
Abstract
Religiosity and spirituality (R/S) encompass organizational activity, private practice, and intrinsic beliefs, which may relate differently to cognitive and mental health outcomes in older adults. This study identified latent R/S profiles among South Korean older adults with mild cognitive impairment (MCI) and Alzheimer’s disease (AD), and examined differences in cognitive function, psychological well-being, and depressive symptoms. Latent profile analysis using Duke University Religion Index indicators was conducted with 518 patients (MCI: n = 224; AD: n = 294). In MCI, three classes that differed in well-being and verbal fluency were identified; they showed no differences in depressive symptoms or other cognitive domains. In AD, four classes were identified that differed in the Short Blessed Test and Word List Recall; in these, well-being, depression, and other cognitive outcomes did not differ across classes. These findings underscore the relevance of diverse R/S patterns in individualized care for older adults with neurocognitive disorders.
Keywords
Distinct religiosity and spirituality (R/S) profiles were identified among South Korean older adults with mild cognitive impairment and Alzheimer’s disease. These profiles showed significant differences in cognitive function and well-being, indicating the need for individualized approaches to religious and spiritual engagement. The findings may contribute to the development of culturally sensitive and diverse R/S supports to improve well-being in patients with neurocognitive disorders.Significance Statement
Introduction
Alzheimer’s disease (AD) is the most common cause of dementia. It affects various cognitive domains, including thinking, memory, independence, learning, speech, language comprehension, and communication. 1 Mild cognitive impairment (MCI), another common neurodegenerative condition in older adults, is characterized by memory impairments and deficits in other cognitive domains (DSM-5, 2013 & ICD-10, 1993).2,3 Older adults with dementia often experience neuropsychiatric symptoms such as depression, anxiety, psychotic symptoms, and apathy, as well as impairments in language (aphasia), motor function (apraxia), and recognition (agnosia). 4 These symptoms result in a global deterioration in thinking and adaptability, disrupting daily social life and relationships. As the older adult population continues to grow globally, identifying psychosocial factors associated with cognitive and emotional well-being in older adults with neurocognitive disorders has become a major public health priority. 5
Among the psychosocial factors that support well-being in older adults with neurocognitive disorders, religiosity and spirituality (R/S) have attracted increasing attention. Many older adults report frequent worship attendance, daily prayer, and strong religious affiliation. 6 Previous research shows that R/S involvement is associated with better self-rated cognitive health and enhanced working memory. 7 Additionally, a growing body of research suggests that R/S may influence cognitive and mental health outcomes via psychosocial pathways such as emotional regulation, meaning-making, and supportive social engagement.8,9 These findings support that R/S is not a singular construct, but rather a multidimensional construct that consists of belief, practice, and engagement; therefore, it may relate differently to individuals’ psychological experiences.
Despite these findings, research on R/S in people with neurocognitive disorders remains limited in several important respects. Existing studies demonstrate heterogeneity across racial, ethnic, gender, and R/S dimensions (eg, organizational, non-organizational, and intrinsic religiosity), yet it remains unclear whether similar variation exists between individuals with MCI and those with AD.10-12 An integrative review of R/S measurement in people with dementia reported that many studies rely on heterogeneous or non-validated instruments, conceptualize R/S as a unidimensional construct, or fail to distinguish levels of cognitive impairment in their analysis. 13 These limitations restrict these studies’ ability to determine which aspects of R/S may be most clinically relevant for individuals at different stages of neurocognitive decline. Furthermore, variable-centered approaches that treat R/S as a single continuous variable do not adequately capture the diversity of individuals’ religious practices and overlook potential subgroup differences in how R/S relates to neurocognitive outcomes.14,15 A more refined analytical framework is necessary to accommodate the multidimensional nature of R/S and the distinct patterns by which individuals engage in it.
A person-centered analytic approach, such as latent profile analysis (LPA), provides a way to identify within-person patterns or latent profiles, 16 offering a more nuanced understanding of the interactions among cognitive, emotional, and existential dimensions. The identified profiles may help determine whether individuals rely more heavily on structured religious participation or on intrinsic belief systems. These profiles may also assist in clarifying whether particular patterns of R/S involvement are associated with differences in current cognitive functioning, fewer neuropsychiatric symptoms, or more favorable psychological outcomes. Lastly, they may also indicate how R/S engagement complements or enhances existing psychosocial and behavioral interventions.
Accordingly, the present study aims to identify distinct profiles of R/S engagement among individuals with MCI or AD using LPA, and to examine whether these profiles are associated with differences in cognitive functioning and mental health outcomes within each diagnostic group. In doing so, this study seeks to provide clinically meaningful insights into the role of R/S in neurocognitive disorders among older adults and establish a foundation for incorporating R/S-informed strategies into dementia care.
Methods
Study Design
This study used cross-sectional data derived from each of the participants’ first outpatient visit. Only the patient’s initial neuropsychological evaluation and R/S assessment were included; there were no repeated or longitudinal measurements. All data were obtained from the evaluations conducted between January 2015 and December 2020 at the Department of Psychiatry, Hallym University Chuncheon Sacred Heart Hospital, Chuncheon City, Gangwon-do, South Korea.
Participants
Participants were older adults aged 60-95 years who presented to the hospital’s outpatient psychiatric clinic between January 2015 and December 2020. A total of 518 individuals who met the inclusion criteria for MCI or AD were included in the final analysis. Diagnostic criteria for MCI were based on common clinical standards and included: (a) subjective complaints of memory decline; (b) no diagnosis of dementia; (c) preserved ability to perform activities of daily living with no significant functional impairment attributable to cognitive deficits; and (d) objective evidence of cognitive impairment, as measured by standardized neuropsychological tests. Participants in the MCI group were required to have a Clinical Dementia Rating (CDR) score of 0.5 or lower and a Global Deterioration Scale (GDS) score of 4 or lower. Diagnosis of AD was based on the criteria of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), requiring progressive cognitive decline affecting at least two cognitive domains. Participants in the AD group were required to have a CDR score of 1.0 or lower and a GDS score of 5 or lower.
Measures
R/S were assessed using the Duke University Religion Index (DUREL), a brief multidimensional instrument developed for use in psychiatric and epidemiological research. 17 It comprises five items measuring three core dimensions: (1) ORA or involvement in public religious activities such as attending religious services (Item 1); (2) NORA or private religious practices such as prayer or meditation (Item 2); and (3) IR or internalized religious commitment and motivation (Items 3 to 5).
The ORA and NORA subscales were refined in collaboration with the National Institutes of Health, 18 whereas the IR subscale incorporates three of the ten items from Hoge’s Intrinsic Religious Motivation Scale. 19 Total scores on the DUREL range from 5 to 27. 20 In its original scoring format, lower scores indicate higher levels of R/S. However, in the present study, reverse scoring was applied for interpretability, with higher scores indicating higher R/S. The internal consistency of DUREL in this study was excellent (Cronbach’s α = 0.94).
Well-being was assessed using the World Health Organization-Five Well-Being Index (WHO-5), a brief, self-administered measure of current mental well-being that has demonstrated adequate validity for screening depression and evaluating outcomes in both clinical and research settings. Item response theory analyses conducted across both younger and older populations have supported its construct validity as a unidimensional measure of psychological well-being. 21
Participants were asked to rate their feelings over the past two weeks in response to five statements: “I feel cheerful and in good spirits,” “I feel calm and relaxed,” “I feel active and vigorous,” “I wake up feeling fresh and rested,” and “My daily life is filled with things that interest me.” Each statement was rated on a 6-point Likert scale, with higher scores indicating better mental well-being. In the Korean validation study, the WHO-5 demonstrated good internal consistency (Cronbach’s α = 0.83). 22
Cognitive function was assessed using the Korean version of the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD-K), which evaluates multiple cognitive domains, including language, memory, visuospatial ability, and attention. Individual test scores of each domain were aggregated to generate composite scores reflecting performance in the corresponding cognitive area.
Language functions were assessed using the Verbal Fluency Test—which requires participants to generate as many words as possible within a specific category in one minute—and the Boston Naming Test—which evaluates participants’ ability to name visually presented objects. These two scores were combined to form a composite language score.
Memory was assessed using the Word List Memory Test and the Word List Recall Test. The former assesses participants’ immediate recall of a list of previously presented words, while the latter assesses their delayed recall. A composite memory score was calculated by combining results from both tests.
Visuospatial function was measured using the Constructional Praxis Test—where participants replicate a geometric figure—and the Constructional Recall Test—which assesses delayed reproduction of the same figure. Attention was assessed using the Word List Recognition Test, in which participants identify previously presented words from a list of distractors.
Additionally, the Korean version of Short Blessed Test (SBT-K), included as a supplementary component of the CERAD-K battery, was used to evaluate global cognitive function. The SBT is a condensed version of the cognitive subscale of the original Blessed Dementia Scale, 23 later refined to six items assessing orientation, memory, and concentration. 24 Errors are scored for each item, yielding a total score ranging from 0 to 28, with higher scores indicating greater cognitive impairment. The SBT has been reported to be both time-efficient (typically completed in under five minutes) and psychometrically robust, with good reliability, sensitivity, and specificity. 25
Depressive symptoms were assessed using the Korean version of the Short Geriatric Depression Scale (SGDS-K), a 15-item abbreviated form of the original 30-item Geriatric Depression Scale (GDS) initially developed by Yesavage. 26 The SGDS-K has been culturally and linguistically validated for use among Korean older adults, demonstrating strong internal consistency and construct validity. A validation study involving community-dwelling Korean elders revealed an optimal cut-off score of 8 to screen major depressive disorder (MDD) (sensitivity = 0.94, specificity = 0.76) and 6 to detect both MDD and minor depressive disorder (MDD) (sensitivity = 0.79, specificity = 0.66). 27 The SGDS-K was also found to be effective for detecting depression in older adults with cognitive impairment.
Data Analysis
Descriptive statistics were conducted to examine demographic characteristics, and correlation analyses were used to assess relationships among key variables. Both analyses were performed using SPSS version 29.
LPA—a model-based clustering technique for analyzing continuous observed variables—was performed using Mplus. Unlike traditional clustering methods (eg, hierarchical, or K-means clustering), which do not provide formal statistical indices to determine the number of clusters, LPA offers model fit indicators such as the Akaike Information Criterion (AIC) and the Bayesian Information Criterion (BIC).
Determining the optimal number of classes remains one of the most challenging aspects of cluster analysis, as no universally accepted criterion or theoretical framework exists for doing so. Therefore, researchers typically consider multiple factors, including statistical fit indices, profile interpretability, class size, and theoretical or clinical relevance when selecting the final model. 28 In this study, the number of latent profiles was determined based on AIC and BIC results, along with considerations of interpretability and substantive significance.
Following class identification, one-way analyses of variance (ANOVAs) were conducted to examine whether statistically significant differences existed among the latent profiles in cognitive function (SBT-K and CERAD-K domains), well-being (WHO-5), and depressive symptoms (SGDS-K). For variables showing significant differences, post hoc comparisons were performed using the Scheffé test.
Results
Demographic and Clinical Characteristics of the MCI and AD Groups
Demographic and Clinical Characteristics of Participants
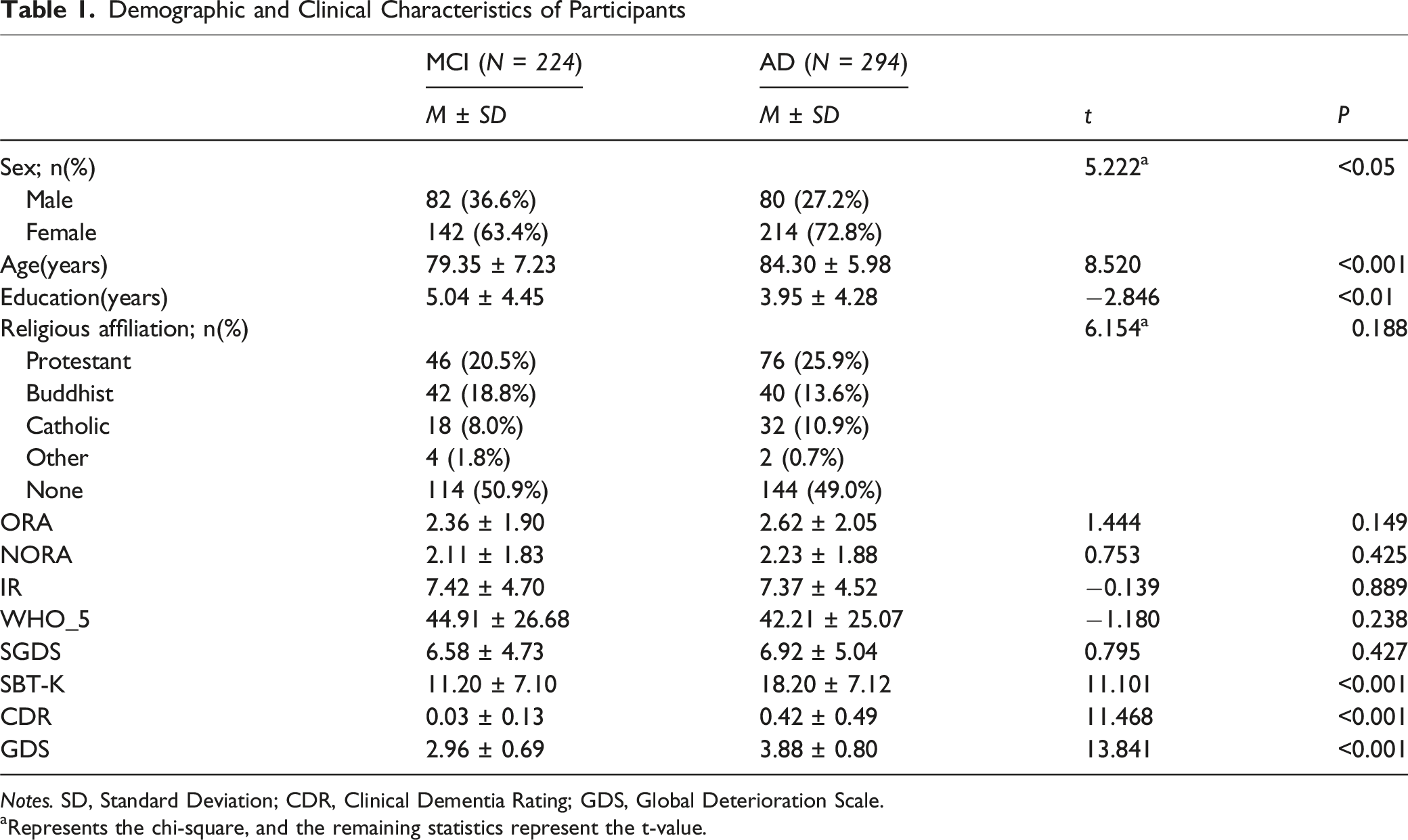
Notes. SD, Standard Deviation; CDR, Clinical Dementia Rating; GDS, Global Deterioration Scale.
aRepresents the chi-square, and the remaining statistics represent the t-value.
Preliminary Correlation Assessment
Correlation Among the Main Variables in MCI (N = 224)
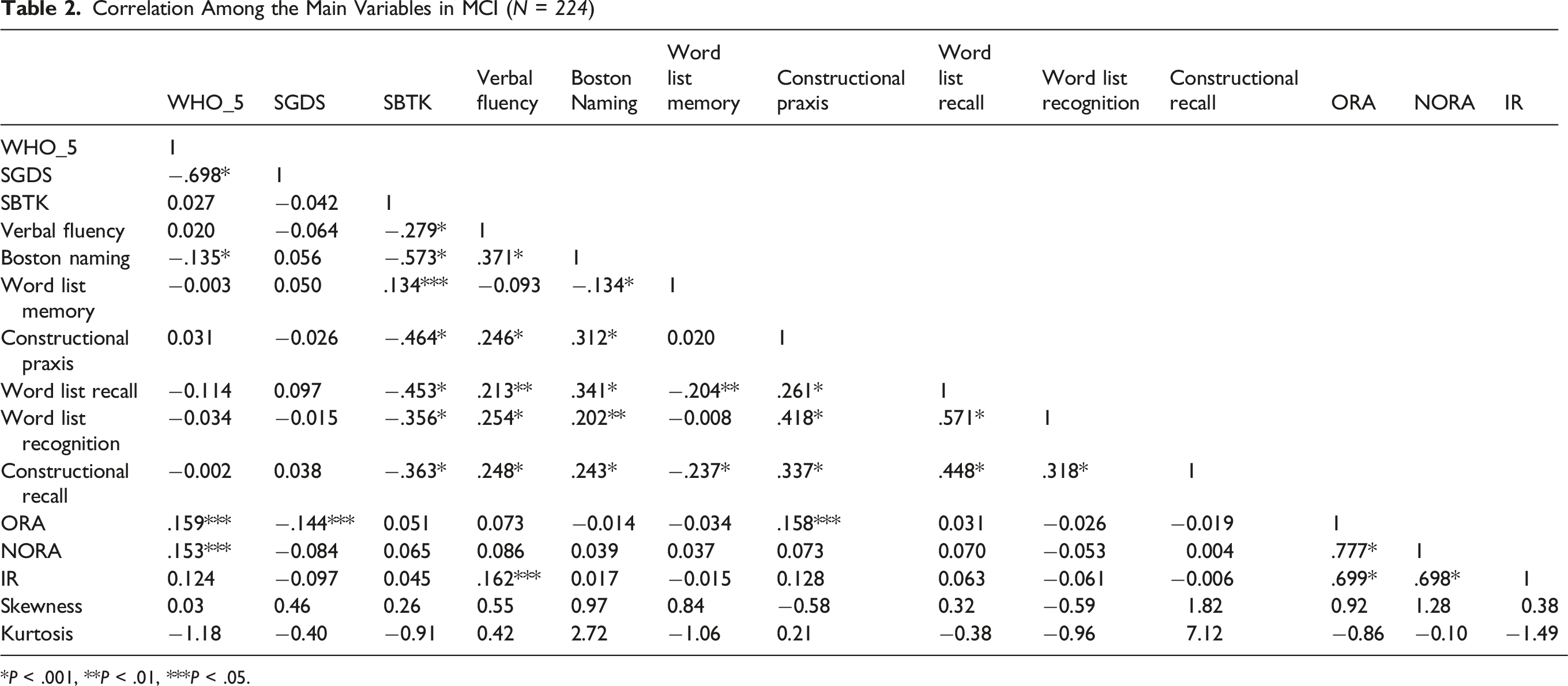
*P < .001, **P < .01, ***P < .05.
Correlation Among the Main Variables in AD (N = 294)
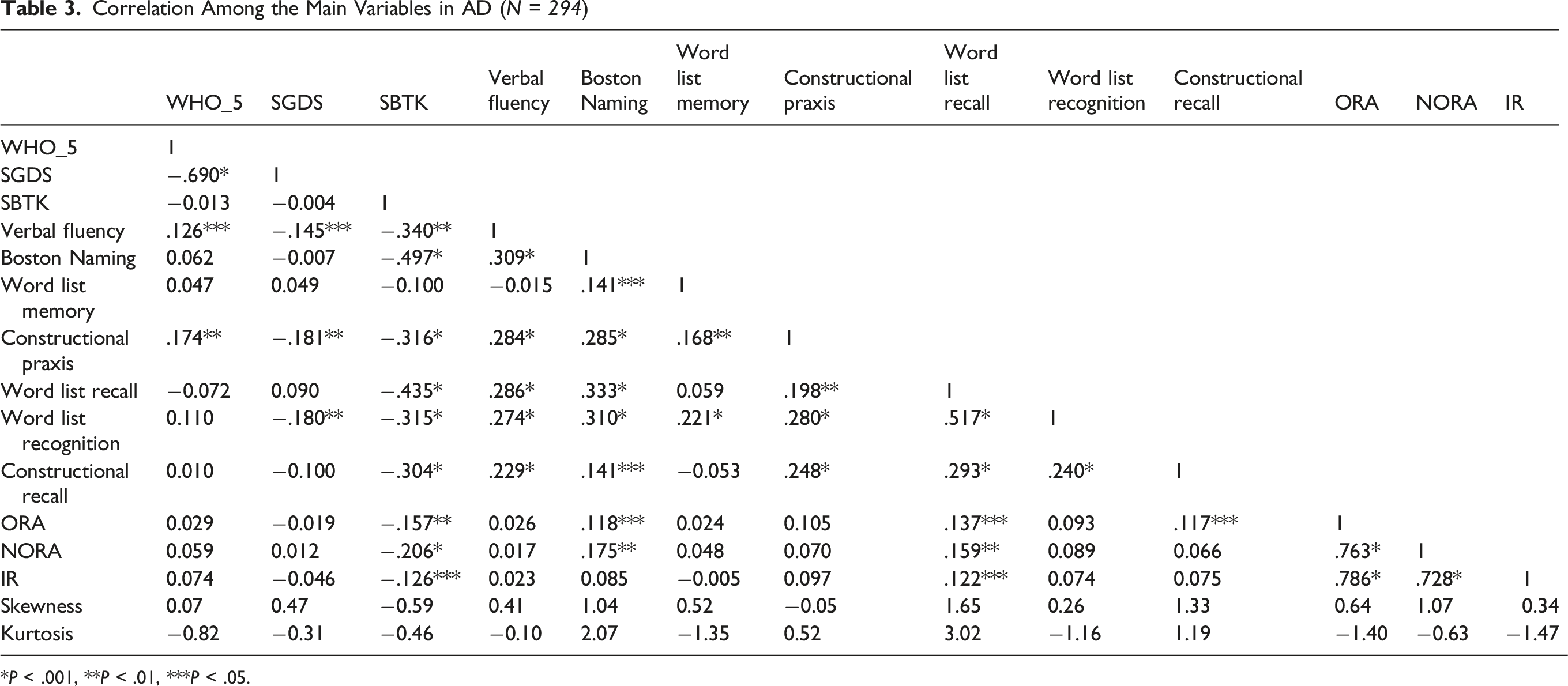
*P < .001, **P < .01, ***P < .05.
In the MCI group (Table 2), significant positive correlations were observed between ORA and both Constructional Praxis (r = 0.158, P = 0.018) and WHO-5 (r = 0.159, P = 0.017). While ORA was negatively associated with SGDS (r = –0.144, P = 0.031), NORA demonstrated a significant positive correlation with WHO-5 (r = 0.153, P = 0.022). IR was significantly positively correlated with verbal fluency (r = 0.162, P = 0.015). No significant correlations were observed between R/S variables and the SBT-K, Boston Naming Test, or memory-related variables such as Word List Memory and Word List Recall.
In the AD group (Table 3), ORA was positively correlated with the Boston Naming Test (r = 0.118, P = .043), Word List Recall (r = 0.137, P = .018), and Constructional Recall (r = 0.117, P = .045). NORA was positively correlated with the Boston Naming Test (r = 0.175, P = .003) and Word List Recall (r = 0.159, P = .006). IR showed a significant positive correlation with Word List Recall (r = 0.122, P = .037). In contrast, the SBT-K was negatively associated with all three R/S variables: ORA (r = –0.157, P = .007), NORA (r = -0.206, P < .001), and IR (r = -0.126, P = .031). No significant correlations were observed between the R/S variables and other cognitive or affective measures, including the WHO-5, SGDS, Verbal Fluency Test, Word List Memory, Word List Recognition, and Constructional Praxis.
Latent Profile Analysis Using Religiosity and Spirituality Indicator
Comparing Model Fit of Latent Class Models in MCI (N = 224)
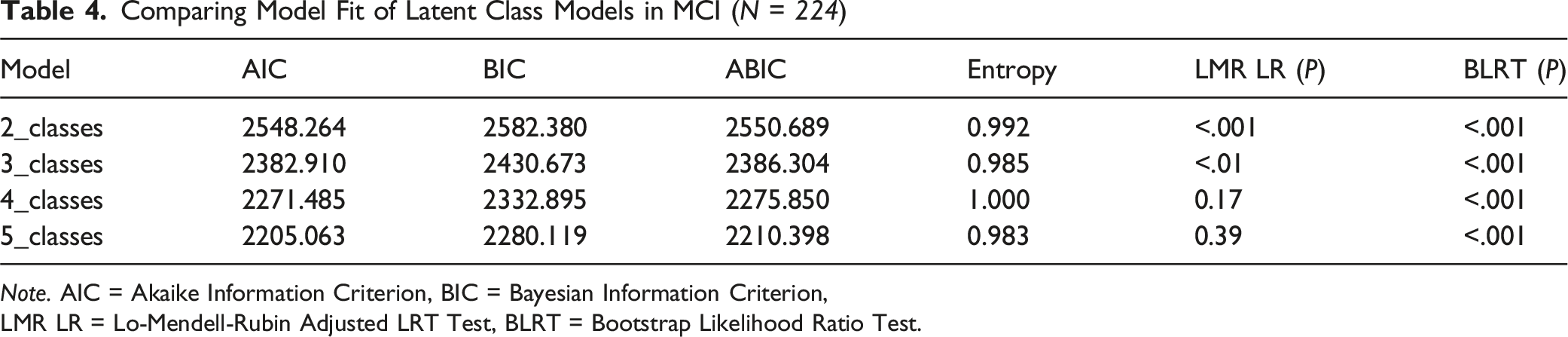
Note. AIC = Akaike Information Criterion, BIC = Bayesian Information Criterion,
LMR LR = Lo-Mendell-Rubin Adjusted LRT Test, BLRT = Bootstrap Likelihood Ratio Test.
Comparing Model Fit of Latent Class Models in AD (N = 294)
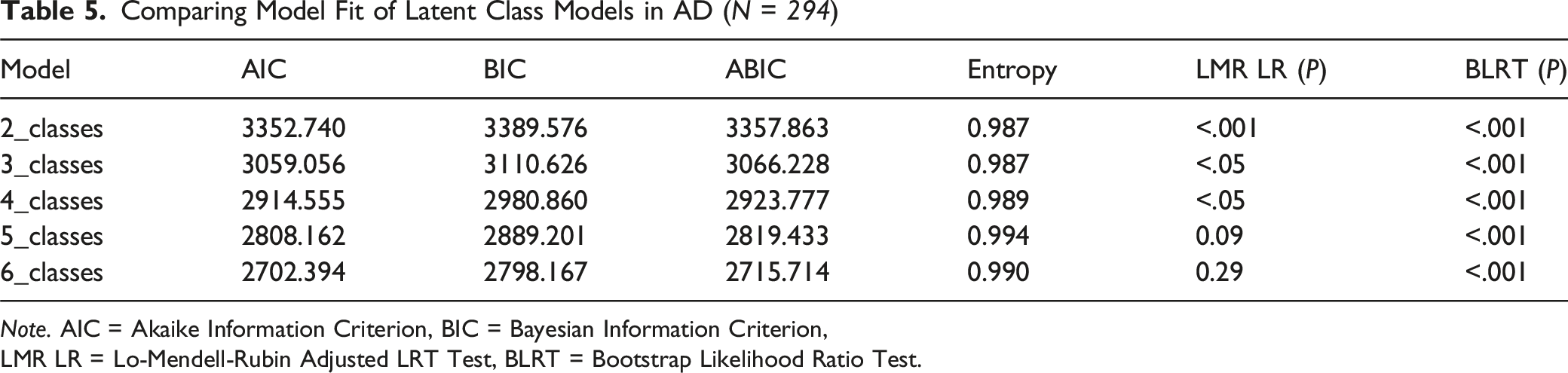
Note. AIC = Akaike Information Criterion, BIC = Bayesian Information Criterion,
LMR LR = Lo-Mendell-Rubin Adjusted LRT Test, BLRT = Bootstrap Likelihood Ratio Test.
Estimated Means and Proportions for Each Latent Class in MCI (N = 224)

Note. ( ) values represent the number of class members.
Estimated Means and Proportions for Each Latent Class in AD (N = 294)
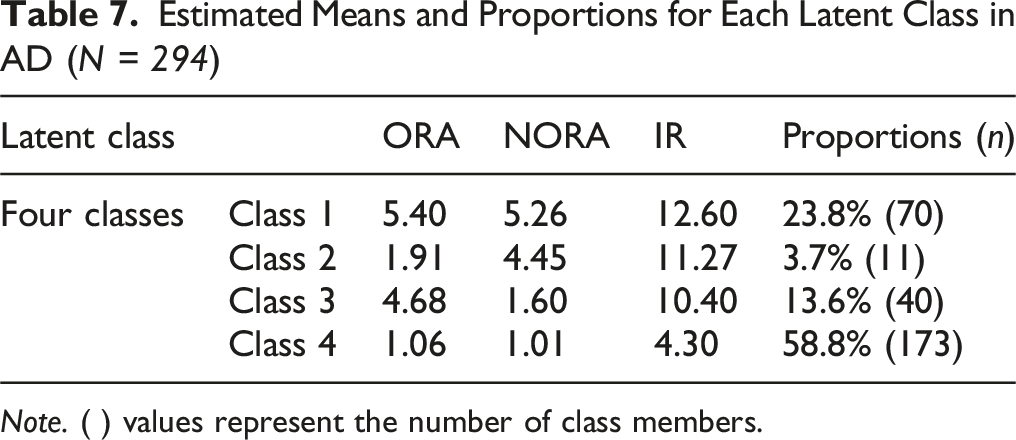
Note. ( ) values represent the number of class members.
The LPA of R/S characteristics in patients with MCI identified three distinct latent classes (Table 6). Class 1 demonstrated mean scores of 4.98 for ORA, 5.25 for NORA, and 13.27 for IR. This group accounted for 23.2% (n = 52) of the total sample and was characterized by high levels of ORA and NORA, along with strong IR. Accordingly, this class was labeled the “Highly Religious Group.” Class 2 exhibited lower scores for ORA (2.32) and NORA (1.32) but a relatively high IR score (10.71). Representing 25.0% (n = 56) of the sample, this group was distinguished by low levels of religious activity but high IR and was thus labeled the “High Intrinsic Religiosity Group.” Class 3, the largest subgroup comprising 51.8% (n = 116) of the sample, exhibited low scores across all dimensions: ORA (1.21), NORA (1.08), and IR (3.22). This group, characterized by minimal religious participation and weak IR, was accordingly labeled the “Low Religious Engagement Group.”
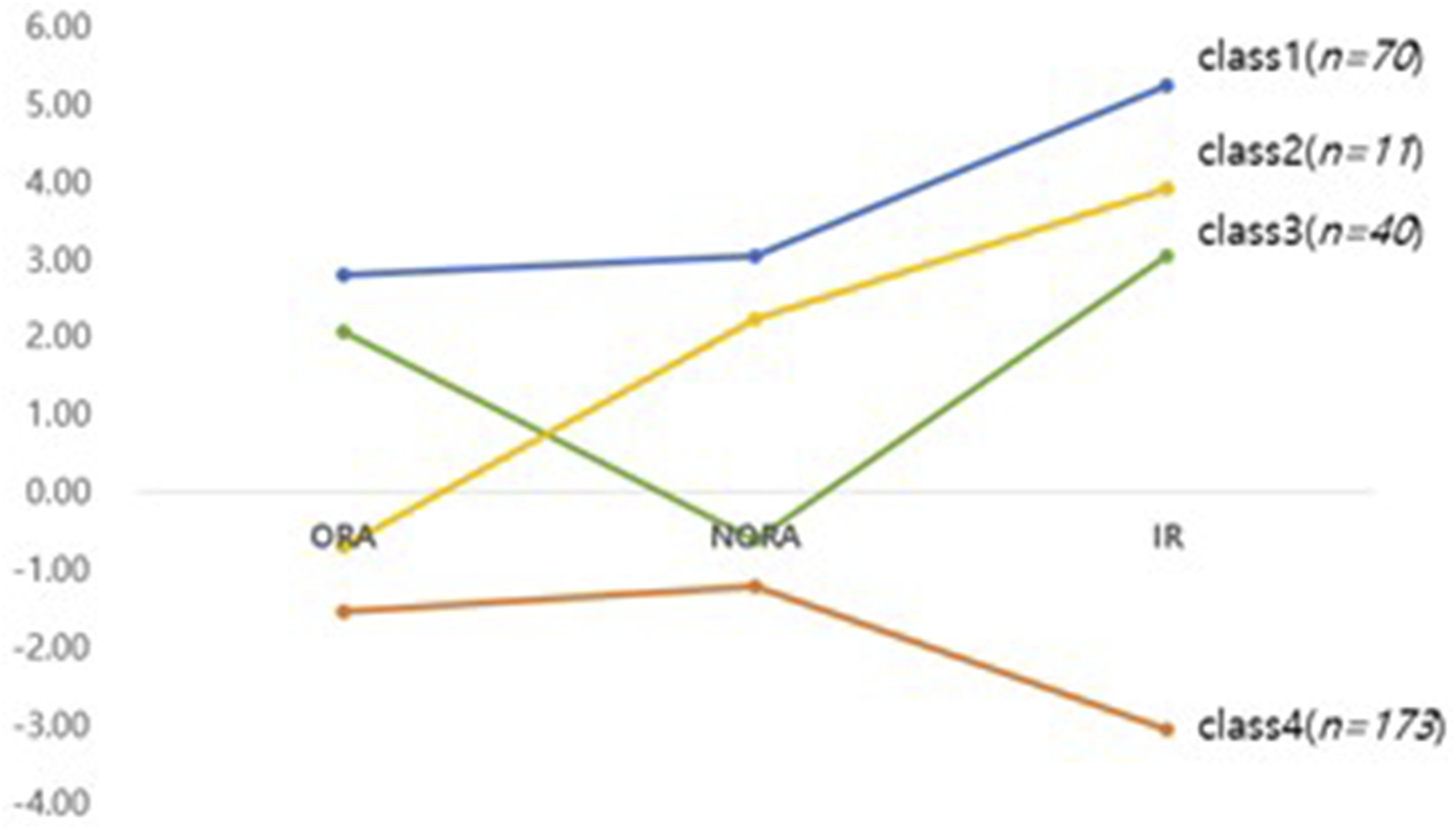
Four distinct latent classes emerged from the analysis of R/S characteristics in the AD group (Table 7). Class 1 comprised 23.8% of the total sample (n = 70) and demonstrated the highest scores across all dimensions, with an ORA score of 5.40, NORA score of 5.26, and IR score of 12.60. This group was characterized by strong engagement in both public and private religious practices, with high IR. Accordingly, this class was labeled the “Highly Religious Group.” Class 2 represented the smallest proportion of the sample (3.7%, n = 11) and had a low ORA score (1.91) but relatively high NORA (4.45) and IR (11.27) scores. This group was characterized by minimal participation in ORA but high levels of NORA and IR. Therefore, it was labeled the “Non-Organized Religious Group.” Class 3 exhibited high ORA (4.68) and IR (10.40) but low NORA (1.60) score. This group accounted for 13.6% of the sample (n = 40) and was characterized by strong engagement in ORA and high IR, with limited involvement of NORA. It was thus labeled the “Organized Religious Group.” Class 4, comprising the largest segment of the sample (58.8%, n = 173), exhibited the lowest scores across all three R/S dimensions: ORA (1.06), NORA (1.01), and IR (4.30). This group was accordingly labeled the “Low Religious Engagement Group.”
Figures 1 and 2 provides a visual representation of the characteristics of each latent class in both AD and MCI patients, using centered scores from the mean (ie, raw score minus group mean) of R/S indicators (ORA, NORA, IR), rather than raw scores, to facilitate clearer comparison and interpretation. Latent profiles of ORA, NORA, IR in MCI patients Latent profiles of ORA, NORA, IR in AD patients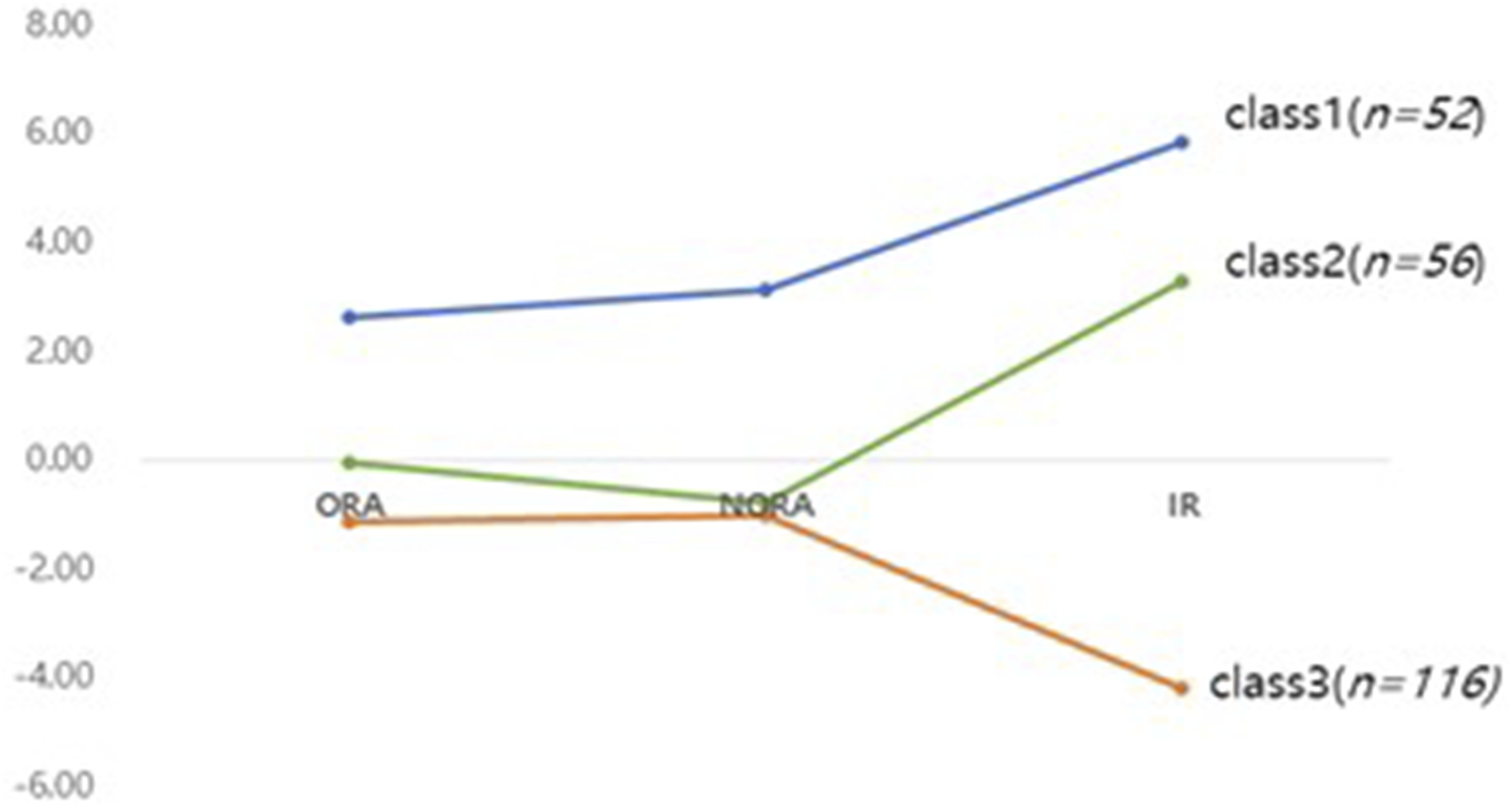
Differences in Cognitive Function, Well-Being, and Depressive Symptoms Across Latent Profile Types
Differences in Variables Across the Three Latent Classes in the MCI Group (N = 224)
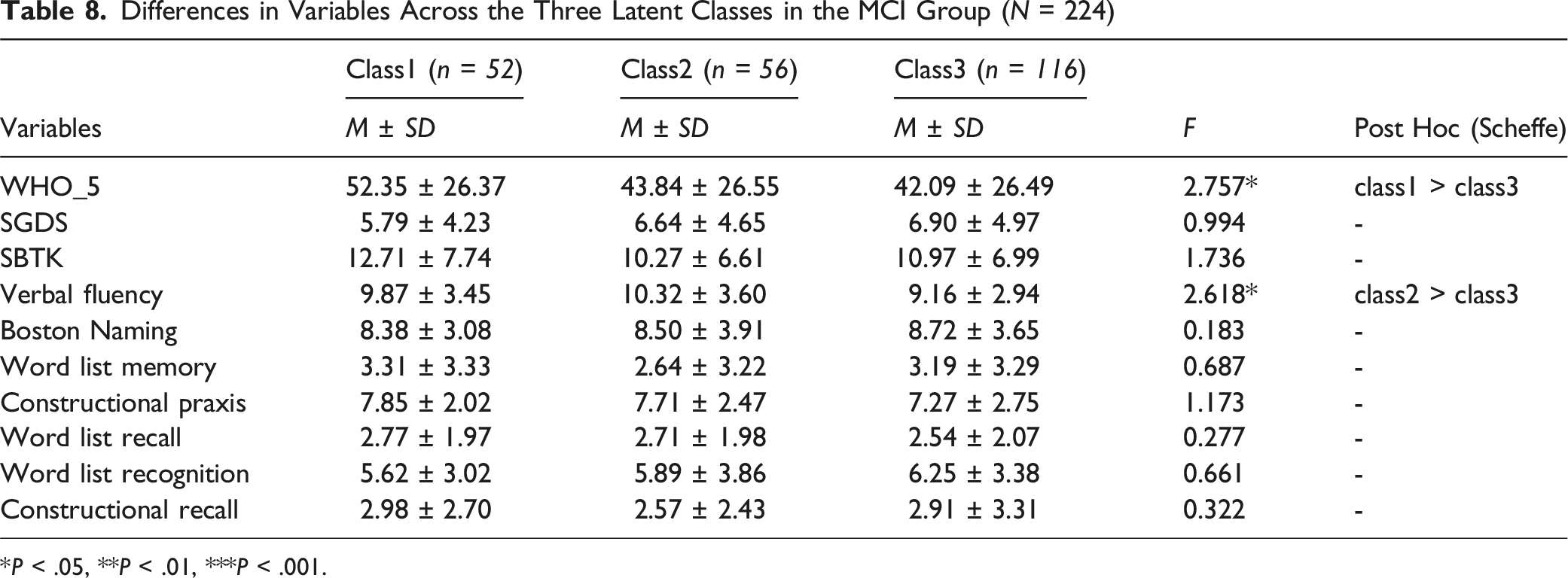
*P < .05, **P < .01, ***P < .001.
Differences in Variables Across the Three Latent Classes in the AD Group (N = 294)
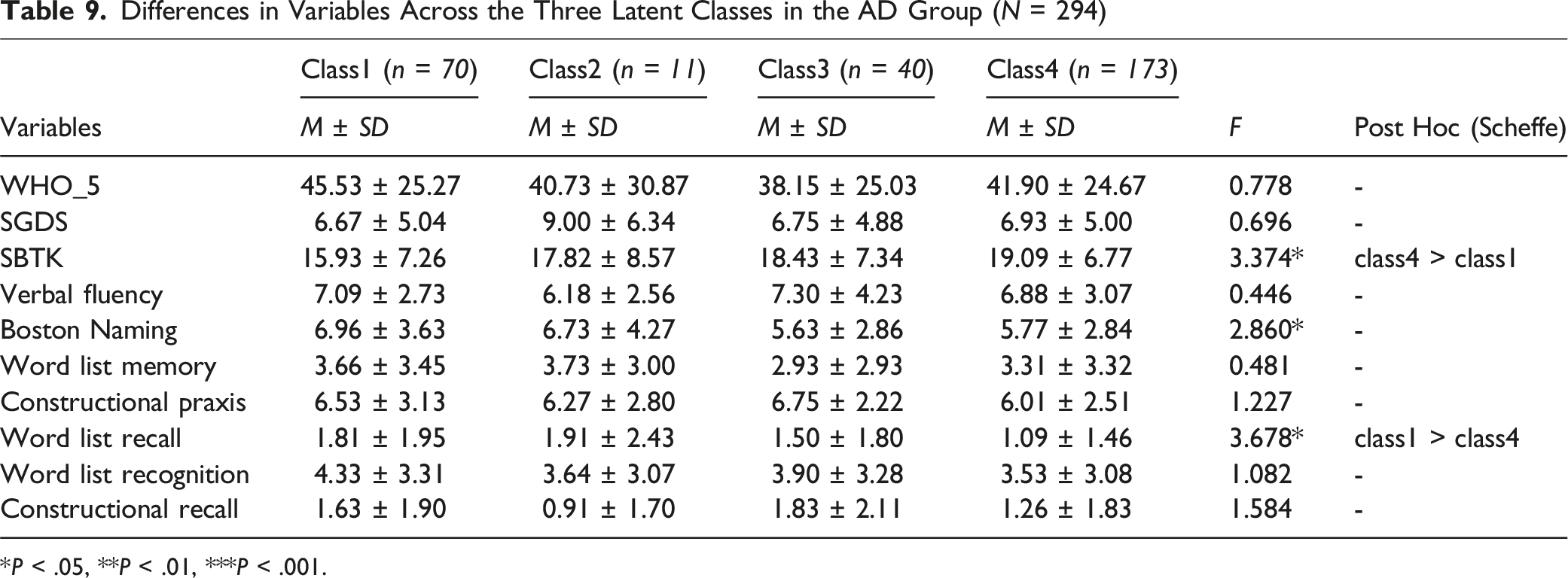
*P < .05, **P < .01, ***P < .001.
Discussion
This study not only identified latent profile types based on the R/S characteristics of patients with MCI and AD but also examined differences in cognitive function, depressive symptoms, and well-being across these profiles. The results revealed that both the MCI and AD patient groups were classified into distinct profiles reflecting the multidimensional nature of R/S. Each profile type demonstrated significant differences in well-being and specific domains of cognitive functioning, but not in depressive symptoms. Importantly, the pattern and nature of these differences varied between the two groups, suggesting that the influence of R/S manifests differently depending on the stage of cognitive impairment.
In the LPA results, three distinct latent classes based on the characteristics of R/S were identified in MCI group: the Highly Religious Group, the High Intrinsic Religiosity Group, and the Low Religious Engagement Group. Notably, the High Intrinsic Religiosity Group was not observed in the AD group. This class accounted for 25.0% of the total sample (n = 56). The R/S profile was characterized by low levels of ORA and NORA but high levels of IR, showing that some individuals with MCI maintain a strong inner belief system despite limited participation in formal or personal religious practices. This pattern also suggests that individuals with MCI, who generally retain greater cognitive capacity, may be better able to seek psychological stability and a sense of meaning in life through IR. Moreover, these findings align with the perspectives that even in the absence of religious affiliation or activity, individuals may find meaning and purpose in life from personal beliefs and values, as well as reflective practices such as meditation, communion with nature, artistic expression, and psychological reflection. 29
Two R/S profiles emerged that seemed to have factors in common across both the MCI and AD groups: the Highly Religious Group and the Low Religious Engagement Group. The Highly Religious Group was characterized by uniformly high levels across all three dimensions of R/S: ORA, NORA, and IR. Individuals in this group actively participate in organized religious practices such as worship services, church-related activities, and religious gatherings, and they frequently engage in personal religious practices, including prayer, scripture reading, and private meditation. IR, reflecting the extent to which religious beliefs are internalized and integrated into one’s daily life and personal values, is also very high among members of this group. The Low Religious Engagement Group, which constitutes more than half of the sample (MCI: 51.8%, AD: 58.8%), is characterized by low ORA and NORA scores as well as the lowest level of IR. This group likely includes individuals with little to no religious affiliation or participation, suggesting that the influence of R/S on cognitive function and mental health may be minimal for these individuals. As such, it provides an important comparison point for examining the impact of R/S engagement on cognitive preservation and psychological well-being.
An analysis of differences in cognitive function, well-being, and depressive symptoms across the three latent classes identified among MCI patients revealed significant group differences, particularly in WHO-5 and verbal fluency scores. The WHO-5 scores showed that the Highly Religious Group reported a significantly higher level of well-being than the Low Religious Engagement Group. The findings of this study suggest that the Highly Religious Group, which reported higher well-being scores, may benefit more from R/S through enhanced psychological stability and positive emotional states. Given the challenges MCI patients face in daily functioning owing to cognitive decline, R/S engagement may serve as a key source of emotional support and psychological stability, strengthening social networks, reducing stress and anxiety, and fostering a positive outlook on life, thereby enhancing overall well-being. 30 R/S involvement has also been associated with greater consistency, meaning, and hope, all of which may help individuals cope more effectively with the increasing stress associated with aging. 31
In addition to well-being, significant differences in verbal fluency scores were observed between the High Intrinsic Religiosity Group and the Low Religious Engagement Group (F = 2.618, P = 0.05). To better understand these differences, it should be noted that although both groups exhibited lower levels of ORA and NORA than did the Highly Religious Group, the High Intrinsic Religiosity Group demonstrated notably higher IR (M = 10.71 vs. M = 3.22). Given that MCI patients typically maintain the ability for introspective thought and verbal communication, those with stronger internal beliefs may be more likely to engage in frequent verbal activities such as self-reflection or reading, which could provide consistent cognitive stimulation, thereby supporting verbal fluency. Furthermore, prior studies have identified cognitive processing speed and inhibitory control as key predictors of verbal fluency in older adults. 32 These findings collectively suggest that high levels of IR may play a protective role in preserving verbal abilities by fostering active engagement in cognitively stimulating verbal practices.
While the MCI group showed three profiles, the LPA of the AD group revealed four distinct profiles. They were named the Highly Religious Group, the Non-Organized Religious Group, the Organized Religious Group, and the Low Religious Engagement Group. The patterns observed in these profiles reflect the differences in how patients with AD engage in R/S, despite functional decline. Across the Highly Religious Group, Non-Organized Religious Group, and Organized Religious Groups, a common feature was their relatively high level of IR.
Among these four profiles, the Non-Organized Religious Group showed particularly notable characteristics. Although this class represents the smallest proportion of the sample (3.7%, n = 11), individuals in this group have low levels of ORA but high levels of NORA and IR. This pattern suggests that patients with AD, who may face difficulties attending structured religious services, can continue to engage in personal religious practices such as prayer, hymn singing, and scripture reading, while maintaining a strong IR belief. Among various non-organizational religious practices, prayer is especially central, and private prayer encompasses a wide range of cognitive processes, including perception, language, emotion, self-concept, memory, decision-making, planning, and social cognition. 33 Individuals with dementia who engage more frequently in private prayer exhibit fewer neuropsychiatric symptoms and better cognitive performance. 34 Listening to religious music is also an important form of private R/S activity and can positively influence mental health and life satisfaction. 35
The Organized Religious Group (13.6%, n = 40) in AD group is characterized by high ORA and IR but notably low NORA, suggesting that some patients with AD maintain high levels of IR primarily through regular participation in structured religious practices. Prior studies have revealed that individuals in the early stages of Alzheimer’s often make proactive efforts to adapt to memory loss, cope with challenges, and preserve a sense of normalcy. These individuals tend to hold strong religious beliefs, engage regularly in religious activities, and experience a slower progression of disease symptoms, particularly in cognitive and behavioral domains, than do those with lower religious involvement.36-38
In the AD group, significant differences were observed in SBT-K and Word List Recall scores across latent profiles. The Highly Religious Group demonstrated better cognitive performance than the Low Religious Engagement Group in these domains. These findings suggest that religious involvement may play a meaningful role in specific aspects of cognitive functioning, particularly memory-related tasks, in AD patients. These findings are consistent with previous research which report higher levels of R/S involvement, including organizational attendance, private prayer, and intrinsic religiosity to be associated with better memory performance and slower cognitive decline in older adults.39,40 Individuals in the Highly Religious Group are likely to engage more frequently in repetitive cognitive activities such as prayer and religious study, which may function as informal memory training. Such religious rituals and practices may stimulate memory and contribute positively to recall ability, as evidenced by performance on Word List Recall tasks.
Among the factors that may explain the influence of R/S on cognitive function, neurological mechanisms likely play a role. R/S may affect cognitive functioning through specific neurobiological pathways involving brain regions such as the medial frontal cortex, orbitofrontal cortex, precuneus, and posterior cingulate cortex—areas associated with emotion regulation, self-referential processing, and cognitive conflict resolution. Functional neuroimaging studies have revealed that engagement in R/S practices, such as prayer and moral reasoning, activates distinct neural networks, potentially contributing to enhanced cognitive functioning and influencing behavioral outcomes related to mood, anxiety, and other psychiatric conditions. 41
In contrast, no significant differences were found across latent classes in terms of depression or well-being among patients with AD. These results indicate that although R/S appears to positively influence cognitive function and memory retention in AD patients, it may not exert a comparable effect on psychological indicators such as depression or overall well-being. These findings diverge from previous studies suggesting that R/S positively influences depression and well-being in older adults. 42 One possible explanation for this discrepancy relates to the challenges of accurately assessing psychological symptoms in individuals with AD. Because measures such as the WHO-5 and SGDS rely on self-reporting, their validity may be limited in populations who experience cognitive impairment. 13 Future studies may benefit from employing clinician-administered instruments that more reliably evaluate the psychological, social, and mental states of individuals with AD.
Because this study did not include a direct statistical comparison between patients with AD and those with MCI, definitive conclusions regarding differential effects of R/S between the two groups cannot be drawn. However, several noteworthy observations emerged from the latent profile analysis and subsequent analyses. Overall, while R/S was associated with both cognitive functioning and emotional well-being in individuals with MCI, its influence in the AD group appeared to be limited to cognitive domains. 13 This may be because MCI patients retain a greater degree of introspective and evaluative capacity compared to those with AD, allowing R/S to exert influence on cognitive functioning and emotional aspects such as subjective well-being. This suggests that the influence of R/S on cognitive and emotional functioning in older adults with neurocognitive disorders may be greater in the earlier stages of cognitive decline than in more advanced stages. It also implies that the impact of R/S on domains such as language, memory, and affect may vary depending on the severity of neurocognitive impairment.
Although higher levels of R/S involvement were associated with better performance in specific cognitive domains, such as verbal fluency in MCI patients and overall cognition or delayed recall in AD patients, the possibility of reverse causality cannot be entirely ruled out. Individuals with relatively preserved cognitive function may be more capable of participating in R/S activities, particularly those requiring organization or verbal interaction. Nonetheless, the lack of consistent differences across all cognitive domains suggests that R/S engagement may not merely reflect global cognitive capacity. To clarify the directionality of these associations, further longitudinal or intervention-based research is warranted. Additionally, prior research has suggested that the relationships between R/S and cognitive or psychological outcomes may vary, based on demographic characteristics, including gender and race.9-11 Because the present study did not incorporate these factors, potential demographic heterogeneity in R/S effects could not be evaluated; this represents an additional limitation. Future studies should investigate whether the influence of the R/S dimension on cognitive and emotional functioning differs across demographic and cultural groups, and employ longitudinal designs to clarify causal pathways.
Conclusion
This study identified distinct latent profiles based on R/S characteristics among patients with MCI and AD, and explored differences in cognitive function, depressive symptoms, and well-being across these profiles. We found that different forms of R/S engagement are associated with distinct cognitive and psychological outcomes depending on the stage of cognitive impairment. Specifically, among patients with MCI, greater IR was associated with enhanced verbal fluency and higher well-being, whereas active religious engagement—particularly structured religious practices— was associated with improved memory performance among patients with AD. Practically, these findings underscore the importance of developing tailored psychosocial interventions that incorporate various dimensions of R/S. Overall, this study provides both theoretical foundations and practical implications for enhancing the care and well-being of older adults with neurocognitive disorders.
Footnotes
Ethical Consideration
This study protocol was approved by the Institutional Review Board of Chuncheon Sacred Heart Hospital (IRB No. 2014-22).
Consent to Participate
All participants provided written informed consent after receiving a comprehensive explanation of the study objectives and procedures. To protect confidentiality, all participant data were anonymized using coded identifiers and securely stored in a locked cabinet and on a password-protected computer accessible only to authorized members of the research team. Additionally, participants consented to the publication of anonymized data derived from this study.
Consent for Publication
All authors have read and agreed to the submitted version of the manuscript.
Author Contributions
MH: writing-original draft, writing-review and editing, conceptualization, data curation, formal analysis, investigation, methodology, project administration, visualization. DHK: writing-review and editing, funding acquisition, project administration, resources, supervision, validation. MK: writing-review and editing, validation. SYM: writing-review and editing, validation. CHL: writing-review and editing, validation, statistical design and analysis advisory. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Education (No. 2021R1I1A3058026).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during the current study are available from the corresponding author upon reasonable request.