
Abstract
Triggering receptor expressed on myeloid cells 2 (TREM2) is upregulated in activated microglia and may be related to cognitive decline in patients with Alzheimer’s disease (AD). There is conflicting evidence regarding the association of peripheral TREM2 mRNA expression/soluble TREM2 (the extracellular domain of TREM2) with cognitive function/neuroinflammation in patients with AD. Herein, we studied the TREM2 and TREM2alt mRNA expression and their association with the cognitive performance in subjects with mild dementia due to AD and healthy controls. In a subgroup of patients with AD, magnetic resonance spectroscopy was used to measure the myo-inositol level in the posterior cingulate cortex, a surrogate marker for neuroinflammation. The results showed that increased TREM2 and TREM2alt mRNA expression is associated with AD pathogenesis at the mild dementia stage, thereby serving as a potential biomarker for early symptomatic stage of AD. TREM2 may exert protective effects on both cognition and central neuroinflammation.
Significance Statement
• The peripheral blood TREM2 and TREM2alt mRNA expression levels were higher in patients with mild AD than in the control group. • TREM2 and TREM2alt mRNA expression levels were positively associated with MMSE score in patients with mild AD. TREM2 might exert a protective function in cognition in the early symptomatic stages of AD. • TREM2 and TREM2alt mRNA expression levels were negatively associated with mI levels at the PCC on MRS, a surrogate marker for neuroinflammation, in patients with AD but not in controls.
Introduction
Alzheimer’s disease (AD), the most common neurodegenerative disease and dementia syndrome, involves amyloid-β (Aβ) deposition, tau aggregation, mitochondrial dysfunction, and cerebral vascular injury. 1 Recent evidence suggests that neuroinflammation contributes to its pathogenesis.1-5 Neuroinflammation in AD can be modulated by microglial activation in response to Aβ pathology. Microglia may exhibit neuroprotective or neurotoxic effects that signify the course of disease.6,7 Triggering receptor expressed on myeloid cells 2 (TREM2), a transmembrane glycoprotein expressed on the surface of microglia, promotes the association between microglia and Aβ plaques. This interaction facilitates the uptake and degradation of Aβ by microglia and appears to exhibit disease progression-dependent effects.8,9 Several rare variants of TREM2 have been shown to increase AD risk by 2-4-fold, which is similar to the effect of a single copy of apolipoprotein E (APOE) ɛ4.10,11
Due to the ectodomain shedding of TREM2, its extracellular domain, soluble TREM2 (sTREM2), can be detected in both the cerebrospinal fluid (CSF) and plasma. However, the relative levels of TREM2 or sTREM2 in the CSF or peripheral blood between healthy controls and patients with AD have been conflicting in previous studies.12-18 In addition, the association between peripheral TREM2 mRNA expression and cognitive status in patients with AD also varied between studies. However, most studies reported a negative correlation between the both the CSF and peripheral TREM2 expression level as well as mini-mental state examination (MMSE) score in patients with AD and patients with amnestic mild cognitive impairment.12-14,19 Finally, the correlation between peripheral TREM2 mRNA expression and central neuroinflammation is uncertain. Previous studies have shown that the level of neuroinflammation can be measured by brain magnetic resonance spectroscopy (MRS), a non-invasive method to measure metabolic, neurodegenerative changes, gliosis, and microgliosis by quantifying N-acetyl-aspartate and myo-inositol (mI).20-22 Elevated levels of mI could be a surrogate of neuroinflammation, an organic glial marker with selective expression of mRNA for sodium-dependent mI transporters in astrocytes.20,21,23,24
A recent study conducted by Moutinho and colleagues have presented experimental findings demonstrating that in the human brain, TREM2 alternatively spliced isoforms (TREM2alt) are translated and secreted as sTREM2. 25 In accordance with these findings, we compared the peripheral expression of all TREM2 mRNA isoforms and TREM2alt, which encodes sTREM2, 26 at the same time in patients with mild AD to healthy controls to examine the clinical significance of different mRNA isoforms in this study. MRS was used to investigate the association between peripheral TREM2 expression and central neuroinflammation. Based on previous studies,12,14,19 we proposed that peripheral TREM2 or TREM2alt expression might be higher in patients with mild AD than in healthy controls and is associated with cognitive function and central neuroinflammation.
Materials & Methods
Participants
We recruited patients with mild AD (clinical dementia rating (CDR) 27 = .5 or 1) and healthy controls at the outpatient clinics of 2 teaching hospitals in Taiwan. According to the National Institute on Aging-Alzheimer’s Association clinical criteria for probable AD, an AD diagnosis was made during a multidisciplinary consensus meeting. 28 The age at onset of the disease needed to be 65 years or older, and a caregiver who could provide a collateral history was required to be present. Patients with AD received a standardized evaluation that included clinical interviews, neuropsychological assessments, laboratory tests, and magnetic resonance imaging (MRI).
Patients with significant neurological diseases other than AD that affect cognition, medical history of chronic inflammatory conditions, and anti-inflammatory or immunosuppressive medication use were excluded from the study. This study was approved by the institutional review boards of the 2 hospitals. Informed consent was obtained from all the patients and their caregivers before participating in the study.
Clinical Evaluation and Procedures
During recruitment, cognitive function was assessed using standard procedures. The MMSE 29 was used to assess global cognition. The CDR was administered to determine the severity of dementia. The 12-item memory test, 30 modified 15-item Boston naming test, 31 category verbal fluency test, 32 trail making test A, 33 and forward and backward digit span tests were used to assess short-term memory, language, executive function, attention, and working memory, respectively. Depression was evaluated using the short form of the geriatric depression scale. 34
TREM2 mRNA Measurement
Total ribonucleic acid (RNA) was extracted from the whole extraction of total RNA according to the standard protocol of the TempusTM Blood RNA Systems (P/N4342792; P/N4380204, Applied Biosystems, CA, USA). The concentration and purity of the extracted total RNA were measured using a NanoDrop® ND-1000 spectrophotometer (Thermo Fisher Scientific). To quantitatively estimate TREM2 mRNA levels, complementary deoxyribonucleic acid (cDNA) was synthesized from 1 μg of total RNA using a High Capacity cDNA Reverse Transcription Kit (P/N4368814, Applied Biosystems, CA, USA) in accordance with the manufacturer’s instructions.
Preamplification was performed using the TagMan® PreAmp Master Mix Kit (P/N4391128; Applied Biosystems, CA, USA). Following the manufacturer’s protocol, the pooled assay mixtures contained TagMan® Gene Expression Assays (P/N4331182, Applied Biosystems, CA, USA) and endogenous control, and Tris-ethylenediaminetetraacetic acid (EDTA) buffer was used to dilute the pooled assays to a final concentration (Assay ID: Hs00219132_m1 to capture all TREM2 transcripts; AI89K96 to capture TREM2alt transcript; glyceraldehyde 3-phosphate dehydrogenase, Hs99999905_m1). The preamplification reaction, including the TagMan® PreAmp Master Mix, pooled assay mix, and cDNA sample, was incubated for 10 min at 95°C, followed by 14 cycles of 95°C for 15 s and 60°C for 4 min, and held at 4°C in an Applied Biosystems Thermocycler (9700). The preamplification product was further diluted with Tris-EDTA buffer to serve as a template for real-time polymerase chain reaction (PCR) analysis.
For quantitative estimation of TREM2 and TREM2alt mRNA levels, the StepOnePlusTM Real-Time PCR System (Applied Biosystems, CA, USA) was used in triplicate for each sample. The final reaction volume was 10 μL using the TaqMan Universal Master Mix with UNG (P/N4440044, Applied Biosystems, CA, USA). Relative mRNA levels were calculated using the 2-ΔΔCT method using StepOne software 2.3 (Applied Biosystems, CA, USA). 35 The median level of healthy controls was used for calibration in all experiments to correct for any observational errors.
DNA Analysis
Genomic DNA was isolated from whole blood using the Gentra Puregene kit, according to the manufacturer’s protocol (Qiagen, Hilden, Germany). The presence of the ε2, ε3, and ε4 alleles of the APOE gene was determined by genotyping the single nucleotide polymorphisms rs429358 and rs7412. An APOE ε4 carrier was defined as having at least one ε4 allele (including ε2/ε4, ε3ε4, and ε4/ε4). Genotyping of rs429358 and rs7412 was performed using the TaqMan genotyping assay (Applied Biosystems, Foster City, CA, USA). PCRs were performed in 96-well microplates using an ABI StepOnePlusTM real-time PCR machine (Applied Biosystems). Allele discrimination was achieved by detecting fluorescence using StepOne software 2.3 (Applied Biosystems, CA, USA).
Magnetic resonance spectroscopy
The second half of the study involved brain MRS in 25 consecutive patients consecutively. Brain MRI studies were performed using a GE Discovery 3 Tesla MRI. A 3D T1 FSPGR image series (TR = 6.8 ms, TE = 2.5 ms, 24 cm2 FOV; 1 mm3 isotropic voxels) was used for the localization of posterior cingulate cortex (PCC) (volume of interest = 2 × 2 × 2 cm3 in the midsagittal PCC region), which is commonly known the site of initial neuropathological changes in AD and has been investigated in many previous studies.36,37 Proton MR spectra were acquired using the PRESS localization sequence with TR = 2000 ms, TE = 35 ms, and 8 and 160 total numbers of scans for each acquisition. Brain MRI and proton MR spectra quality were visually assessed by an expert neuroradiologist (Lirng JF) blinded to the clinical condition. Peak areas of creatine (Cr) + phosphocreatine (PCr) and mI were calculated using LCModel. The glial marker for neuroinflammation was measured using the mI relative to Cr + PCr at the PCC.
Statistical Analysis
The demographic and neuropsychiatric data of the AD and control groups were compared using the chi-square test or Mann-Whitney U test when appropriate. The skewness values of TREM2 and TREM2alt mRNA expression exceeded one. Thus, we log-transformed TREM2 and TREM2alt mRNA expression values for further analysis. 38 Differences in TREM2 and TREM2alt mRNA expression levels between the 2 groups were examined using a one-way analysis of covariance after adjusting for age, sex, and APOE ɛ4 carrier status. In addition, the linear regression stratified by sex was also performed. The associations between MMSE and TREM2 and TREM2alt in patients with AD were examined using Spearman’s correlation and linear regression after adjusting for age, sex, years of education, and APOE ɛ4 carrier status. To further evaluate the association between TREM2 expression and mI level (mI relative to Cr + PCr) on MRS, Spearman’s correlation and linear regression analyses were performed after adjusting for age, sex, and APOE ɛ4 carrier status.
Results
Subjects and Demographics
Clinical Characteristics and Neuropsychological Data of all Participants.
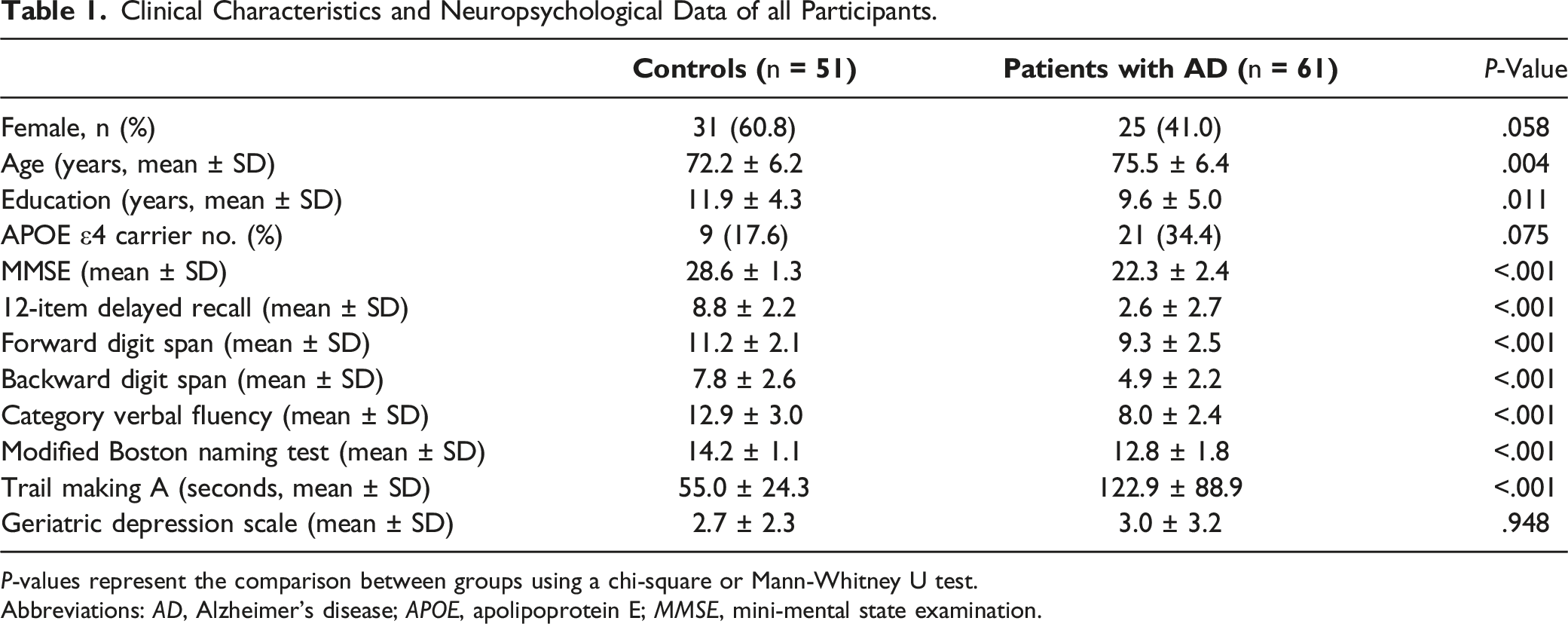
P-values represent the comparison between groups using a chi-square or Mann-Whitney U test.
Abbreviations: AD, Alzheimer’s disease; APOE, apolipoprotein E; MMSE, mini-mental state examination.
TREM2 and TREM2alt mRNA Expression Levels
After log-transforming the TREM2 and TREM2alt mRNA expression values, patients with AD showed a significantly higher expression of TREM2 mRNA than the control group (1.28 ± .46 vs 1.05 ± .44, P = .013). Patients with AD also showed significantly higher expression of TREM2alt mRNA compared to the control group (1.52 ± .77 vs 1.03 ± .48, P = .001) (Figure 1). Comparison of the peripheral TREM2 and TREM2alt mRNA expression levels between patients with AD and controls. The expression of TREM2 and TREM2alt mRNA showed significant differences between patients with AD and controls (TREM2, P = .013; TREM2alt, P = .001).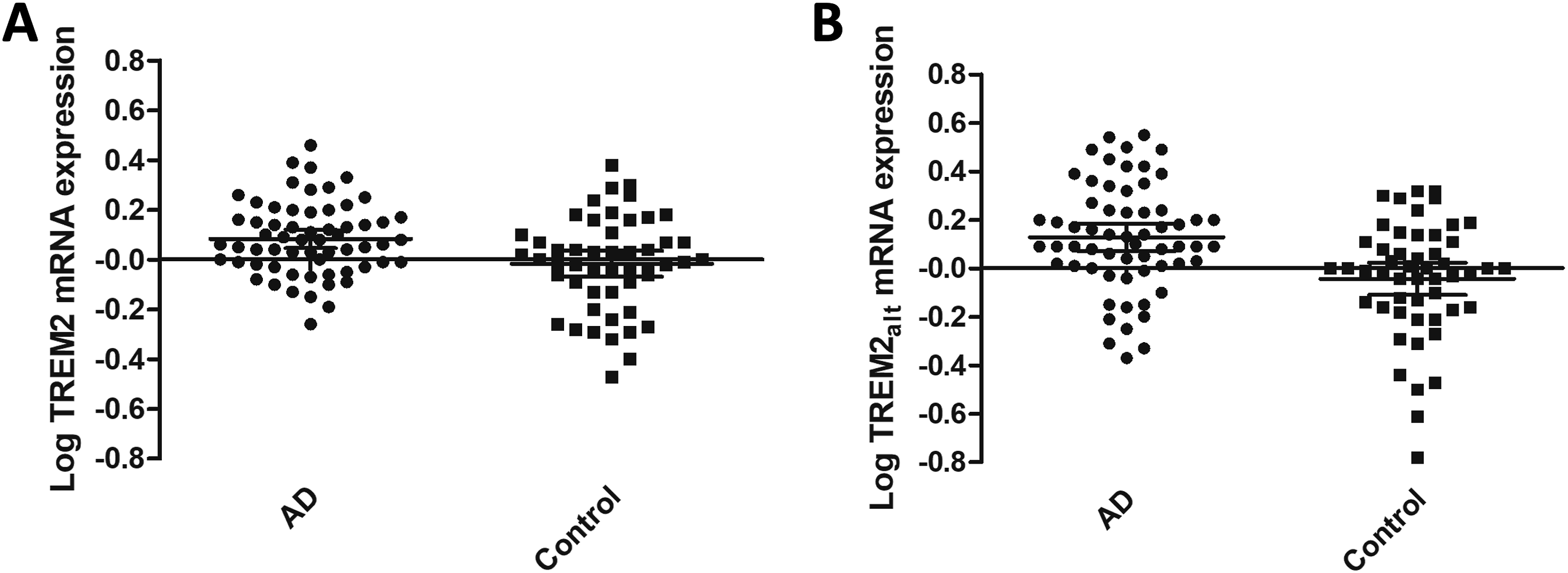
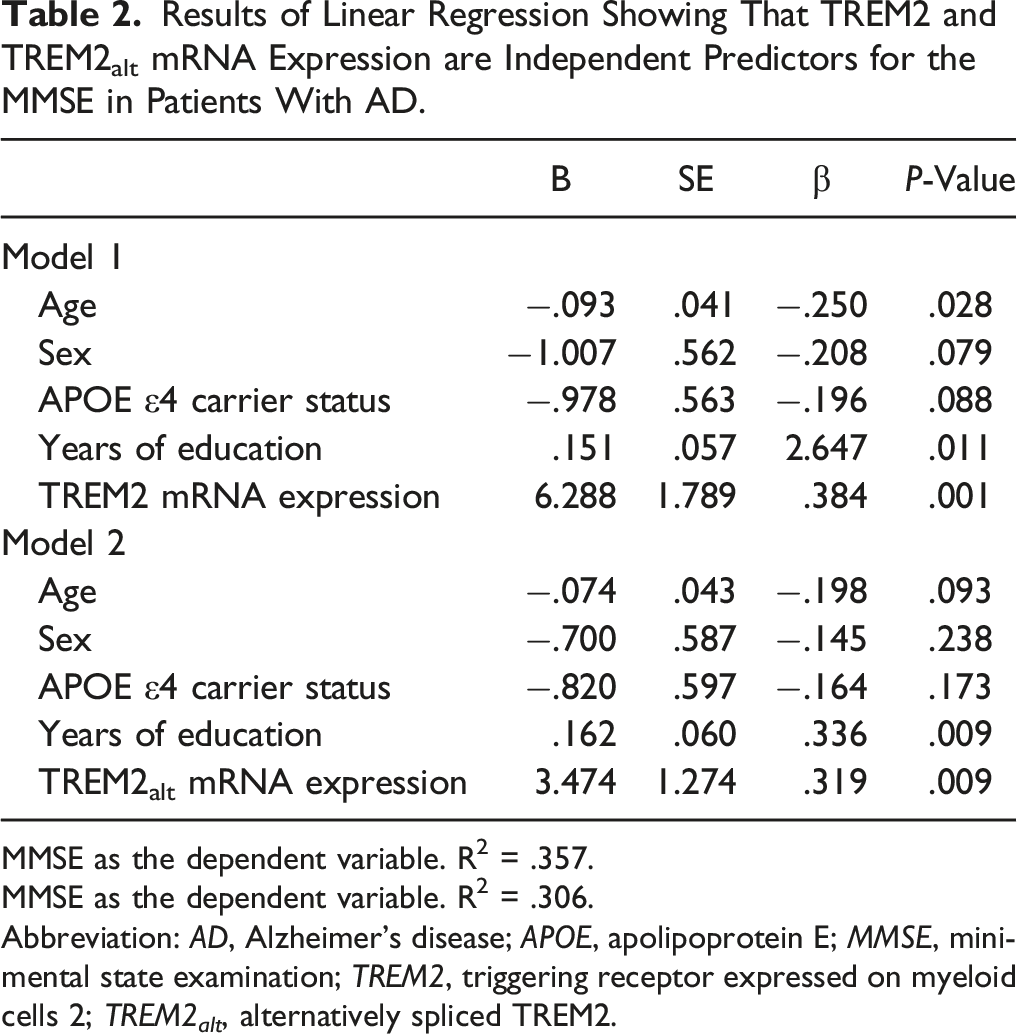
Associations Between MMSE and TREM2, as Well as TREM2alt mRNA Expression in Patients with AD
After log-transforming the TREM2 and TREM2alt mRNA expression values, there were significant positive correlations between the MMSE score and TREM2 mRNA expression (rs = .305, P = .017) and TREM2alt mRNA expression (rs = .302, P = .018) in patients with AD (Figure 2), but not in controls. After adjusting for covariates, linear regression also showed that TREM2 and TREM2alt mRNA expression were independent predictors of the MMSE scores in patients with AD (TREM2, P = .001; TREM2alt, P = .009) (Table 2). Furthermore, in the linear regression stratified by sex, there was still a significant correlation between TREM2 mRNA expression and MMSE in both male and female AD patients, although this correlation was less pronounced for TREM2alt mRNA expression (Supplemental Tables 1 and 2). Correlation between the MMSE score and TREM2 and TREM2alt mRNA expression in patients with AD. Significant correlations between the MMSE score and TREM2 mRNA expression (rs = .305, P = .017) and TREM2alt mRNA expression (rs = .302, P = .018). Results of Linear Regression Showing That TREM2 and TREM2alt mRNA Expression are Independent Predictors for the MMSE in Patients With AD. MMSE as the dependent variable. R2 = .357. MMSE as the dependent variable. R2 = .306. Abbreviation: AD, Alzheimer’s disease; APOE, apolipoprotein E; MMSE, mini-mental state examination; TREM2, triggering receptor expressed on myeloid cells 2; TREM2
alt
, alternatively spliced TREM2.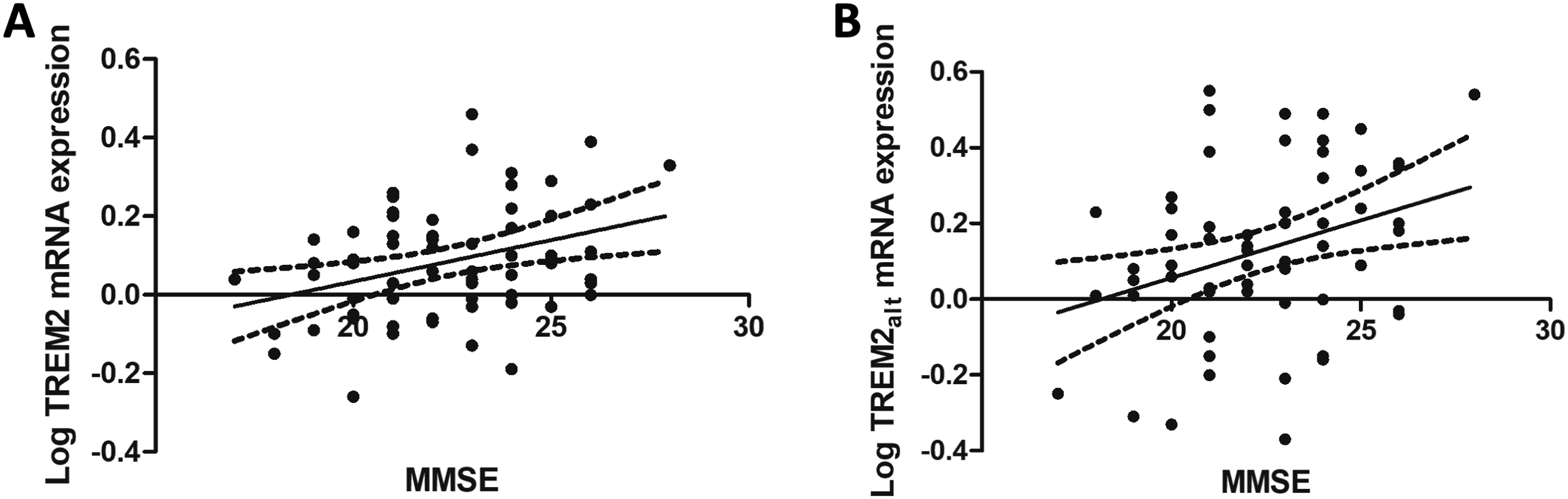
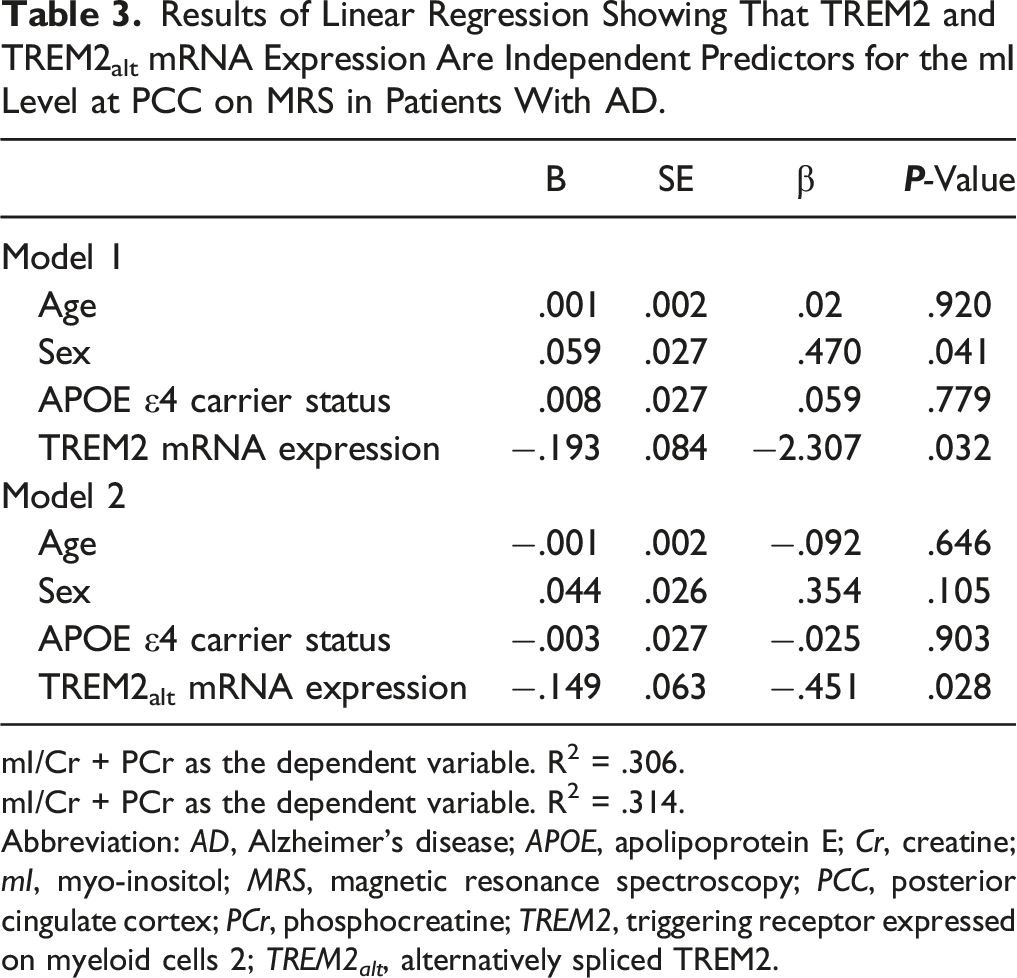
Associations Between mI Level at PCC on MRS and TREM2 as Well as TREM2alt mRNA Expression in Patients with AD
In total, 25 patients underwent MRS. There were no differences in the sex ratio (P = .51), age (P = .82), years of education (P = .96), the prevalence of APOE ɛ4 carriers (P = 1.00), and MMSE score (P = .72) between this subgroup and the subgroup without MRS. After log-transforming the TREM2 and TREM2alt mRNA expression values, there were significant negative correlations between mI levels at the PCC on MRS and TREM2 mRNA expression (rs = −.426, P = .034) and TREM2alt mRNA expression (rs = −.447, P = .025) in patients with AD (Figure 3), but not in controls. After adjusting for covariates, linear regression also showed that TREM2 and TREM2alt mRNA expression were independent predictors of mI levels at the PCC on MRS in patients with AD (TREM2, P = .032; TREM2alt, P = .028) (Table 3). Correlation between the MRS-measured mI level (mI/Cr + PCr) at PCC and TREM2 and TREM2alt mRNA expression in patients with AD (n = 25). Significant correlations between the MMSE score and TREM2 mRNA expression (rs = −.426, P = .034) and TREM2alt mRNA expression (rs = −.447, P = .025). Results of Linear Regression Showing That TREM2 and TREM2alt mRNA Expression Are Independent Predictors for the mI Level at PCC on MRS in Patients With AD. mI/Cr + PCr as the dependent variable. R2 = .306. mI/Cr + PCr as the dependent variable. R2 = .314. Abbreviation: AD, Alzheimer’s disease; APOE, apolipoprotein E; Cr, creatine; mI, myo-inositol; MRS, magnetic resonance spectroscopy; PCC, posterior cingulate cortex; PCr, phosphocreatine; TREM2, triggering receptor expressed on myeloid cells 2; TREM2
alt
, alternatively spliced TREM2.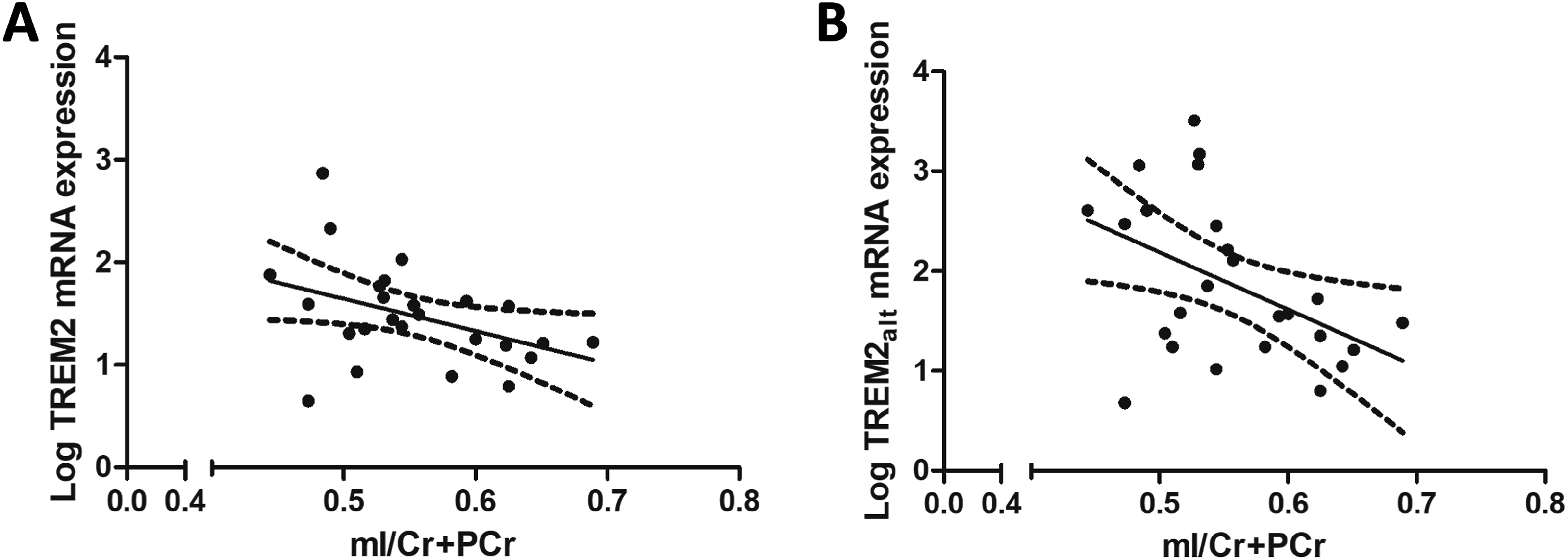
Discussion
The present study showed higher peripheral blood TREM2 and TREM2alt mRNA expression levels in patients with mild AD than in the control group. In addition, TREM2 and TREM2alt mRNA expression were positively associated with cognitive status and negatively associated with the marker of central neuroinflammation. These findings suggest a protective function of peripheral TREM2 in cognition and neuroinflammation in the early symptomatic stages of AD. Furthermore, we observed increased peripheral TREM2 and TREM2alt mRNA expression levels in patients with mild AD. The results provide additional evidence of changes in TREM2 expression during the early symptomatic stage of AD. They indicate that peripheral TREM2 and TREM2alt mRNA levels could be potential biomarkers associated with neuroinflammation in the early stage of AD dementia.
The increased peripheral TREM2 mRNA expression in patients with AD echoed most of the findings of previous studies.12-14 However, the present study is the first to demonstrate that peripheral TREM2alt mRNA expression is higher in patients with AD. TREM2alt is responsible for encoding sTREM2, the extracellular domain of TREM2 due to ectodomain shedding. The CSF sTREM2 level serves as a surrogate measure of microglial activity and tauopathy.39,40 While many studies demonstrate an elevation of CSF sTREM2 along the AD continuum, inconsistencies exist regarding disease stages, 41 thereby reducing the discriminative power necessary for diagnostic purposes. A previous study showed that TREM2alt mRNA expression was also higher in the temporal cortex of patients with AD, but this difference was not significant after adjusting for covariates. 26 Similarly, a recent research also demonstrated elevated levels of TREM2alt mRNA and other isoforms in several AD brain regions. 25 One of the few studies addressing the implication of peripheral sTREM2 in AD demonstrated that plasma sTREM2 levels correlate with inflammatory activity in the peripheral circulation and vary across different stages of the disease. 42 Therefore, the findings of the present study suggest that the measurement of TREM2alt expression in the peripheral blood may reflect the activation of TREM2-related signaling and an altered peripheral immune activity in response to early-stage AD pathology.
Our study found a positive correlation between the MMSE score and TREM2 expression in patients with mild AD after adjusting for covariates, including APOE ɛ4 carrier status, but not in controls. In AD pathology, the continued activation of microglia and prolonged neuroinflammation may adversely affect brain function and contribute to neurodegeneration. The upregulation of TREM2 in peripheral blood mononuclear cells appears to offer protection against neuroinflammation by suppressing sustained microglial activation, enhancing phagocytosis, and facilitating the clearance of apoptotic neurons. 43 Hence, TREM2 might prove valuable as an early peripheral biomarker for AD development. Our discovery suggests possible alterations in systemic TREM2 function during the early stages of cognitive decline, highlighting its significance as a crucial player in a broader, potentially systemic immune response in AD.
The cognitive protective function of TREM2 was also supported by other studies, although indirectly. In vivo studies have shown that functional TREM2 plays a role in the phagocytic clearance of amyloid seeds during early amyloidogenesis 44 and that TREM2-deficient microglia exhibit strong cerebral metabolic defects and increased stress markers. 45 A recent study also showed that CSF sTREM2 expression was decreased in the earliest asymptomatic phase of AD with the presence of abnormal Aβ pathology but not tau pathology or neurodegeneration, and an increased sTREM2 level in the CSF in an early symptomatic stage of AD was associated with tau-related neurodegeneration instead of Aβ pathology. 46 Together, these findings suggest that CSF TREM2 expression might be a response to tau pathology in the early symptomatic phase of AD and that CSF TREM2 has a protective effect during the early stage. However, the results of studies examining the correlation between peripheral mRNA expression levels of TREM2 and MMSE were contradictory. One study showed a significant negative correlation between peripheral TREM2 expression and MMSE scores in patients with moderate to severe AD (MMSE: 0-16). 12 Another study reported that higher serum TREM2 levels were correlated with lower MMSE scores after correcting for APOE ɛ4 carrier status. 13 Another study evaluating patients with AD and schizophrenia showed no correlation between peripheral TREM2 levels and MMSE scores. 14 These conflicting findings suggest dynamic changes or a disease stage-dependent effect of peripheral TREM2 expression during the disease course of AD18,47 and an interaction among cognitive status, APOE ɛ4 carrier status, and TREM2 expression.
Our study had several limitations. First, the diagnoses of AD were made based on clinical criteria without biomarker evidence of Aβ and tau, which may have influenced diagnostic accuracy. Second, we did not measure the corresponding peripheral TREM2 protein level at the same time because previous studies have shown similar results between the protein level and mRNA expression. 12 Third, while many pharmacological or metabolic factors may alter serum TREM2 mRNA expression levels in study participants, we only excluded subjects with infective or inflammatory conditions or anti-inflammatory or immunosuppressive medication use at the time of blood sampling. Fourth, the relatively small sample size may have limited the statistical power of our study. Another independent cohort study with more participants should be conducted in the future to confirm the results. Lastly, the carrier status of the TREM2 R47H variant, a risk mutation linked to AD, was unknown among the studied subjects. Consequently, we are unable to account for this variable in the study.
In conclusion, increased peripheral TREM2 and TREM2alt mRNA expression are associated with AD pathogenesis in patients with mild dementia. The positive associations of both peripheral TREM2 and TREM2alt mRNA expression with the MMSE score in mild AD suggested that TREM2 may exhibit protective effects on cognitive status. In contrast, the negative association of serum TREM2 mRNA levels with mI levels at the PCC in the subgroup of patients with AD might suggest the role of TREM2 in modulating central nervous system inflammation. Peripheral TREM2 and TREM2alt mRNA levels may be potential biomarkers associated with neuroinflammation in the early symptomatic stages of AD.
Supplemental Material
Supplemental Material - Different Splice Isoforms of Peripheral Triggering Receptor Expressed on Myeloid Cells 2 mRNA Expressions are Associated With Cognitive Decline in Mild Dementia Due to Alzheimer’s Disease and Reflect Central Neuroinflammation
Supplemental Material for Different Splice Isoforms of Peripheral TREM2 mRNA Expressions are Associated With Cognitive Decline in Mild Dementia Due to Alzheimer’s Disease and Reflect Central Neuroinflammation by Yi-Kuan Chiang, Yung-Shuan Lin, Chun-Yu Chen, Jiing-Feng Lirng, Yu-Hsiu Yang, Wei-Ju Lee, and Jong-Ling Fuh in American Journal of Alzheimer’s Disease & Other Dementias®
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by grants from the Academia Sinica of Taiwan (AS-BD-108-2; AS-KPQ-111-KNT), National Health Research Institutes, Taiwan (PH-112-GP-08, NHRI-11A1-CG-CO-05-2225-1), the Ministry of Science and Technology, Taiwan (NSTC 111-2321-B-001-010-, 111-2314-B-075 -069 -, 111-2321-B-A49-011-, 111-2634-F-A49-014-, 112-2314-B-075 -036 -MY2, 112-2321-B-001 -008 -). Taipei Veterans General Hospital (V111C-216, V112C-016), Taichung Veterans General Hospital (TCVGH-1093402C, TCVGH-1103401C, TCVGH-1103401D, TCVGH-113401D), and the Brain Research Center, National Yang Ming Chiao Tung University from The Featured Areas Research Center Program within the framework of the Higher Education Sprout Project by the Ministry of Education (MOE) in Taiwan.
Ethical Statement
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.