
Abstract
Parent–child interaction therapy (PCIT) is an empirically supported behavioral parenting intervention developed for families with young children who have significant behavior problems. In Japan, PCIT was introduced in 2008 as a parenting intervention method and later introduced to therapists. This case study reports on the detailed use of PCIT, originally developed in Western cultures, for a 5-year-old Japanese boy with behavioral problems and his mother. During the treatment, the mother successfully acquired PCIT skills in the early stages of the coach sessions that led to improvements in the child’s problematic behavior. However, especially in the later stages of the treatment, the mother was too tired/distressed to focus on the treatment, which complicated the implementation of PCIT (e.g., unable to do homework, canceled sessions). This was mainly because she was a full-time working mother who was very busy with work, housework, and child-rearing, and also had no help from her husband. Cases such as this are commonly seen in current Japanese society. In summary, this case study supported the potential effectiveness of Western-originated PCIT for Japanese families with children who have behavioral problems, and also argued that there is a need for PCIT therapists to carefully assess and address the primary caregiver’s distractions outside the session room especially when working with Japanese working mothers.
1 Theoretical and Research Basis for Treatment
Parent–child interaction therapy (PCIT) is a short-term, evidence-based intervention designed for families with young children displaying a broad range of behavioral, emotional, and family problems (Eyberg, 1988). PCIT is unique among parenting interventions in its use of live, bug-in-the-ear technology to deliver incidental coaching to parents during therapy (Lieneman et al., 2017). The PCIT therapist coaches parents while making real-time adjustments to the treatment based on observations of parent–child interactions. PCIT typically progresses through two distinct phases: a relationship-enhancement phase (child-directed interaction [CDI]), in which parents learn the principles of nondirective play therapy to strengthen parent–child bonds and increase the prosocial behavior of their children; and a discipline phase (parent-directed interaction [PDI]), in which parents learn behavioral strategies to reduce noncompliance and other negative behavior in their children. During both phases, daily homework is given to provide an opportunity for parents to practice/apply their acquired skills with their children at home.
Several meta-analyses have demonstrated that PCIT is effective in improving numerous child behavior problems both in the short- and long term (Cooley et al., 2014; Thomas et al., 2017). PCIT was originally developed in the United States, but it has been translated to several languages and disseminated internationally, not only in Western countries (e.g., United States, Australia, Germany, the Netherlands, Switzerland) but also in non-Western countries (e.g., Indonesia, Jamaica, Lebanon, Hong Kong, Taiwan, South Korea, Japan; PCIT International, n.d.). However, although increasing evidence suggests the efficacy of PCIT even when transported from the United States or Australia to other countries (Thomas et al., 2017), a more careful examination or observation of cultural differences in parent–child interactions and the impact of these differences on treatment is needed.
In Japan, PCIT was introduced in 2008 as a parenting intervention method and later introduced to therapists; it is currently being practiced mainly by PCIT-Japan (PCIT-Japan, n.d.). PCIT-Japan was established in 2011, working closely with PCIT International, and promotes fidelity in the practice of PCIT in Japan through research, training, and continuing education of Japanese therapists and trainers. The Japanese version of the PCIT protocol was developed in the following steps: (a) The original PCIT protocol was initially translated into Japanese by researchers from PCIT-Japan, (b) the translated protocol was transferred to a Japanese–English bilingual translator who was not involved in the initial translation for a back-translation, (c) the back-translated protocol was reviewed by the original developers (Eyberg and her colleagues), and (d) PCIT-Japan researchers, a bilingual translator, and the original developers reviewed and fixed it to finalize the protocol. There were no major cultural modifications to the protocol. Following this, Kamo (president of PCIT-Japan) and her colleagues then performed a first pilot trial among 11 Japanese cases and reported the potential efficacy of PCIT for children and parents who experienced domestic violence (Kamo, 2010). Hosogane and colleagues (2018) recently published the first case study written in English, describing how PCIT effectively worked in improving the problematic behaviors of two Japanese children with attention-deficit hyperactivity disorder (ADHD). However, none of the studies have addressed the cultural perspectives of using PCIT for Japanese cases.
In this article, we describe the treatment course of PCIT for a 5-year-old Japanese boy with significant behavioral problems and his mother. We also highlighted and discussed complications in therapy that are possibly influenced by Japanese culture (e.g., parenting practice, problems of working mothers in Japan).
Ethics Approval and Informed Consent
Written consent for the current case study was obtained from the mother, and the study was approved by the Ethics Committee of Nihon Fukushi University in Japan (approval number: 18-03).
2 Case Introduction
Akira (pseudonym) was a 5-year-old boy who went to a nursery school. His 38-year-old natural mother, Miki (pseudonym), was a full-time office worker at a general hospital, and also did all of the housework and child care. The family composition included the biological father (40 years), Miki, Akira, and a younger sister (3 years); they were living together.
3 Presenting Complaints
Miki sought consultation because she was experiencing high levels of stress from Akira’s problematic behavior and was having difficulty with child-rearing. Miki wanted to ameliorate Akira’s restless behavior. Akira sometimes had trouble with his classmates at the nursery school, so Miki also wanted to improve his friendships. Miki sometimes hit her children. Miki said that she required stress relief, as she tended to feel irritable and take it out on her children. Her husband (Akira’s father) worked as a banker, and Miki said that he was not cooperative with child care and housework. He was mostly away during weekends because he played golf with his work colleagues.
4 History
Akira was born in an urgent premature delivery and weighed 2,285 g at birth. His developmental history revealed that he had no physical illnesses or injuries and had no delay in developmental milestones, including intellectual development. Miki was not particularly concerned about him until the arrival of the second child. Around the time she was hospitalized (for about a month) for urgent premature delivery of the second child, she began to feel that Akira was making impossible demands and did not listen to her, and she started feeling frustrated and angry with his behavior. Around the same time, Miki was told by his nursery teacher that Akira was drawing on another child’s paper and hit his friend if he did not get his way. His teacher also reported that his concentration was poor compared with other children. Miki then became concerned with Akira’s problematic behavior. The nursery teacher suggested that she should consult with the local child welfare center regarding his problematic behavior as well as Miki’s inability to control her emotions leading to her hitting Akira. Miki then visited the local child welfare center, but the contact person just noted her complaints and offered no particular guidance.
Miki has a bachelor’s degree and had no history of learning disability or developmental problems. When she was a university student, she had some interpersonal problems and received counseling. When her current job became busy, she got stressed and went to a psychiatric clinic and was prescribed medications for autonomic dystonia; but she decided to stop taking it. When she received an annual stress-check program at her workplace, she was identified as a high-stress employee and then referred to a private counseling center, the Caring Life of Women and Children Research Group (LifeCWC).
5 Assessment
At the baseline assessment, the following Japanese versions of measurements were used: the Child Behavior Checklist for Ages 1.5 to 5 (CBCL1.5-5; Funabiki & Murai, 2017), the Parenting Stress Index (PSI; Araki et al., 2005), the Eyberg Child Behavior Inventory (ECBI; Kamo, 2016), and the Beck Depression Inventory–II (BDI-II; Kojima et al., 2002). Both the ECBI and BDI-II were also assessed before every session.
CBCL1.5-5 was used to evaluate the child’s behavior level. At the baseline assessment, Akira scored 33 on the Introversion Scale (T score = 85) and 39 on the Extraversion Scale (T score = 86), which was in the clinical range for flagging. Akira also scored 31 on the Aggressive Behavior subscale, suggesting strong traits of ADHD.
The ECBI consists of 36 items and is administered to parents to assess behavioral problems in children between 2 and 16 years old. The ECBI provides an intensity score that quantitatively captures a child’s problematic behavior (clinical cutoff ≥ 132) and a problem score that measures the caregiver’s subjective feeling of child care difficulties (clinical cutoff ≥ 15). At the baseline assessment, Akira’s intensity/problem scores were 177/19, which meant that he had a high frequency of, and several significant, behavioral problems. Highly rated items were “has poor table manners,” “dawdles in getting dressed,” “has temper tantrums,” “whines,” “is easily distracted,” and “is overactive or restless.”
The PSI was used to identify dysfunctional parenting and predict the potential for parental behavior problems and child adjustment difficulties within the family system. The parents’ stress is assessed with the Child Domain and the Parent Domain subscales. Miki scored high on all items: The total score was 295, Child Domain was 135, and Parent Domain was 160, which indicated a need for professional care. Scores for “few responses that please the parent,” “the child’s bad mood,” “social isolation,” “depression/guilt,” and “difficult to feel an attachment to the child” were in the 95th percentile or above, suggesting that Miki had a weak attachment to the child and that she found raising the child stressful.
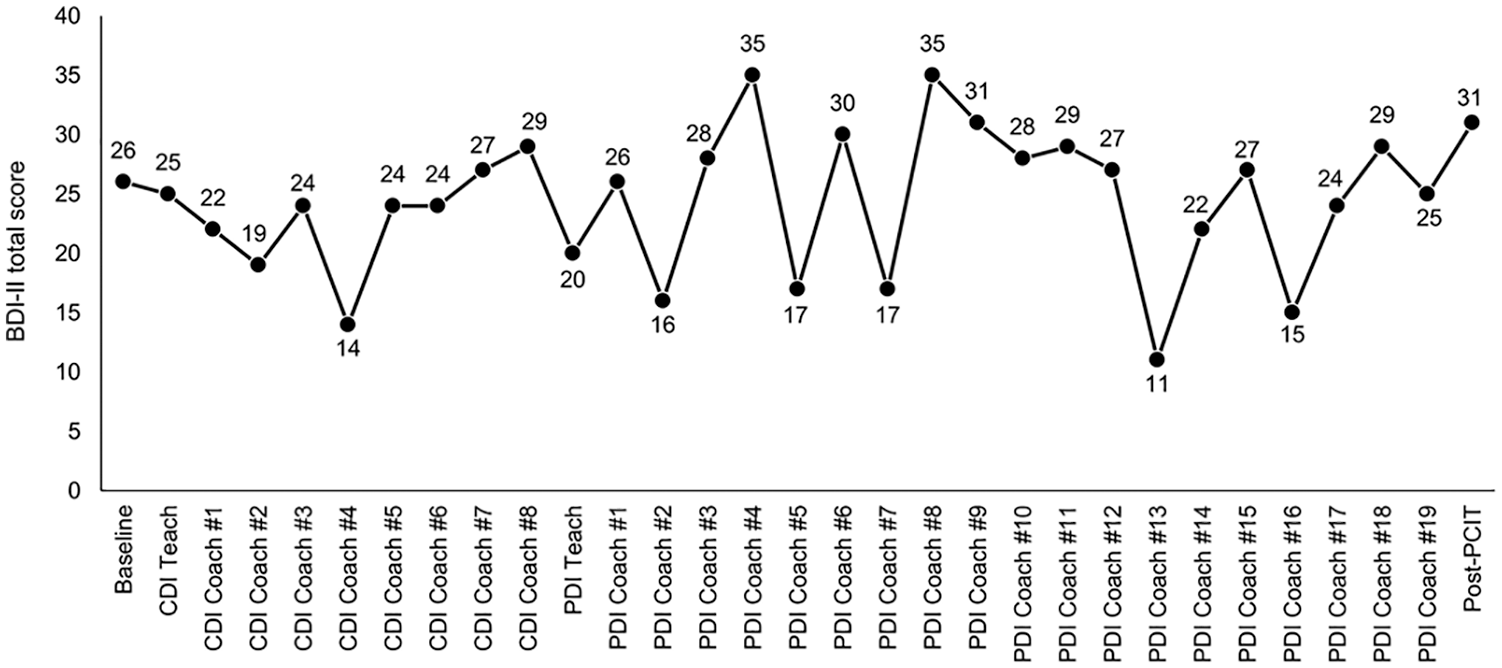
The BDI-II, a self-report instrument that comprises 21 items with a 4-point response scale, was used to measure Miki’s depressive symptoms. At the baseline assessment, Miki scored 26, suggesting that she had moderate depression.
We also video recorded Akira and Miki playing in the observation room. We used these video records to assess the quality of Miki’s verbalizations when interacting with Akira by counting the frequency of parent verbalizations based on a structured behavioral coding system (Dyadic Parent–Child Interaction Coding System [DPICS]; Eyberg et al., 2005). The DPICS measures several categories of parent and child behaviors, which are documented using a video coding system based on frequency in real time. We used the results of DPICS to create a composite of “do” skills (behavior descriptions, reflections, labeled praises) and “don’t” skills (questions, negative talk, and commands). At the baseline assessment, Miki did not speak to Akira very often. Akira was initially focused on his play but appeared to get bored soon, and started walking around the room touching the video camera. At this point, Miki called Akira’s name in a loud voice so as to stop his behavior, but he did not take notice of her command. Miki often asked “why” in response to Akira’s actions and issued prohibitive orders, such as “don’t do that.”
6 Case Conceptualization
Based on reports from Miki, a variety of assessment measures, and an observation, Akira presented several behavioral problems such as aggression, inflexibility, annoying others, disobedience, hitting, emotion dysregulation, and running away. These problems occurred at home, school, as well as in community settings. The CBCL1.5-5 and ECBI scores suggested that he had strong traits of ADHD, but did not meet the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) criteria for ADHD.
His mother, Miki, also had problems such as distress, depression, and fatigue, leading her to physically punish her children. She thought that these emotional/behavioral problems were mainly due to Akira’s behavioral problems. In addition, Miki felt stress because she was very busy with work, child care, and housework, and did not receive enough support from her husband, parents, public institutions, or medical facilities.
We initially aimed to reduce Miki’s stress by improving parent–child interaction and reducing Akira’s behavior problems. More specifically, our goal with Akira was to teach him to pay attention to appropriate behavior, follow parental directions, and use appropriate communication with Miki. Our goal with Miki was to help her learn to reinforce Akira’s appropriate behavior, ignore his inappropriate behavior when possible, and use a consistent discipline plan when needed. To reach these goals, PCIT was selected as the intervention plan because of positive evidence for this approach in treating young children with behavioral problems (Thomas et al., 2017). Through PCIT, Miki would learn adequate skills for taking care of Akira and correcting his problematic behavior, and thereby reduce her stress.
7 Course of Treatment and Assessment of Progress
Akira and Miki attended weekly 90-min PCIT sessions (total 29 sessions, including two teach sessions) provided by two therapists (AF and KH). The first author (AF) served as the leading therapist; she was a registered nurse and completed 40 hr of a PCIT-Japan initial workshop. During therapy, the therapists also received regular supervision by the PCIT International Certificated Master Trainer in Japan.
CDI Phase
In the CDI teach session, Miki learned to follow Akira’s lead during play, and reinforce his behaviors through the use of three core skills (“do” skills: labeled praise, reflections, and behavior descriptions), while using a learned plan to ignore his inappropriate behavior. To encourage Akira to lead the play and to improve his compliance/self-esteem, Miki also learned not to give commands, ask questions, or use negative talk (i.e. “don’t” skills). Miki seemed to listen to the therapist’s instructions seriously in this teach session.
During the CDI coach sessions, the therapists coached Miki in the use of CDI skills via bug-in-the ear technology through a one-way mirror to achieve mastery of CDI skills (defined as 10 behavioral descriptions, reflections, and labeled praises coded within the 5-min observation, as determined by DPICS coding). Figure 1 summarizes Miki’s progress toward CDI skill mastery. At the second CDI coach session, Miki’s behavioral description significantly increased to the mastery level. So the therapists encouraged Miki to use more reflection and labeled praise skills while reducing questions and indirect commands. Around the second and third sessions, Akira’s problematic behavior also stopped. However, after the fifth session, Miki got busy and stressed because of the Christmas and New Year season; so she was sometimes unable to do CDI homework. Her ECBI and BDI-II scores also got worse (see Figures 2 and 3). Although her busy life continued, she demonstrated mastery of CDI skills at both the seventh and eighth sessions, so Miki and Akira advanced into the PDI phase. At the final (eighth) CDI session, Miki told the therapists that “my parenting has really changed, and my friends and Akira’s teacher said he is calmer now” and “recently, Akira sometimes fawns upon me.”
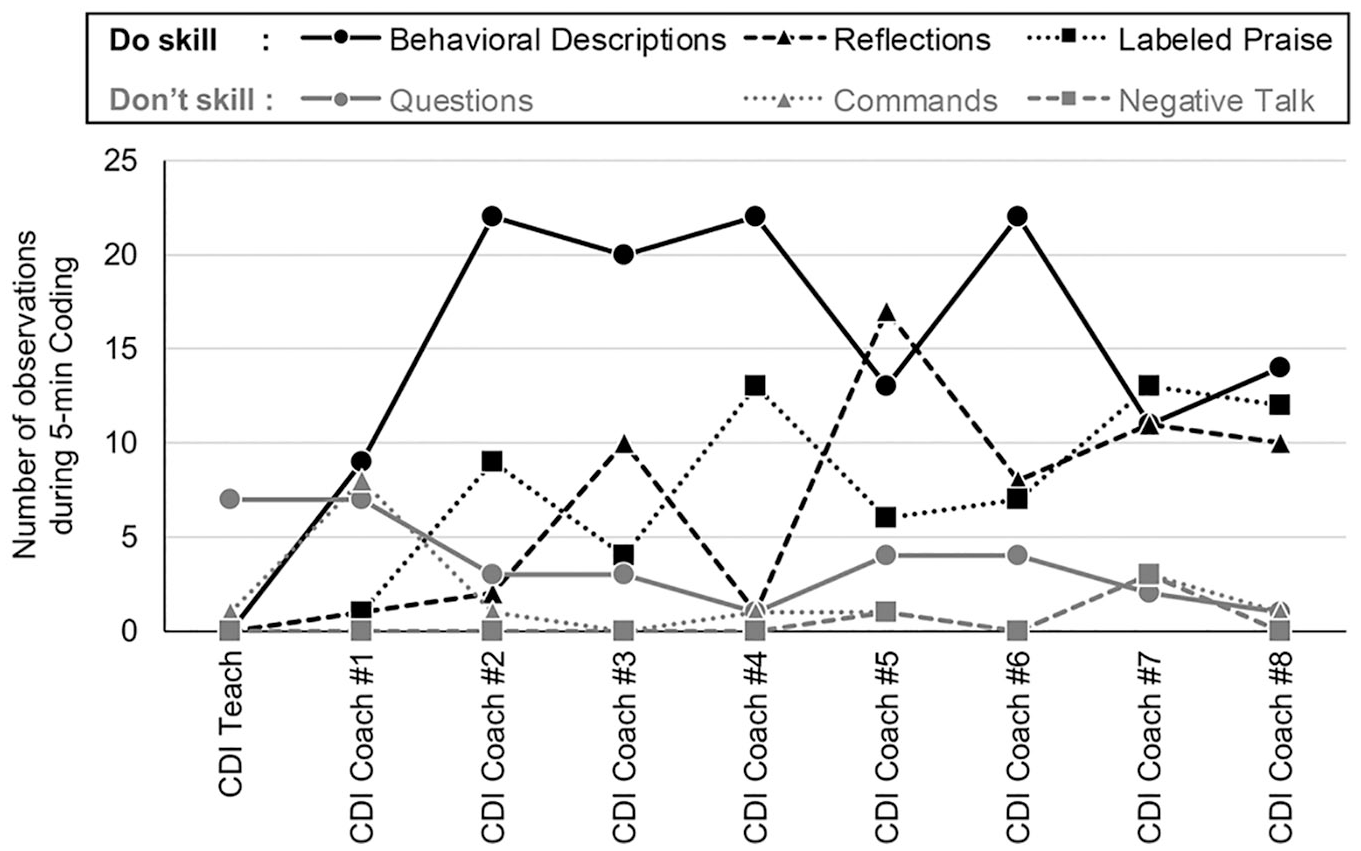
Mother’s progress in mastering PCIT CDI skills.
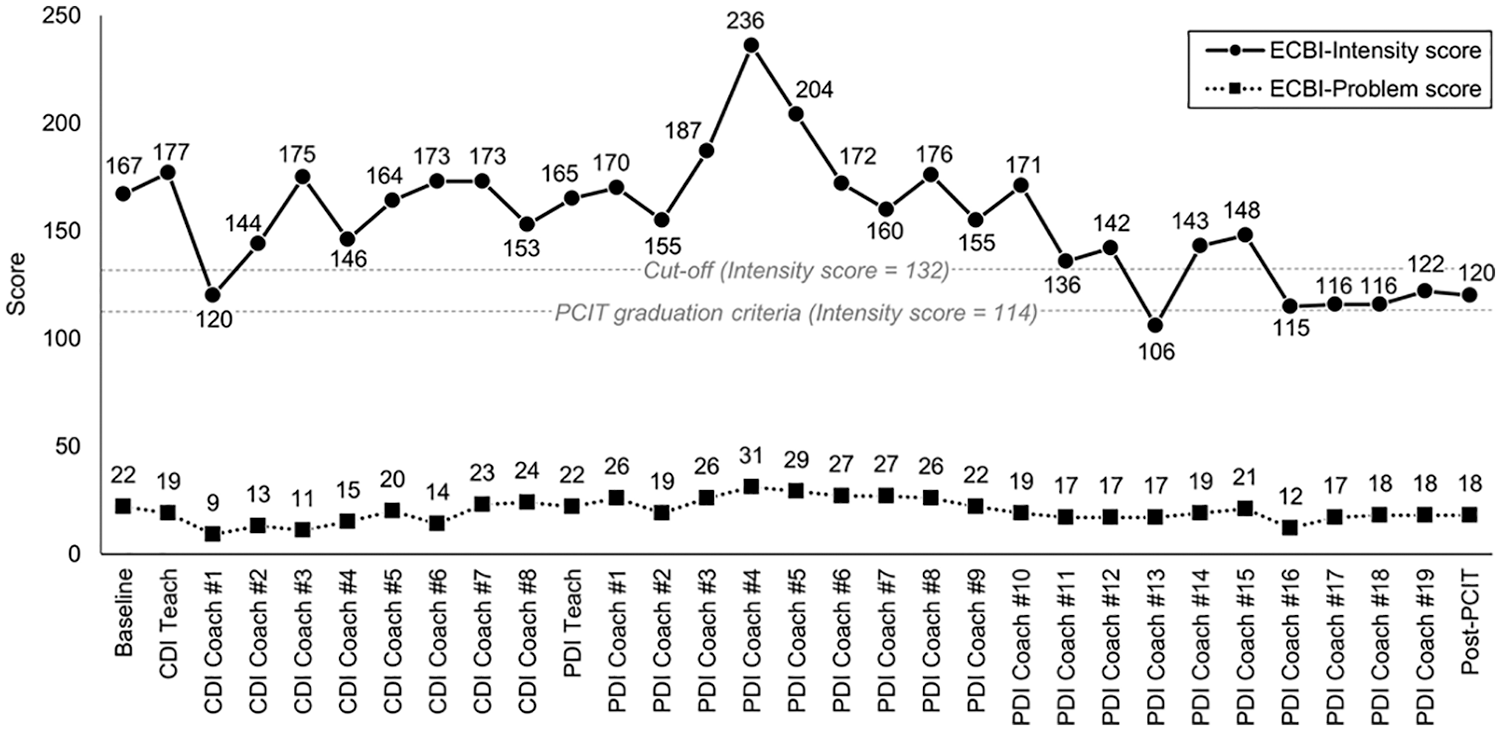
Mother’s ECBI ratings over the course of PCIT.
Mother’s BDI-II ratings over the course of PCIT.
PDI Phase
In the PDI teach session, Miki was taught to use effective commands and a structured, consistent time-out sequence to increase the immediacy, predictability, and consistency of punishment for noncompliance. Effective commands were modeled, practiced, and reinforced by the therapists. Mastery of PDI skills is defined as (a) at least 75% of commands given by parent are effective and (b) 75% of the parent’s commands have a correct follow-through (i.e., labeled praise for compliance, appropriate use of the time-out warning/procedures for noncompliance).
During the PDI coach sessions, Miki initially struggled to give a direct command (in the first session), but in the following session, she was able to completely avoid indirect commands and Akira demonstrated 100% compliance with her direct commands. In the third session, Miki continued to use direct commands, and also gave warnings when Akira did not comply with her commands.
However, during the following five sessions, Miki got busy again outside the treatment. She needed to work a lot of overtime, and was also busy preparing for several of Akira’s school events (e.g., school trip), while doing housework and taking care of her children without any help from others. So she could neither get enough sleep nor perform PDI homework. Around this time, Akira often did not listen to Miki and got in fights with classmates. During the sessions, Miki sometimes gave commands that demanded two actions at the same time, and even when she gave a direct command, she could not wait until Akira followed the command, but instead angrily gave the next command. Miki’s ECBI and BDI-II scores at the fourth session were her worst (ECBI-Intensity/Problem = 236/31, BDI-II = 35). So the therapists recommended that she see a psychiatrist or other mental health professional, but she refused.
During the ninth to 14th sessions, when Miki’s work had temporarily settled down, she was able to give effective commands and use a time-out sequence for noncompliance both in the session room and at home. At the 14th session, Miki achieved the mastery criteria for PDI skills and Akira was also compliant with 100% of her commands. Most of the time, however, she was very busy at work and home, so she could not practice PDI skills at home (especially the time-out warning/procedures) and sometimes canceled sessions. So the therapists and Miki decided to do a few more PDI sessions to establish acquired PDI skills in her daily life.
However, during the subsequent PDI sessions, Miki’s situation grew even worse. She was transferred to a different department and needed to do more overtime, and Akira had several school events (e.g., sports festival). She wanted to seek help from her husband, but she could not discuss it with him because she was hesitant and did not make time. She sometimes hit Akira when he did not follow her commands at home. During sessions, she often yawned and looked tired/sleepy due to lack of sleep, but continued to use CDI and PDI skills effectively with Akira. However, she often could not work on PDI homework and found it difficult to implement/practice time-out warnings at home.
At the 18th session, Miki said she wanted to end the PCIT sessions because she was currently too busy to attend on a weekly basis. In addition, Akira was going to enter elementary school soon, so she would be very busy preparing him for school every day. Miki’s ECBI-Intensity score of 116 was still above the PCIT graduation criteria (= 114), but was below the cutoff score (= 132; see Figure 2). Although she could not use CDI and PDI skills at home, she reached the CDI and PDI mastery level in the session room. Thus, the therapists decided to accept Miki’s offer to end the PDI/PCIT sessions.
In the discharge session (19th session), the therapists and Miki reviewed and summarized the concepts and strategies/skills she had learned throughout the PCIT. She noted that through receiving PCIT, “I have realized that praising is important. But when I am overwhelmed, I cannot praise him” and “I have realized that it is important to praise him properly after issuing a command.” The therapists again recommended that she see a psychiatrist or other mental health professional for help because she still had clinically significant depressive symptoms (see Figure 3).
8 Complicating Factors
The one factor that complicated PCIT implementation was that Miki, the primary caregiver in PCIT, was too tired/distressed to focus on the treatment. She was a full-time working mother who was very busy with work, housework, and child-rearing, and had no help from others. So, she could not perform PCIT homework and attend sessions on a regular basis, making it difficult to implement/practice acquired PCIT skills in daily life. Especially, when she was terribly busy, it seemed that Miki’s acting out toward Akira (e.g., yelling, hitting) led to Akira’s problematic behavior (e.g., got in fights with his classmates).
9 Access and Barriers to Care
Japan utilizes a universal health care system and patients usually pay 10% to 30% of their total medical fees according to patients’ age and socioeconomic status. PCIT was not covered by the national health insurance, but Miki and Akira received PCIT free of charge because the treatment provided at the LifeCWC center was funded by a research grant. They also had reliable transportation to the center, which was within a reasonable distance from their home. However, they were sometimes unable to attend weekly PCIT sessions because Miki could not organize her work and/or housework. No other access issues or barriers to care were identified.
10 Follow-Up
A follow-up session/assessment with Miki was conducted 2 months post-PCIT. Miki’s ECBI-Intensity/Problems scores remained relatively stable, but the BDI-II score was increased to a severe level (see Figures 2 and 3). Miki told the therapists that she had been as busy and stressed as ever, and sometimes got in fights with her husband because he never helped with housework or child care even when she was having difficulty. Akira sometimes took impulsive action toward other children at nursery school, but was currently able to enter and attend elementary school. After this follow-up session, Miki was referred back to her workplace and followed up by an industrial nurse (Certificated Nurse Specialist).
11 Treatment Implications of the Case
In addition to the previous PCIT case study conducted in Japan (Hosogane et al., 2018), this article gives a more detailed description of how PCIT developed in Western cultures can be used for Japanese families who have children with behavioral problems. In the present case, the mother successfully acquired PCIT (CDI/PDI) skills in the early stages of the CDI and PDI coach sessions, and the child’s problematic behavior was also immediately reduced (although somewhat sporadically—when the mother was not so busy). However, from a cultural perspective, this case also emphasizes the need for supporting busy working mothers involved in PCIT because this is a common situation in Japan.
Japan’s gender gap is by far the largest among all advanced countries (Japan ranks 121st out of all 153 countries on the Global Gender Gap Index 2020; World Economic Forum, 2020). In Japan, the employment rate of women with children below 18 years has been rising steadily during the 2000s (53.1% in 2000 to 72.2 in 2018), and currently, 23.9% of all households are dual-earner families (Japanese Ministry of Health, Labor and Welfare, n.d.). However, among dual-income households with children below 6 years, almost 70% of fathers do not participate in housework or child care (Statistics Bureau, Japanese Ministry of Internal Affairs and Communications, 2017). In the present case, Miki’s husband was a typical example, in that, he was rarely involved in domestic work, so Miki had to do all of it in addition to her full-time work.
Her husband also did not actively participate in PCIT; the father’s absence in the session room was also seen in the two Japanese cases that appeared in the previous case study (Hosogane et al., 2018). Among East Asian countries, Chinese fathers are also generally reluctant to attend parent education programs (Leung et al., 2009). However, several studies have demonstrated that the father’s involvement enhances treatment outcome, so all family members/caregivers are encouraged to participate in PCIT (Bagner, 2013). Interestingly, in most PCIT case studies from the United States, fathers were actively involved in treatment both inside and outside of the session room (e.g., Armstrong et al., 2014, 2015; Cooper-Vince et al., 2016; Gordon & Cooper, 2016; Parlade et al., 2020).
It will take some time for Japanese society to overcome these hurdles facing Japanese families, but the government has taken several measures to support Japanese working mothers, especially since the 2010s (e.g., increasing the number of day care facilities, encouraging Japan’s business associations to increase the hiring, promotion, and empowering of women among member firms; Alkubati, 2019; Holloway & Nagase, 2014). In line with such changes, contemporary Japanese fathers may have become more involved in child-rearing in recent years, but they are still less likely than men in other countries to have a strong interest in parenting (Holloway & Nagase, 2014). Thus, in this case presentation, it seemed that Miki needed to seek help from her husband in an effective way to balance her work and family life. For example, the therapists could have set a patient-only session to teach assertive communication skills so that she would be able to ask her husband to perform more of the housework/child care duties (Speed et al., 2018; Yoshinaga et al., 2018). If Miki has an excessive fear of negative evaluation/rejection from her husband or sticks to the idealized traditional role of Japanese mothers (e.g., ryosai kenbo [good wife, good mother], mothers are expected to take full responsibility for taking care of family matters), a thought challenging record and/or behavioral experiment (one of the cognitive restructuring techniques of cognitive behavioral therapy) can be applied to modify her dysfunctional beliefs before implementing her assertive skills with her husband (Nakagawa et al., 2017; Yoshinaga et al., 2013, 2019).
12 Recommendations to Clinicians and Students
This case study supports the potential effectiveness of Western-originated PCIT for Japanese families who have children with behavioral problems, and also argues that there is a need for PCIT therapists to carefully assess and address the primary caregiver’s distractions outside the session room especially when working with Japanese working mothers.
As discussed earlier, contemporary Japanese mothers tend to take full responsibility for taking care of family matters even if they are working full time. Such cultural models are, of course, not necessarily applicable to all individuals in a community, but in the case of Japan, there may be more homogeneity than in most countries, due to the fact that Japan has a long island country history behind it, has sharply restricted immigration, and does not have the racial and ethnic diversity of the United States or Western Europe (Holloway & Nagase, 2014). In this case study, the series of treatments largely adhered to the Japanese version of the PCIT manual, without major modifications to the original protocol. However, to best fit the needs of the Japanese family, flexible adaptations/modifications of manualized PCIT are required, such as modifying session structure (e.g., order/length of sessions), content (e.g., additional individual support for parents), and delivery methods (e.g., more live coaching/feedback, in-home sessions).
Although PCIT is an evidence-based and widely used treatment, it has often been modified from its original protocol in both content and context because of cultural concerns, equity of access to intervention, and/or expectations that specific populations require modifications to PCIT (e.g., Carpenter et al., 2014; Leung et al., 2009; McCabe et al., 2012). However, it is still unknown whether these modifications affect PCIT outcomes; thus, further experimental studies and/or meta-analyses that directly compare clinical effectiveness between modified and unmodified PCIT are required.
Footnotes
Acknowledgements
The authors would like to express their gratitude to Dr. Toshiko Kamo for supervising the treatment as the PCIT International Certificated Master Trainer; Prof. Miyoko Nagae for representing, managing, and running the Caring Life of Women and Children Research Group (LifeCWC); and Mr. Richard White for checking and editing the English language.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Grant-in-Aid for Scientific Research (KAKENHI) (B) from the Japan Society for the Promotion of Science (JSPS), Grant Number 16H05611.