
Abstract
Foreign-born people living with cognitive impairment (PLwCI) and their family caregivers may have distinct caregiving networks compared to their U.S.-born counterparts. Data is drawn from the 2022 wave of the National Health and Aging Trends Study. Descriptive statistics and mean difference tests were run by native and foreign-born PLwCI. Linear and logistic regressions were run controlling for foreign-born PLwCI demographics with categorized time in the U.S. as the predictor of network characteristics. Foreign-born PLwCI networks were more likely to have a daughter caregiver and engage in household task-sharing, but less likely to have a spouse and non-family caregiver. In adjusted regressions, residing in the U.S. for less than 30 years was associated with greater odds of having a daughter and generalist in network, and greater task-sharing in household and self-care/mobility domains, relative to those residing over 50 years. Results underscore the importance of acculturation in shaping care networks among PLwCI.
Introduction
Within the United States the landscape of aging adults is changing, as 2023 marked the largest population of immigrants (hereafter referred to as foreign-born adults) living in the U.S. in its history at more than 47.8 million. 1 As the number of foreign-born older adults within the U.S. is projected to increase to 22 million by 2060, 2 the annual number of new cases of Alzheimer’s and other dementias is predicted to double by 2050. 3 Foreign-born older adults are at higher risk for dementia and more likely to remain undiagnosed,4,5 posing unique concerns for the older adult and their family caregivers. Community-dwelling adults living with dementia rely primarily on family and friends for assistance, creating a network of helpers who aid in one or multiple domains of care. The availability of family caregivers is an important determinant of health for older adults, 6 as these individuals impact the resources and quality of care available to the care recipient. 7 Within a dementia context, the demand in care needs often increase with the progression of the disease (eg, progressive cognitive impairment, behavioral and psychological symptoms, declining function), facilitating greater reliance on the care network. 8 This requires greater support for the care recipient, but also the caregiver. Family caregivers experience prolonged stress and frequently report caregiving-related role overload, 9 leading to greater likelihood of burn-out, role-captivity and depression.10,11 Caregivers to foreign-born older adults report greater caregiver burden than caregivers to U.S.-born older adults 12 and are observed to have higher rates of co-residence and engage in more time-consuming caregiving duties. 13 Understanding the composition of the caregiving networks and how such networks function in provision of care among foreign-born persons living with cognitive impairment (PLwCI) is vital to providing both the caregiver and care recipient with resources or services that lessen the likelihood of negative psychosocial and health outcomes for both individuals.
As caregiving practices are in-part shaped by cultural beliefs, dementia caregiving networks can vary dependent on the cultural and ethnic backgrounds of the older adult. For instance, sociocultural norms with greater emphasis on familial obligations and traditional gender roles impact who is involved in the care network and how tasks are distributed across members. 14 Delineating how foreign-born caregiving networks vary is instrumental in understanding who is in need of care related support and the quality of assistance provided to the older adult (eg, potential for unmet needs in the care recipient related to the structure and functioning of the care network). 15 Dementia-related research has focused on racial and ethnic disparities among native-born populations (eg, Black, Latinx, White), but less emphasis has been placed on understanding the nuances of caregiving strategies in foreign-born populations. Far less understood is how compositional facets of caregiving networks (eg, number of helpers, relationship to care recipient, care collaboration by networks) differs between native and foreign-born U.S. populations. Moreover, how length of time in the U.S. for foreign-born PLwCI is associated with the composition and structure of caregiving networks remains unclear. Utilizing a nationally representative study of Medicare eligible older adults, the National Health and Aging Trends Study (NHATS), this study compares characteristics of caregiving networks for PLwCI or dementia by nativity status and observes whether length of time in the United States predicts compositional facets of foreign-born PLwCI’s caregiving networks.
Cultural Components of Caregiving
The Hierarchical Selection and Task Specificity Model suggests that the caregiving networks of older adults are cultivated following a hierarchical selection process, which is dependent on the individual needs of the older adult and the availability of helpers in their network. 16 Within this hierarchy, older adults rely primarily on spouses and children, followed by friends and neighbors and finally formal assistance. Foreign-born PLwCI may have greater reliance on individuals proximal to them for care needs as migration may reduce the number of helpers available to participate in care. 17 Migration-related factors, such as the loss of extended family and social networks may significantly shape caregiving practices and the composition of the care network. 18 These stressors can influence who provides care, the availability of support, and the quality of assistance received, yet it remains underexamined in the context of dementia caregiving.
Cultural backgrounds also play an important role in shaping care approaches. The Social Ecological Model 19 describes individual health outcomes as an interplay of social systems and environmental context, each influencing behavior and development. Within these interconnected social systems, both immediate family background and broader cultural influence have impact on individual characteristics such as knowledge of health practices and beliefs surrounding care.20,21 In the context of dementia caregiving, a foreign-born individual’s country of origin and familiarity with the health care system can influence their understanding of dementia and affect the types of caregiving resources they access.22-25 Specific to dementia care, lower income countries rely more heavily on informal caregivers in comparison to high-income countries, which demonstrate greater reliance on social care such as residential and nursing home facilities. 26 For recently migrated families, familiarity with caregiving practices prior to migration may lead family caregivers to provide key aspects of care themselves.23,27 Additionally, education and economic status may necessitate the need to depend on close familial ties for care support, as formal care services exist outside of their financial means or in complex healthcare systems they may be unfamiliar with.28,29 Moreover, in comparison to U.S. culture norms, migrant families have a strong emphasis on collectivism and familial obligation and demonstrate smaller social networks,30,31 which may limit the numbers of available caregivers in their network while placing greater reliance on immediate family. Although, the roles and responsibilities of caregivers within these networks may evolve over time following migration, whether the caregiving networks of long-term immigrants differ from those of recent immigrants remains unexplored.
Time of Migration and Acculturation
Immigrant families face unique challenges as they acclimate to a new cultural and healthcare environment. However, with time, the opportunity to assimilate may give way to new caregiving strategies. Aligned with the Social Ecological Model, 19 foreign-born care approaches for PLwCI may be impacted by broader cultural norms, both from countries of origin and the newer home country. These dual influences may cause shifts in beliefs, norms and expectations in a process known as acculturation. For immigrants entering the U.S., previous cultural attitudes regarding caregiving duties may change over time influencing the composition and functioning of the caregiving network, ultimately, impacting care outcomes for both themselves and their care partner(s). Studies in Hispanic and Latin communities have shown that acculturation can positively influence self-perceptions of health, increase the likelihood of using preventative health screenings, and improve engagement with healthcare utilization. 32 However, assimilation can also have negative effects on health. For example, immigration is often associated with economic disadvantages and changes in diet quality, leading to higher rates of obesity and other health disparities.33,34 Related to network composition, certain cultures may uphold more traditional gender norms, placing greater reliance on women within the network to provide aspects of caregiving related to household tasks such as meal preparation and cleaning. 14 Consequently, there may be less perceived need to seek formal services for these tasks, as they are viewed as familial obligations. 35 For example, values such as familism, particularly prevalent in Hispanic and Latinx communities, emphasize strong interpersonal bonds and frame caregiving as a family obligation. 29 Additionally, foreign-born adults more recent to America may have fewer helpers within their family network to select from, requiring those caregivers who are available, to assist to multiple care domains at once (ie, assisting in bathing, meal preparation and transportation to doctors’ visits). Immigrant-related factors such as acculturation, reduced stigma around dementia, improved language proficiency, and growing familiarity with the healthcare system may lead to greater acceptance of formal care and broader inclusion of helpers in the caregiving network.28,36,37 This suggests that differences in caregiving networks may be partially shaped by acculturation or length of residency in the U.S., with implications for how care is distributed and managed within foreign-born families caring for PLwCI. These differences are especially salient in dementia caregiving, where long-term and intensive care needs are common. Yet, the relationship between time of migration and the evolution of caregiving networks remains an important but understudied area.
The Current Study
Guided by The Hierarchical Selection and Task Specificity Model and the Social Ecological Model, we posit that caregiving network characteristics of foreign-born PLwCI differ in comparison to U.S.-born networks. We examine whether time of migration is associated with differences in caregiving network characteristics and task engagement in care domains among foreign-born PLwCI. The aims of this research are to: 1) compare compositional facets of care network characteristics and task engagement in care domains between foreign-born and U.S.-born PLwCI, 2) assess differences in care network characteristics and task engagement by time in the U.S. among foreign-born PLwCI and, 3) observe whether length of time in the United States is associated with caregiving network characteristics and task engagement within foreign-born PLwCI, accounting for the PLwCI demographic and care characteristics. The following exploratory hypothesis is proposed given the limited research on how foreign-born networks vary following acculturation. We hypothesize that foreign-born PLwCI residing in the U.S. for a shorter length of time will have greater reliance on immediate family for care and demonstrate greater task-sharing in care domains.
Methods
Data and Sample
We utilize data from the 2022 wave of the National Health and Aging Trends Study (NHATS), a nationally representative, longitudinal dataset of Medicare eligible older adults (aged 65 or older). Our sample includes community-dwelling adults with possible or probable dementia receiving assistance from at least one helper for a medical, household, mobility/self-care, or transportation task. Additionally, we group participants by nativity status based on whether they report being U.S.- or foreign-born. In NHATS, participants can identify individuals who are cognitively impaired based on 1) self or proxy report of a dementia diagnosis, 2) score of 2 or higher on the AD8 Dementia Screening Interview, and 3) cognitive test performance (memory, executive function, orientation), details in Kasper et al,. 38 For this study we included participants classified as having either probable or possible dementia (hereafter person living with cognitive impairment; PLwCI) meaning a diagnosis of dementia was reported, AD8 criterion for dementia were met, and/or participants scored ≤1.5 SD below the mean in at least 1 cognitive testing domain. Sensitivity and specificity are strong relative to an in-home assessment and medical record informed diagnosis by consensus panel from the Aging, Demographics, and Memory Study (ADAMS). 39 Additionally, we selected individuals receiving some form of functional assistance from one or more helpers. NHATS participants are asked if smeone helps them with any self-care or mobility, household, medical, or transportation tasks and provide all names of individuals who help as well as what their relationship is to the participant. All named individuals populate a file that represents the full helper network for each participant, and which tasks each network member assisted with.
In 2022, there were 6327 participants of which 5512 were community-dwelling and of whom 4532 had complete data on study variables. Of these, 4520 had at least one helper in the network file. Next, 895 had probable or possible dementia. Finally, our analytic sample included 223 foreign-born community-dwelling PLwCI with at least one helper and 672 U.S.-born community-dwelling PLwCI with at least one helper. Only the foreign-born sample is used in regression models.
Measures
Network Characteristics
Network size was defined by the number of helpers (family and non-family) who assisted with at least one of the following domains of care: 1) medical: defined by assistance in tracking medications and/or attending doctor’s appointments with the PLwCI, 2) household: defined by assistance with laundry, shopping, hot meal preparation, and/or banking and bills, 3) mobility/self-care: defined by assistance with eating, bathing, using the toilet, getting dressed, getting out of bed, and/or getting around outside or inside, and 4) providing transportation.
We further consider the makeup of the network in terms of whether or not a particular relationship (ie, family/non-family) is assisting with care. Network membership is defined by the presence of a particular relationship type in one’s network including any: spouse, daughter, son, non-immediate family member (eg, niece/nephew, grandchild), non-family member (eg, neighbor, friend) or paid helper.
Based on prior work by Spillman and colleagues, 40 we define helpers as “Generalists” or “Specialists” based on their extent of assistance to the PLwCI. Generalists assist in multiple domains of care (e.i., tracking medications, ie, medical and getting out of bed, ie, self-care/mobility). On the other hand, a Specialist assists in only one domain of care (ie, assists with laundry and preparing hot meals, ie, tasks in the household domain). Task sharing is defined by two or more helpers assisting in one of the four aforementioned domains of care.
Key Covariate
In regression models, our key covariate is a foreign-born PLwCI’s time in the US in years. Based on the spread of the data, we broke this into tertiles of less than 30 years, 30 to 50 years, and more than 50 years in the U.S. (reference). As a sensitivity test, we consider self-reported English-speaking proficiency as a predictor on a four-point Likert scale categorized as not well at all (reference), not well, well, and very well.
Demographic Controls
We account for the PLwCI’s age, gender, chronic medical conditions (a count of 9 conditions, eg, heart disease, cancer), race/ethnicity (classified as non-Hispanic White, non-Hispanic Black, Hispanic, and Other-reference group), education (classified as less than a college degree and college degree or higher form of education), and living arrangement (classified as living alone-reference vs with others).
Analysis
First, descriptive statistics were run by U.S.- and foreign-born PLwCI with independent samples t-tests and chi-square tests run to compare mean group differences. Second, ANOVAs were run to examine mean differences in demographic and care network characteristics across length of time in the U.S. amongst the foreign-born sample (N = 223) classified as those residing less than 30 years, 30 to 50 years, or more than 50 years in the US. Next, linear and logistic regressions were run controlling for foreign-born PLwCI demographics with categorized time in the U.S. as the key predictor of network characteristics. Based on prior literature, we specifically examine the association between time in the U.S. and network size, presence of a daughter, spouse, or generalist in the network, and network task sharing of self-care and mobility, household, medical, and transportation tasks.
Results
Of the community-dwelling PLwCI receiving assistance from at least one care partner in the 2022 wave of NHATS with complete data on study variables, 25% were born outside the United States. On average, foreign-born PLwCI had lived in the U.S. for 43.6 years and less than one-third reported speaking English well or very well. The foreign-born sample had a significantly larger proportion of female PLwCI (65.0% vs 53.1%, t = 4.55, P = .04) and was significantly less likely to have a college degree (16.1% vs 30.9%, t = 7.65, P = .008). As expected, race/ethnicity differed dramatically between the groups. Only 6.5% of the U.S.-born sample was Hispanic while 65.0% of the foreign-born sample was Hispanic (ie, making up 2/3 of the foreign-born sample) (t = 231.34, P < .001).
Demographic and Care Network Characteristics of Older Adults Living With Cognitive Impairment by Nativity Status

Demographic and Care Network Characteristics of Foreign-Born Older Adults Living With Cognitive Impairment by Time in the US
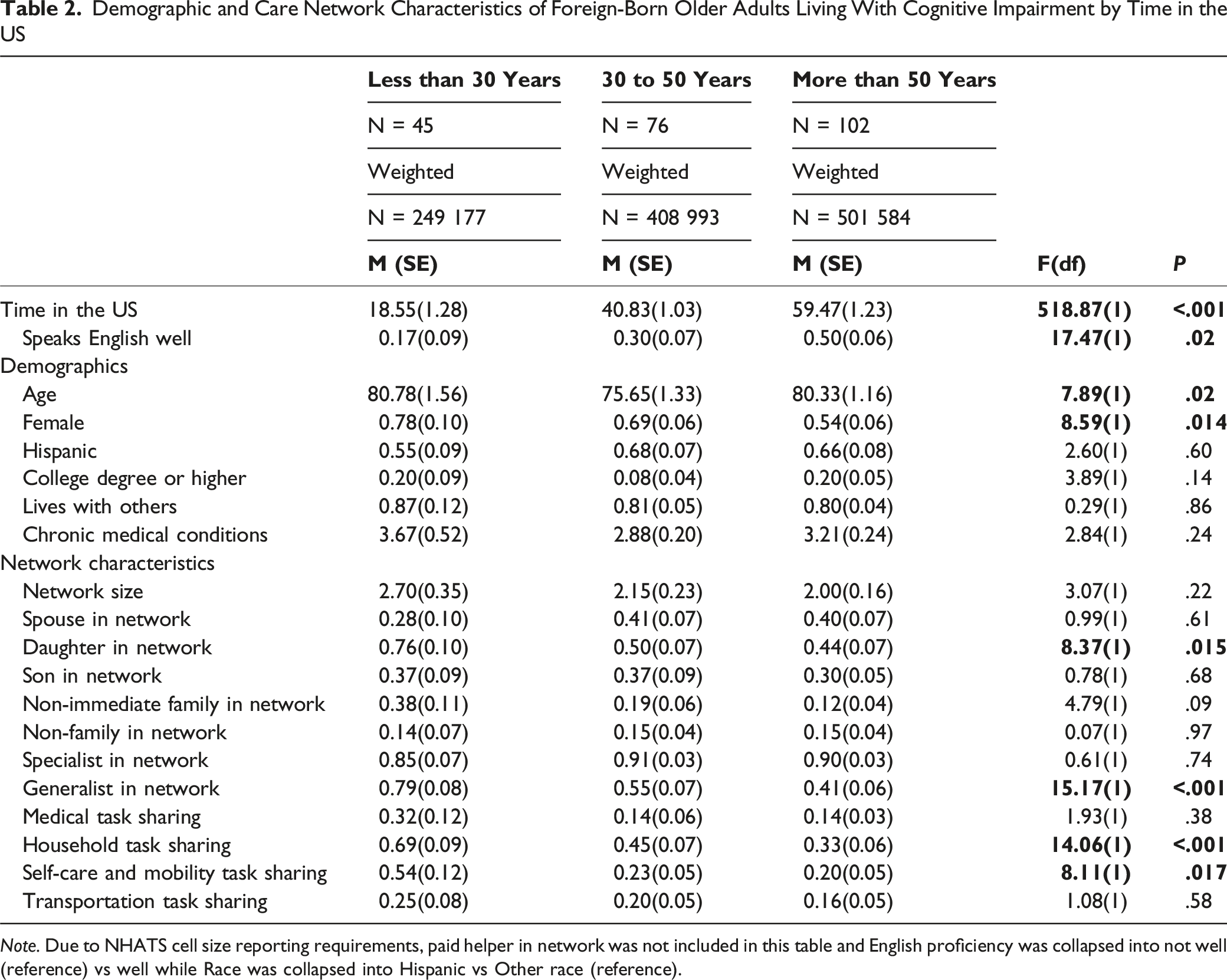
Note. Due to NHATS cell size reporting requirements, paid helper in network was not included in this table and English proficiency was collapsed into not well (reference) vs well while Race was collapsed into Hispanic vs Other race (reference).
Associations of Time Lived in the United States With Care Network Membership Characteristics of Foreign-Born Older Adults Living With Cognitive Impairment

*p < 0.05 , **p < 0.01, *** p < 0.001. aReference is Non-Hispanic White.
bReference is more than 50 years in the US.
Associations of Time Lived in the United States With Task Sharing in Care Networks of Foreign-Born Older Adults Living With Cognitive Impairment

*p < 0.05 , **p < 0.01, *** p < 0.001. aReference is Non-Hispanic White.
bReference is more than 50 years in the US.
Discussion
To our knowledge, this study is among the first to use nationally representative data from a Medicare-eligible population to examine care network characteristics among foreign-born PLwCI. We explored whether the length of time spent in the U.S.—a proxy for acculturation—was associated with care characteristics and engagement in care tasks among foreign-born older adults. Our findings contribute to a critical gap in dementia care literature by examining how nativity and migration-related factors are associated with informal caregiving arrangements in the context of cognitive impairment and dementia. Our results show foreign-born PLwCI were more likely to have an adult daughter but less likely to have a spouse and non-family member, and more likely to task share in household-related care activates, than their U.S.-born counterparts. This pattern aligns with prior literature on immigrant caregiving norms, which often emphasize filial responsibility—particularly among daughters— and less engagement with formal service and non-kin support systems. 41
Acculturation and Network Composition and Functioning
We observed differences in caregiving networks by length of residence in the U.S. Foreign-born PLwCI who had lived in the U.S. for fewer than 30 years were more likely to have care networks that included both daughters and “generalists” — caregivers who assist across multiple domains —compared to those residing 50 years or more. As a sensitivity test, we compared the foreign-born group with 50+ years since migration to the U.S.-born group, but did not find significant differences except for a lower likelihood of non-immediate family presence in the foreign-born networks. Moreover, compared to those residing more than 50 years, PLwCI living in the U.S. less than 30 years were more likely to have caregivers task sharing in household and self-care/mobility domains. Two-thirds of our foreign-born sample identified as Hispanic, and within Hispanic and Latinx communities’ cultural concepts such as familism may reinforce caregiving as a family duty. The observed greater reliance on women for household caregiving tasks, particularly within the first 30-year following migration, may suggest that recently migrated Hispanic individuals adhere more closely to caregiving expectations rooted in their country of origin, which may reflect cultural norms that emphasize traditional gender roles.14,29 Our findings align with previous research which finds that Mexican-born older adults are more likely to receive assistance with household tasks from their adult-child and reside in households with someone other than a spouse, in comparison to U.S-born older adult parents. 42 Moreover, these cultural expectations may reduce perceived need for formal services, especially in the earlier years post-migration. 35 Framed within the Social Ecological Model, 19 these findings highlight how caregiving practices are influenced by broader cultural and structural environments.
Our findings indicate no significant differences in care network size. However, the network composition between migrants who had lived in the U.S for 30 to 50 years and those residing for over 50 years differed. Those residing 30 to 50 years had a greater likelihood of having a daughter, spouse, and generalist in network, and more task-sharing across care domains, compared to those residing 50+ years. This may suggest that overtime factors such as cultural adaptation, reduced stigma regarding dementia, and increased familiarity with healthcare systems may facilitate broader inclusion of helpers and greater acceptance of formal support.
Potential Implications
Although the length of time in the U.S. may not impact the size of the care network, foreign-born PLwCI who migrated more recently may require greater assistance from caregivers living proximal to them, resulting in more intensive and robust, despite smaller and less diverse, networks. In line with similar research on foreign-born care approaches, adult daughters may assist in multiple care domains, as opposed to distributing care tasks across other members, due to traditional gender roles reflected in their country of origin’s culture, 43 as well as less familiarity with the healthcare system, 37 which may hinder the likelihood of seeking formal services that could relieve some care responsibilities. Within the U.S., over one-third of dementia caregivers are adult daughters, 3 but their presence in care networks is even more prevalent in foreign-born populations.22,27
It’s important to mention that, in comparison to their U.S.-born counterparts, foreign-born older adults are more likely to be living in poverty 2 and face structural barriers such as ineligibility for services or financial constraints that reduce the accessibility of paid or formal caregivers.28,29 As a result, family caregivers may assume broader responsibilities, especially for high-need tasks like household related assistance. Foreign-born adults with longer residency in U.S., on the other hand, may be more acculturated and aligned with U.S. norms that emphasize autonomy and the use of formal care services. These networks may include a broader range of caregivers, that may engage less frequently in direct caregiving tasks and engage in less task sharing, resulting from a lower reliance on family for care. The literature also suggests that adults who immigrate at older ages and in poorer health, often reunite with family due to existing care needs. 44 This “late-life migration” leads to greater reliance on family support. In contrast, long-term immigrants may arrive earlier in life, adapt over time, and age with greater independence resulting in dispersed support networks.
Caveats and Limitations
This study examined a nationally representative sample of PLwCI who needed some level of assistance with functional care activities. Caregiver assistance in the care domains examined in this study is evaluated by responses to a limited number of tasks within each of those domains. NHATs defines assistance in medical care by responses to two variables, whether the caregiver aids in either tracking medications or is present during doctors’ visits. Similarly, assistance in the transportation domain is defined by whether caregivers’ respond yes to providing any transportation assistance. As less variables exist within the medical and transportation care domains, the opportunity to engage in task-sharing is narrowed as there are fewer number of tasks caregivers can select from. Caregivers’ involvement in those domains may not be represented if they engage in other tasks related to transportation or medical assistance not accounted for in NHATs, potentially accounting for the lack of association with length of time in the U.S. In contrast, the household care domain contains four tasks in which the caregiver can engage in, and the mobility/self-care domain contains 6 tasks.
Additionally, the sample of foreign-born PLwCI was small (n = 223) and did not allow for inferences to be made around certain variables with low frequency of endorsement (eg, use of paid care) and henceforth such variables could not be included to adhere to policies of the dataset and general inferential statistics guidelines. For those reasons, to compare foreign-born PLwCI across time in the U.S., we collapsed race and ethnicity into Hispanic vs Other and English language proficiency into well vs not well. Future research with a larger sample may be able to consider interaction effects or greater variability in care and demographic constructs as they relate to caregiving networks of foreign-born PLwCI. In our sample, length of residence in the U.S. was categorized into three groups (less than 30 years, 30 to 50 years, more than 50 years), following the distribution of data. However, this categorization may not reflect how caregiving network composition varies the first few years post-migration for adults who immigrated later in life. The experiences of migrants entering the U.S. is vastly different from year 1 in comparison to year 29, and cultural beliefs and integration is especially impactful during this period. Those older adults who migrate later in life may acculturate more gradually, as they tend to have smaller social, are less likely to join the work force, and therefore may have limited exposure to American cultural customs.30,45,46 Additionally, the NHATs sample is drawn from individuals enrolled in the Medicare program, which contains unique eligibility requirements for immigrants. To be eligible for enrollment, immigrants must meet either 1) age and work history requirements or 2) have resided in the U.S. for 5-year as a lawful permanent resident. Therefore, our sample by design is inherently skewed toward migrants with a longer duration of residence in the U.S. Future research should observe whether the compositional trends observed in this study remain within a more narrowed distribution of time in the United States. This may be essential in providing aid and resources for the PLwCI during a critical period, allowing for tailored care assistance and intervention for the care recipient and essential support and knowledge for the caregiver. A potential direction for future research should consider how foreign-born care networks of PLwCI differ in paid help utilization depending on length of residence in the U.S. Finally, this study is cross-sectional and provides comparisons between groups by lengths of time in the U.S., but cannot imply change over time in caregiving networks, a key future direction of this work. Considering cohort differences based on key historical and cultural events that occurred in correspondence with migration to the U.S. may be another fruitful area of inquiry to understand how such events (eg, COVID pandemic, financial recession) may impact caregiving networks.
Conclusion
This study raises important questions on how caregiving networks vary over the immigrant life course and whether care networks become more concentrated—or less diversified—with longer exposure to U.S. social and healthcare systems. Results of this research underscore the importance of nativity and acculturation in shaping the structure and characteristics of care networks among persons living with cognitive impairment. As the U.S. population continues to diversify, understanding how immigrant experiences influence informal caregiving arrangements is critical for designing outreach strategies and evaluating family support needs across diverse communities. As Alzheimer’s disease and related dementias are progressive conditions, the ability of a network to adapt to changing care needs may play a key role in both quality of care received by a PLwCI and the extent of role overload and burden experienced by the caregiving network.
Footnotes
Ethical Considerations
This research was approved by the Wayne State University Institutional Review Board (IRB-22-07-4841)
Author Contributions
Study concept and design: George, Tsuker, Leggett. Acquisition, analysis, or interpretation of data: All authors. Drafting of the manuscript: Tsuker, Lai, Leggett. Critical revision of the manuscript for important intellectual content: Leggett, Tsuker, Lai. Approval of the submitted version: All authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is funded by a NIA R01AG079097 (PI: Leggett). Dr Leggett is also funded by NIAP30AB072931. The National Health and Aging Trends Study and National Study of Caregiving are produced and distributed by ![]() with funding from the National Institute on Aging (U01AG032947, R01AG054004).
with funding from the National Institute on Aging (U01AG032947, R01AG054004).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.