
Abstract
SAD is an intense fear or anxiety associated with past, current, or future social situations. The Clark and Wells (1995) cognitive model for SAD has been proved to be clinically effective in adults, and its developmentally sensitive adaptations for adolescents have recently shown promising results. Given this evidence and considering that adolescence is typically the age of onset for the first SAD symptoms and a critical developmental period for the delivery of evidence-based interventions, we adapted CT for adolescents for online intervention (CT@TeenSAD) encompassing 10 weekly, 90 min sessions, extended by two booster sessions. This work presents the first case study of that intervention as applied to Merida (M.; pseudonym; 17-year-old, girl). The estimated Reliable Change Index shows M.’s progress for most of her symptoms, from pre-to post-treatment (RCI-1 range: −.53 to −8.03), and the maintenance of benefits at 3 months follow-up (RCI-2 range: .00 to −2.25). A relapse in the adoption of safety behaviors was seen between post-treatment and follow-up, which might be explained by the life-changing challenges experienced by M. between session 10 and follow-up, concerning her transition from high school to college. M.’s case study offers a first glance on the promising results of CT@TeenSAD related to its efficacy and feasibility. Likewise, it offers the opportunity to critically appraise the limitations of the intervention as well as practical challenges and suggestions thought to be useful for therapists willing to implement CT@TeenSAD in the future.
1 Theoretical Background and Basis for Treatment
Social Anxiety Disorder (SAD) is defined as an intense fear or anxiety associated with exposure to social scrutiny in past, current, or future social situations. Social situations might involve interactions (e.g., having a conversation with someone familiar or a stranger), being observed (e.g., while eating or writing), or performing in front of others (e.g., during a presentation). Socially anxious individuals experience social situations with intense anxiety due to concerns about being humiliated or embarrassed. Typical concerns are about displaying anxiety symptoms (e.g., blushing or sweating) or of seeming inappropriate (e.g., boring or incompetent). Ultimately, anxiety symptoms and what is perceived to be inappropriate behaviors are thought to potentially lead to rejection by others or are feared to unintentionally offend others (American Psychiatric Association, 2013). In Europe, SAD has a 2.4% lifetime prevalence (Alonso et al., 2004) and only a 40% natural remission rate (Beesdo-Baum et al., 2012).
Women and people of younger ages are the most affected groups, with 75% of SAD diagnoses being established between the ages of 8 and 15 (American Psychiatric Association, 2013). The common age for establishing the diagnosis may be related to the mismatch between social demands, newly acquired cognitive skills, and the lingering neurodevelopmental milestones associated with the social and emotional brain. That is, neural networks that are involved in self-regulation and cognitive flexibility only reach their maximum between the ages of 21 and 30 (Dajani & Uddin, 2015). Consequently, adolescents need to face social and self-imposed demands with still-developing skills.
Adolescents diagnosed with SAD often experience compromised daily routines and academic achievement (Van Ameringen et al., 2003) and lower mood and higher perceived loneliness, and approximately half present other anxiety and mood disorders (e.g., Ranta et al., 2009). Therefore, adolescence is a critical period for the onset of SAD symptoms and, simultaneously, an opportunity for delivering theoretically sound and evidence-based interventions, thus optimizing mental health resources available over the lifespan.
The Clark and Wells (1995) model for social anxiety disorder in adolescents
The Clark and Wells model (1995) offers a strong theoretical background for understanding SAD. The model was originally developed for adults to address the lack of specificity of extant, psychological, broad-reaching interventions aimed at SAD core maintenance factors. According to Clark and Wells (1995), social situations are seen as potentially threatening, thus triggering physiological, cognitive, and behavioral anxiety responses that persist due to several maintenance factors. These include prevalent negative cognitions (about the self and social situations) that involve: (1) excessive high standards concerning self-performance (“I must be fluent all the time”); (2) conditional beliefs about the consequences of one’s own inadequate performance (“If I stutter, people will think I am a fool”); and (3) unconditional beliefs about the Self (e.g., “I’m boring”). Another key maintenance factor is the spontaneous processing of the Self as a social object, which is then used to infer how others perceive one’s behavior (e.g., “When I shake, others think I look stupid”), mistaking the felt sense of anxiety with looking anxious. The appraisal of anxiety symptoms as signs of social failure leads to negative perceptions and negative interpretations of ambiguous social cues and an enhanced attention towards negative social cues (Leigh & Clark, 2018a).
Anticipatory worry (pervasive negative thoughts) about future social events and ruminative thinking (the self-focused process of revisiting an individual’s social experiences post-mortem) also contribute to the development and maintenance of social anxiety (Clark, 2001). Safety behaviors are another maintenance factor discussed by Clark and Wells’ model and convey the set of behaviors intended to prevent or minimize the feared outcomes (e.g., avoiding eye contact) and to ensure that a good impression is conveyed (e.g., planning what to say next), offering temporary relief (Leigh & Clark, 2018a).
SAD maintenance factors, as described by Clark and Wells’ (1995) model for adults, have been found in adolescence as well. For example, excessively high standards for one’s own social performance were found to predict social anxiety in adolescents (Rudy et al., 2014). Prevalent negative social cognitions and attitudes were found to mediate the association between self-focused attention, negative self-image, pre- and post-event processing, and the adoption of safety behaviors in adolescents (e.g., Schreiber et al., 2012). Attentional bias to negative social cues and self-focused attention seem to contribute to anticipatory worry and ruminative thinking in adolescents (Haller et al., 2017; Pergamin-Hight et al., 2016). Safety behaviors seem to be more frequent in SAD and in more socially anxious adolescents than in less socially anxious adolescents and subclinical groups (Ranta et al., 2014).
The efficacy of cognitive therapy for SAD (CT-SAD) has been recognized in adult populations (Mayo-Wilson et al., 2014) and adolescents (CT-SAD-A; Ingul et al., 2014). Due to its beneficial profile, minimal side effects, and cost-effectiveness, CT-SAD is recommended as the first-line treatment for adults diagnosed with SAD by the National Institute for Health and Care Excellence of the UK (https://www.nice.org.uk/guidance/cg159, 2013), and its promising results for adolescents suggest it may be soon recommended for early ages as well.
The online CT@TeenSAD intervention
The first publication reporting CT-SAD delivered via the internet used written messages and telephone calls (the iCT-SAD), showing promising results for 11 adult patients diagnosed with social anxiety (Stott et al., 2013). The robustness of evidence in favor of the efficacy of the CT-SAD (both in-person and online) and CT-SAD-A motivated the development of the CT@TeenSAD intervention within the broader project TeenSAD: Changing the Course of Social Anxiety in Adolescence (ClinicalTrials.gov Identifier: NCT04979676). In the first stage, we translated CT-SAD-A to the Portuguese population and adapted it to 10 sessions of 90 min (instead of the 14 sessions originally suggested; Leigh & Clark, 2016), so that it would conform to the remaining comparator interventions. Because CT@TeenSAD was intended to be delivered online, it incorporates Warnock-Parkes et al. (2020) suggestions for CT-SAD-A remote intervention.
To our knowledge, beyond the published Leigh and Clark (2019) protocol for a randomized clinical trial using an online version of the CT-SAD-A, no efficacy data has been reported whatsoever. Consequently, the current case report offers the first description of the applicability of CT-SAD-A as an online therapy for adolescents.
In CT@TeenSAD, the weekly sessions are organized across four modules, extended by two booster sessions to occur monthly after the core program has ended. The first three modules address the five essential components of CT (i.e., individualized cognitive model of social anxiety; unhelpful effects of negative thoughts, self-focused attention, and safety behaviors; attention training; anticipatory worry and post-event processing, and behavioral experiments). The last module reviews gains and addresses relapse prevention. The two booster sessions aim to recall achievements, prompt the application of learned skills, expand the generalization of results, and address relapse prevention (see Table 1). Between sessions, the therapist sends three weekly reminders via Whatsapp—one to summarize the content of the previous session, another about the challenges the adolescent is prompted to accomplish during the week, and a third as a reminder of the session scheduled for the next day.
Structure of the CT@TeenSAD Intervention.
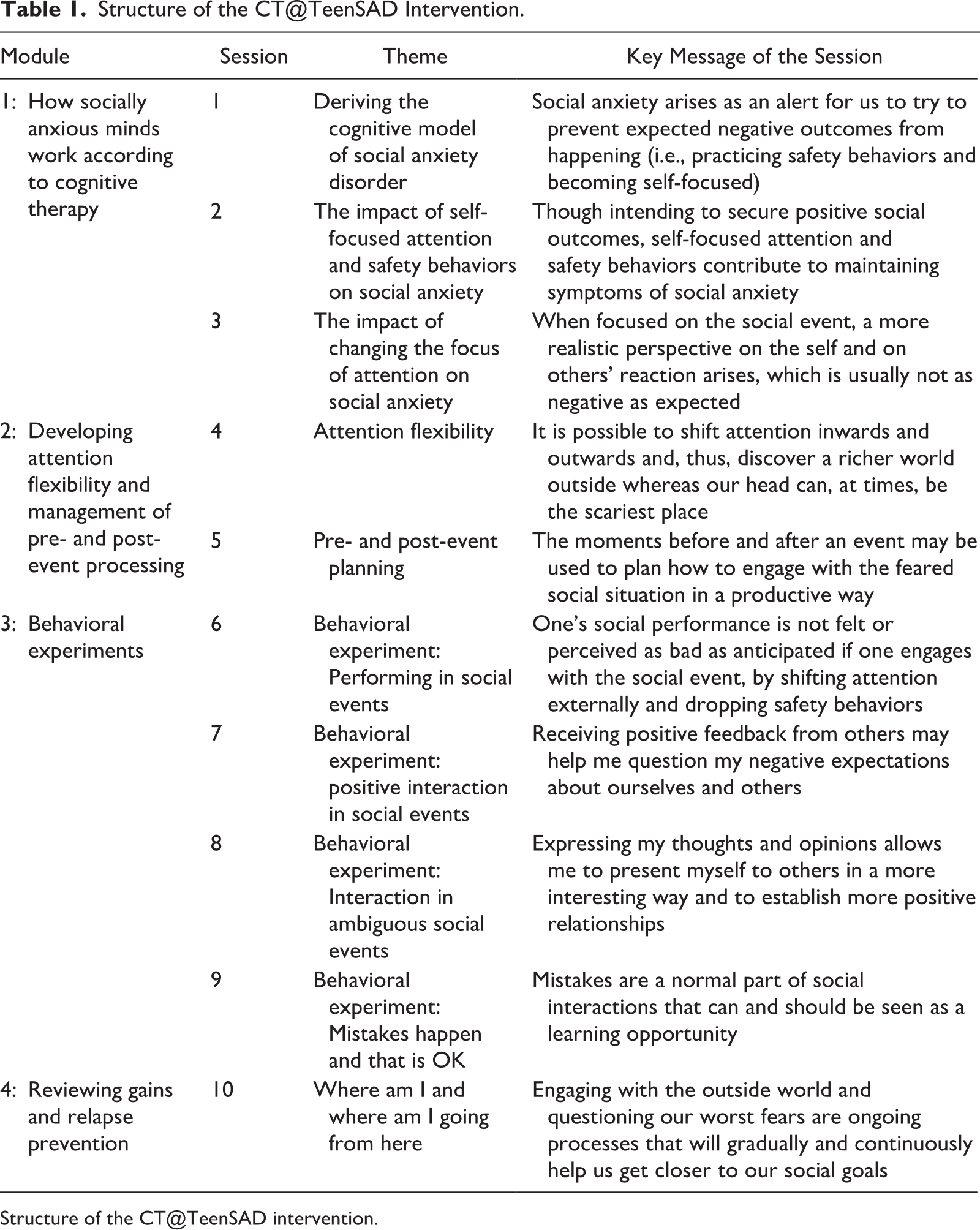
Structure of the CT@TeenSAD intervention.
The structure of Sessions 2 to 10 is similar, starting with the welcoming message, followed by a short overview of the insights brought by the previous session and an interactive discussion of the adolescent’s experiences during the week’s challenges. The second part of the sessions includes one or more exercises around the central topic and a new week challenge. To close, a synthesis of the sessions’ core aspects is explored with the adolescent. The goals for each session are detailed in Table 1.
The therapist and the patient were required to secure their privacy during sessions. The setup for the therapist and M. included a laptop or desktop computer connected to a 13-inch screen (minimum), with a built-in or external web camera, a headset (preferable), and a stable internet connection. A Pro version of Zoom (Zoom Video Communications, Inc., 2020 [Computer software]) was used to guarantee interruption-free sessions and secure internal record savings.
2 Case Introduction
Merida (M.; pseudonym) is a 17-year-old girl that participated in the program after her mother provided informed written consent and M. provided oral consent; confidentiality and anonymity of all data collected were guaranteed. At the recruitment stage, M. completed the assessment protocol, scoring 82 on the Social Anxiety Scale for Adolescents (SAS-A) (La Greca & Lopez, 1998), which was above the one standard deviation of the mean for the Portuguese population (Cunha et al., 2008). She was further diagnosed with a primary diagnosis of Social Anxiety Disorder using a diagnostic interview (see Assessment section). Other measures collected at pre-and post-treatment are further discussed in the Assessment section and depicted in Table 2.
Merida’s Scores From Baseline to Post-Treatment and Clinical Improvement.
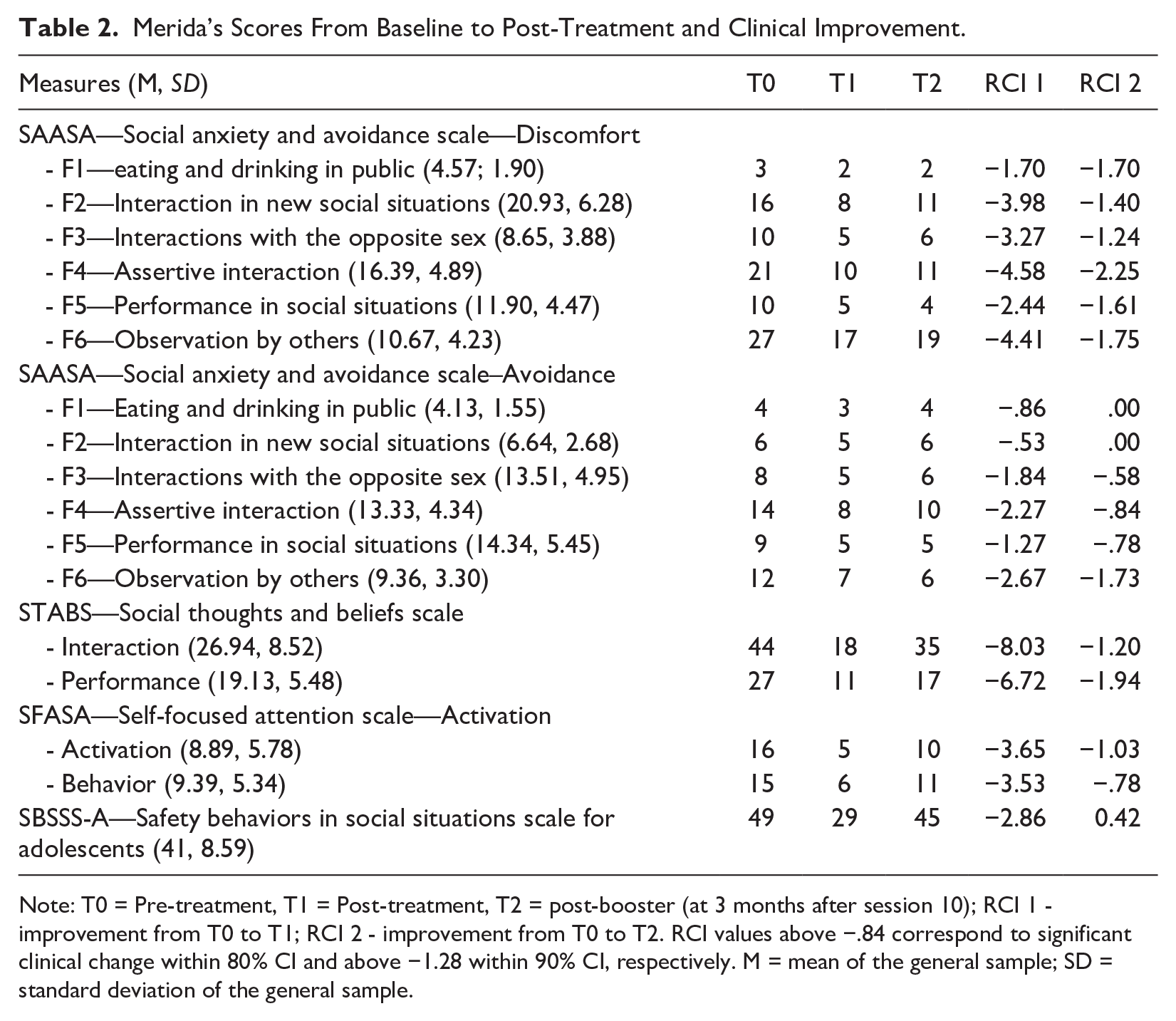
Note: T0 = Pre-treatment, T1 = Post-treatment, T2 = post-booster (at 3 months after session 10); RCI 1 - improvement from T0 to T1; RCI 2 - improvement from T0 to T2. RCI values above −.84 correspond to significant clinical change within 80% CI and above −1.28 within 90% CI, respectively. M = mean of the general sample; SD = standard deviation of the general sample.
3 Presenting Complaints
M. presented a four-year history of SAD. During interviews, she describes an intense fear of a range of social situations where embarrassment or humiliation may occur, as when going to social gatherings, calling others’ attention to herself (e.g., by asking for help in class or making a mistake), and when potentially exposing her body (e.g., using the dressing room). In social interactions, M.’s thoughts concerned the high probability of being unable to get her words out and of blushing. M.’s main fears were that “people will look at me and judge my weight,” “I will have nothing interesting to say to strangers,” “I will look less intelligent than others,” and “I will stutter.” In social interactions, she had an image of herself as physically unattractive, unintelligent, and too shy and uninteresting to be approached. When performing in public (e.g., a presentation in class), these thoughts would repeat, along with her self-image of someone unable to hide her nervousness, twirling her hair, and blushing, leading people to think she is foolish or unacceptable. To cope with her fear, M. would frequently not speak out and would prefer to keep her thoughts to herself working to make herself invisible, even with her closest friends. M.’s anticipatory worries were about whether she would have anything to say and about what others would think about her. She would also go over social situations post-mortem, presenting ruminative thoughts about others’ judgements of her behaviors (e.g., forgetting to buy a birthday present for a close friend), leading her to dwell on guilt, shame, and embarrassment, and to fear social rejection.
4 History
M.'s personal history was collected from the pre-treatment assessment MINI-KID (Sheehan et al., 2010; Portuguese Authorized Version by Rijo et al., 2016) and from a second interview conducted after treatment by the psychologist that delivered the intervention.
M.’s mother pregnancy progressed as expected. M. was born to term, no complications were reported, and developmental milestones were achieved as anticipated. In her childhood, M. was diagnosed with asthma and, since a young age, she was overweight. Until the age of three, she stayed with her grandparents while her parents were at work.
M.’s father was an alcoholic, impulsive, and violent man. Although, as a child, M. describes a lovable relationship with her father, she has several memories of his violent behavior, particularly at home, towards her mother. When M. was four, her parents got divorced after a violent episode during which M.’s father threatened his wife at the dinner table with a knife and M. stood by her mother. M. recalls this episode as the foundation of her shame and disappointment towards her father’s violent behavior, which was at the antithesis of her young idealized paternal figure. Following this episode and for the next 2 days, M. lost her voice and avoided socializing with neighbors, physically distancing herself both from adults and other children. M.’s father left home, and M. continued living with her mother and older sister.
Her mother was diagnosed with major depression around this period, with extreme weight loss and severe impairment of her daily routine for several months. Although today she is a functional woman, she is still medicated. M.’s sister was diagnosed with hyperthyroidism at the age of 17 (when M. was eight), which developed into acute thyroid storm episodes from time to time, with associated dizziness, shortness of breath, fast/irregular heartbeat, and loss of consciousness. M. was frequently her sister’s first aid during these episodes.
Between the age of three and five, M. went to kindergarten. She started elementary school 1 year earlier than expected (at five) because, according to her teacher, she was well developed and the tallest child in her kindergarten class. During her elementary school years, M. attended the same school where her mother worked as support staff and she was an above-average student, although shy. Despite always having had a small group of close friends, the fear of others making fun of her and worries about not being lovable and about her appearance were frequently present, limiting the quality of her relationships.
Between the ages of 11 and 13, M. moved to a different school and an acute change occurred in her behavior, negatively reflecting in her academic achievement. She suffered bullying due to her physical appearance and sexual orientation (she defines herself as bisexual), and in response, she started to be aggressive and sometimes violent towards other children. At home, she was dismissive of her mother and her sister. M. started missing classes and earning low grades, which ultimately led her to fail the sixth grade. By the age of 13, she remembers experiencing intense confusion regarding her sexual orientation and frequently feeling trapped, as she was constantly being compared to her older sister at school.
At the age of 14, M. and her mother moved to M.’s stepfather’s village, and her sister (already 22 years old) went to live with her partner and two children of their own. Moving to a new home in a new village led to a new school that M. attended for her final 5 years of public education.
At this school, M. has felt free from her troublesome past, as no one knew her or her family. She started hanging out with the “good” students’ and regained her focus on school tasks and activities. Although currently M. feels at ease at this school with her closest friends, she still worries about disappointing or contradicting them, which she believes might lead them to not loving her anymore. Also, M. feels trapped by worries about the anxiety symptoms she is not able to hinder (e.g., stuttering when speaking in public) and what others might think of her intelligence during a conversation or when performing or completing a new task in front of others. Her lack of confidence about her appearance and worries about others making fun of her body are pervasive and she tries to hide in large clothes and avoids large gatherings.
At the age of 16, M.s’ asthma developed into a cardiac arrest during the night. Recently, she developed additional health issues that, by the time of the interview, were still under study for differential diagnosis for inflammatory bowel disease, after two in-patient hospitalizations (of about 1 month each) in the past 2 years.
At the start of the intervention, M. was living with her mother and her stepfather. She was academically driven, attending the school theatre group, and an active member of the church youth group. M. was also starting to prepare for college preparatory exams in the Arts by the end of the school year.
5 Assessment
Establishing the Primary Diagnosis With the Mini International Neuropsychiatric Interview for Children and Adolescents
The baseline assessment was conducted by a psychologist that used the MINI-KID (Sheehan et al., 2010; Portuguese Authorized Version by Rijo et al., 2016) 3 weeks before the start of the program. The MINI-KID is a short, structured diagnostic interview that assesses a broad range of Axis I diagnoses in children and adolescents as described in the DSM-V (American Psychiatric Association, 2013) and the ICD-10 (World Health Organization, 2004). The MINI-KID offers a summary profile to support the clinician’s decision regarding the primary diagnosis, considering the symptoms identified and rendering to its level of impairment and time of onset. According to the original authors, the interrater reliability (IR) was excellent across diagnoses, except for dysthymia (Sheehan et al., 2010).
During the interview, M. was slow to speak, talking in a low voice and making eye contact only from time to time. Even displaying a shy stance, M. built rapport easily with the interviewer and was able to disclosure herself, and her difficulties, openly and clearly. M. was diagnosed with a primary diagnosis of Social Anxiety Disorder and an additional diagnosis of Attention Deficit and Hyperactive Disorder, predominantly inattentive.
Characterization of M.’s Social Anxiety
At pre-treatment, M. completed the Social Anxiety and Avoidance Scale for Adolescents (SAASA; Vagos et al., 2014 adapted from Cunha et al., 2008), a dimensional and a-theoretical self-report measure of social anxiety assessing the intensity of discomfort and the frequency of avoidant behaviors across six factors: F1—Eating and drinking in public; F2—Interaction in new social situations; F3—Interaction with the opposite sex; F4—Assertive interaction; F5—Performance in social situations; F6—Observation by others. Comparing M.’s scores at baseline for the anxiety subscale factors and the mean values for girls in a Portuguese sample of adolescents diagnosed with SAD (Cunha et al., 2008) we can tell that M.’s score of 10 in F3 indicates her discomfort when interacting with the opposite sex (potentially associated with her sexual orientation), her score of 21 in F4 indicates her discomfort during assertive interactions (e.g., related to her fear of rejection if she disagrees with others), and her score of 27 in F6 indicates her extreme discomfort when being observed by others (e.g., doing physical exercise, using the dressing room at school, and going to parties). Surprisingly, M.’s score of 10 for F5 is within the average, which contrasts with M.’s reported fears of performing in formal situations during the interview. Similarly surprising was M.’s score at baseline on the avoidance subscale. When compared with girls in the general Portuguese sample, we can tell that M. is above average just for F6, where she scored 12, indicating that her avoidance is limited to social events where she perceives she will be observed.
To understand M.’s negative thoughts and beliefs, we used the Portuguese version of the Social Thoughts and Beliefs Scale (STABS; Turner et al., 2003) by Vagos et al. (2010) that assesses the degree to which a particular thought or belief related to social interactions and public performance is present. Considering the mean values for the total score for girls in the Portuguese population, M.’s baseline scores of 44 and 27 on discomfort in social interactions and discomfort in public performance, respectively, suggest the presence of intense discomfort and pervasive negative thoughts across distinctive social situations. At the item level. M.’s thoughts about her appearance, self-worth, and fears of being judge by others during interactions and beliefs about her performance are predominant.
We assessed M.’s self-focused attention using the Portuguese version of the Self-focused Attention Scale for Adolescents (SFASA; Bögels et al., 1996) adapted by Fontinho and Salvador (2012). The SFASA measures the focus on one’s behavior (SFA-behavior) and the focus on one’s physiological arousal (SFA-arousal) in social situations. Considering the mean values for Portuguese girls for SFA-behavior and SFA-arousal, M.’s baseline scores of 16 and 15, respectively, suggest that her self-focused attention is increased compared to average girls of her age. M.’s scores were particularly high in monitoring processes of her social behavior when in interaction (i.e., checking her speech fluency and her understanding about what others are saying, confirming whether her behavior is adequate, etc.).
To assess M.’s use of safety behaviors, we administered the Safety Behaviors in Social Situations Scale for Adolescents (SBSSS-A; Silva et al., 2010). M.’s baseline score of 49 is clearly above the mean, showing her extreme adoption of safety behaviors. As expected, when safety behaviors are intensively adopted, avoidance is less needed, which might explain M.’s within-the-average scores in all measures of SAASA Avoidance. That is, M.’s adoption of avoidance behaviors across most social situations is within the average because her use of safety behaviors when interacting is quite extensive, offering the needed temporary relief to bear social interactions. M.’s assessment scores per instrument at baseline (T0) can be found in Table 2.
6 Case Conceptualization
M. presents all the typical components of social anxiety, according to Clark and Wells (1995) (i.e., negative cognitions, psychophysiological arousal, self-focused attention, negative self-image, and safety behaviors), which makes her case particularly suitable for cognitive therapy aimed at addressing the uniqueness of SAD. When facing social situations, M. usually activates negatively biased cognitive assumptions about her cognitive abilities (e.g., “I am not as good as others”), her social skills (e.g., “I will have nothing to say”), and her appearance (e.g., “I am not attractive”). These may result from M.’s early traumatic experiences (e.g., exposure to domestic verbal and physical violence) and potential social shame about her family. Additionally, negative experiences with her peers (e.g., bullying) and teachers (e.g., being compared to her older sister in her behavior and grades) might have contributed to her negative cognitions about her self-worth as a teenager.
Based on these assumptions and concurrent negative assumptions activated when facing social events, social situations are perceived as threatening and encompassing social danger, namely because M. fears negative social outcomes such as making a fool of herself, feeling embarrassed, or being judge by others. These fears are then materialized into a vivid self-image (e.g., “I don’t look attractive”), eliciting intense psychophysiological arousal (e.g., blushing, accelerated heart rate). As a way of preventing her fears from becoming true and her symptoms from being noticed, M. keeps her attention focused on how she is coming across (i.e., her negative self-image) and on checking if the impression she is conveying is enough to keep her fears from coming true (e.g., monitoring her movements and speech or appearance). Such assessment is negatively biased by her self-perception as flawed.
To prevent herself from experiencing her worst fears, whenever possible, M. avoids interactions (e.g., conversations with the opposite sex, assertive interactions, such as asking a favor, or situations where she might be observed by others, such as oral presentations and parties). When avoidance is not possible (e.g., in class), M. adopts her safety behaviors (e.g., looking down, wearing unappealing clothes, speaking faster than she should when presenting in class or keeping herself aside from others, entertained with her mobile phone when at parties, circumventing meeting new people). Although these behaviors prevent her from being evaluated or rejected, they also keep her from updating her negative assumptions, frequently leading to unwanted results (e.g., a sense of a muddled speech and stuttering) that, according to her, have been negatively impacting her school grades. A vicious cycle then unfolds.
Above and beyond M.’s anxiety during social events, she presents pervasive anticipatory worries that interfere with her sleep and encompass her fears of not knowing what to say or how to behave, particularly in formal social situations. She would also go over social situations repeatedly post-mortem, presenting ruminative thoughts about how others would have judged her attitudes or behaviors, leading her to dwell on feelings of guilt, shame, and embarrassment, and to fear social rejection. Figure 1 depicts M.’s personalized model of social anxiety.
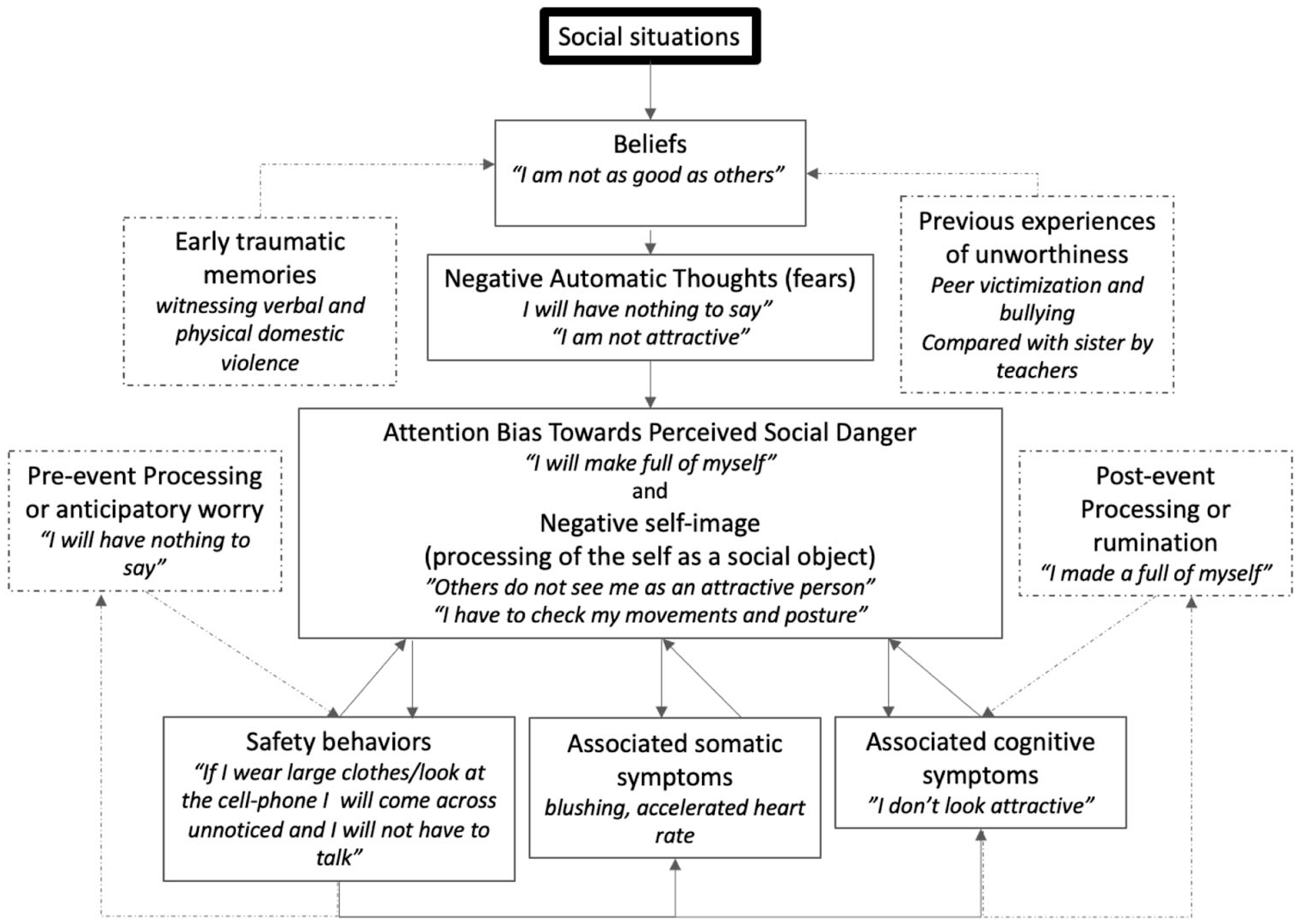
M.’s personalized model of social anxiety according to Clark and Wells’ (1995) model.
The CT-SAD-A approach offers a model that provides adolescents with new tools to work through each element of their Social Anxiety personalized model and the links between these elements. These tools are thought to help interrupt the chain of internal events (psychophysiological and cognitive) SAD adolescents experience and prevent the adoption of safety behaviors each time they face a current or forthcoming social event. In the case of M., intense attentional training in and outside sessions, and learning to identify her personal signs of somatic or cognitive symptoms of anxiety, will help her notice when attention is self-focused and shift attentional resources outwards to detect important cues of the social context. Also, according to the model, learning by experience (using role-play and video feedback) is expected to decrease self-focus and bring awareness about the negative impact of adopting safety behaviors. In addition, CT-SAD-A approach works with adolescents to connect with more realistic images of the Self through video feedback and discussion of learnings about the Self and others based on information gathered from behavioral experiences implemented in and outside sessions, thus weakening the previously prevalent negative self-image and the processing of the Self as a social object. Overall, by deconstructing the cycle of Social Anxiety, symptoms are relieved, and the core beliefs and automatic thoughts about the Self are restructured or reappraised.
7 Course of Treatment and Assessment of Progress
M.’s therapist in the CT@TeenSAD program was a psychologist with 20 years of clinical experience and training in Cognitive Behavioral Therapies. The first seven sessions with M. occurred during a confinement period (late December 2020 to early April 2021). The last three sessions occurred when M. had already returned to school. The 10 core sessions progressed smoothly for 12 weeks, and the two booster sessions happened four and 8 weeks after the 10th session, respectively.
Module 1 (Sessions 1–3)
M. was always very pleasing and collaborative, easily picking up the psychoeducational content about the nature and treatment of SAD. M. developed her personalized model of social anxiety derived from a recent experience of social discomfort during a presentation she gave in a philosophy class; from this exercise, M. was able to apply it to other situations occurring outside therapy. During this module, M. was also confronted with the beneficial effects of keeping her attention externally focused (e.g., feeling less anxious and letting go of self-monitoring) and the negative impact of practicing safety behaviors (e.g., avoiding eye contact while interacting with others). M. confirmed that, contrary to her predictions, when she lets go of her safety behaviors and focuses her attention externally, she represents herself more confidently. That is, she feels her negative self-image is not so pervasive, she feels amused during the interaction, and her nervousness seems to be less noticeable than she predicted. Ultimately, M. was able to update her self-image to a more realistic one.
Module 2 (Sessions 4 and 5)
Within this module, M. learned to sustain the focus of her attention externally and to increase the flexibility of her attentional shifting through systematic training using guided visual and auditory non-social stimuli, as suggested by Warnock-Parkers et al. (2020). Visual stimuli included an in-house video of landscapes, objects, and plants and close ups of colors, textures, reflections, and shadows [2.24 min]. The auditory stimulus was the music “When I’m 64” from The Beatles, remastered (2009) [2.38 min]. The social stimuli included one in-house video depicting outside city scenes with people walking from the perspective of a bystander observer [3.04 min]. Additionally, the therapist read a passage of a text to the patient depicting an interaction situation [3–3.20 min]. In-session learnings were further practiced between sessions both when M. was by herself and when with others. To better use her new attentional skills, M. was taught to identify her anxiety cues-bodily states or thoughts that signal when an anxiety cycle is starting and when attention should be deployed to the outside world. With home practice on deploying her attention externally, M. was able to successfully modify her previous negative cognitions brought on by her self-focused attention, in relation to her performance (e.g., “I am not as good as others”), and her appearance (e.g., “I am not attractive”). By shifting the focus of attention externally and dropping safety behaviors, M. was able to progressively modify those dysfunctional thoughts.
By being able to identify the starting point of her anxiety response, shifting the focus of her attention to the outside world, letting go of her safety behaviors (e.g., looking away), and using alternative behaviors (e.g., look up and around), M. realistically understood the extent to which her sense of being observed was exaggerated. Also, M. presented more realistic thinking about others judgmentally starring at her and was surprised by the comfort that adopting alternative behaviors brought to her. It was important that such learnings were achieved early in the program, as these supported M.’s learnings in the forthcoming behavioral experiments.
Anticipatory worries and ruminative thinking were two cognitive processes present in M’s thinking, with the latest being predominant. Therefore, the second goal of Module two was to offer M. the adequate tools to manage the spiraling post-event processing that could detrimentally override the beneficial effect of the behavioral experiments. The main topic of M.’s ruminations were her fear of saying foolish things and embarrassing herself in front of others. When trapped in these ruminations, M. would have a negative image of herself stuttering while speaking and blushing in front of the big group. Together with her therapist, M. developed her personalized “Memory Card” with the synthesis of the advantages and disadvantages of ruminative thinking, supplemented by an alternative plan to implement when she found herself stepping into rumination, which included her favorite externally focused attention exercises, the planning for a behavioral experiment around her ruminative thoughts and (then) other distracting activities of her preference.
Module 3 (Sessions 6 to 9)
Across this module, M. realized that her predictions rarely happen as expected and that her anxiety symptoms are not as visible to others as she thought. Also, M. experienced the benefits of trying alternative behaviors when participating in positive emotional interactions and when approaching others and interrupting a conversation to take part of it. M. additionally experienced the advantages of exposing herself more, disagreeing with friends, and the consequences of making mistakes. As a result, she revised her beliefs about herself (e.g., “I can build on good arguments”) and the school setting (“All students are at school to learn and teachers are pleased to help, which decreases the risks of embarrassment”) and was able to let go of some of her fears of rejection. Of core importance, M. experienced firsthand the effect of triggering others' interest when expressing her own opinions. These findings were extended between sessions by the autonomous planning and implementation of new experiences.
Closing-Session 10
The goal here was to promote engagement with the outside world and manage M.’s worst fears related to past and future social events. M. and her therapist assessed the treatment trajectory and M. realized she had achieved her individual goals almost to 100%. Additionally, M. shared that she found the attentional focus training the most useful tool to break free of the safety behaviors and to realize the actual image she conveys to others. On the contrary, her self-focused attention towards her fear of stuttering when performing in public was still hampering her full success in situations that involved her speaking in public.
By Session 10, M. started working part-time while completing high school and preparing herself for college in the forthcoming year. Therefore, M.’s anxiety was increasing in response to the current challenges. She and her therapist discussed to what extent the tools previously learned would be sufficient for M. to autonomously navigate the social contexts that would follow. M. shared her fears about the future, but was, at the same time, optimistic about her achievements, confident about her skills, and committed to continuous practice.
Maintenance-Booster Sessions 11 and 12
The first booster session aims at establishing the planning of social experiences as part of the adolescent’s routine. For that, M. and her therapist discussed one successful and one not-so-successful social experience from the previous weeks. Together, they reviewed M.’s individual model regarding the two events to find the contrasting components and elected M.’s focus of attention to her negative thoughts as the key factor that triggered her anxiety response. They reviewed the strategies to prompt attentional shifting by revisiting M.’s “Memory Card” and reviewed the step-by-step on how to plan successful behavioral experiments, boosting previous learnings and increasing the odds of success in the future. Of note, M. shared her increased confidence in her appearance, which recently led her to go shopping to buy new clothes that best fit her body shape and made her look more feminine.
The second booster session aimed at reviewing M.’s experience across the program and set the stage for her future managing her social fears autonomously. M. and her therapist reviewed M.’s path, went through M.’s successes and difficulties in the past weeks, recalled M.’s achievements, and defined her future goals. To prepare possible setbacks, a list of strategies for M. to implement when facing new challenges and social discomfort was built.
8 Complicating Factors
M. started her participation in the intervention during a confinement period. Therefore, Sessions 1 to 7 were conducted while the school was closed and classes were attended online, significantly reducing the number of opportunities for regular social interactions with peers in the school setting. Additionally, M. lives in a suburban area and the confinement reduced the number of people outside. These two factors highly limited the richness of social interactions at school and other settings (e.g., the supermarket, the park, and at the bus stop). However, M.’s case study also has shown that despite the limited richness regarding social experiences, the progress across the program was achieved as expected, suggesting that restricted but systematic and well-consolidated behavioral experiences are more important than an intensive set of experiences.
Another complicating factor concerned the final three sessions. By then, M. started working part-time, which added to her busy school schedule; her fatigue was evident during these sessions. Also, these last sessions were conducted a couple of weeks before M.’s annual exams and while she was preparing her application for and making decisions about college, which is always a stressful process for teens. The pressure to make this life-changing decision potentially consumed most of M.’s daily preoccupations, distracting her from the content of the program and the weekly challenges proposed within the intervention. Also, M.'s social fears associated with her future (moving away from her family, meeting new people in college, having roommates, etc.) were brought up by M. and lightly addressed as new factors of stress; however, it was not possible to fully address these new worries within the program; though during the program, these factors did not interfere much with the content of the sessions, it seems they might have had a clinical impact, according to M.’s worse scores being reported in the follow-up (T2) compared with post-intervention (T1; see Section 10).
9 Access and Barriers to Care
During the 10 sessions and the two boosters, M. presented all the conditions needed to access treatment (e.g., easy access to a reliable internet connection, high-quality connection, headset, webcam, and privacy).
10 Follow-up
Post-treatment assessment (T1) was conducted right after Session 10 and the follow-up assessment (T2) was done 12 weeks after, both using the measures described in Section 4. To calculate M.’s improvement from T0 to T1 (i.e., RCI1) and from T0 to T2 (i.e., RCI2) across social anxiety components, we used the Reliable Change Index (RCI; Jacobson & Truax, 1991) applied to each measure. We estimated the RCIs ratio with the difference between scores in two distinctive moments (in our case, pre- and post-intervention) in the numerator and the standard error of the difference score (in our case √2(SD0*√1–α)2 in the denominator, where SD0 was the standard deviation of the non-clinical population and α was the internal consistency index of the instrument. The RCI provides a measure of change in standardized units, informing whether the arithmetical change across treatment exists and, thus, the null hypothesis of no change must be rejected. Positive RCIs correspond to rejection of the null hypothesis with potential clinical deterioration, whereas negative RCIs correspond to rejection of the null hypothesis with potential clinical improvement. The threshold to reject the null hypothesis for a p < .05 lies at the z-score ≤ −1.96. Therefore, RCI z-scores lower than −0.84 indicate significant change, with a confidence interval (CI) of 80%, and z-scores lower than −1.28 indicate a significant change with a CI of 90% (Wise, 2004). RCIs per measure and time point are depicted in Table 2.
In the SAASA discomfort subscale (Vagos et al., 2014), M.’s scores improved across all factors from T0 to T1 and from T0 to T2 at least within the 80% CI, regardless of its scores being normative or above the population’s average at T0. Particularly important was M.’s improvement regarding her discomfort in a myriad of social situations such as when being observed, in assertive interactions, when in new social situations, and when interacting with the opposite sex. As for the avoidance subscale, despite scores for Factors 1 through 5 being within the mean at T0, improvement or maintenance was overall found from T0 to T1, but showed no clinically relevant change from T0 to T2. Also, avoidance when being observed (the single clinically relevant factor in T0) reliably improved from T0 to T1 and this gain was still significant at 3 months follow-up.
According to STABS (Vagos & Pereira, 2010) scores, M.’s clinical change in social cognitions, both in interactions or when performing in public, considerably improved from T0 to T1, and gains were maintained (although with a decrease) at 3 months follow-up. Additionally, M.’s self-focused attention as assessed by SFASA (Fontinho & Salvador, 2012), improved between T0 and T1. However, at follow-up, clinical improvement was decreased. Improvement was still significant in what concerns self-focused attention towards signals of arousal (potentially associated with the normative experiences leading to college), but was lost in what concerns self-focused attention towards monitoring her behavior. As discussed in Sections 6 and 7, M. was faced with new life-changing challenges between Session 10 and the assessment at 3 months follow-up. Moreover, these challenges might have distracted M. not only from the awareness of having new social skills to face social situations, but also from practicing those skills. This may well explain the worsening of symptoms that are seen between T1 and T2, specifically those referring to safety behaviors.
11 Treatment Implications of the Case
This case study aims to illustrate the structure and challenges of CT@TeenSAD, an intervention based on the original CT-SAD-A (Leigh & Clark, 2016) and designed to be delivered individually and online. Although the focus of this article is not methodological, there is a set of challenges related to online therapy delivery that need to be addressed. The online application of CT-SAD-A, and particularly the individual change process it encompasses, had not been reported before, which should sustain important clinical implications, not only concerning CT for SAD, but also relating to its application using a briefer version (i.e., 10 sessions) and an online format.
This case study demonstrates the efficacy of CT@TeenSAD in an adolescent of 17–18 years of age, in what concerns the quantitative assessment of SAD core maintenance factors, and the qualitative impact observed across the program by the therapist and as expressed by the adolescent. Particularly, changes in social thoughts and social beliefs were observed along with clinical improvement in what concerns discomfort in social situations, even for those processes that lay at normative degrees at the beginning of treatment. The apparent relapse at follow-up was found in more contextual sensitive factors (e.g., safety behaviors) and less in thoughts and beliefs. Because the program aims to sequentially build upon each module’s learnings to support the adolescent in overcoming social events with increased comfort and relying on Clark and Wells’s (1995) model on the primacy of negative thoughts and beliefs, one may infer that, as far as the improvement in these factors is sustained, clinical improvement might be conserved to a certain extent.
M. ended her participation in the program right before the transition period that encompasses finishing high school and moving to college. M.’s increased anxiety in this stage of her life is aligned with the literature that characterizes the transition from high school to college as a developmental period of increased vulnerability to stress-related mental health issues (e.g., Diehl et al., 2018). The critical external challenges related to the life-changes that encompass this stage of uncertainty may have led to the apparent loss of clinical gains at follow-up concerning self-focused attention and practice of safety behaviors in particular. In the future, the development of an adjusted CT@TeenSAD program to the specificities of this period may increase adolescents’ resilience and promote healthier trajectories across the stressful experience of losing close parental support and leaving school peers behind to navigate new social environments. Whether CT@TeenSAD was effective regarding long-lasting changes in more phenomenological cognitive components such as negative thoughts, beliefs, and improved self-image that survived school to college transition can only be confirmed by a new follow-up assessment that might be conducted after M. steads in her new life context. Alternatively, a qualitative approach to M.’s experience throughout the program could bring to surface her experiential and transformative material (similarly to what was previous done by McManus et al. (2010)).
The COVID-19 pandemic requested services and providers to adapt to innovative ways to deliver health services remotely through videoconferencing. Remote mental health provision further brings advantages, being particularly interesting in the current and future pandemic situations, as it decreases the risk of contamination while increasing accessibility to services. For instance, it decreases time and cost for those living outside urban areas, overcomes the stigma associated with mental health appointments, and reduces anxiety for those with social anxiety symptoms for whom meeting in-person and navigating new social environments might be more challenging. Indeed, some of these obstacles were exceeded in M.’s case study, who otherwise would not have had the opportunity to participate in the program if it was delivered in-person and at a clinic or university setting.
The establishment of the therapeutic relationship online is a key factor of success that must be addressed from the beginning. For two decades now the literature has shown that online sessions can guarantee the desirable high quality of the therapeutic alliance, while simultaneously ensuring successful outcomes, at least similarly to what is found in face-to-face contexts (Backhaus et al., 2012; Sucala et al., 2012). However, legitimate concerns about this modality, arguing on the grounds of a putative decreased quality of the therapeutic relationship have hindered its benefits. M.’s case offers the opportunity to confirm not only the efficacy of the CT@TeenSAD program but also the acceptability of videoconferencing as a powerful context for a meaningful therapeutic change, embedded in a wealthy therapeutic alliance. Amidst the COVID-19 pandemic, M.’s proficiency in using technologies and her familiarity with online conferencing context (eventually due to her previous experience with friends and more recently with online synchronous classes), offered the enabling context to overcome one’s natural resistance to online therapy.
Limitations
This case study faces the typical limitations of manualized interventions built to address general difficulties across adolescence. Between 15 and 18 years, adolescents require distinctive social and cognitive abilities to adequately address developmental life challenges and properly fit their individual needs. Although the effect of CT@TeenSAD is evident, the relapse of contextual-dependent symptoms seen in M. suggests that it might be most beneficial to adolescents between 15 and 17 years, before they face major normative transitions. On the other hand, for late adolescents, individualized adaptations could include one or two sessions dedicated to major expected life transitions.
Also, CT@TeenSAD did not include memory work (to address traumatic memories), nor work with parental attitudes and behaviors (e.g., overcontrol), school setting factors (e.g., quality of the relationship with peers, bullying and victimization) or the use of social media. These factors were either previously integrated into CT-SAD-A programs (Leigh & Clark, 2016) or suggested to be considered as needed. The work with parents, the school setting and the use of social media seems to be particularly interesting at younger ages to improve implicit self-esteem which might transform these contexts into leverages rather than obstacles to the therapeutic change (Leigh & Clark, 2018a, 2018b). Although with M. the opportunity to work with previous memories of bullying in the school setting or memories of abandonment by her father could have supported core changes in her low implicit self-esteem, current parental attitudes, and relationships with peers at school were predominantly positive and modules addressing these were not deemed necessary. Overall, the take-home message is that individualized adjustments to the program according to the adolescent experience and idiosyncrasies might be beneficial.
Another reason that might be argued to be associated with the symptom resurface in M. at follow-up is the reduced number of sessions. However, the randomized clinical trial by Ingul et al. (2014) showed the efficacy of a shorter version in adolescents, with 12 sessions of 50 min (which is far less than our CT@TeenSAD of 10 90-min sessions, plus two booster sessions).
12 Recommendations to Clinicians and Students
CT@TeenSAD was built to be delivered through videoconferencing, so all technical tools to ensure the appropriate delivery of sessions are required (e.g., high-quality internet connection and an adequate headset). The videoconferencing system and connections should be secure, and patients should be instructed on how to achieve user proficiency. Although in some cases it is not possible, adolescents should preferably attend sessions through their computer so that a wide screen for displaying materials is available. Because video feedback uses in-session video recordings, a wide screen is recommended so that the adolescent has a higher quality image to analyze. Additionally, the in-built recording function is an essential feature, allowing the therapist to select parts of the session that need be analyzed during video feedback tasks. To overcome the typically increased self-consciousness of adolescents (and even more so for those with SAD) while video conferencing, the system should allow the capability for the user to hide or turn off self-view. Alternatively, the adolescent should be instructed to cover his/her image (e.g., using a post-it).
Although video feedback is a core feature of this program, it has a few limitations when the content is delivered online. It may not be possible to properly record important avoidance behaviors (e.g., hiding hands) or anxiety-related physiological responses (e.g., trembling, blushing), meaning that special attention should be paid to those anxiety manifestations that can be effectively worked out during the provision of video feedback (e.g., avoiding eye contact, minimal verbal expressions). To address some of these limitations, behavioral experiments, including social interactions in virtual reality (VR) environments, could be added to the program (see Caponnetto et al., 2021 for a systematic review). However, while in VR, avoidance behaviors, such as hiding hands and avoiding eye contact (using eye-tracking methods) can be recorded, anxiety-related physiological responses might be lost. General requirements and further details about the best practices and guidelines to conduct videoconferencing therapeutic sessions can be found in Warnock-Parkes et al. (2020).
Videoconferencing-based interventions have been described in the last two decades to manage distinctive disorders (e.g., Ojserkis et al., 2014; Fleming et al., 2017). However, these interventions seem to be particularly suited for adolescents as natural digital users. Further, the program seems to fit adolescents’ communication needs and therapists’ perceptions that the communication and the establishment of the therapeutic alliance with adolescents is easier and faster using online tools (Himle et al., 2012). To build a strong therapeutic alliance when conducting CT@TeenSAD online, we suggest considering a few communication enhancement strategies. For a good emotional tuning, the therapist should take care that both him/her and the adolescent secure good eye contact. Also, despite the static script of a manualized intervention, the therapist should not refrain from regularly checking in and intentionally use his/her body posture, facial expressions, and voice tone to better tune with the adolescent. The therapist should feel comfortable to regularly enquire about meanings associated with the adolescent’s facial expressions and body posture. This sometimes mean that whatever the adolescent brings to session will be prioritized. Finally, the therapist should should take maximum advantage of prosody, velocity of speech, rephrasing, summarizing, and iterative strategies to increase the session’s dynamic. For further reading about communication enhancement strategies for online therapy, we suggest Simpson et al. (2020).
Testing the efficacy of developmentally sensitive therapeutic interventions specifically targeting SAD symptoms in adolescence is of the utmost importance to reduce the probability of chronicity and to mitigate the broad-reaching negative impact that SAD brings to adolescence and adulthood. CT@TeenSAD is well-aligned with the global future of digital mental health delivery services, and M.’s case study and its preliminary findings set the stage for the efficacy of the CT@TeenSAD approach to be further consolidated, namely by investigating larger samples, long-term follow-up assessments, and comparisons with face-to-face interventions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fundação para a Ciência e a Tecnologia (PTDC/PSI-ESP/29445/2017). The Center for Research in Neuropsychology and Cognitive and Behavioral Intervention (CINEICC) of the Faculty of Psychology and Educational Sciences of the University of Coimbra is supported by the Portuguese Foundation for Science and Technology and the Portuguese Ministry of Education and Science through national funds and co-financed by FEDER through COMPETE2020 under the PT2020 Partnership Agreement [UID/PSI/01662/2013].
Data Availability
The data that support the findings of this study are available from the corresponding author (AGA) upon reasonable request.