
Abstract
Little is known about how individual behavioral and psychological symptoms of dementia (BPSD) impact the person with dementia. This cross-sectional, retrospective study examined the association between one BPSD, aggressive behavior, and a patient-identified outcome, sadness, among people with moderate and severe dementia (n = 5001) using clinical administrative Resident Assessment Instrument 2.0 data. For people with moderate or severe cognitive impairment, the odds of sadness were significantly higher if verbal aggression was exhibited 4 to 6 (adjusted odds ratio [aOR] = 2.85, P < .001) or 1 to 3 (aOR = 2.28, P < .001) times per week, or daily (aOR = 1.77, P = .003). People with severe cognitive impairment and who displayed physical aggression either daily (OR = 2.16, P = .002) or 1 to 3 times per week (OR = 1.45, P = .023) also had an increased odds of sadness. Aggression may harm the person with dementia’s mental well-being, depending on the level of cognitive impairment, and type and frequency of aggression. Prospective studies can build on these correlational findings.
Keywords
Introduction
Dementia describes syndromes of progressive cognitive impairment which affect memory and day-to-day function and is the leading cause of disability and dependence among older adults with chronic illness worldwide. 1 Behavioral and psychological symptoms of dementia (BPSD) affect an estimated 90% of people with dementia and their caregivers, 2 -4 and management of BPSD is a top priority for long-term care home research. 5
Behavioral and psychological symptoms of dementia are not one thing: they reflect a highly varied set of issues, including wandering, anxiety, delusions, aggression, and others. 6,7 Despite this variation, research has usually examined BPSD as a symptom or behavioral cluster measured as a mean score in a BPSD index. This is useful to capture a range of possible symptoms and behaviors, but problematic for understanding the causes and consequences of each BPSD. Each symptom may have different social and environmental causes 6,7 and distinct effects that could be identified by assessing individual behaviors and their specific associated outcomes. 8
Aggression is one BPSD that is particularly difficult to manage. 6 From the caregiver’s perspective, aggressive behavior can be highly distressing, 9,10 but little is known about the impact on the person with dementia as a consequence of their own aggressive behavior. Exploratory qualitative research suggests that aggression may directly affect sadness, from the perspectives of people with dementia, and this body of research was used to generate hypotheses to guide this study. 11,12
Literature Review: Aggression and Sadness
Little research has tested the hypothesized association of aggression and sadness. One study found that sadness predicted onset of physical aggression, but did not assess associations with verbal aggression. 13 A larger, related body of literature has tested the association of aggression and depression (related because sadness is one symptom of depression). 14,15 This literature does not directly reflect the specific hypotheses generated from previous qualitative research which guided this study, but it is important to review here given the dearth of research on aggression and sadness.
Hypotheses of why aggression and depression may be linked, and the results of studies that test these associations, are inconsistent. Cross-sectional studies support that aggression is associated with higher levels of depression, and the strength of association depends on whether the aggression is physical or verbal. 16 -20 Yet, a prospective study found that depression was only indirectly linked to aggression onset (ie, mediated by pain or caregiver burden). 21 Some posit that dementia causes depression and aggression. 13 Others suggest that depression may cause aggression. 19 Alternatively, research to capture perspectives of people with dementia suggests the reverse: that poor quality relationships, indicated by things like aggression, may cause sadness, 12 which could lead to depression. The present study builds on this latter proposition and tests how the association between aggression and sadness changes, depending on the type of aggression, and level of functional and cognitive impairment.
Conceptual Framework
Systematic reviews of over 40 qualitative research studies suggest that people with dementia perceive that feeling connected to others promotes quality of life 11,12 and prevents sadness. 12 In contrast, aggression that is verbal (eg, screams, cursing) or physical (eg, hitting, spitting) may reflect an experience of intense interpersonal conflict and disconnect from others. 11,12 People with dementia have described interpersonal conflict as increasing the risk of poor quality of life and sadness. 11,12 Level of cognitive impairment and functional dependence may change the association between aggression and sadness. When people become more dependent, they rely on other individuals to meet their needs. Experiencing conflict with people one relies upon may have particularly harmful effects for the person with dementia. 12
Purpose
The purpose of this study was to evaluate the associations of verbal and physical aggression with sadness for long-term care residents with moderate and severe dementia. The primary hypothesis was that frequent verbal and physical aggression would be associated with higher odds of sadness. By testing interaction terms (ie, effect modifiers), the influence of cognitive impairment, functional dependence, and type of aggression upon these associations was also explored.
Design and Methods
Sample
This is the second report from a cross-sectional, correlational analysis of clinical administrative data. 22 There was a complete sampling frame available of the 18 400 people with dementia who lived in Ontario long-term care homes. 23 At least 4840 residents were needed to detect a small (ie, OR = 1.3), statistically significant finding with 80% power (given α = .05, aggression prevalence = 15%, and sadness prevalence = 20%). 24
De-identified data from annual (April 2012 to May 2013) Resident Assessment Instrument (RAI 2.0) evaluations were obtained from the Canadian Institute for Health Information. Staff at each facility complete quarterly RAI 2.0 assessments for each resident, which involves medical record review and observation. Facility managers determine who should complete the assessment but must ensure that those involved have the necessary knowledge and contact with the resident in order to complete the assessment accurately. RAI 2.0 assessment is most often lead by a health care professional like a registered nurse or social worker and involves discussion with other members of the interdisciplinary team and family and friends of the resident. 22 Evidence supports interrater reliability and consistency and criterion, convergent, and predictive validity of the RAI 2.0. 23,25 -28 The random sample included 5324 Ontario long-term care home residents who had lived at a facility for at least 3 months, were older than the age of 65, and who had a dementia diagnosis. People who were comatose or who had a current psychiatric condition (ie, depression, anxiety disorder, manic depression, or schizophrenia) were excluded. After data acquisition, additional exclusions were people with mild dementia (n = 318) and who were of ‘other’ sex (n = 5). These groups were excluded because the small numbers of each created empty cells when testing interaction terms and in the sex-adjusted model.
Independent Variables: Aggression
Verbal (ie, threaten, scream, or curse at others) and physical (ie, hit, shove, scratch, or sexually abused others) aggression are measured in the RAI 2.0. A RAI 2.0 assessor observes and consults with direct care staff to record the frequency of aggression directed at other residents or staff in the last 30 days. The usual weekly frequency from 0 to 3 is recorded: not exhibited = 0, or occurred on 1 to 3 days = 1, 4 to 6 days = 2, or daily = 3. Interrater reliability (r = 0.95) and κ (0.84) were high for a problem behavior index, which included verbal and physical aggression, in previous research. 29
Dependent Variable: Sadness
The dependent variable, sadness, was operationalized with 3 RAI 2.0 items. These are similar to the items included specifically to measure sadness (as opposed to other symptoms of depression) from a validated depression screening tool 30 : (1) negative statements; (2) sad, pained, worried facial expression; and (3) crying/tearfulness. Weekly frequency over the last 30 days is scored from 0 to 2: not exhibited = 0, or occurred on 1 to 5 days = 1, or ≥6 days = 2. 31
It is unknown if any sadness indicator (eg, crying vs sad expression) reflects more or less sadness, so a dichotomized variable was used for the analysis (ie, any weekly expression of sadness = 1 or none = 0). Previous research supports the interrater reliability (r = 0.89) for sadness items (contained in a mood index) and an acceptable κ value (0.56). 29
Adjustment Variables
The reason for sadness was not available in this data set. However, a number of other variables which may affect the association between aggression and sadness identified in a comprehensive review of the literature 32 were available and were adjusted for in the analysis. Cognitive impairment (Cognitive Performance Scale) 33 and functional dependence (Activities of Daily Living-Hierarchy Scale or ADL-HS) 34 were tested as effect modifiers. Cognitive Performance Scale scores were categorized based on correspondence with average Mini-Mental State Examination ratings found in previous research 33,35 : mild impairment = 0 to 1, moderate = 2 to 3, and severe = 4 to 6. To prevent empty cells, the 7-category ADL-HS variable was dichotomized into clinically relevant categories: 0 to 2 reflected relatively independent to limited impairment, and 3 to 6 reflected extensive help to severe or total dependence. Other potential confounding variables selected from the comprehensive review of the literature 32 were also measured with RAI 2.0 data: age, sex, education, length of stay, hearing impairment, vision impairment, daily visits from family/friends prior to admission, lack of current visits from family/friends, pain, and use of psychopharmacological medications (operationalized as any use of antipsychotic, antianxiety, antidepressants, or hypnotics in the last 7 days).
Analysis
STATA 13 was used for analysis. There were no missing data. Box plots or frequency tables were used to assess variable distributions. Descriptive statistics (means/standard deviations or proportions) were calculated and checked for small cell counts using cross-tabs.
Nonstepwise, purposeful logistic regression model procedures were used to derive the model. 36 The final model contained: (1) independent variables of verbal and physical aggression, (2) confounders of clinical or theoretical importance, (3) confounders statistically significant in bivariate analysis (at a conservative P ≤ .20 to avoid premature exclusion of adjustment variables) that affected the aggression-sadness associations by more than 15%, and (4) statistically significant interaction terms (P ≤ .05). All models were adjusted for within-facility correlation using the “cluster” command in STATA. The Hosmer-Lemeshow test result (probability > χ2 = 0.281) was nonsignificant, indicating that the model fit the data. Age, the only continuous variable in the model, did not meet the linear assumption. It was broken into quartiles and included in the model as a categorical variable. Psychopharmacologic medication use variables (from 0 to 7 days) resulted in small cell counts, which can bias estimates, and were dichotomized into use versus nonuse for each specific medication type. Multivariable logistic regression is the correct analysis for the current study but produces odds ratios (ORs) which can be less intuitive than and overestimate the prevalence ratio, when the initial prevalence of the outcome is high. 37 To support clinical interpretability of the findings, the ORs in the final model were also converted to prevalence ratios using a formula for use in situations where the prevalence of the outcome of interest is >10%. 38
Ethical Approval
The Human Research Ethics Board at the University of Alberta approved this study [Pro00011753_CLS9]. Canadian Institute for Health Information procedures were followed for data storage and security.
Results
Sample Characteristics
The sample was 5001 people with moderate and severe dementia from 613 (of a possible 683) Ontario long-term care homes. 23 The mean age was 86.3 years (standard deviation: 7.03), and the majority (72.1%) were female, experienced sadness (58.5%), and had moderate cognitive impairment (55.1%; Table 1). There were between 1 and 41 residents from each of the 613 facilities.
Sample Characteristics.

Abbreviation: SD, standard deviation.
Unadjusted Results
All independent variables and potential confounders were assessed for their association with sadness when entered alone in a logistic regression model. Age and hypnotic use were the only variables not statistically significant (P ≤ .20) in bivariate analysis but were both retained for the confounder analyses to be conservative as they did not complicate the analysis and because age was of clinical significance. All categories of both verbal and physical aggression were statistically significant (P ≤ .05) in bivariate analysis (Table 2).
Bivariate Results: Odds Ratio (OR), 95% CI, and P Value for Independent Variables When Entered Alone in a Logistic Regression Model.

Abbreviation: SE, standard error.
a Standard errors adjusted for clustering within 613 long-term care homes.
Effect Modification
Cognitive impairment modified the association between physical aggression and sadness for those who exhibited daily physical aggression (P = .021). Functional dependence did not modify the association between physical aggression and sadness (ie, the P values for the interaction terms were >.05). The association of verbal aggression and sadness also remained the same, regardless of level of cognitive impairment or functional dependence.
Adjusted Results
None of the proposed confounding variables affected the aggression-sadness associations by more than 7%, so adjustment was made only for those of clinical (age, sex, pain) or theoretical (cognitive impairment, functional dependence, current contact) importance. Given the significant interaction term, adjusted ORs are reported by type of aggression (verbal or physical), frequency of aggression (1-3 days, 4-6 days, or daily), and level of cognitive impairment (moderate or severe; Table 3).
Odds Ratio (OR), Adjusted Prevalence Ratio (PR), 95% CI, and P Values for Independent Variables (Reference = Not Exhibited) in a Multivariable Logistic Regression Model, Adjusted for Covariates.a

a Adjusted for age, sex, functional dependence, level of cognitive impairment, pain, and contact with family/friends.
b Robust standard errors adjusted for clustering within 613 long-term care homes.
c Based on PR = OR/(1 − P0) + (P0 × OR), where PR = prevalence ratio, OR = odds ratio, and P0 = the prevalence of the outcome (ie, sadness) in nonexposed patients (Zhang and Yu 38 ).
d P ≤ .001.
e P ≤ .05.
f P ≤ .01.
There was a higher odds of sadness for people who were verbally aggressive as compared to those who did not exhibit verbal aggression, regardless of level of cognitive impairment. The odds of sadness were highest for those who were verbally aggressive 4 to 6 times per week (OR = 2.85, P < .001) or 1 to 3 times per week (OR = 2.28, P < .001) and lowest among people who were verbally aggressive daily (OR = 1.77, P = .003). Converting the ORs to prevalence ratios: the prevalence of sadness among those who did not exhibit verbal aggression was 54% and was 1.43, 1.35, or 1.25 times higher for those who were verbally aggressive 4 to 6 times per week, 1 to 3 times per week or daily, respectively (Table 3).
The physically aggressive with moderate cognitive impairment had the same odds of sadness as those who were not physically aggressive. However, people with severe cognitive impairment, and who were physically aggressive, had higher odds of sadness as compared to the not physically aggressive. The odds of sadness were highest for those with severe cognitive impairment who were physically aggressive daily (OR = 2.16, P = .002) and lower for those physically aggressive 1 to 3 times per week (OR = 1.45, P = .023) or 4 to 6 times per week (OR = 1.45, P = .081, borderline significant). The prevalence of sadness among those with severe cognitive impairment and who did not exhibit physical aggression was 73% and was 1.17 or 1.09 times higher among those with severe cognitive impairment who were verbally aggressive daily or 1 to 3 times per week, respectively.
Discussion and Implications
The large literature on BPSD has to date focused much attention on the impact of aggression as part of a cluster of behaviors and symptoms on caregivers 39 or caregiving approaches to manage BPSD. 40 This study extended the literature on BPSD to assess the potential impact of a specific BPSD, aggression, on sadness for people with dementia. Hypotheses of associations of other BPSDs with outcomes that matter to people with dementia should be generated, and qualitative research is essential to this agenda. 32
The focus of this study was to quantify the association(s) of an individual BPSD (aggression) with an outcome (sadness) identified from the perspectives of people with dementia. Quantifying associations and identifying effect modifiers, like cognitive impairment and type of aggression, provides the foundation to design prospective studies to establish temporality. The findings also have implications for practice. Results identify subgroups of people with dementia at risk of poor mental health. Clinicians can identify individuals at risk based on the clinical assessment (ie, RAI) data collected as a part of routine practice in long-term care settings across North America. The highest odds of sadness occurred among people with moderate or severe cognitive impairment who were verbally aggressive up to 6 times per week and for those with severe cognitive impairment that were physically aggressive everyday. The findings of the present study align with a meta-analysis on the factors influencing loneliness for older adults that showed that the quality of one’s relationships was at least as important as the quantity of relationships to support well-being. 41
Those exhibiting daily verbal aggression had a lower odds of sadness than people who were verbally aggressive up to 6 times per week, an unexpected finding. In the case of daily physical aggression, there was a statistically significant increase in odds of sadness only among those with severe cognitive impairment. These patterns (see Figure 1) may be explained by people with dementia’s use of nonverbal communication to express their needs as cognitive function deteriorates. 42 -44 People with moderate cognitive impairment may react to a perceived conflict with verbal aggression, while the communication impairment typical of severe dementia may lead to physical aggression in response to conflict.
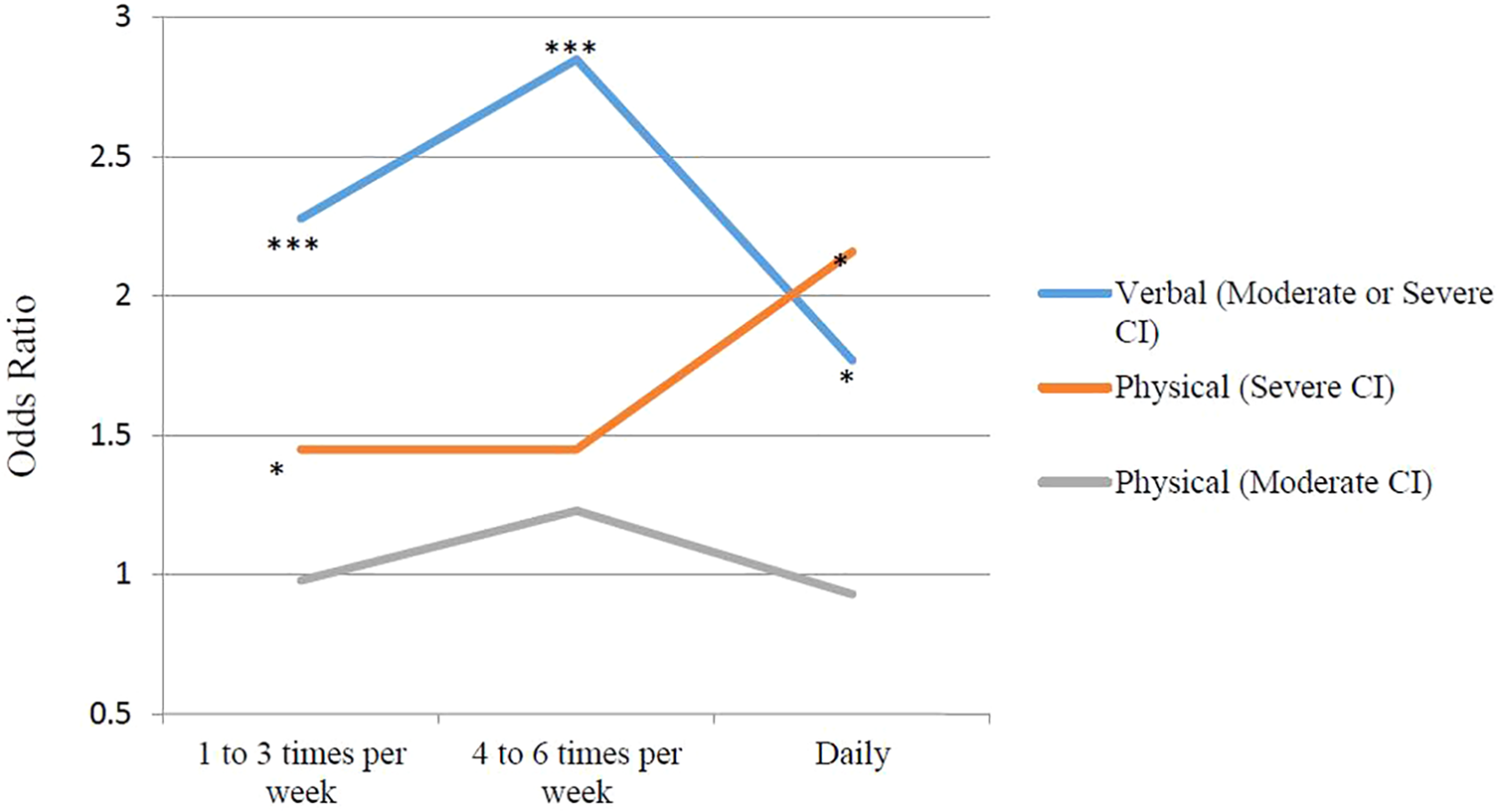
The odds of sadness according to the frequency of aggressive behaviors and level of cognitive impairment. CI, cognitive impairment. ***P ≤ = .001; **P ≤ = .01; **P ≤ = .05. No asterisk indicates a finding that is not statistically significant.
Health care providers find it more difficult to communicate with the person as dementia severity and communication impairments increase. 45 Careful and empathetic interaction with people with dementia is needed to prevent aggressive conflict and subsequent harm to the person with dementia. Health care providers can identify those who display aggressive behavior and seek opportunities to support the person with dementia to experience more positive interpersonal interactions. Research is needed to design and evaluate interventions to address aggressive conflict, tailored to the person’s level of dementia severity, and type and frequency of aggression.
Strengths and Limitations
The study sample was large and representative of Ontario long-term care home residents who may also be similar to residents in many other jurisdictions. Important covariates were adjusted for, as well as within-facility correlation resulting from residents living in the same long-term care home. Limitations of this study include that people with mild dementia were excluded and the cultural background of participants was not known. We suggest using stratified random samples to test the hypotheses in groups with mild dementia and from other cultural backgrounds and jurisdictions. A final limitation is that the measures of aggression that we used did not differentiate between aggression directed toward staff, other residents, or family; who conflict occurs with may affect the association with sadness. 12,22
Conclusion
Verbal aggression and physical aggression were associated with higher odds of sadness. The odds of sadness was the highest for those with moderate cognitive impairment who exhibited verbal aggression less than daily, and for those with severe cognitive impairment who were physically aggressive every day. Future research should include prospective studies to test the temporal nature of the aggression–sadness relationship. Longitudinal studies are needed to assess how aggression and sadness may predict depression.
Footnotes
Authors’ Note
Coauthors made equal contributions to the manuscript.
Acknowledgment
Parts of this material are based on data and information provided by the Canadian Institute for Health Information. However, the analyses, conclusions, opinions, and statements expressed herein are those of the authors and not those of the Canadian Institute for Health Information.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article: This work was supported by Knowledge Translation Canada; Alberta Innovates Health Solutions; University of Alberta Killam Trusts; and the Vanier Canada Graduate Scholarships Program [all trainee stipend support to the first author].