
Abstract
Objective:
Oral health status may be associated with dementia, which in turn results in higher medical costs among older people.
Methods:
This STUDY enrolled 4,275 older individuals. Generalized linear models were constructed with the medical costs of dementia as the dependent variable, and number of teeth, Community Periodontal Index (CPI), and other factors as independent variables.
Results:
Individuals with fewer teeth or with poor periodontal condition had significantly higher medical costs ratios for dementia independent of other confounding variables. The adjusted medical costs ratios of dementia were 4.13 (95% CI [confidence interval]; 1.79–9.56) for those with ≤9 teeth compared with those with ≥20 teeth and 3.48 (95% CI; 1.71–7.08) for those with personal CPI code 4 compared with those with personal CPI code 0–2.
Conclusions:
Oral health status was associated with the medical costs of dementia. Preventing tooth loss and maintaining periodontal health may contribute to controlling dementia costs.
Introduction
There are 46.8 million patients with dementia worldwide and this number is predicted to increase as the population ages. 1 Dementia interferes with daily life and significantly reduces the quality of life (QOL). 2 As a result, dementia is one of the 10 most burdensome conditions among older people worldwide. 1 Since dementia patients require more support for daily life, such as with using the toilet, bathing, and eating, than patients with other diseases, it affects not only the patients themselves but also the QOL of their families and caregivers. The costs associated with dementia are increasing and are estimated to exceed $2 trillion worldwide in 2030. 1 The increasing cost is a global problem; in high-income countries, it accounts for more than 80% of the global cost of dementia, with an annual cost per dementia patient exceeding $30,000. 1 With population aging, dealing with dementia is an important issue that must be addressed by society as a whole.
Systemic diseases such as diabetes and dyslipidemia are risk factors for dementia, 3 as are lifestyle habits, such as smoking and a lack of exercise. 4 Furthermore, oral health status, such as tooth loss and periodontal disease, is associated with dementia. 5,6 A 4-year follow-up study of community-dwelling older adults reported that those with few teeth have a significantly higher risk of cognitive decline. 5 A study using Korean health insurance data found that individuals with chronic periodontitis had a significantly higher risk of developing dementia than those without periodontitis. 6 Decreased masticatory function due to tooth loss and chronic inflammation due to periodontal disease are considered risks of dementia.
While many studies have investigated the relationship between oral health and dementia, 5 -7 no study has examined the relationship between oral health and dementia in terms of medical costs. Clarification of the relationship between the medical costs of dementia and oral health status may help to control the overall costs of dementia. Therefore, this study examined the effects of the number of teeth and periodontal condition on the medical costs of dementia among older people.
Methods
Study Population
The study enrolled people insured by the medical care system for the elderly in Mie Prefecture. The insurer of this medical care system conducts annual health checks for insured persons. The government started supporting dental examinations for older people in 2014 and the insurer for the elderly in Mie Prefecture has been conducting dental examinations for 75- and 80-year-olds. The target population for dental examinations in fiscal 2014 was 33,378. Of these, 4,984 people who underwent dental examinations were enrolled in this study. The oral health examinations were performed as components of periodic health checkups for aged individuals. We obtained permission from the insurer to use de-identified data and the study was approved by the institutional review board of Aichi Gakuin University School of Dentistry (approval number 443) and was conducted in full accordance with all relevant dictates of the World Medical Association Declaration of Helsinki.
Dental Examination
In September 2014, 75- and 80-year-old individuals living in Mie Prefecture were sent information on dental examinations, which were performed at dental clinics belonging to the Mie Dental Association from October 1, 2014 to November 30, 2014. The state of each tooth was recorded as sound, decayed, filled, or missing, and the total number of sound, decayed, and filled teeth excluding the third molars was taken as the number of teeth, and the Community Periodontal Index (CPI) was used as an index of periodontal condition. 8 The oral cavity of each participant was divided into 6 sectors and teeth 11, 16, 17, 26, 27, 31, 36, 37, 46, and 47 were evaluated as representative teeth. The CPI for each sector was coded as follows: 0 for healthy, 1 for bleeding after probing, 2 for dental calculus detected by probing, 3 for 4∼5 mm periodontal pocket, 4 for ≥6 mm periodontal pocket, and X for relevant teeth missing. The highest value of the CPI, excluding code X, for the 6 sectors was used as the personal CPI of periodontal status. For those in whom all sectors were code X, the personal CPI was defined as code X.
Questionnaire
A self-reported questionnaire was used to survey lifestyle and current medical history. Information on current smoking habit (yes or no), body mass index (BMI; kg/m2), and current medical history (stroke, cardiovascular disease, and diabetes mellitus) was obtained.
Medical Costs
Medical costs related to dementia were calculated from medical cost data managed by the insurer for the elderly in Mie Prefecture. As medical costs, the accumulated medical costs for 4 years from April 2015 to March 2019 were used. A diagnosis of dementia was based on the International Statistics Classification of Diseases and Related Health Problems (ICD-10) disease classification code 501 (vascular and unspecified dementia) and code 602 (Alzheimer’s disease). The medical costs of dementia were the sum of the medical expenses for each medical institution when the main disease was dementia. The medical costs of dementia were not recorded for those who had received treatment for dementia whose main disease was another disease. Medical costs were calculated in yen (100 yen = 0.84 USD; exchange rate on 1 April 2015). Medical costs were limited to those incurred in medical institutions and did not include dental, non-institutional pharmacy/dispensary, or visiting nursing costs.
Statistical Analysis
Of the 4,984 participants undergoing baseline dental examinations in 2014, 488 who died by March 2019, 152 participants with missing data, and 69 who received treatments for dementia in 2014 were excluded from the analysis. Finally, we analyzed 4,275 participants. The number of teeth was classified into 3 categories: ≤9, 10–19, or ≥20 teeth. The CPI was divided into 4 categories (codes 0–2, 3, 4, or X). BMI was divided into 3 categories (<18.5, ≥18.5 to <25 kg/m 2 , or ≥25 kg/m 2 ). Because the frequency distributions of the medical costs of dementia are often zero, and others are continuous, these data were mixed and include compound Poisson and Gamma distributions. The response variable, the medical costs of dementia, was analyzed using generalized linear models (GLM) with the Tweedie (1.5) error structure and a log link function. 9 In the analyses of GLM using the medical costs of dementia as the dependent variable, the crude effects of each independent variable (i.e., age, sex, smoking status, BMI, medical history, number of teeth, and CPI) were analyzed and the medical costs ratios and 95% confidence intervals (CIs) were calculated. In the multivariate analysis, the major explanatory variables such as the number of teeth and CPI were entered simultaneously, and we analyzed 3,894 participants excluding edentulous participants and those with personal CPI code X. We applied 3 different models, with the following confounding variables: age and sex in Model 1; age, sex, and current smoking habit in Model 2; and age, sex, current smoking habit, BMI, and medical history in Model 3. The goodness of model fit was calculated by dividing the deviance by the degree of freedom. All statistical analyses were performed with SPSS ver. 26.0 (IBM, Armonk, NY, USA). A P-value <0.05 was considered statistically significant.
Results
Of the 4,275 participants analyzed, 201 were charged for medical costs of dementia during the 4-year period. Table 1 shows the number of individuals and medical costs of dementia of each category for each variable for the participants with dementia.
Number of Participants With Dementia and Medical Costs of Dementia Among Subject With Dementia During Follow-up Period.
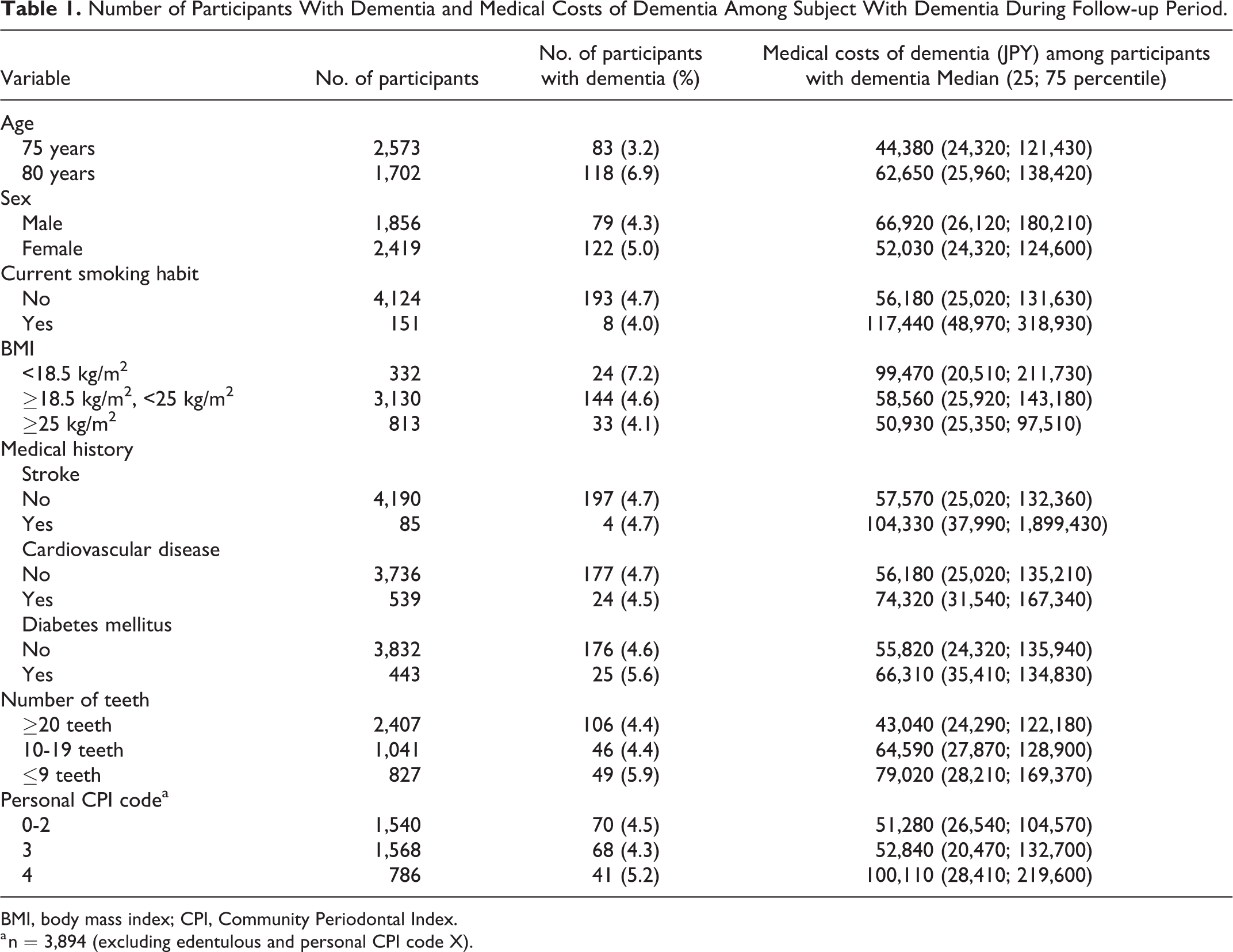
BMI, body mass index; CPI, Community Periodontal Index.
a n = 3,894 (excluding edentulous and personal CPI code X).
Table 2 shows the results of the generalized linear model with the medical costs of dementia as the dependent variable. Age, number of teeth, and personal CPI code were significantly related to the medical costs of dementia. The medical costs ratios of dementia were significantly higher in participants with ≤9 teeth compared with those with ≥20 teeth and in the participants with personal CPI code 4 compared with those with personal CPI code 0–2; the crude medical costs ratios were 3.79 (95% CI 1.46–9.87) and 4.04 (95% CI 1.43–11.47), respectively.
Relationship Between Each Independent Variable and Medical Costs of Dementia by Generalized Linear Model With a Log Link and Tweedie Distribution.

CI, confidence interval; BMI, body mass index; CPI, Community Periodontal Index.
a n = 3,894 (excluding edentulous and personal CPI code X).
Table 3 shows the multivariable medical costs ratio of oral factors from the generalized linear model. In Model 1 adjusted for age and sex, the medical costs ratios of dementia were significantly higher in participants with ≤9 teeth compared with those with ≥20 teeth and participants with personal CPI code 4 compared with those with personal CPI code 0–2; the multivariate medical costs ratios were 4.49 (95% CI 1.79–11.21) and 3.19 (95% CI 1.38–7.33), respectively. In Model 2 adjusted for age, sex, and current smoking habit, the multivariate medical costs ratios of dementia for participants with ≤9 teeth and for those with personal CPI code 4 were 4.49 (95% CI 1.80–11.23) and 3.17 (95% CI 1.38–7.28), respectively. In Model 3 adjusted for age, sex, current smoking habit, BMI, and medical history, the multivariate medical costs ratios of dementia for participants with ≤9 teeth and for those with personal CPI code 4 were 4.13 (95% CI 1.79–9.56) and 3.48 (95% CI 1.71–7.08), respectively.
Relationship Between Oral Health Factors and Medical Costs of Dementia by Generalized Linear Model With a Log Link and Tweedie Distribution (n = 3,894)a.

CI, confidence interval; CPI, Community Periodontal Index.
a Excluding edentulous and personal CPI code X.
bAdjusted for age and sex.
cAdjusted for age, sex, and current smoking habit.
dAdjusted for age, sex, current smoking habit, body mass index, and medical history (stroke, cardiovascular disease, and diabetes mellitus).
Discussion
This study examined the relationship between oral health status and the medical costs of dementia, and found that the number of teeth and periodontal status were significantly related to the medical costs of dementia.
Older people with ≤9 teeth had significantly higher medical costs of dementia than those with ≥20 teeth. It has been reported that tooth loss is associated with dementia. In a follow-up study of community-dwelling elderly, those with fewer teeth had a higher risk of dementia. 10 Tooth loss may accelerate cognitive decline. 11 However, it is not clear how tooth loss is a risk for dementia. A possible mechanism is that the decreased masticatory function due to tooth loss may increase the risk of dementia.
Chewing may prevent cognitive decline by increasing cerebral blood flow and activating the brain. 12,13 Experiments with mice have shown that mice with low masticatory function had reduced learning and memory functions, and that the number of neurons in the hippocampus was low. 14 Conceivably, the decrease in masticatory function due to the loss of many teeth leads to decreased blood flow to the brain and a decrease in nerve cells, and thereby increases the risk of dementia. Thus, having fewer teeth may increase the medical costs of dementia.
People without molar support have a higher risk of dementia. 15,16 Mice missing molars had impaired spatial learning and neuronal changes in the hippocampus. 17 Preventing tooth loss and maintaining masticatory function may then reduce the medical costs of dementia. Therefore, it is necessary to restore masticatory function and occlusal support by performing appropriate prosthetic treatment for those who have lost their teeth.
Many studies have reported associations of diet and nutrition with dementia. 18 -20 No definitive results have been obtained regarding the association of certain foods and nutrients with dementia, but it was reported that undernutrition and weight loss are associated with the onset and progression of dementia. 21 In a cohort study of patients with Alzheimer’s disease, the patients with weight loss had rapid cognitive decline. 21 Since the decline in masticatory function due to tooth loss leads to malnutrition, 22,23 it may be a risk for dementia. Preventing tooth loss and subsequent malnutrition may contribute to preventing dementia and reducing dementia-related costs.
In this study, individuals with severe periodontitis also had significantly higher medical costs of dementia than those with healthy periodontal tissue. There are many reports on the relationship between periodontal disease and dementia. 7,24 A study of patients with dementia reported that those with periodontal disease at baseline had more significant cognitive decline than those with healthy periodontal tissue. 7 Since periodontal disease increases the blood levels of C-reactive protein and tumor neurosis factor alpha, 25 it was suggested that systemic inflammation may increase the risk of dementia. Amyloid β is a major component of senile plaque, which is a pathological hallmark of Alzheimer’s disease, and amyloid accumulation has been reported to be associated with neuronal dysfunction. 26 Periodontal disease is associated with amyloid deposits, and a study of healthy older individuals showed that amyloid deposits were prominent in those with periodontal disease. 27 Experiments with mice have shown that a toxin produced by Porphyromonas gingivalis, the cause of periodontal disease, induced amyloid β production. 28 In the present study, the high medical costs of dementia for individuals with severe periodontitis may have been associated with an increased risk of dementia due to the effects of periodontal disease. Maintaining healthy periodontal status may contribute to the prevention of dementia and control the medical costs related to dementia.
Although smoking habits, vascular disease, and diabetes mellitus are known risk factors for dementia, 3,29,30 none were significantly associated with the medical costs of dementia in this study. This might be because there was no significant association between these factors and dementia since we analyzed the medical costs of dementia rather than dementia development.
This study has several limitations. Since the dental examinations of this study examined applicants who visited the dental clinic, these participants were likely those with a high level of interest in their oral health and in relatively good health. Indeed, a higher percentage of participants in this study had 20 or more teeth than the same age group in a national survey. 31 This suggests that there was selection bias, as our study participants were more likely to have good oral health compared to the overall older population. Therefore, the results of this study cannot be generalized to all older individuals. Because the information on BMI and medical history was based on questionnaires, there may be bias in the results. The data used in this study were based on the health examinations conducted as part of community health projects, and periodontal status was assessed using the CPI. As the CPI is a partial examination method, it may underestimate periodontal disease. The medical costs of dementia were based on the costs calculated for the main disease treated at each medical institution and, therefore, the costs of dementia were not recorded when another disease was the main disease. Therefore, the estimate is likely to be lower than the actual medical costs. In addition, socioeconomic status (i.e., economic conditions and education level) is a very important factor in conducting epidemiological researches related to health status because it affects health behaviors, including medical consultations. However, we did not obtain information on socioeconomic status in this study using data managed by a medical insurer. Therefore, future epidemiological studies should consider socioeconomic factors to clarify the effects of oral health status on medical costs.
In conclusion, the number of teeth and periodontal status were significantly associated with the medical costs of dementia. Preventing tooth loss and maintaining healthy periodontal condition may contribute to controlling dementia costs.
Footnotes
Authors’ Note
Individuals with many lost teeth have higher medical costs for dementia.
Individuals with severe periodontal disease have higher medical costs for dementia.
Maintaining oral health may contribute to controlling dementia costs.
Acknowledgments
I confirm that I have listed all coauthors contributed significantly to this work. We are very grateful to the participants in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI Grant Number 19K10429 from the Ministry Education, Science, Sports, and Culture of Japan, Tokyo, Japan.