
Abstract
Objective:
To investigate the dementia knowledge and care approach used by caregivers in residential aged care facilities (RACFs) in China.
Method:
A cross-sectional survey of 785 caregivers from a random sample of 34 RACFs in China. Caregivers’ knowledge and care approach were assessed using the Chinese version of the Dementia Knowledge Assessment Tool 2 and Advanced Dementia Care Questionnaire.
Results:
The majority of caregivers showed limited knowledge of dementia and tended not to adopt a person-centered approach to care. Educational level, dementia care training, and years of work experience were positively associated with dementia knowledge. Educational level and years of work experience were also associated with a person-centered approach to care.
Conclusions:
This study provides insight into the care available to people with dementia in RACFs in China. The results suggest dementia care education programs as well as person-centered care training are urgently needed for caregivers in China.
Background
It is estimated that more than 9.5 million people live with dementia in China—20% of the total number of people in the world with dementia. By 2030, it is expected that more than 16 million people will be living with dementia in China. 1 Taking care of the increasing number of people with dementia is an urgent concern in China and places great pressure on both the families of the person with dementia and the health system.
In order to address the care needs associated with the increasingly aging population, the Chinese government established 3 tiers of services for people with dementia: home care as the “basic” level of care, community-based services as “backing,” and residential aged care facilities (RACFs) as “support.” 2 Institutionalized care of people with dementia is still stigmatized by Chinese society due, to some extent, to the Confucian philosophy of “filial piety” that supports a tradition of family-based care for the elderly individual as the default form of care. 3,4 However, with the changing socioeconomic and demographic structure of Chinese families resulting from the one-child policy, 2,5 the increased internal migration for employment and the improved social status of Chinese women in the workforce (who were traditionally housewives in previous years 3 ) have made it impossible to continue to rely exclusively on family care. 6 In practice, the availability of home and community-based support is limited and government policy efforts have focused on increasing the availability of RACFs 7 and have promoted RACFs as a smart strategy to meet the demand of caring for people with dementia. 2 The rapid growth of the elderly population has resulted in an exponential growth in the number of beds in RACFs between 1990 and 2012 (from 735 000 to 4.2 million). 8
The increasing number of RACFs has exposed a number of shortcomings in the caring for residents. Given the recent innovation of RACFs in China, management expertise are limited and few managers or staff have skills or experience in health, aged or social care, or public health management.
Few RACF organizations understand the objective of providing holistic care for elders. Although “taking care in daily life” is considered the main task of the RACFs, few have employed health professionals or staff who are trained in the care of the elderly individual and people with dementia. The majority of caregivers are from rural areas. Research has demonstrated that the lack of qualified caregivers in RACFs is one of the most urgent problems in China. 9 Hao et al investigated the current dilemmas of nursing homes in Chengdu and found that the majority of caregivers were farmers (58.1%) or laid-off or retired workers (38.7%) and that 98.5% of caregivers had an education level of junior middle school or less. 10 In addition, the vast majority of caregivers are inadequately trained. The Chinese government policy requires aged care workers to receive a minimum of 12-week certified training before engaging in caring for elders. 5 Some RACFs ignore this requirement due to lack of financial support. Some caregivers are unable to take training courses because of heavy workloads. A survey conducted in 141 RACFs in Tianjing reported that 57.4% direct caregivers had not received any professional training program. 11 Dementia-specific training is not always a component of basic or continuing elderly care education programs.
An adequate level of knowledge of staff, underpinned by safe and evidence-based care practices, is the most important factor that affected the quality of care for people with dementia. 12 Early theories in psychology, such as the Theory of Planned Behavior, suggests that beliefs/knowledge influence attitudes and attitudes influence intentions and actions. So, caregivers with a higher level of dementia knowledge are better equipped to care for people with dementia and are more likely to employ a person-centered dementia care approach rather than reality-orientated care approach compared to those with poor dementia knowledge and attitudes. 13 The effectiveness of person-centered care on people with dementia has already been demonstrated by many researchers in developed countries. Caregivers who adopt a person-centered approach to providing care are better able to perform activities of daily living and provide a higher quality of nursing support. 14 -17 Person-centered interventions can reduce agitation, neuropsychiatric symptoms, and depression and improve the quality of life of patients with dementia. 14 -17 However, a reality-oriented care approach is more likely to give staff a sense of “doing something” for people with dementia and the whole care process focuses on the communication of instructions and information instead of human interaction. Furthermore, constantly attempting to reorientate people with dementia about time/place/person may remind them of an intolerable reality, which can lead to frustration, depression, anxiety, a lowering of self-esteem, and provoke anger and misery. 18
Taking care of elderly people in residential facilities is still an undeveloped care option in China. 19 The capability of people caring for residents with dementia in RACFs is questioned. 11 In order to know more about the situation of dementia care in RACFs in China, as well as to enhance the quality of dementia care, it is essential to first assess the extent of caregivers’ knowledge about dementia and the extent to which a person-centered care approach is adopted. No previous research has explored the capability of caregivers in RACFs in China to adequately provided appropriate care for people with dementia. This study aimed to assess the RACF’s caregivers’ knowledge of dementia care and their approach to providing care for people with dementia in China.
Methods
Study Design
A cross-sectional survey of Chinese frontline caregivers in 34 RACFs in 4 different levels of cities was conducted to explore dementia knowledge and care approach between March and October 2018.
Sample and Setting
The quality and the extent of health care in different cities in China are closely related to the level of development of the city. Cities in China are classified by tiers according to the economic strength, political and cultural status, and industrial development level. “First-tier” cities have lager populations, have higher levels of education, and are more technologically advanced than lower tier cities. In 2018, there were 5 first-tier cities, 30 second-tier cities, 60 third-tier cities, and 107 fourth-tier cities.
In order to fully understand the dementia knowledge and care approach of caregivers for people with dementia, RACFs were sampled through a stratified cluster sampling process. First, one city was selected randomly from each of the 4 different levels of cities. Second, one RACF was randomly chosen from each administrative region of the 4 selected cities using a random number generator. Third, all of the frontline caregivers employed by the selected RACFs were invited to participate in this study. The characteristics of the RACFs that participated in this study are displayed in Table 1.
Characteristics of Residential Aged Care Facilities (RACFs) That Participated in the Study.

Participant Recruitment
Managers of RACFs were contacted by authors Y.Y.D., S.M.L., and C.C.Z. to invite their organization to be part of the study. To promote participation, a token payment of $35 was offered, in recognition of the time involved. Questionnaires were mailed to the RACF managers who distributed the questionnaires to the caregivers and returned the completed questionnaires to the research team.
Measurements
Demographic Data
Demographic data collected from RACFs staff include age, gender, education level, the length of caring for people with dementia, and dementia care training.
Dementia Knowledge Assessment Tool 2
The Dementia Knowledge Assessment Tool 2 (DKAT2) was developed to evaluate foundation-level knowledge of the dementia trajectory and care in aged care staff, family carers, and care worker. 20 It contains 21 items. Each correctly answered item is awarded 1 point. Incorrect statements or “don’t know” statements receive 0, the total score can range from 0 to 21. The Cronbach α of the Chinese version of DKAT2 is .70, demonstrating good internal validity. 12 Compared with other dementia knowledge tools, this tool is much easier for caregivers to understand and finish since a majority of Chinese caregivers in the RACFs is with a low level of education.
Approach to Advanced Dementia Care Questionnaire
The Approach to Advanced Dementia Care Questionnaire (ADCQ) was used to assess participants’ approach to care for people with dementia. 21 This questionnaire presents a background scenario of a woman with severe dementia and bizarre behaviors. It includes 13 sets of statements, and 5 indices were constructed: (1) orientation of time, place, and situation (statements 1, 3, 5); (2) correction of behavior (statements 2, 7, 11); (3) emphasis on the past or the present(statements 4, 9, 12); (4) the aim of communication (statements 6, 10, 13); and (5) and whether confusion had any meaning for the patient (statement 8). Each set includes 2 statements, one is based on a reality orientation and the other is on a personhood-focused approach. The reality-oriented approach answer earned a score of 0, whereas the person-centered answer earned 1 point. The total score range is 0 to 13, with a higher score indicating greater tendency to employ a person-centered care approach. The original English questionnaire was translated into Chinese and then back-translated, with the Chinese version finalized after comparing the 2 versions. The content validity index was 0.92 for description clarity and 1.00 for relevance of questions and concept based on the input of 3 experts. Twenty-nine nurses who participated in a pilot study responded to a revised version of the questionnaire, which earned a Cronbach α is .60. 12
Statistical Analysis
All analyses were conducted using SPSS (version 22.0) software (IBM Corp). Descriptive analyses were used to describe DKAT2 and ADCQ scores and sociodemographic data. The independent-sample t test and Pearson correlation analysis were used to measure differences in the DKAT2 and ADCQ scores between participants with different sociodemographic characteristics. Multivariate regression with “stepwise” selection procedure was employed to explore the net effect of independent variables on the DKAT2 and ADCQ scores. Statistical significance was based on P value <.05 in 2-tailed tests.
Results
Participants’ Characteristics
Of the 785 questionnaires administered, 735 questionnaires were returned (response rate is 93.6%). Demographic characteristics of RACFs caregivers are displayed in Table 2. The majority of participants were female. Mean age was 49.8 years (range 31-67 years). The longest any participants had worked in caring for patients with dementia was 18 years. Some caregivers (12.3%) were unwilling to undertake any dementia care training courses, the main reasons being they were too old or lacked the ability to gain new knowledge.
Demographic Characteristics and Their Relationship to the Dementia Knowledge Assessment Tool 2 (DKAT2) and Advanced Dementia Care Questionnaire (ADCQ).

a Statistic was based on Pearson correlation analysis.
b Statistic was based on independent-samples t test.
Dementia Knowledge Assessment Tool 2 Scores
The mean dementia knowledge score of all participants was 13.1 (SD = 2.37, range 6-19) of 21 (equivalent to a mean score of 62.2%). Items with the lowest scores included those related to pathophysiology (items 3, 5, 6, and 7) and symptoms (items 8 and 12). Only 34.7% of participants knew that Alzheimer is the main cause of dementia, with some indicating they do not know what “Alzheimer” is. More than half of participants were unaware that patients with dementia have their own psychological activity and sensory perception, with 52.4% answering incorrectly that changing environment makes no difference to the person with dementia and 60.4% answering incorrectly that it is possible to tell if in pain (Table 3).
Percentage of Correct Responses to Dementia Knowledge Assessment Tool 2 (DKAT2) Items.

Approach to ADCQ Scores
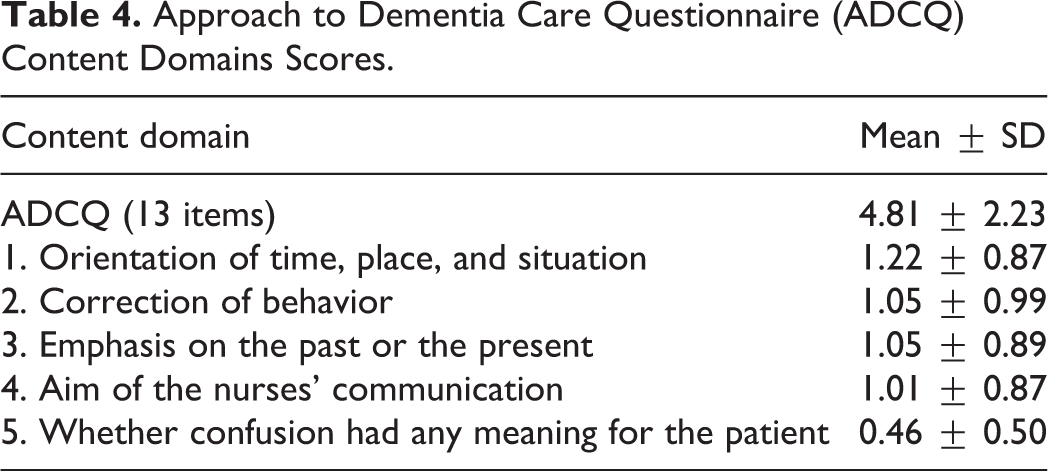
The overall mean ADCQ score of RACF caregivers was 4.81 (SD = 2.23, range 0-11) of a possible 13. Almost three-quarters (73.7%) of participants thought they should correct the patient’s behavior and tell her what she ought to do, and 66.9% considered today’s reality is important for Ms N.N. She should, therefore, be reoriented to time, place, and situation. Less than one-third (30.7%) of staff thought the aim of communicating with the patient with dementia should be to stimulate her feelings connected to the past. Participants were more likely to employ reality orientation care approaches instead of person-centered care approaches (Table 4).
Approach to Dementia Care Questionnaire (ADCQ) Content Domains Scores.
Caregivers who had higher education demonstrated higher dementia knowledge score and were more likely to employ a person-centered approach to care (P < .001), as did participant who had longer work experience in caring for people with dementia (Table 2). A weak correlation was found between dementia knowledge scores and person-centered care scores (r = 0.146, P < .001).
Predictors for the Dementia Knowledge and Approach to Dementia Care
Variables (age, gender, educational level, cities, years of caring for patients with dementia, dementia care training experience) were stepwise entered as independent variables in the 2 separate multiple linear regression models. Educational level, years of caring for people with dementia, and RACFs in different level of cities were predictors of the DKAT2 scores (F = 39.92, P < .001) and the ADCQ scores (F = 12.41, P < .001), explaining 14.1% of the total variance in dementia knowledge and 5% of the total variance in person-centered approach care (Table 5).
Multiple Regression Analysis for the Knowledge Assessment Tool 2 (DKAT2) and Advanced Dementia Care Questionnaire (ADCQ; n = 735).

Abbreviation: RACFs, residential aged care facilities.
Discussion
This is the first study of RACFs caregivers’ knowledge and approaches to the care of people diagnosed with dementia in China. It is essential to understand the capability of caregivers in caring for people with dementia so that appropriate policies and education programs can be designed and implemented in RACFs to ensure that the increasing number of people with dementia in China are cared for appropriately. The study found that caregivers do not have adequate knowledge of dementia and a person-centered approach to care.
Caregivers in China reported lower levels of knowledge than their counterparts in several other countries. The mean DKAT2 scores (M = 13.1) is lower than those caregivers reported in Spain (M = 15.57), 22 the United States (M = 14.0), 20 and Australia (M = 15.87) 23 as well as Australia nursing students (M = 14.51). 24 These differences may reflect that the vast majority of RACF caregivers in China have a lower educational background. Our study found that education level has a positive relationship with RACF caregivers’ dementia knowledge.
A national RACFs survey conducted in the United States reported that 13% of RACFs’ staff were registered nurses, 20.1% were licensed practical nurses, and 65.5% were certified nursing assistants. The majority of certified nursing assistants (87.1%) had a high school diploma or general equivalency diploma, 25 while 75.2% of caregivers in our study had only a middle school or less education. The result is consistent with other Chinese research, which found that more than 80% of RACF caregivers were illiterate or semi-illiterate. 10,11
An important contributing factor to the lower level of knowledge about dementia among RACF caregivers in China could be the limited availability of dementia-specific continuing education programs. Dementia care is not yet integrated into the medical and nursing baccalaureate curricula in China and is not always provided by training centers that focus on elder care. 13 Lack of government regulation and mandated education may also have contributed to the poor access to training in this field. 11 One-third (32.9%) of caregivers in our study never received dementia care training courses. Previous research in China found that more than half (52.7%) of RACF staff never received dementia care training. 10,11
The establishment and use of RACFs as an option for elder care in China is an emerging innovation. Policies and regulation for their development, management and functioning, and the development of standards for care are yet to be established. A systematic approach to the development and implementation of policies for the management of RACFs is needed, and regulations about minimum qualifications for caregivers should be established and monitored. In the early development of this care model, government-directed/administered education programs may need to be a preemployment requisite and continuing education programs monitored to ensure high-quality care for this vulnerable population.
Person-centered care is a holistic alternative to conventional care practices and is considered a core component of dementia care competence. 13 It is well recognized, both in China and internationally, that person-centered care enhances the quality of life and well-being of people with dementia 16,17 as well as effectively reducing dementia-compromised behaviors such as agitation and helps maintain the dignity and personhood of the individual. 14 However, we found that caregivers were less likely to implement person-centered care in dementia care. The concept of person-centered care is still not well understood in health care in China. “Person-centeredness” and “patient-centeredness” are frequently regarded as the same in China; therefore, there is no specialized education in person-centered care in China. 26 Both an educated care team and advanced organization management are essential requirement for implementing person-centered care. 13 Low staffing levels, lack of knowledge, and lack of financial support for RACFs in China all contribute to the difficulties encountered by RACFs in providing person-centered care. Our study found that the longer caregivers had worked in dementia care and the better educational background, the higher likelihood that caregivers used a person-centered approach. Lin et al 12 and Wang et al 27 also found that work experience and education level influenced caregivers’ approach for people with dementia.
Residential aged care facility caregivers in our study who were employed in services in the higher tier cities demonstrated higher levels of knowledge about dementia care and a person-centered approach. These findings support a commonly held belief that people living in more advanced cities receive better education as well as better health care than their counterparts in less developed areas. To help overcome such disadvantage, government assistance may be required to enhance health care education for the primary/community health care sector of the less developed cities. To further promote a more contemporary, holistic aged care sector, RACFs must also contribute to the ongoing education and integration of a person-centered approach to care into daily practice.
Study Limitations and Future Research Directions
Although our study has a large sample and high response rate, there are a number of limitations to its generalizability to all of China. First, the study was conducted only in urban areas. As a consequence, the findings may not reflect the RACFs in the rural areas. Second, there was a considerable amount of variance of knowledge and care approach that cannot be explained by the sociodemographic characteristics, dementia care training experience, and experience in dementia care. The multivariate regression models need to be improved to better explain the level of knowledge and care approach in future studies. For example, person-centered training programs in dementia care would be included in the future to develop a predictive model that explains more of the variance.
Conclusion
This study reveals that RACF caregivers in urban China have limited caregiver dementia knowledge and poor knowledge of a person-centered approach in dementia care. In the context of an increasing number of people with dementia and a rapidly aging population in China, the option of RACF care is one important strategy to ensure that members of this vulnerable population receive appropriate care. However, to ensure such care is safe, effective, and optimizes quality of life and well-being, there is an urgent need for qualified RACF staff with the relevant knowledge and understanding of the needs of this population. To promote this level of expertise, dementia care training programs to all RACF caregivers prior to employment and continuing education should be accessible and promoted by all nursing care facilities.
Footnotes
Authors’ note
Ethical approval was granted by Human Research Ethics Committee of Guilin Medical University (project number 20180713). All participants received written information about the aims of the study and that participation was voluntary. Completion and submission of the questionnaires was regarded as implied consent.
Acknowledgments
The authors would like to express their appreciation to all the participants who took part in this study, as well as the managers or the leader of the 34 nursing homes who contributed to this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Guangxi Young and Middle-aged Teacher Promotion Project Grant (ref# 2017KY0493). Yunyun Dai is supported by a China Scholarship Council Scholarship (ref#201810006).