
Abstract
Current research suggests that ketamine-assisted psychotherapy has benefit for the treatment of mental disorders. We report on the results of ketamine-assisted intensive outpatient psychotherapeutic treatment of a client with treatment-resistant, posttraumatic stress disorder (PTSD) as a result of experiences of racism and childhood sexual abuse. The client’s presenting symptoms included hypervigilance, social avoidance, feelings of hopelessness, and intense recollections. These symptoms impacted all areas of daily functioning. Psychoeducation was provided on how untreated intergenerational trauma, compounded by additional traumatic experiences, potentiated the client’s experience of PTSD and subsequent maladaptive coping mechanisms. Ketamine was administered four times over a 13-day span as an off-label, adjunct to psychotherapy. Therapeutic interventions and orientations utilized were mindfulness-based cognitive therapy (MBCT) and functional analytic psychotherapy (FAP). New skills were obtained in helping the client respond effectively to negative self-talk, catastrophic thinking, and feelings of helplessness. Treatment led to a significant reduction in symptoms after completion of the program, with gains maintained 4 months post-treatment. This case study demonstrates the effective use of ketamine as an adjunct to psychotherapy in treatment-resistant PTSD.
Keywords
1. Theoretical and Research Basis for Treatment
Introduction to Psychedelic-Assisted Therapies
Over the last decade there has been a growing interest in psychedelic-assisted psychotherapy for the treatment of a variety of mental health conditions such as anxiety, depression, substance abuse, OCD, and posttraumatic stress disorder (PTSD; Luoma et al., 2020). Psychedelic-assisted psychotherapy refers to pairing psychedelic substances with psychotherapeutic interventions to maximize therapeutic outcomes. Research indicates that psychedelics and substances that induce non-ordinary states of consciousness can provide a significant reduction in symptoms, so much so that the U.S. Federal Drug Administration (FDA) has granted some medications Breakthrough Therapy designation (e.g., Thomas et al., 2016). This means that the substances have shown preliminary clinical evidence demonstrating that the drug may have an advantage over the currently available therapies (Federal Drug Administration [FDA], 2018).
Emphasis of Ketamine
A single infusion of ketamine has been found to alleviate depressive symptoms in treatment-resistant depressed patients within hours and these effects may be sustained for up to 2 weeks (Berman et al., 2000; Diazgranados et al., 2010). Ketamine is one of the few medications recently granted Breakthrough Therapy designation as an off-label treatment for depression (Popova et al., 2019). In 2019, a double-blind, active-controlled, multicenter study for ketamine-assisted psychotherapy was conducted at 39 outpatient referral centers. The results showed significant improvements in depression symptoms among those in the esketamine group compared to the placebo group 4 weeks into the study (Popova et al., 2019). Another study conducted by Calabrese (2019) comprised 231 adults and adolescents with treatment resistant depression where most participants to partook in individual psychotherapy while also receiving as many as six ketamine infusions over a 2 to 3-week period. This study demonstrated a 79% decrease of suicidal ideation in participants who previously experienced multiple suicide attempts, psychiatric hospitalizations, and where 80% of the sample failed at least four different antidepressant trials. Ketamine has been shown to increase the structural plasticity in human brains (Collo & Pich, 2018). Therefore, psychotherapeutic interventions may be optimized when used in conjunction with this critical period.
Selective serotonin reuptake inhibitors (SSRIs) are considered a first-line pharmacological treatment for PTSD, however response rates rarely exceed 60%, and less than 20% to 30% of patients achieve full remission (Berger et al., 2009). New research suggests that ketamine also has benefit for the treatment of PTSD (Feder et al., 2014, 2021), although, there are fewer studies that examine ketamine-assisted psychotherapy (KAP) for this condition (Liriano et al., 2019). PTSD is a chronic and debilitating condition arising after exposure to a severe traumatic event, characterized by persistent reexperiencing, avoidance, and hyperarousal symptoms. Ketamine, known as a dissociative anesthetic, is classified as an arylcyclohexylamine (Kolp et al., 2014). Arylcyclohexylamines, predominantly target the neurotransmitter glutamate, which is an excitatory messenger thought to be involved in pathophysiology of PTSD and depression (Nair & Singh, 2008). It predominantly blocks the N-methyl-D-aspartate (NMDA) receptor, a target for the neurotransmitter glutamate in the brain, and prevents the NMDA receptor from being activated by glutamate. When given at a dose that produces a non-ordinary (altered) state of consciousness, ketamine promotes relief from negativity, an openness to new perspectives, and increased access to the whole self (Dore et al., 2019). This improves a client’s ability to engage in more meaningful psychotherapy during and after administration, making it a potent tool for recovery from both depression and traumatization.
Recently, Dore et al. (2019) examined the outcomes of KAP at three different outpatient clinics; where most clients were being treated for major depressive disorder (MDD) and PTSD, and those with complex PTSD showed the greatest improvements.
Racial Trauma
Racial discrimination can have deleterious effects on the mental health of African Americans (Chae et al., 2011). Williams et al. (2018b) describe racial trauma as “a traumatic response to race-related experiences that are collectively characterized as racism, including acts of prejudice, discrimination, or violence against a subordinate racial group based on attitudes of superiority held by the dominant group. Racial trauma can be caused by overt or covert actions carried out by individuals or society.” PTSD is a distinct mental health diagnosis that requires exposure to a traumatic incident as part of its diagnostic criteria (American Psychiatric Association [APA], 2013). Acts that can cause or contribute to racial trauma include racial slurs and threats made in a variety of environments (work or social), police harassment, body searches, or assaults, and community violence. Racial and ethnic groups appear to differ in other ways that might be associated with PTSD risk as well. For example, Roberts et al. (2011) found that people of color are at greater risk for trauma related to maltreatment during childhood particularly in relation to immigration, witnessing war, and witnessing domestic violence.
Subtle forms of racism such as microaggressions are also linked to trauma (Williams et al., 2018c). Microaggressions include a wide range of verbal and nonverbal communications, intentional and unintentional, that portray insensitivity, disrespect, and/or negligent attention to another person due to their marginalized heritage or identity. Due to the many ways in which people of color may be exposed to traumatic events that do not always neatly fall under the “Criterion A” DSM-5 PTSD qualifier, this has led to arguments about the legitimacy of racism and oppressive acts as worthy of a PTSD diagnosis (Holmes et al., 2016). Supporting evidence from the quantifiable impacts of microaggressions, to discriminatory racial climates and social inequalities, has demonstrated the negative implications that racism has on mental health leading to symptoms of trauma (Williams et al., 2018c).
Basis for Treatment
There is evidence supporting the efficacy of psychedelic-assisted psychotherapy for the treatment of PTSD (e.g., Dore et al., 2019; Mithoefer et al., 2019), however a literature review conducted by Michaels et al. (2018) found that 82% of participants in these studies were non-Hispanic White. It should be noted that there is a mistrust with communities of color participating in medical/scientific studies due to historical atrocities, for example an experiment in Lexington, Kentucky where incarcerated Black men were dosed with LSD for 77 days in a row (Rosenberg et al., 1963). Additionally, Black communities are disproportionately arrested and incarcerated for non-violent drug offenses which could further lead to apprehension toward therapeutically consuming substances deemed illicit. Nonetheless, there is some preliminary evidence that psychedelics can reduce symptoms of racial trauma, based on survey data in naturalistic settings (Williams et al., 2020a). Because Robyn had tried behaviorally-based interventions before with only limited or temporary success, adding a psychedelic to help potentiate treatment seemed like an important next step. In terms of choice of psychedelic, although there is more research evidence supporting MDMA for PTSD, as of this writing, ketamine is the only legal option for psychedelic-assisted psychotherapy in the US outside of a research study.
Third wave CBT approaches may be well-suited for psychedelic psychotherapy, particularly for people of color (Miller et al., 2015; Sloshower et al., 2020; Walsh & Thiessen, 2018). Functional Analytic Psychotherapy (FAP) is a therapeutic approach rooted in the contextual behavioral tradition that focuses on the therapeutic relationship as the agent of change to improve the client’s relationships (Tsai et al., 2009). FAP promotes intrapersonal awareness as well as interpersonal awareness between the client and therapist, encouraging a strong and authentic connection. This approach prompts FAP therapists to take interpersonal risks by experiencing, processing, and disclosing reactions to the client as they occur in-session in the service of client growth, and therapists encourage their clients to do the same. When the client engages in courageous self-expression in FAP sessions, the therapist in turn responds with genuine feedback to increase the intimacy of the exchange. This vulnerability and immediacy serves as a model to help the client improve connections with others, which is an important transdiagnostic outcome (Wetterneck & Hart, 2012).
Mindfulness is described as “the awareness that emerges through paying attention on purpose, in the present moment, and non-judgmentally to the unfolding of experience moment by moment” (Kabat-Zinn, 2003, p. 145). Mindfulness therefore promotes mental wellbeing by changing the relationship individuals have with their thoughts, increasing the ability to observe thoughts and emotions in an accepting way. Mindfulness-Based Cognitive Therapy (MBCT) is a modality where focus is placed on becoming more aware of thoughts and feelings with an emphasis on changing the relationship a client has with their thoughts rather than changing or challenging the content of the thoughts (Segal et al., 2002). MBCT has been used successfully as an adjunct therapy for PTSD arising from childhood sexual assault in women of color (Frye & Spates, 2012). Although both FAP and MBCT have been used for the treatment of PTSD as individual modalities and with psychedelic-assisted psychotherapy (Kohlenberg et al., 2006; Thompson et al., 2011), they have not yet been examined for their utility in treating racial trauma.
2. Case Introduction
Robyn (pseudonym) is a 58-year-old African American woman who was self-referred after going on disability following experiences of race-based discrimination in the workplace. Robyn had complex PTSD and spent many years in traditional talk therapy attempting to resolve her past traumas without much relief. At the time she reached out to the clinic, Robyn was attending a high-profile PTSD program and, unfortunately, experienced microaggressions from White providers there (Williams & Halstead, 2019). Robyn was in search of relief from her symptoms and wanted to process and treat the race-based trauma so she could return to work. At the time, Robyn’s symptoms included hypervigilance, intense recollections, and anxiety. She also had a secondary diagnosis of Persistent Depressive Disorder and had ongoing suicidality. Robyn expressed feelings of hopelessness around her mental health challenges and was ready to explore the option of ketamine-assisted psychotherapy.
3. Presenting Complaints
When beginning treatment Robyn was isolative and struggled to make trips to the grocery store, fearing she might experience further acts of discrimination. For example, Robyn reported being worried about microaggressions that she would likely face during public interactions and how this might further exacerbate her PTSD symptoms. Although she was able to carry out various activities of daily living, she struggled with severe anticipatory anxiety that would sometimes linger for hours at a time. Robyn also felt that she did not have any close platonic friendships, and explained that it was difficult to trust anyone because she assumed that they would either not believe her experiences, or not understand the extent of what she experienced. Robyn was in a romantic relationship, which was dissatisfying due to a lack of support and compassion from her partner, which manifested as invalidations and minimizations of her lived experiences. Robyn explained that it was better to have someone to confide in than no one at all. She therefore felt that it was necessary for her to suffer through the relationship rather than to break it off.
4. History
Robyn had a challenging upbringing filled with extreme abuse and neglect. She would sometimes go without food, experience sexual and physical abuse from multiple family members, and be the target of severe racial discrimination at school. Robyn disclosed that she was often called various racial epithets, spit on, and assaulted. She reported that despite her sharing this information with her parents and teachers, no one ever intervened until an instance in 3rd grade where another child pushed her into a wall knocking her front teeth out.
It wasn’t until much later in life that Robyn pursued treatment, and she was officially diagnosed with PTSD in 2003. She reports trying a variety of treatment modalities including various SSRIs, counseling, Eye Movement Desensitization Reprocessing (EMDR), Cognitive Behavioral Therapy (CBT), and Dialectical Behavior Therapy (DBT). She found the combination of DBT and anti-anxiety medications (Buspirone and Lorazepam) helped her the most with stress tolerance, but she was still suffering greatly. In 2017 Robyn also underwent an intensive outpatient program (IOP) for PTSD, which she felt, provided relief from her aversive childhood experiences. Despite receiving successful treatment for the various aversive childhood events, her PTSD symptoms returned when she was re-traumatized at work where she was repeatedly discriminated against once more. Since the IOP in 2017, Robyn had continued ongoing treatment with a local therapist.
5. Assessment
Robyn was assessed based on her prior history, clinical interview, and clinician administered and self-report measures, which included the following:
Mini International Neuropsychiatric Interview (MINI; Sheehan et al., 1998): A structured clinical interview used to assess the most common psychiatric disorders.
UConn Racial/Ethnic Stress and Trauma Survey (UnRESTS; Williams et al., 2018a): A structured clinical interview used to identify racial trauma in individuals to develop a qualitative understanding of their experiences for case conceptualization and culturally informed care.
Beck Depression Inventory-II (BDI-II; Beck et al., 1996): A popular 21-item self-report measure of depressive symptoms occurring over the last 2 weeks. Items are rated from 0 to 4, with higher numbers indicating greater symptom severity.
Posttraumatic Cognitions Inventory (PTCI; Foa et al., 1999): A self-report questionnaire that is designed to assess negative cognitions about self, negative cognitions about the world, and self-blame. Items are rated from 1 to 7, with higher numbers indicating greater symptom severity.
Cultural Genogram (Hardy & Laszloffy, 1995): An information-gathering tool that serves as a pictorial display of a person’s family and medical history within the context of a person’s culture and race and/or ethnicities (discussed further in first Preparatory Session section).
Robyn’s symptoms presented as a pervasive sense of hopelessness, insomnia, agitation, and loss of enjoyment in almost all areas of her life. On the MINI, Robyn met criteria for both PTSD and MDD. On the UnRESTS, her experiences of racism met criteria for PTSD. She scored a 40 on the BDI-II, which placed her in the “Severe Depression” range, and her score of 207 on the PTCI was over a standard deviation higher than the median score for those with PTSD diagnosis. Robyn reported experiencing these symptoms for the last 3 years.
6. Case Conceptualization
Robyn’s symptoms were conceptualized through a culturally-informed model of how cumulative traumatic incidences acquired over time can lead to PTSD (Williams et al., 2018b). Since social determinants of health have a direct impact on treatment outcomes, therapists also considered Robyn’s unique social background (e.g., race, gender, age, geography, education, upbringing) to inform the treatment plan. Both childhood sexual abuse and racial traumas were presumed to create assumptions in Robyn’s views about herself and the world. This early negative self-concept later led to feelings of worthlessness, inadequacy, and hopelessness which was then further exacerbated from the subsequent work-related discrimination she endured. Due to living in a rural, predominantly White area, Robyn recalls experiencing acts of discrimination during the majority of her social outings. Robyn often feared going into public spaces because she was uncertain whether or not she would endure more discrimination either overtly (racially profiled, followed in stores) or covertly (lack of eye contact, being overlooked). Additionally, as a Black woman, she had been socialized in a manner that emphasized the importance of caregiving, self-denial, and enduring adversities against all costs, which can contribute to exhaustion, anger, and feeling less control over her own life (González-Prendes & Thomas, 2009).
Therapists took an eclectic approach to treatment, guided by several empirically supported therapeutic orientations. Therapists primary treatment modalities consisted of FAP and MBCT to address the many experiences that Robyn reported. FAP provided an excellent basis for which therapists could model emotional intimacy and connection and deepen the therapeutic alliance throughout treatment. MBCT was chosen to help Robyn re-conceptualize her challenges and distress surrounding her experiences of racism. It was very easy for Robyn to often focus on the worst-case scenarios, so MBCT would allow Robyn to be present with the moment unfolding before her so she could begin to apply appropriate cognitive techniques or coping strategies instead of responding in maladaptive patterns that no longer served her. Because Robyn endured countless instances of discrimination it was important that the therapeutic modalities used did not minimize nor misinterpret her experiences but validated and provided compassion.
7. Course of Treatment and Assessment of Progress
Robyn worked with a diverse therapist team which is believed to also aid in the outcomes of treatment for this particular case. Clinician S.R. is a Black woman, who is a Licensed Marriage and Family Therapist, and M.H. is a multiracial (Creole and Native American) woman who is a Licensed Practicing Counseling Associate. The prescribing clinician R.K. was a White man with a Doctor’s of Nursing Practice and Board Certified Advanced Nurse Practitioner. M.H.’s supervisor and the clinic director (M.T.W.) was an African American female Clinical Psychologist. All therapists had extensive training in working with diverse populations and had training in psychedelic-assisted therapies.
Treatment took place over a 13-day span where Robyn met with her two therapists and the prescribing clinician. Robyn completed a series of both drug and non-drug treatment sessions throughout her IOP. Sessions included preparation, dosing, and integration sessions over the 13-day period. This structure allowed for a balance between preparatory, dosing, and integration sessions respectively. 150 mg of ketamine was administered sublingually on 4 days of the IOP treatment (75–300 mg is typical KAP range). For sublingual administration, the bioavailability can vary, estimated at 15% to 49%, (Chong et al., 2006). After each dosing session, therapists completed a risk assessment to further ensure the safety of the client after being in vulnerable states and engaging in potentially difficult material. During integration sessions therapeutic interventions included cognitive restructuring, MBCT and various FAP techniques. Most preparatory and integration sessions also consisted of a guided mindfulness exercise lasting from 5 to 15 mins on average. In terms of frequency of treatment, Robyn met with therapists individually or jointly for two, 90-min therapy sessions on integration and preparatory days. Typically, this was structured as one 90-min session in the morning, and one 90-min session in the evening. Therapists and Robyn did not meet on Sundays. The spacing of integration sessions to dosing sessions was partially modeled after the protocol developed by the Multidisciplinary Association of Psychedelics (MAPS) study of 3,4- methylenedioxymethamphetamine (MDMA) assisted psychotherapy for the treatment of PTSD (e.g., Mithoefer et al., 2019).
Pre-Treatment Sessions
Robyn completed a series of assessments (as noted previously) to help determine initial eligibility for treatment. During administration of the MINI, Robyn reported high suicidality stating she thinks about suicide roughly four times a week but reported no current plan or intent. Robyn reportedly had a safety plan in place with her local therapist who was also aware of her suicidal ideation. Due to the client’s complex history of trauma, therapists understood that building rapport with her would be essential to the overall success of the treatment. As such, each therapist spent time understanding the client’s symptoms through her own lens.
Psychiatric and Medical Evaluation
Upon completing the initial eligibility for ketamine therapy treatment, Robyn was then evaluated by the prescribing clinician. After confirming that ketamine therapy was appropriately indicated, and that she did not have any health diagnoses that would disqualify her for this treatment, Robyn was cleared to begin the KAP-IOP.
Preparatory Sessions
Therapists began Robyn’s treatment by going through the informed consent form in detail, highlighting current ketamine therapy research, the subjective effects of ketamine, expectations of dosing sessions, and the ongoing process of consent to treatment. A deliberate, detailed informed consent process is critical in building trust with people from vulnerable groups (e.g., Black women) due to the historical harms inflicted upon those groups in medical practice and psychedelic assisted research (Rosenberg et al., 1963; Washington, 2007; Williams & Labate, 2020). Once Robyn consented to treatment, therapists gathered information about her symptoms and functioning. Robyn reported feeling hyper-vigilant about being in social spaces where she could encounter incidents of racism, and apprehension about eventually returning to work. Overall, Robyn described a desire to learn new skills to deal with the discrimination she experienced in the workplace. She also expressed dissatisfaction with her current romantic partner who would often dismiss her fears and generally not provide emotional support in her pursuits to better herself throughout various domains of her life. Robyn expressed wanting to work toward developing meaningful friendships with other people of color, given that she was living in a predominately White suburb. Although Robyn expressed some anxiety about the dosing sessions, she was overall optimistic and motivated to begin treatment.
Because Robyn experienced multiple traumas throughout her life, starting in her early childhood, it was important to understand how these still impacted her beliefs about herself, the world, and her current relationships. Ethnocultural genograms have been used successfully to understand clients in culturally-informed manner (Díaz-Martínez, 2003). In Robyn’s case, clinicians were able to use this tool to identify various internalized messages from childhood such as “your abuse doesn’t matter,” “Black people are worthless,” and “I am stupid.” These beliefs organized the way Robyn responded to the world around her. Therapists were also able to explore the intergenerational trauma passed down through her family. Robyn described how she not only grew up taking on her parents’ hyper-vigilant and emotionally-unavailable dispositions, but that this was a trend also witnessed in her grandparents. She also recalled her father having nightmares or not sleeping at all. With these disclosures and the historical context of racism enacted on African Americans, the therapists understood this to be indicative of intergenerational trauma, or the cumulative effects of historical atrocities that increase the risk for PTSD in subsequent generations (Goosby & Heidbrink, 2013). Themes included distorted views about ethnic identity, dysfunctional interpersonal relationships, and internalized feelings of anger, fear, and shame. Examples of questions used to gather this information included:
What did your family teach you about Blackness?
Was lighter skin privileged in your family? What messages did you receive about your skin tone and hair texture?
Did your siblings discuss experiences growing up in segregated schools versus your experience in integrated schools?
After obtaining relevant clinical information and developing goals that Robyn hoped to achieve during treatment, therapists spent time providing psychoeducation on various grounding and self-regulation techniques such as diaphragmatic breathing, somatic interventions (rocking, tapping, humming; Menakem, 2017), and using mantras/affirmations such as “I am safe” as supportive techniques that she could use during potentially difficult moments during the dosing sessions (Brom et al., 2017). To further set the tone of each medication session, therapists suggested that Robyn develop an “intention” that she could use to further remind her of why she sought ketamine treatment, what she hoped to achieve, and to help her stay with difficult material that might arise. Techniques were provided to support Robyn in staying with and deepen her experience, rather than push difficult emotional processes away as she reportedly had in the past. During this time Robyn was also instructed to complete a daily ABCD log (Figure 1) to address and challenge core beliefs. The ABCD log was created by Ellis (1991), as a CBT based intervention to address cognitive distortions. Therapist S.R. adapted the log to help address Robyn’s constant rumination, address her common cognitive distortions via negative self-talk and maladaptive coping mechanisms, and help Robyn develop action-oriented steps to reinforce these new cognitions.
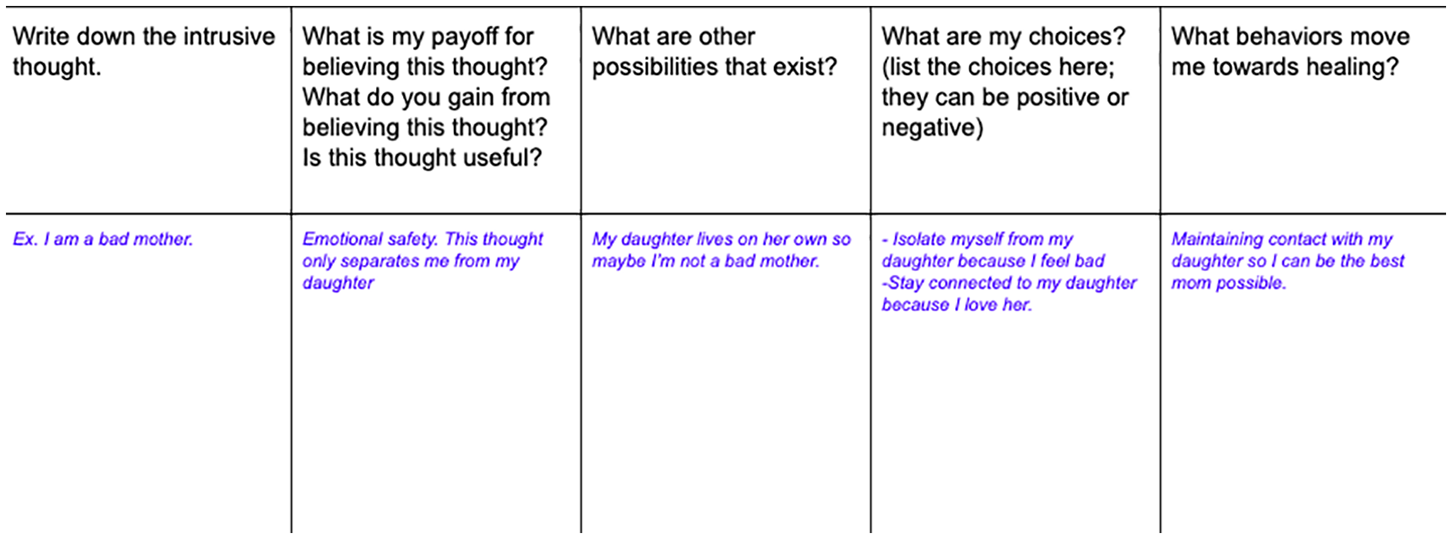
Client’s ABCD log.
First Dosing Session
Therapists arrived at the prescriber’s office approximately 30 mins prior to the session start time to help set the space and check in about the dosing session. The setting included a warm office environment, live plants, candles, a mat with pillows, and floor seating for the therapists. Upon arrival, Robyn was greeted and welcomed. Prior to administering the medication, R.K. checked her blood pressure and made sure she adhered to certain lifestyle modifications prior to the dosing session (e.g., not taking certain anti-anxiety medications as benzodiazepines can suppress the mental health benefits of ketamine; Albott et al., 2017). Robyn reported that her intention, or goal, for this session was to determine what needed to be healed for her to process and move past her various traumatic experiences. With the intention held in her awareness, the medicine was offered, and Robyn courageously took the lozenges, holding it in her mouth for 10 mins before swallowing.
During the onset medication effects, Robyn reported “feeling the most relaxed she had ever been in her life.” Coupled with the relaxation, however, was a desire to work, to jump into processing and heal some of her deepest wounds. As a Black woman with such a complex trauma history, and not often having the space to relax, therapists understood this client’s reflex contextually, and invited her to stay with the relaxed feeling as long as she could as an important part of healing. Robyn stayed with the feeling and it led her to deep somatic processing of past traumas and wounds from her relationships with her mother, father, daughter, and eldest brother. Robyn encountered various somatic pains (stomach, hips, pelvic area) and was able to successfully utilize breathing techniques to move through them. Robyn also described various disappointments that she had with herself and others close to her.
Robyn realized that self-critique was one way she learned to distract herself from experiencing pain. She discussed many self-critiques and internalized messages she received from her external world like “never being smart enough or good enough.” Experiences of racialized trauma also came up for processing when she recounted a childhood experience where another student called her the n-word (Saleem et al., 2020). She also described fears she had of disclosing the harms that happened to her for fear of how it would reflect on her, because in many of her childhood relationships, her testimonies about traumatizing events were dismissed or minimized. It was a new experience to feel witnessed and validated by her therapists as she re-processed these childhood wounds.
Robyn also shared that her partner called her the night before and made dismissive comments about treatment and culture. She explained that this led to an argument and a decision for her to proceed with treatment with minimal contact with him so that she would not be distracted. This was a significant boundary that Robyn willingly set in order to prioritize her needs during treatment. Therapists provided positive reinforcement for taking care of herself in this manner. Therapists and R.K. completed risk assessments after the dosing session, and Robyn denied any suicidal ideation, plan, or intent and was cleared to return to her overnight stay.
Integration
Robyn expressed some lingering anxiety over the next few days. She reported her usual before-bed anxiety but, unlike before, she was able to sit with the discomfort by repeating the affirmation, “I am safe.” She also described a new way of being present with sadness, stating the sadness felt “smaller” as she is learning to acknowledge and feel it without being consumed by it. She reported various instances of racial trauma that she had not remembered before, and discussed how these experiences impacted her racial identity development and negative views about herself.
Robyn continued to integrate and develop healing practices around her somatic manifestations of trauma. For example, with the ongoing anxiety and distress she experienced as pain in her back and pelvic area, she explored various self-regulation techniques (e.g., humming) to help her ground in the present moment. Robyn began building awareness around her trauma responses so she could explore what it was like to intentionally consider other choices—outside of a fear response—when encountering an intrusive traumatic memory. Robyn described feeling sad and empathetic about her experience of early childhood abuse. There was a cognitive shift in how she conceptualized this to her thoughts about herself in the present day. Robyn was able to verbalize that she did not deserve the abuse she experienced, which indicated notable progress.
Therapist M. H. used an art directive, addressing feelings of anger with clay for continued integration with Robyn (Sholt & Gavron, 2006). The purpose of this was to provide experiences of expression and continued processing from the first dosing session. Robyn was first guided through a meditation focusing on “hard emotions” and sources of anger. She was then instructed to create an object of anger with the use of air-drying clay. Robyn created an unstuffed teddy bear and a pair of empty baby shoes. Robyn felt that these items embodied her struggle never being allowed to be a child both due to abuses within the home, but also various racialized traumas she endured throughout her childhood. During this discussion Robyn recalled when she was in grade school the White children would often destroy her schoolwork, including art projects. Throughout her life Robyn lived in predominantly White, rural areas, and she described that the adults around her did not usually address the bullying and racism she received. During the directive Robyn described feeling child-like and empowered to be able to create something that was praised and would not be destroyed.
The key therapeutic gains from these first integration sessions highlighted the various links between the internalized racism negatively impacted Robyn’s racial identity development (Williams et al., 2016). Although Robyn expressed shock that the first session included content from her childhood, it appeared that there were other race-related messages that were compounding her later work-related traumas. During these sessions, therapists integrated mindfulness exercises with various CBT skills such as Socratic questioning, cognitive restructuring, and various progressive relaxation interventions.
Second Dosing Session
Robyn arrived at this session with her two therapists ready to begin with the intention to break the ruminative “loops” or cycles that created distress for her. Ketamine administration began shortly after 10 am and psychoactive effects peaked around 40 mins.
This dosing session was very difficult for Robyn as she made contact with some of her most painful traumatic memories. She wavered between tearfulness and moderate anxiety throughout the session. She described some of her worst moments of extreme neglect, sexual abuse, and various act of racism that occurred to her when she was at school and at home. At one point, Robyn disclosed an intense but indescribable pain where she expressed suicidal ideation to the therapists. With the assistance of therapists, Robyn was able to use some of the previously discussed self-regulation techniques to help her reorient and regulate her emotions as she moved through the painful content (Frye & Spates, 2012). Therapists also used Internal Family Systems (IFS) interventions to help Robyn ultimately acknowledge the parts of her that wanted to die (e.g., old, internalized beliefs) and not fuse with those thoughts, allowing her to develop a new relationship with herself (Schwartz et al., 2009). Robyn responded well and was able to move through the material and not get stuck. “Multiplicity of parts,” another IFS technique therapists used to help Robyn to identify different parts of her identity that have helped her compartmentalize and cope with the emotional injuries from her past (Lucero et al., 2018). This evidence-based intervention aids in personifying and identifying aspects of one’s self in a way that decentralizes pathology while addressing difficult content. At the end, therapists completed additional risk assessments, and she reported no further suicidal ideation. As an additional precaution, therapists and Robyn still developed a safety plan and scheduled a follow-up phone call for later in the evening.
Integration
This series of integration sessions included Robyn processing past challenges of cross-racial dynamics, in both personal and professional spaces. Robyn described a microaggression she experienced while having breakfast at the hotel she was staying at during treatment. She was standing in line in the dining area, when another guest made the assumption that she was part of the staff, despite not being dressed in the hotel’s uniform. Robyn responded by telling the person that she did not work there. During the session Robyn explained that this type of incident would have previously left her perseverating over the experience for the remainder of the day or longer, but she noted that this time she was able to move past the incident. Robyn reported that unlike before, she did not internalize the incident as evidence of her flaws or lack of worth. She explained she recognized that this microaggressive act did not actually have any bearings on her as an individual and was rather the internalized assumptions of the aggressor. Robyn’s increased awareness allowed her to name the experience for what it was (a microaggression) and maintain power within the dynamic by using her voice and believing her story. This was a major feat for Robyn. She even described being able to successfully use a positive affirmation as a remainder to not enact old coping mechanisms.
Robyn also discussed various injuries she sustained from systemic racism, and how she believed she could “out-do” racism and assimilate to White culture. She described feeling very uncomfortable in predominantly White spaces and sometimes speaking with White people, so she would find ways to present that made her seem more “polite,” “safe,” and “approachable.” As such, she developed a conditioning, a pattern, around these cross-racial dynamics. Robyn’s therapists honored these parts of herself that developed out of necessity and wanted to expose her to other possibilities of engaging with White people. With Robyn’s trauma history in mind, clinicians enlisted a White therapist at the clinic to have a discussion with Robyn about the therapist’s experiences with White privilege and to provide Robyn with the space the share her personal experiences with White people in an empathetic and supportive manner (e.g., Miller et al., 2015). After the exposure with the other therapist, Robyn described shock and disbelief that a White person was willing to openly discuss privilege and did not minimize or try to change her perception of her lived experiences. Robyn integrated the insights well and overall reported a decrease in anxiety and depression symptoms.
Third Dosing
This session was pivotal for Robyn, as she began to harness a deeper presence within her body and trust in herself to process through emotional experiences. Robyn’s intention for this dosing session included gaining clarity on her career and continuing to understand the survival behaviors she developed that no longer served her. Up until this point in treatment, Robyn was anticipating going back to the same work environment where previous discrimination took place. She described feeling like her choices were limited despite the fact that she had a very impressive work history and skill set for her field.
The content of this dosing session included continuing to process the internalized beliefs Robyn acquired from childhood and naming “safe” White people she encountered in her lifetime. She was able to identify moments that negatively impacted her while also recognizing she deserved better. Some insights she expressed include: “I know why I had so many problems in the classroom. It was the racism. How could I learn while being spit on and hit?” and “I have some fears with work and how people will treat me. . .Why should I have to leave? They should leave. They hated me, but I knew my stuff, so they couldn’t fire me.” When asked by therapists what she had learned in regard to her workplace discrimination, Robyn responded, “I did nothing wrong. There is nothing wrong with me.”
During this session Robyn began to find acceptance and compassion for herself from those past experiences and accessed memories of her experiencing joy, and what it meant to be human. Robyn described positive memories of having fun for the first time in her life, and individual moments where she felt what it was like to be free from oppression. As Robyn defused from the negative internalized messages from her past, she recognized the magnitude of her oppressive work environment, and even began to explore alternative work options. Therapists completed a risk assessment after the ketamine effects wore off, and Robyn denied any suicidal ideation, plan, or intent.
Integration
The next morning, Robyn presented to therapy with mild anxiety but described feeling more proficient in her ability to use various coping skills to stay with the discomfort until it passed. She reported feeling her anxiety turn to anger since processing so much content from the dosing session the day before. Robyn explained that the anger seemed to be toward the various injustices she had faced over the past few years. She shared that exercising served as a healthy outlet for managing anger and finding ways to “let go”. At this point in treatment, Robyn began speaking in future-oriented terms and identified how people in her immediate circle have held similar roles as those that abused her during her early childhood experiences. She noted, “My spouse is like a repeat of my family,” drawing comparisons on how he often dismissed her and provided very little support, just as her parents did.
In addition to Robyn’s successful use of coping skills, she also reported applying for new jobs in a new geographic location. While part of this session was spent integrating the powerful breakthroughs that Robyn experienced, she also became very energized and motivated to explore her options surrounding obtaining a new job in a new city. Therapists continued to reinforce Robyn’s new ways of coping and taking on action-oriented means to change her more immediate, environmentally based problems. During the first half of treatment Robyn was very focused on how to cope when she no longer qualified for disability and how to re-enter her previous toxic work environment. After the third dosing session Robyn was able to acknowledge how reentering this environment had potential for additional harm, and that she had a variety of options in terms of seeking new employment. Not only did she see a new job as viable, but she also was able to state that she was very much qualified for various positions.
Fourth Dosing
Robyn’s intention for this dosing session included deepening her awareness of herself and beginning to recognize her power. Robyn entered the session with mild anxiety and described having four very vivid dreams the night before. She and therapists briefly processed through the content of the dreams as she found them to have very symbolic tones in relation to her previous dosing session. The themes included taking control during conflict, providing for the Black community, and decision-making.
At the onset of the medication Robyn described a sensation of “being pulled through time,” by her higher self, and was being pushed toward her present experience and looking ahead. “Ketamine is waking everything up,” she shared. Robyn described fears about the possibility of facing additional trauma and the exhaustion that she felt as a Black woman existing in oppressive spaces. Similarly to the third dosing session, Robyn spoke in future-oriented terms and began exploring life beyond her trauma lens, and what she would leave behind. She had moments to grieve those losses, and eventually found her way to laughter, enjoying the idea of what it means to fear-less.
Robyn discussed possibilities of starting a new life, a new job, and developing new relationships. She described an understanding of the challenges ahead, but also described a newfound confidence and trust in her abilities in taking risks. She described a recent moment where she went on a hike and had a few memorable experiences. The hike provided various unmarked trails, which she was able to navigate her way through without getting lost. She explained only taking “rights” so that she could navigate back without losing her way. Despite her apprehension of exploring a new area, due to fear around potentially racist interactions, she proceeded anyway and felt more confident because of it. Robyn ended the session discussing what it means to feel safe. She described spending years creating a safe space for herself, and began recognizing how, in relationships and the workplace, she mistook comfort for safety. She arrived at the awareness that she knows how to keep herself safe, as she’s been doing it her entire life. She concludes with “it feels good to trust myself.” She found safety with herself and was able to imagine new possibilities for her life as a result. Therapists completed a risk assessment after the ketamine effects wore off, and Robyn denied any suicidal ideation, plan, or intent.
Integration and Assessment
During these sessions, therapists administered the closing measures (BDI-II and PTCI) and helped Robyn continue consolidating the gains she made over the past 13 days. Robyn reported a new ability to move through her difficult memories and emotions rather than allowing them to consume her or pushing the emotion away. Therapists reviewed the many CBT skills, breathing techniques, and additional therapeutic tools Robyn found most helpful. When asked what she was able to take from treatment, Robyn reported a new awareness of her emotional processes and an ability to be proactive rather than reactive during moments of stress. She stated, “Failures are part of the process, and those failures mean nothing about me.” Robyn explains a hope to translate these skills to the workplace in the near future.
Robyn also shared she had a job interview scheduled for the following week, which further demonstrated her ability to successfully maneuver her behavioral responses despite the fears she described in the most recent dosing session. Robyn reported that she felt her bigger area of opportunity was working on her negative self-talk through reframing rather than her habitual response to self-criticize. Her post-treatment plans consisted of continued therapy with her local therapist and follow up sessions with S.R. and M.H. at 1 month, 3 months, and 6 months.
Outcomes
Robyn’s overall levels of anxiety and depression decreased significantly in the 2-week span. She also experienced an improvement in her sleep, sleeping an average of 8 to 10 hr a night, whereas prior to treatment she struggled to maintain 4 hr. Robyn reported a decrease in ruminative thoughts and felt a deeper understanding of herself and her traumas. Robyn’s self-report scores demonstrated a consistent reduction in anxiety, distorted cognitions, and depression symptoms throughout treatment, with her depression symptoms decreasing to a sub-clinical range as measured by the BDI-II. At intake Robyn scored a 40 on the BDI-II and on her final day of the KAP-IOP her score decreased by 27 points. This decrease in symptoms was also demonstrated in Robyn’s decreased score on the PTCI. At intake Robyn scored 207 on the PTCI and by the end of the 2-week KAP-IOP she experienced a decrease by 70 points. At the 6-month follow up session, Robyn experienced a 1-point decrease in her PTCI score (136) but a 16-point increase on her BDI-II (29). These changes are shown in Figure 2.
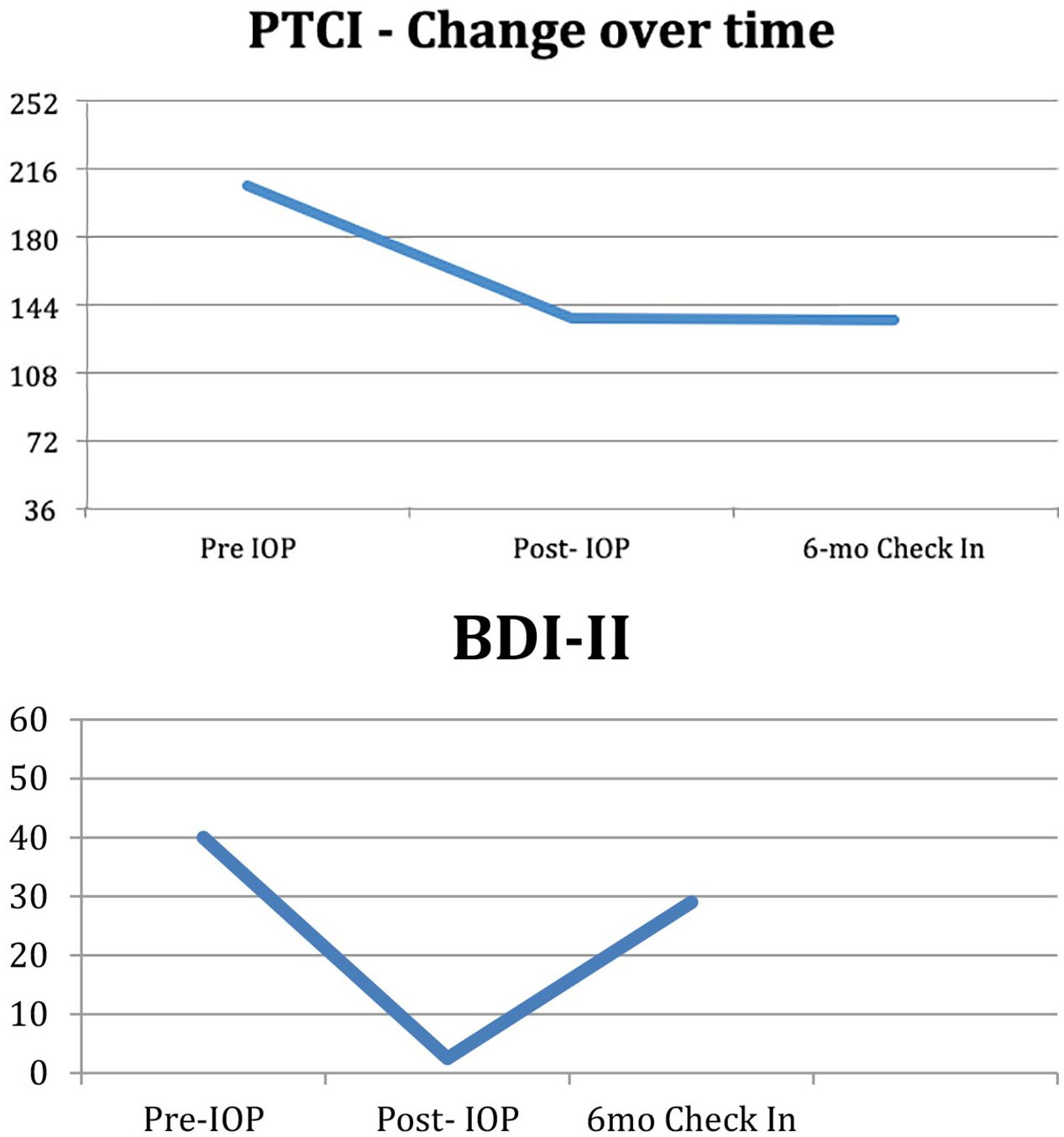
Changes in test scores over time.
8. Complicating Factors
It is important to note that it takes presence, patience, and skill among therapists to work with clients in altered states of consciousness who experience suicidal thoughts. While many traditional psychotherapeutic interventions are useful in addressing suicidality, some interventions can create more harm or feelings of confusion for clients in such a vulnerable state, like a dosing session. Although a detailed account of how to work with suicidality in a dosing session is beyond the scope of this paper, there are a couple of considerations the authors want to highlight: (1) make sure your de-escalation tools or techniques are culturally appropriate, (2) encourage clients to stay with the feeling versus fusing with the thoughts, (3) at the conclusion of the session complete a risk assessment and develop a safety plan. Sensations of dying, fears about dying, or wanting to die can all be a valuable part of the therapeutic process. One study by Carbonaro et al. (2016) found that the degree of difficulty with undergoing a challenging psychedelic experience was positively correlated with the subjective personal meaning to the participant. For Robyn, it was a necessary and valuable part of her process as she was able to move through this experience.
Although Robyn made tremendous gains during her time in treatment, it was anticipated that she would inevitably return to various environments where she would experience new acts of racism. This was already exemplified during day 8 of treatment when she was mistaken for a hotel staff member. At the onset of treatment Robyn described struggling to spend time in public spaces due to fears of discrimination. Because the IOP clinic was located in a small town, not only were Robyn’s options very limited, but the unfamiliarity led to some resistance with spending time in public locations separate from her discrimination fears.
9. Access and Barriers to Care
Experiences of discrimination are common, traumatizing, and create barriers to care. One study found that Black American adolescents experience as many as five acts of discrimination on a daily basis (English et al., 2020). Given the high rates of discrimination experienced by African Americans, many may feel hopeless in finding a clinician who understands these issues or finding relief from the mental health sequalae of racism. Indeed, few clinicians are trained or equipped to treat racial trauma (Hemmings & Evans, 2018).
In Robyn’s case, the trauma of racism was combined with barriers that included lack of access to care in her locale, financial constraints, and lack of an adequate support system. Robyn’s PTSD symptoms had increased so greatly that she could no longer work, and this led her to collect temporary disability while undergoing treatment. In addition to the financial constraints and only having enough funds for her necessities, Robyn had to travel across state lines in order to obtain quality treatment. Robyn did not have nearby access to culturally competent care, and it was still quite expensive for her to be enrolled in the KAP-IOP, and then arrange lodging and transportation. Affordability and local access continue to be a barrier for treatment for many people who could otherwise benefit from KAP. Further, because Robyn traveled from out of the area, the KAP sessions were spaced closer together than some approaches that may provide more time between sessions for integration work.
10. Follow-Up
Follow-up is critically important for KAP clients (Ryan & Bennett, 2020). As such, clinicians conducted triadic follow-up sessions at 2-weeks, 3-months, and 6-months. These sessions took place virtually using encrypted, video conferencing software. Due to Robyn’s symptom presentation, sessions continued with the 90-min format to provide ample time for processing and continual integration of ketamine experiences. Clinician S.R. continued to meet with Robyn on a biweekly basis for 3 months after the 2-week follow up. It should also be noted that Robyn also had a supportive therapist back home whom she continued to work with on the weeks that she did not meet with S.R. After 2-months Robyn discontinued therapy with her local therapist and continued telehealth care with S.R.
Two-Week Follow Up
At her 2-week follow-up, Robyn spoke confidently and with conviction about the changes she began to make in her life. She reported successfully implementing interventions for anxiety, negative self-talk, and emotional self-regulation. During this time Robyn also received an invitation for a second and third interview with the company she applied for while in treatment. Despite Robyn’s described fears throughout the session, she made several encouraging statements including: “I set the standard for my life,” “I am flexible and can adapt to change,” and “I honor my past, but it does not dictate my narrative.”
Robyn continued to experience the positive effects from the KAP-IOP. As a Black woman who experienced discrimination in the workplace, Robyn’s fears of starting a new job with a new company were warranted, but she overcame those fears and replaced them with healthy coping strategies and more affirming views about herself. Some of those affirmations include “it’s okay to be happy; I am learning to retrain my thoughts; It’s amazing what your mind can do when trauma does not guide your life.” She also reported an increased awareness around her behaviors and began engaging in more meditative practices. Although no measures were used to assess her symptoms at this point, the language Robyn used to describe her life and current circumstances demonstrated her gains.
Three-Month Follow Up
At the 3-month follow up with Robyn, she began making action-oriented changes for her mental health and livelihood. She got the job she applied for while in treatment and was in the process of putting her home on the market to move to the new city where she would begin work. Robyn continued to reframe various negative interactions she had with others and explained that she was able to not personalize or internalize those experiences as she had so often in the past. Robyn also reported that she was no longer in a relationship with her previous partner, and that she began attending various “MeetUps” in the surrounding area. Her social-based fears continued to dissipate as Robyn implemented the healthy coping mechanisms learned in treatment. After the 3-month check in, Robyn continued to meet with S.R. for ongoing clinical care.
Six-Month Follow Up
After starting a new job in a new state, Robyn experienced an increase in depressive symptoms when adjustments to a new environment and new culture proved challenging. It must be noted that this increase in symptoms also took place just 2 months into the SARS-CoV-2 (COVID-19) pandemic. Shelter-in-place orders, limited social support in a new environment, and the uncertainty of the pandemic left Robyn feeling vulnerable and unsafe. Robyn’s depressive symptoms were assessed through a verbal report to S.R. which led to the decision for a supplementary ketamine dosing session. During this session Robyn was administered 75 mg of ketamine via lozenge, half of the dose that was administered during the IOP. The majority of the session Robyn experienced several affirming experiences and made statements such as, “I can feel happiness coming out of my chest!” and “I’ve been re-creating patterns of suffering throughout my life. Suffering was my comfort. . .. Love and peace can be new ways I comfort myself.” After the medication’s effects wore off, Robyn reported feeling like her mood “lifted.” S.R. continued to meet on a weekly basis for further integration of Robyn’s experiences.
11. Treatment Implications of the Case
The successful initial treatment of Robyn’s depression and PTSD provides evidence to support the use of ketamine-assisted psychotherapy for the treatment of racial trauma with comorbid depression and suicidality. While Robyn no longer met diagnostic criteria for Persistent Depressive Disorder at the conclusion of the IOP, she did require ongoing care to address her complex trauma history. Despite still experiencing some symptoms of PTSD, Robyn was able to regain functioning in all domains of her life, which was remarkable given her presentation only 2 weeks prior. With ongoing biweekly treatment, the likelihood of Robyn’s residual PTSD symptoms continuing to decrease was strong.
12. Recommendations to Clinicians and Students
Robyn’s case includes several important considerations surrounding the experience of racialization, psychedelic medication, and trauma. Because people from communities of color may mistrust mental health practitioners, clinicians can reduce barriers by learning about racism, microaggressions, and increasing their cultural competence (Williams & Halstead, 2019). A study by Hook et al. (2016) found that some of the most common microaggressions committed by therapists included a denial or lack of awareness of stereotypes and bias, and avoidance of discussing cultural issues. This can cause problems in psychedelic-assisted therapy if cultural or racial materials arise during sessions and therapists are not prepared to address it in a skillful manner (Williams et al., 2020b). When treating clients who have experienced discrimination, it is important that they approach these disclosures with openness, curiosity, and maintain cultural humility. Cultural humility means that clinicians maintain an other-oriented perspective that involves respect, lack of superiority, and attunement to patients’ cultural heritage (Hook et al., 2016). Some orientations that emphasize mindfulness and humility within therapist-client interactions are FAP and MBCT, third-wave behavioral therapies which were useful in this case (Walsh & Thiessen, 2018).
A qualified medical professional should evaluate all clients considering ketamine-assisted psychotherapy before beginning treatment (Ryan & Bennett, 2020). This is to ensure that the client does not have any preexisting health conditions that could disqualify them from treatment, such as specific heart conditions or a mental health diagnosis involving psychosis. In instances such as Robyn’s, it is also important to continuously assess for suicidal ideation, especially when someone has engaged in previous attempts. While ketamine has tremendous effects in decreasing suicidal ideation (e.g., Calabrese, 2019), such thoughts can temporarily worsen (Ryan & Bennett, 2020). Further, for clients with severe dissociation in PTSD, there is some concern that ketamine may be contraindicated due to its dissociative effects (Liriano et al., 2019). Dr. Raquel Bennet of the Kriya Institute notes that high doses are not recommended (1.0 mg/kg bioavailable) and even lower doses KAP should be done with care and caution in this population; the quality of the therapeutic relationship is critical for success in these cases (personal communication, December 31, 2020). For situations in which a client may not qualify for KAP, it is important to have alternative treatment options readily available.
Another important consideration for treatment is the client’s support system. Robyn’s case was unique in that she did not go home or to her partner’s house for the 2 weeks the treatment took place due to traveling out of state for care. However, psychedelics often leave clients feeling vulnerable and susceptible to subsequent traumas or injuries. Robyn was willing to place boundaries with her partner at the beginning of the IOP, but having the additional emotional hardship of his criticisms could have changed her trajectory.
A final recommendation for treatment is for clinicians to also have their own self-care strategies in place throughout psychedelic assisted treatments such as ketamine. During dosing sessions clients can enter states of re-experiencing and emotional dysregulation that can be intense and taxing. Due to the length of the dosing sessions it is imperative that clinicians maintain focus and attentiveness to the client’s needs that may arise at any moment. In the case of Robyn, her treatment consisted of a total of 16 hr of dosing sessions and 24 hr of integration/preparatory sessions across a 2-week period. This case study suggests that existing evidenced-based treatment, delivered with necessary adaptations, can produce successful outcomes. Robyn’s case illustrates that a client of color suffering from racial trauma can improve with ketamine-assisted psychotherapy, when the therapy is completed within a culturally attuned container/framework. Regarding her perspective on ketamine-assisted psychotherapy, Robyn shared, “Ketamine therapy treatment helps you become who you were supposed to be; I feel like I am living a dream. The encouragement from my therapists helped me to believe that, maybe, I can do anything.”
Footnotes
Acknowledgements
The authors would like to thank Julian Finnegan and James DiLoreto for help with treatment and Joseph La Torre for proofreading assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was undertaken, in part, thanks to funding from the Canada Research Chairs Program.