositional defiant disorder (ODD), schizophrenia (SZ), childhood-onset, and schizophrenia, disorganized type, under partial control with medication.
Consistent with a BP diagnosis, James has reported and presented periods of rapidly shifting moods ranging from predominant irritable mood to periods of increased energy, often demanding to engage in many simultaneous activities such as shopping, party planning, and movie production, which despite his interests, he has little to no knowledge or experience. As indicated in past psychological evaluations, James SZ symptoms have included hallucinations and delusions, incoherent speech, grossly disorganized behavior, and sensory deficits such as negative empathy, no insight into his behavior, and a tangential thought pattern. Evaluations suggested that James’ psychotic episodes have been mitigated by medication. James’ medication history at the time of services included antipsychotic, antidepressant, anti-anxiety, and bipolar disorder related medications. Additionally, at the time of services, James’ presented clinical characteristics that are consistent with a diagnosis of autism spectrum disorder (American Psychiatric Association, 2022). Results of a recent parent-completed Gilliam Autism Rating Scale-3 (Gilliam, 2014) supported a diagnosis of Autism Spectrum Disorder, Level 3 – Requiring Very Substantial Support for deficits in social communication and restrictive, repetitive behaviors, with accompanying intellectual impairment.
With intensive training, James was able to demonstrate independently completion of some daily living tasks such as washing tables and windows, sweeping and vacuuming floors, and self-care skills like brushing teeth, showering, dressing himself, and preparing simple meals (evaluated using the LIFE Functional Assessment, Dixon, 2021). Results of a recent parent-completed Adaptive Behavior Assessment System (ABAS-II) indicated that James’ General Adaptive Composite score was at the 0.1 percentile overall. Further evidence of a diagnosis of mild to moderate intellectual disability (ID) comes from James’ two most recent IQ assessments (i.e., Wechsler Intelligence Scale for Children and Wechsler Adult Intelligence Scale) that resulted in Full Scale IQ scores of 55 and 59, respectively. In summary, given James’ history of psychiatric treatment at an early age, multiple referrals for psychiatric inpatient treatment, consistent diagnoses and clinical presentation of ASD, BP, SZ, and intellection disability, these appeared to be the most relevant diagnoses within the current clinical case study.
Prior to referral to his current alternative school program, James’ resident school district was located in a community of fewer than 2000 residents and served k-12 students from several surrounding towns in two rural counties. The district did not have the special education services to meet James’ needs nor the transportation staff or vehicle that could keep James and staff safe during the more than 3-hour daily round trip commute to an alternative school-based day-treatment program that James attended to better accommodate his educational, social, emotional, behavioral, and mental health needs. James’s mother provided daily transportation to and from his alternative treatment program. For both James and his mother, the daily trip was one of few excursions from home that they felt was feasible and safe for James.
3 Presenting Complaints
James was referred to his current alternative school program after he was discharged from an inpatient residential treatment center due to multiple elopement attempts and physical assaults of others. James presented similar problems towards his mother at home, including property destruction (e.g., James removed the door molding of the front door of his home in an attempt to run away), threats of life-changing physical harm to his mother (e.g., James attempted to run over his mother with a lawn mower while telling her that he wanted to kill her), running away from home, breaking into neighbors’ homes (and subsequently threatened with a firearm by homeowner), and police contacts for property destruction and refusing to leave stores until he was given what he demanded. James’ social, emotional, and behavioral presentation prevented him from pursuing and benefiting from activities such as shopping, spending time with friends, participating in school-based extracurricular activities, and other social activities. James’ mother indicated that, at home and in the community, antecedents to his aggression and elopement typically included situations when he does not get what he wants, transitions from one setting or activity to another, misinterprets what is to happen, e.g., thinks his mother is going to take him shopping and she has no plans to do so, wants his mother’s attention, and wants to avoid having to do chores. School staff indicated that academic or behavior instructions are the antecedent in 76% of behavior problems, transitions between activities account for 11% of behavior problems, and correction by adults is an antecedent for another 13% of behavior problems. More than 73% of behavior problems occur during the first 2 hours of the school day, lending further support that transitions from less (e.g., home) to more (e.g., school) structured settings are a challenge for James. At the time of the intervention, James' history of aggression and elopement also prevented him from being accepted into multiple residential placements during the first 2 years he was enrolled in the program.
4 History
Prior to James’ placement in the program, he attended several placements in residential treatment facilities and alternative school programs. Placements had been terminated due to daily attempts to elope and physical aggression toward peers and staff. Injuries to staff have included minor cuts and bruises, broken bones, and lost time due to injury. In the 2 years prior to the intervention, James’s mother had made several applications to residential programs in his state of residence. All applications were denied. At the community level, family trips to grocery and retail stores resulted in property damage and the involvement of local law enforcement. Data from James’s current day-treatment program indicated that during the 2-months prior to the present intervention, James presented an average of 146 min of aggressive behavior per week. Academic instruction and transitions from one class or activity to another preceded 59% of James’ aggressive events in the program.
5 Assessment
Prior to the start of the intervention, the treatment team included two university-based behavior analysts and graduate assistants/behavior technicians, 1 day treatment program behavior analyst, and 1 day treatment research psychologist. The team consulted with James’ mother and IEP team to choose the correct assessment and procedural layout for the case. Several pre-assessments were identified to gain a thorough understanding of James’ challenges, guide intervention development, and outline client, parent, school program staff, and involvement of university case consultants.
Subjective Units of Distress Scale
Prior to the start of services, we conducted an interview with James’s mother to assess her priorities to be addressed with the intervention. During the interview, the Subjective Units of Distress Scale (SUDS; Wolpe, & Lazarus, 1966) was used to help identify which of James’ challenging behaviors were of greatest concern to her and assess her level of concern with the target behaviors that she chose. James’ mother was asked to rate her feelings about target problems and situations on an 11-point scale from 0 (totally relaxed) to 100 (Highest distress/fear/anxiety/discomfort that you have ever felt). A score of 80 or higher has been used as a cutoff for inclusion in prior studies (e.g., Salas et al., 2011). The SUDS has been found to have good psychometric properties (Kim et al., 2008). James’ mother provided a rating of 100 for concerns with James’ threatening behavior toward her and for the risk he presented to himself and others when he ran from home, broke into others’ homes, or was gone for extended periods of time despite her searches and those of law enforcement.
Open-Ended Functional Assessment Interview
The Open-Ended Functional Assessment Interview (OEFAI; Hanley, 2012) is a 20-item interview process designed to gain further information about the topography of target behavior(s), which behaviors should take precedence, and the fundamentals of antecedent and consequential events (Hanley, 2012). The OEFAI was selected to assess the function of James’ aggressive and elopement behaviors and guide intervention development. Open-ended FAI questions were created to be accessible for therapists to interview caregivers, staff, and/or clients with varying levels of functioning with a goal of assessing the core functions of behavior, i.e., attention, tangible, escape, avoidance, and/or sensory. The interview component of gathering James’ function of behavior provided opportunity for his mother and school staff to contribute to treatment development. After the interview, results, and determination of function(s) were reviewed by the treatment team. OEFAI results from interviews with James’ mother and school staff suggest that James’ target behaviors serve primary functions of escape from non-preferred task demands, gaining attention from others, and accessing rewards and preferred activities.
Question About Behavioral Function
The Question About Behavioral Function (QABF; Matson & Vollmer, 1995), is comprised of 25 items with the intention of assessing the function of a client’s behavior. The QABF utilizes a Likert scale (e.g., X = Doesn’t Apply, 0 = Never, 1 = Rarely, 2 = Some, 3 = Often) approach to measure how closely a respondent agrees or disagrees with a series of provided statements. The QABF was selected to assess and validate the function of James’ aggressive and elopement behaviors and guide in developing the intervention and to provide an additional data point to guide the functional assessment. The QABF subscales include attention, escape, non-social, physical, and tangible with five items representing each subscale. Respondents are asked to indicate either that the item does not apply to this client or identify the frequency with which target behaviors occur using a 4-point Likert scale (i.e., Doesn’t Apply,X to Often Applies, 3; Matson & Vollmer, 1995). Scoring is completed by summing scores for items related to each subscale with the highest subscale scores indicating the potential function of the target behavior. QABF results from James’ mother and school staff indicated that primary functions of James’ aggressive and disruptive behaviors were consistent with OEFAI results supporting a combined function of escape and access to tangible activities.
Children’s Psychological Flexibility Questionnaire: Caregiver Report
The Children’s Psychological Flexibility Questionnaire (CPFQ; Dixon & Paliliunas, 2018) is designed to assess a client’s psychological flexibility from the perspective of the client and the client’s caregivers. The CPFQ was selected to obtain the perspectives of James’ psychological flexibility from key adults in James life. The CPFQ also serves to validate James’ self-rating of his psychological inflexibility (i.e., an inverse of his psychological flexibility rating). Psychological flexibility is described as one’s ability to flexibly respond to one’s challenging life conditions in ways that are aligned with one’s values and goals. Acceptance and Commitment Therapy (ACT) and training have as a goal of increasing one’s psychological flexibility. The CPFQ has reasonable psychometrics and has been found to be appropriate for the assessment of psychological flexibility with children and adults (Lenoir et al., 2022). Both client and caregiver questionnaires are comprised of 24 questions with response options of a 5-point Likert-type scale ranging from Never (0) to All the Time (4). Scores range from 0 to 96 with higher scores indicating greater psychological flexibility. For the purposes of this case, the CPFQ-Caregiver Report was completed by school staff and James’ mother. CPFQ subscales are aligned with the six core concepts of the ACT Hexaflex (i.e., contact with the present moment, acceptance, defusion, self-as-context, committed action, and values; Hayes et al., 2004). Subscale ratings are summed to obtain an overall score providing perceptions of James’ psychological flexibility by key adults in his life. Results from the CPFQ completed by school staff and James’ mother suggest that prior to the start of the intervention, James demonstrated psychological inflexibility in multiple areas.
Avoidance and Fusion Questionnaire for Youth
The AFQ-Y8 (Greco et al., 2008) is a shortened version of the 17-item Avoidance and Fusion Questionnaire for Youth and is intended to assess older children’s and adolescents’ self-reported psychological inflexibility. Psychological inflexibility among children and adolescents often results in the use of habitual behaviors that are detrimental to one’s development of healthy, prosocial behaviors. In James’ case, he frequently relied on aggression and elopement to escape from non-preferred demands, gain attention from others, and access preferred items and activities. He rarely independently thought of alternative, helpful strategies to gain what he wanted. This shortened form is composed of eight items such as “My thoughts and feelings mess up my life.” and “I stop doing things that are important to me whenever I feel bad.” Respondents are asked to rate how true each item is on a 5-point Likert scale (0 = Not at all true; 4 = Very true). Scores for the AFQ-Y8 can range from 0 to 32 with higher scores indicating client psychological inflexibility. Studies report that the AFQ-Y and AFQ-Y8 are psychometrically sound (Greco et al., 2008). The AFQ-Y8 was read to James by a familiar staff member and James’ responses and comments were recorded verbatim. James’ pre-intervention AFQ-Y8 results are consistent with parent and school staff results from the CPFQ (i.e., James has fairly rigid cognitive processes).
PEAK-Equivalence Pre-Assessment
The Equivalence module from the PEAK Comprehensive Assessment (Dixon, 2019) was used to determine if an ACT-based approach would be appropriate for James, where this type of intervention may not be appropriate when learners do not demonstrate derived relational responding. The PEAK Equivalence assessment tests for concepts such as Reflexivity (matching stimuli, such as A = A), Symmetry (deriving relations in an untrained direction, such as A = B; therefore B = A), Transitivity (deriving relations among untrained stimuli, such as A = B and B = C; therefore A = C), and Equivalence (deriving relations among two or more untrained stimuli such as A = B and B = C; therefore, A = C and C = A). Results from the PEAK Equivalence assessment suggest that James possessed the verbal and cognitive skills necessary to participate in and benefit from the intervention (Dixon, 2015).
Social Validity Questionnaire
We created a social validity questionnaire to assess changes in behavior occurring in James’ home as a measure of intervention progress. Social validity describes the degree to which changes in the behavior are perceived as meaningful to those involved. In this case, we conducted the social assessed changes in James’ use of language to communicate with others and changes in James’ challenging behavior. Both assessment areas contained 5 Likert-Scale type questions ranging from Strongly Disagree to Strongly Agree, where a response of 5 suggested no change in behavior during the intervention relative to the period prior-to the intervention occurring. The questions and responses obtained from James’ mother, teacher, and behavior specialist are summarized in the results section.
6 Case Conceptualization
Priority outcomes identified by James, his mother, and the team were to increase access to typical young adult social experiences with James’ particular interest in shopping for preferred toys and food items. James’ mother’s priorities were reductions in elopement and aggression and acceptance to residential services. Based on assessment results, the team hypothesized that James’ elopement and aggression functioned as (a) escape from non-preferred tasks and limitations to activities and (b) access to preferred items and experiences. These functions suggested that supporting change in James’ response to inflexible, unhelpful, and harmful thought processes, coupled with learning alternatives to his habitual behavioral responses to angry and frustrated feelings would be treatment priorities. Interventions grounded in ACT appeared to be effective influencing James’ aggressive behaviors and promote greater access to the community through intervention. In particular, AIM lessons were developed to focus on James’ stated values of accessing his community more fully (which was restricted due to his aggressive behavior). Present moment exercises were designed to assist James in noticing urges to engage in aggressive behavior and thoughts that showed up in those moments. Acceptance exercises were designed to assist James to not only notice challenging thoughts and urges to aggress towards others, but to accept those feelings in the moment and commit to engaging in alternative response strategies, like walking away or engaging in defusion exercises like saying the thought in Yoda’s voice. One example of an adapted activity included labeling an X-Wing stuck in the swamps of Dagobah as James’ value and having James mention committed actions, where each committed action served as the force to pull the X-Wing out of the swamp. Self-as-context activities were designed to weaken self-as-content labels and were largely based around the light-side and the dark-side of the force (e.g., Anakin Skywalker is still Anakin, his past behavior does not define who he is here-and-now).
7 Course of Treatment and Assessment of Progress
Course of Treatment
James’ 10-week treatment began near the conclusion of the regular school year and continued through the summer sessions. Follow-up data were collected during the first 6 weeks of the following school year at 1-month post-intervention. The intervention included two primary changes in James’ weekly routine: (a) strategically identified lessons from the AIM curriculum that occurred twice weekly, and (b) a CC that included an adapted token economy with which James was familiar. All intervention elements were themed based on Star Wars. Information about the AIM curriculum and a copy of the CC was shared and reviewed with James, his mother, and school staff.
AIM Curriculum
AIM Lesson Adaptation Examples.
Contingency Contract
Contingency contracts (CC) have a long history of use with students of various age who present with a variety of diagnoses and challenging behaviors (Alwahbi, 2020). In the current case, the CC was developed collaboratively by James, his mother, and agency staff after completing a task analysis of safe community exposure. The CC focused on values identified by James and his mother for achieving greater autonomy and independence and safely accessing community-based activities. This CC was presented to James as an agreement to work towards his goals and consisted of five skill sets aligned with (a) preparing for shopping, (b) traveling to the store, (c) shopping in store, (d) traveling home, and (e) putting away purchased items. A visual component for tracking his progress in obtaining daily points was incorporated by adding an outline of Yoda on the back of James’ point sheet that graphically indicated how many points James earned that day. James’s mother adapted the contingency contract for use at home to include contingently earned activities and items, however, James did not earn points nor were points transferred from home to James’ school total.
Assessment of Progress
Aggression Results
Two dependent variables were measured throughout the case study, including the frequency (tracked through time sampling) and duration (on-set to off-set of aggressive episodes) of aggression. James’ school day started at various times throughout the intervention for a variety of reasons ranging from delays due to behavior problems at home to road construction during the daily commute to the school program. To compensate for the inconsistent length of James’ school days the percentage of each school week during which James presented aggressive behavior was calculated. The percentage of each school week spent in aggressive behavior was computed by summing the total number of minutes of weekly aggression (e.g., 135 minutes), dividing the sum by the total number of minutes James spent at school each week (e.g., 1200 minutes) and multiplying the result by 100 (e.g., 11.3%).
As shown in Figure 1, James presented aggressive behaviors, on average, during 18.8% of his school week during baseline (Range = 14.1% - 26.5%). During the 10-week intervention, James’ rate of aggressive behaviors decreased, on average, to 8.6% of the week (range = 0.0%–16.7%), or less than half of his baseline aggression. During the 6-week follow-up period, the percentage of the school day that James’ presented aggressive behaviors continued to decrease, on average, to 6.0% of the week (Range = 0%–12.5%). Overall, James’ rate of aggressive behaviors decreased by 68.1% from baseline to 1-month follow-up and decreased by another 37% at 1-year follow-up (Figure 1). Percentage of school day engaging in aggressive behavior.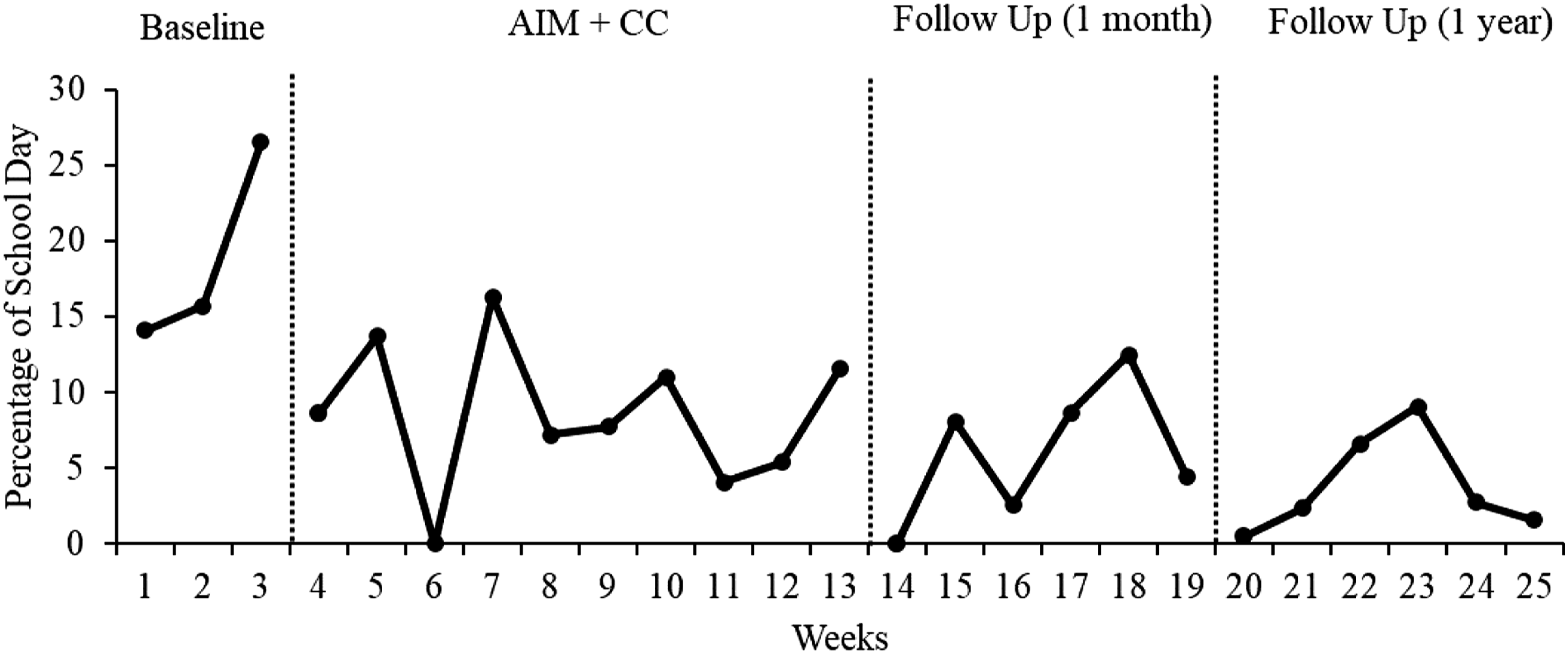
We also tracked the duration of James’ aggression and reported the most severe aggressive episodes as the longest in duration. The total number of minutes of the most severe incident per day was summed across each week of school which provided a total number of minutes per week of James’ most severe behavior. As shown in Figure 2, James presented, on average, 207.3 minutes per week during baseline (Range = 164 – 294 min) of severe aggressive behavior. During intervention and follow-up phases, rates of severe aggression decreased, on average, to 110.0 min (Range = 60 – 156 min) and 82.0 min (Range = 40 – 130 min), respectively, a decrease of 60.0% from baseline to 1-month follow-up; then, increased, on average, by 18%–97 min at 1-year follow-up (Figure 2). Total minutes of most severe daily incidents per week.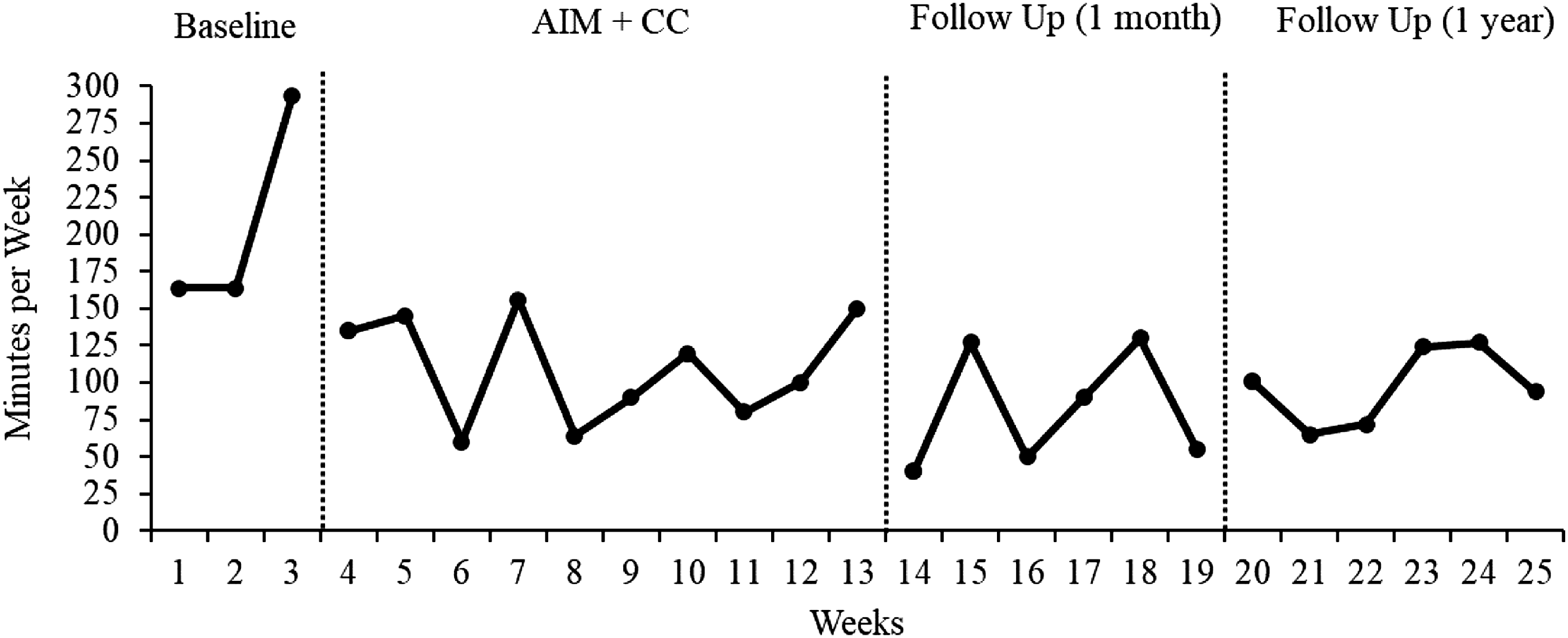
Contingency Contract Results
James earned points throughout the day for prosocial behaviors such as making a list of things to do during the first and second half of the day (similar to making lists of items to purchase during a store visit) and practicing other shopping related interactions such as arriving to school on time, following directions, asking for permission, and accepting decisions without arguing or aggression. Points earned on James’ contingency contract were summed, entered into a database daily, and made available to James each Friday for use at the school store which included a variety of items such as preferred snacks, posters, and time to engage in preferred activities. During the 10-week intervention, James earned an average of 117 points per day (Range = 62–213). The average daily point total increased to 168 points per day during the 1-month follow-up period (Range = 119–197) and decreased slightly to 151 points per day at 1-year follow-up (Range = 65 to 215; Figure 3). Average daily number of contingency contract points earned per week.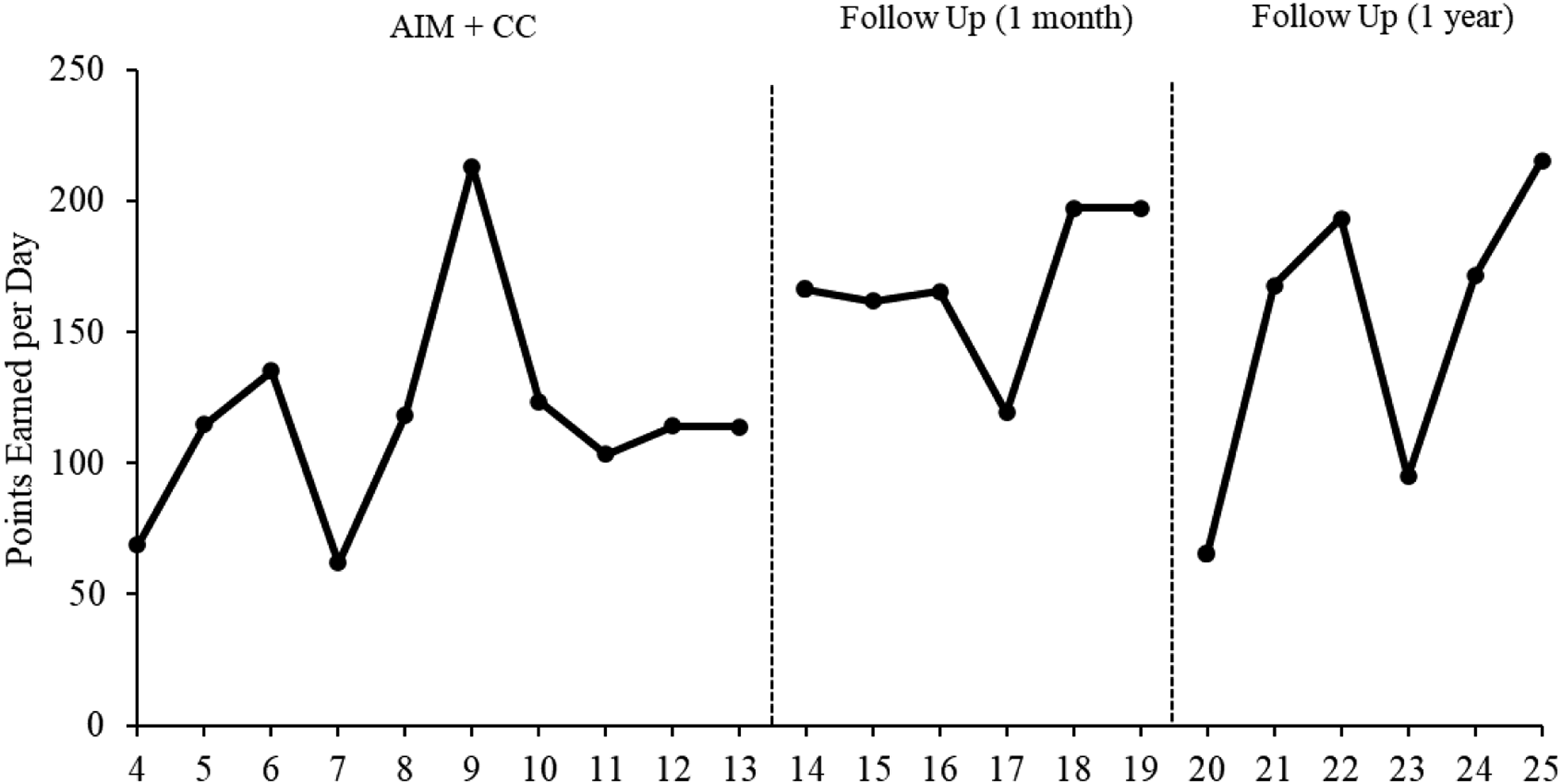
Psychological Flexibility Results
Changes in psychological flexibility were measured using the AFQ-Y8 over the course of baseline and during the intervention. We used the AFQ-Y8 because of prior use in intervention research and established psychometric properties of the measure. High scores on this measure suggest that a participant is psychologically inflexible. As shown in Figure 3, James’ scores decreased significantly across measurement periods on the AFQ-Y8, supporting that improvement in psychological flexibility may have been a process that facilitated reductions in aggressive behavior observed in this case. We do see an increase during the 1-year follow-up in psychological inflexibility; however, this score was still below baseline levels as shown in the figure (Figure 4). Acceptance and fusion questionnaire for youth (AFQY-8): Participant Results. Note. Higher scores indicate higher levels of psychological inflexibility; lower scores indicate higher levels of psychological flexibility and lower levels of psychological inflexibility.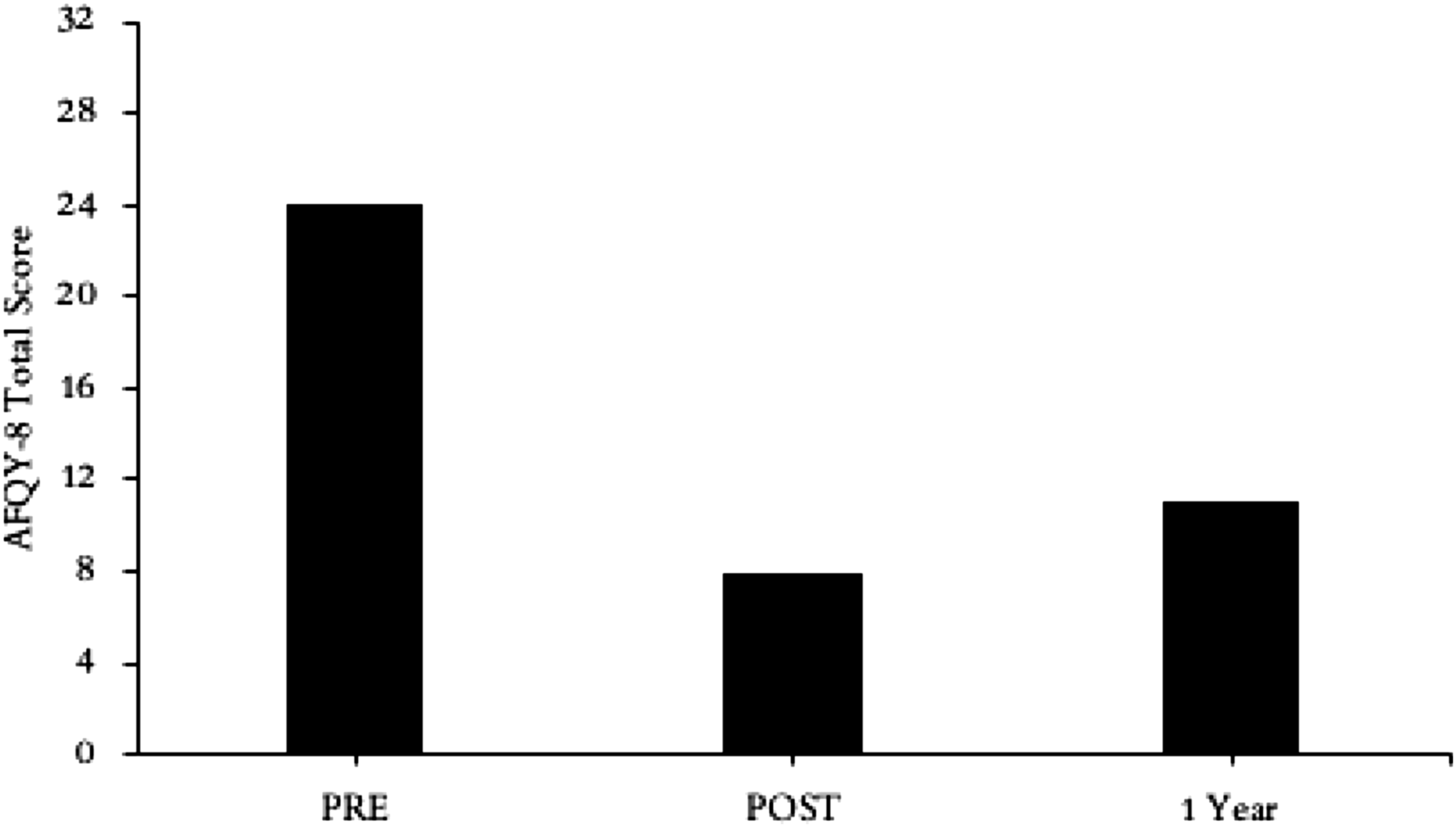
Social Validity Questionnaire Results
Social Validity Ratings for Language, Communication, and Behavior Post Intervention, where “5” is a Neutral Score (i.e., same as baseline).
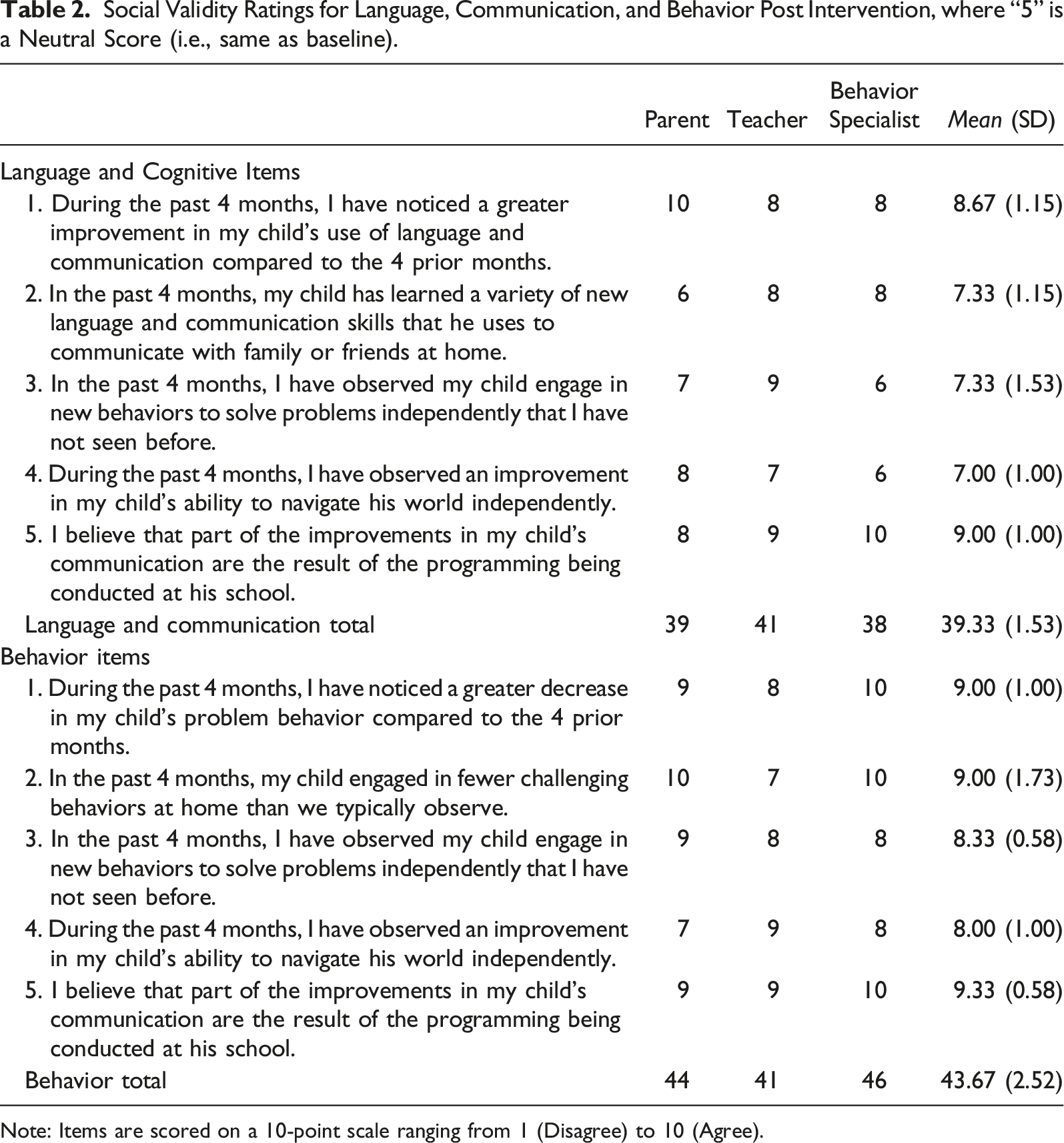
Note: Items are scored on a 10-point scale ranging from 1 (Disagree) to 10 (Agree).
8 Complicating Factors
There were few complications, especially when considering the number of variables and individuals contributing to development, implementation, and assessment of the intervention. One unique aspect of this intervention was that AIM lessons were delivered via telehealth with a young adult diagnosed with ASD, BP, and SZ who presented with escape-related behaviors when faced with non-preferred tasks. Fortunately, James and his school staff had experience with telehealth during the recent year of online educational services due to COVID-19. The same school staff facilitated James’ access to the telehealth experience during the current intervention. This prior experience, coupled with adaptation of the AIM lessons to accommodate James’ preferred interest may have facilitated James’ engagement with this component of the intervention.
One other complicating factor was related to James’ lengthy transportation to the alternative school each day which often resulted in changes to the timing of his twice weekly AIM lessons. Fortunately, implementers were flexible with start and end times and were able to adjust schedules as needed to accommodate most scheduling changes.
9 Access and Barriers to Care
The nationwide shortage of special education teachers and paraprofessionals (Schwartz & Diliberti, 2022) is a current – and long-standing barrier to care for many students from rural school districts (Ludlow et al., 2005). Additionally, parents of students diagnosed with ASD living in rural communities report (a) having limited access to professionals with adequate or specialized training for ASD and (b) a need for services related to social skills, communication, and behavior management skills, in particular (Murphy & Ruble, 2012).
In the current case, the development of James’ services included several specially trained professionals working collaboratively with James’ mother and the school-based alternative program staff. The day-treatment program is located in a rural community that serves pre-K to grade 12 students from eight counties (an area of more than 4500 square miles) who have exhausted all special education services in their resident district. This collaboration between alternative treatment program and university staff and students led to adapted evidence-based intervention that contributed to James’ progress, thereby overcoming this barrier faced by many rural individuals and their families.
James’ mother reported many barriers to effective care prior to James’ current placement in the alternative school-based program. Her efforts to overcome these barriers included being persistent in her pursuit of treatment options, and willingness to consent to additional services and remain actively involved throughout the current intervention. For example, James’ mother requested copies of the AIM curriculum and contingency contract so she could use similar strategies at home. James’ mother (a) implemented contingent privileges when he completed work at school and home without presenting aggressive behaviors, (b) reviewed and discussed with James strategies that he was learning in the AIM lessons, and (c) followed through with repeated practice of strategies such as deep breathing when upset and encouraging choices based on valued outcomes. Her commitment was critical to generalization of intervention strategies across settings and James’ success, overall.
10 Follow-Up
Figures 1 and 2 indicate that aggression and severity of daily incidents continued to decrease during the 6-week follow-up period after AIM sessions were discontinued. In addition, James’ ratings of his psychological inflexibility improved from pre-to post-intervention and remained improved at 1-year follow up when compared to baseline ratings. Responses to the social validity questionnaire suggested that adults in James’ life were more likely to notice behavior changes than language and cognitive changes and link those changes to the intervention.
One-year post-intervention, James’ mother was interviewed to assess his progress with both residential placement and opportunities for trips into the community. During the year prior to the start of the study, James’ mother had applied to one private and one state-run residential treatment program. Despite a review process that spanned several months, James’ was denied placement at both facilities. At 4 months after the intervention, James was admitted to a residential program and has since been admitted and transferred to a second residential program due to his mother’s concerns with care received in the first program. James also progressed in his CC and graduated from once per month community outings with his mother to three to four outings per week, including trips to restaurants, shopping at big box stores, and attending local sporting events (personal communication, October 21, 2022). While community contacts have increased substantially during the past year, James is closely monitored in all settings and remains in a secure residential program as he attempted to elope twice during the first 6-months in the program.
11 Treatment Implications of the Case
While causal status of this intervention cannot be assumed given the multiplicity of James’ services, results from this case study contribute to treatment options for young adults with multiple challenges that severely limit their social, educational, and residential opportunities. This case study illustrates how a combination of empirically supported interventions can be successfully adapted to meet the needs and interests of individuals with co-morbid diagnoses and severe aggressive behaviors. Moreover, third or even fourth-wave therapeutic approaches rooted in cognitive and behavioral models including ACT are increasingly combining idiographic strategies that allow for individuation of intervention based on multiple sources of assessment data at the subject level with nomothetic principles established at the population level (e.g., “psychological flexibility”, Hayes & Hoffman, 2018). In this case, the AIM lessons and contingency contract were developed from the reported functions of James’ aggressive behavior and on-going behavioral and psychological flexibility data were obtained throughout the intervention. In this way, the intervention was designed to strengthen psychological flexibility while establishing environmentally supported, values-based contingencies to both reduce aggressive behavior and to allow for increased access to highly valued community experiences that were achieved during the intervention and follow-up.
12 Recommendations to Clinicians and Students
James is a unique young adult with a challenging history that included medical and mental health services across alternative school programs, in-patient hospitalization, and residential programs. Over time, his challenges resulted in increased severity, frequency, and duration of maladaptive behaviors and consequences that included lost opportunities for education, socialization, and typical childhood and adolescent experiences, among others.
James’ case includes four key recommendations for clinicians and students. First, the current study underscores the benefits of a targeted collaborative effort in particularly challenging cases. Rarely does one clinician, service, or program possess all the knowledge and capabilities that challenging cases require. As a student and clinician, opportunities to collaborate with colleagues and develop relationships with experienced clinicians in areas in which we have limited experience or training, can help improve our performance as clinicians (Rothrauff-Laschober et al., 2013). As a student, select a program of study that provides you with challenging internships. As uncomfortable as these cases may be, challenging internships are positively related to supervisors’ evaluations of students’ career potential (De Pater, Van Vianen, Fischer, & Ginkel, 2008) and can expand opportunities for preferred employment opportunities after completing a graduate program. The graduate student involved with James’ case was willing to undertake the challenges of working with James without having prior experience with online intervention or students with these diagnoses or treatment history.
Second, the AIM manual was critical for aligning assessment outcomes with treatment. As a clinician working with challenging cases, it is beneficial to have a variety of resources – including manuals and knowledgeable colleagues – on which we can rely for treatment strategies and adaptations that enable us to match services and interventions with clients’ needs.
Third, when working in school settings, it is critical to find a match between school staff’s experiences and skills needed to implement interventions with fidelity. The alternative program was fortunate to have an experienced one-on-one staff who previously had worked successfully with James, was committed to implementing AIM strategies throughout the school day and gave James the critical practice with strategies across time and conditions.
Finally, James’ mother’s involvement throughout the treatment process increased James’ exposure to AIM strategies when she adapted strategies for his use at home. Daily contact with James’ mother was instrumental in keeping her aware of intervention and progress and provided support for her efforts to generalize treatment strategies to the home and community settings. As a clinician, helping clients apply strategies in situ can be challenging; finding key individuals to help clients with these efforts is critical to their success over time.
Footnotes
Authors’ Note
Data will be made available upon reasonable request by the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Project was funded by research awards developed by
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.