
Abstract
Objectives:
Dementia Care Mapping (DCM) is an established practice method to implement Person-centred Care in dementia care settings. However, it is not easy to carry out DCM because of its high complexity. The aim of this study is to solve DCM complexity by adopting technology.
Methods:
Authors developed (1) a new information-communication technology (ICT) based DCM support system based on the investigation of difficulties and/or burden encountered during mapping (n = 33) and (2) a new evaluation test method, using role-play videos, for assessing the usefulness and reliability of the system. Mapping data, collected using the support system or the conventional paper-based DCM (n = 22), were compared.
Results:
We obtained users’ positive ratings of the system for burden reduction and its usability. Moreover, the developed prototype system indicated to have already reached the level of conventional paper-based DCM in terms of mapping accuracy.
Conclusion:
Usefulness of the ICT-based support system was confirmed to help overcome DCM complexity.
Keywords
Introduction
Among several methods attempting to look at quality of life of older people with dementia, 1,2 Dementia Care Mapping (DCM) 3,4 was developed aiming at implementing Person-centred Care 5 in formal dementia care facilities. Dementia Care Mapping is a developmental evaluation system through which care quality is observed and fed back to care staff team for developing better care practice via its repetitive cyclic process (Figure 1). The feature of DCM is to promote an understanding of care practice from the viewpoint and personal experience of people with dementia, 5,6 which is represented by mappers. Hence, mappers play a very important role in DCM.

General framework of DCM; the developmental evaluation system. DCM consists of 5 stages: (1) Observers (mappers) give a briefing to staff on the purpose and the total process; (2) mappers conduct observation and collect structured data; (3) mappers analyze and evaluate the data and make summary documents; (4) selected summaries are fed back to staff teams to share good practices and areas for development; (5) staff team works with mappers to develop action plans for care improvement. Then, the staff team implement the action plan aiming to deliver better-quality Person-centred Care. DCM indicates Dementia Care Mapping.
Dementia Care Mapping is a well-developed method, which is standardized in the United Kingdom, 7 and has been used successfully worldwide for over 20 years. 8 -12 However, recent randomized controlled trials (RCTs) of DCM have reported mixed results on efficacy and indicated that process and implementation issues are potential factors to explain the differences in the results. 13 -15 To explore the issues, Surr et al 16 conducted a systematic review to examine the primary research evidence on the processes, barriers, and facilitators to implementing DCM. They pointed out that, from the relatively little evidence available on how the approach was applied in practice, appropriate manager support and adequate staffing were essential to successful implementation of DCM. They also conducted an RCT for evaluating the effectiveness and cost-effectiveness of DCM based on the study protocol. 17 During the process evaluation conducted as part of the RCT, Griffiths et al 18 identified the barriers and facilitators to DCM implementation at the mapper level (eg, motivation and confidence), the intervention level (eg, understanding of DCM), and the care home level (eg, staffing issues, manager support). It was highlighted by these studies that good understanding and strong support by managers and staff were quite important for successful implementation of DCM; however, it is all the same that mappers are required to play an extremely important role.
To become a mapper requires attendance at a DCM training course licensed by the University of Bradford to gain a good understanding of the method. However, it happened to some mappers that they could not explain properly to make managers/staff have full grasp of what DCM was all about, even right after the training. 18 Also reported was that a few weeks delays between the training completion and their first DCM trial led to them forgetting the details and losing their confidence. 18 The most complex process involved in DCM is the observational method, and its complexity is likely to account for posing issues at both the mapper and the intervention levels. The authors think it is possible to solve the complexity by utilizing technology; thereby, mappers can make best use of their ability of observing people with confidence, without concerning for the complex method. Schematic explanation, often used in engineering, may also provide easier understanding of DCM, as described in “Methods” section.
Hence, we have set the goal of this study to make it easier for mappers to carry out DCM by utilizing Information-Communication Technology (ICT). First, we investigated what difficulties and/or burden mappers had experienced during mapping by questionnaires. Based on the responses from 33 mappers, we have developed an ICT-based DCM support system and implemented it on a tablet PC (Figure 2). We also developed a new evaluation method for the support system using role-play videos and assessed the usefulness and reliability of the support system by 22 mappers (subjects).

Graphial user interface (GUI) of the developed DCM support system with handwritten notes. DCM indicates Dementia Care Mapping.
In this article, we report on the usefulness of the developed support system and discuss its reliability, potential for increasing mapping accuracy, extendibility, and limitations. This study is based on DCM 8, the latest edition of DCM published in 2005. 4 To the best of our knowledge, there is no research published to date concerning development of ICT-based DCM support systems except our study. 19
Methods
Development of the ICT-Based Support System for DCM
The DCM observational method is described elsewhere. 8,20 Because the method is complex, the explanation tends to be lengthy, typically starting with something like “A mapper observes to evaluate quality of care services by tracking 5 elderly people with dementia (participants) continuously over a representative period (eg, 6 hours during the waking day) in communal areas of care facilities.”
The authors made schematic explanations (Figures 3 and 4) to provide a clear picture of the method for clarifying the complexity that imposes difficulty on mappers, as well as to emphasize the necessity of a support system for DCM. As shown in Figure 3, a mapper observes the participants’ activities and their state of well/ill-being (WIB), using (1) the Behavior Category Code (BCC) and (2) the Mood and Engagement value (ME value). The BCC describes 1 of 23 different domains of participant behavior. The ME value describes the participant’s mood state alongside their level of engagement with their environment, being expressed on a 6-point scale ranging from −5 to +5. After each 5-minute period (time frame), a mapper records what has happened to each participant during the time frame. When 2 or more behaviors occur within one time frame, a mapper decides what BCC to record by following (3) the DCM operational rules (Figure 4). 4 The rules prescribe the procedures how to decide the representative BCC and ME value for each time frame in line with predefined priorities of the coding system and other predominant conditions. The collected time series data look like (4) resultant chart. The ME values can be averaged to arrive at a WIB score, indicating the participant’s mean WIB during the total mapping period. A mapper also records qualitative notes concerning (5) personal detractions and personal enhancers whenever they occur. Personal detractions and personal enhancers are staff behaviors that have the potential to undermine/uphold the 5 psychological needs of people with dementia. Finally, a mapper analyzes the results to write a report into (6) a summary for giving feedback to the care staff team. 4

Schematics of mapping and feedback process of DCM. DCM indicates Dementia Care Mapping; PwDementia, the person with dementia (the participant of DCM); PD, personal detraction; PE, personal enhancer; WIB score, well/ill-being score.

Decision-making of the representative BCC and ME for each time frame. BCC indicates Behavior Category Code; ME, Mood and Engagement.
Thus, the method sets high requirements on the mapper to (1) remember the unique coding systems, (2) observe and record the participant’s behavior and mood/engagement in detail on a frequent basis, (3) decide a representative pair of BCC and ME value after each time frame in line with the operational rules, and so on.
We investigated the mappers’ difficulties and/or burden being experienced during mapping by a single-administration questionnaire to 33 domestic mappers, 6 advanced and 27 basic DCM users. In the questionnaire, potentially difficult items for mappers were listed, from one of the authors’ own experience who had attended the DCM training course, and proposed to be rated qualitatively. Respondents were categorized into 3 groups depending on the experience or skill level (mapper level), and we quantified the ratings to calculate mean value of degree of difficulty for each group. “Degree of difficulty” is indicated qualitatively for providing better visibility than numerical mean values in Table 1, which shows the mappers’ difficulties and the degree of difficulty for each item per mapper level, where [++] ≥ 1.5; 1.5 > [+] ≥ 0.5; 0.5 > [−] ≥ 0. Those items with [−] rating for all levels of subjects were eliminated, resulting in 17 items. Naturally, those of lower mapper level felt more difficulty than those of higher mapper level. The responses were, in summary, (1) the DCM operational rules are hard to remember and execute, and (2) strict timekeeping is difficult and burdensome.
Mappers’ Difficulties and Degree of Difficulty per Mapper Level.

Abbreviations: BCC, Behavior Category Code; ME, Mood and Engagement; ++, difficult; +, a little difficult; −, not difficult.
Based on the survey, we have set the major support target at less experienced mappers and developed an ICT-based DCM support system having the following functions:
Basic functions that automatize, whenever possible, the operational rules, the decision rules of ME value, and other miscellaneous rules of DCM.
4
Real-time, that is, second by second, recording function. Burdensome timekeeping can be managed strictly by this function.
Handwriting input function, which makes it possible to take qualitative notes quickly and timely.
Reservation function and Alert function, both of which are helpful for increasing mapping accuracy. When a mapper cannot decide or recall a proper BCC that represents the participant’s specific behavior at the exact moment of occurrence, a mapping entry delay occurs, as shown in Figure 5A and B.
Reservation function allows a mapper to record just the entry timing without specifying BCC (Figure 5C), and they can assign an appropriate code later when it is fixed (Figure 5D), thus can compensate for entry delay retroactively.
Alert function helps prevent mappers’ overlooking changes of participants’ conditions, by means of alert indications. Red blinking (Prompting) emerges when a certain code has been kept unchanged for a given length of time (ΔT
1), followed by red light (Warning) after another set of time (ΔT
2). Not to be a nuisance, we allocated 95 and 60 seconds to ΔT
1 and ΔT
2, respectively.
Multiple event recording function. A mapper can enter up to 2 BCCs simultaneously.
Variable time frame length function. It is possible, by this function, to allocate an arbitrary length of time as a time frame, the default value of which is 5 minutes.
Functions (1) through (3) were intended to solve most of the difficulty items in Table 1. In addition, we have implemented functions (4) through (6) for adding extra value to DCM in order to make the best use of ICT.
The developed support system works as follows:
Once started, the system keeps time. A mapper is to simply record what is observed at a given moment. Then the system processes recorded BCCs and MEs automatically to finalize the representative [BCC, ME] pair for each time frame according to the operational rules. Thus, a mapper can concentrate on observation, without paying attention to keeping track of time as well as the complex operational rules to record the codes for each time frame.
Data Collection
In order to assess usefulness and reliability of the support system, we made role-play videos of dementia care scenes for mapping. Video mapping is advantageous over the mapping in actual care settings because (1) there arise no ethical issues; that is, risk of abusing privacy of people with dementia; (2) it is easier to conduct the experiments; and (3) tests can be repeated under the same condition; every subject watches the same videos.
Aiming to replicate actual events in the videos, we built a scenario based on the real mapping data provided by 5 advanced DCM users, by selecting the scenes of as many kinds of BCCs and MEs as possible. The videos were displayed on 2 monitors of 24″ size, each of which showed a role-play of different participant in a dementia care setting (Figure 6). The scenario was composed of 2 parts. Part 1, the former half, is the scene of a care facility during 10:00 to 13:00, including lunchtime. Part 2, the latter half, is the scene during 13:00 to 16:00. Each part was crammed into hour-long videos to show a series of comparatively more “active” scenes than normally observed in real care settings. The reason why we have made the videos more “dense” than real-life experience was to make the video mapping compatible with real-life mapping in terms of attention demand; that is, a mapper usually observes 5 participants at a time in real mapping while 2 participants were to be observed on the videos. Two accredited advanced trainers of DCM prepared model answers for the video mapping.
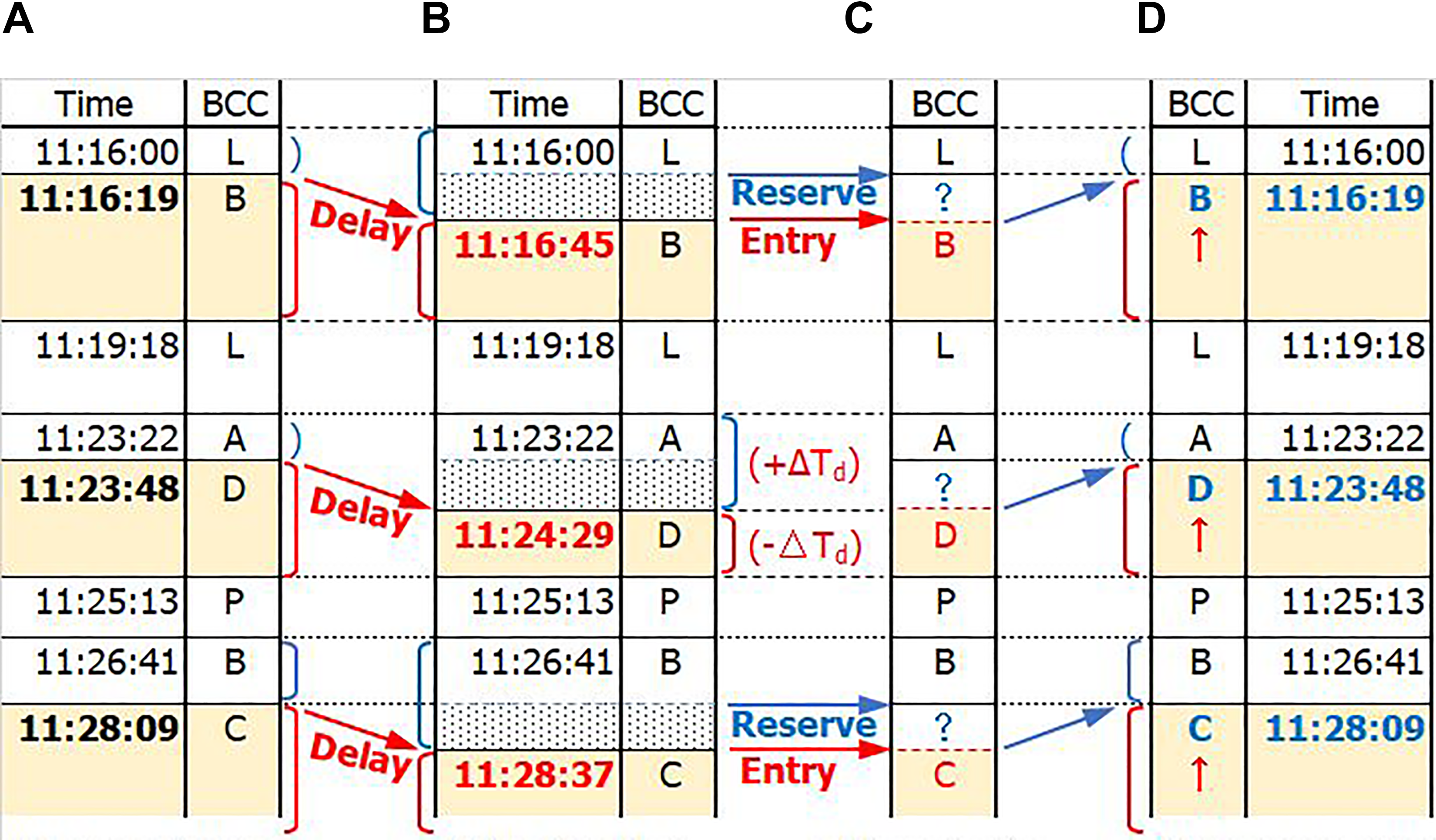
Reservation function for BCC entry compensation for mapping delay. (A) Entry of BCC at the exact moment of occurrence, (B) an entry delay causes the record duration errors of ±ΔT d, (C) reservation of the entry timing and assigning of BCC later, (D) compensation for the exact duration of the BCC record. BCC indicates Behavior Category Code; ΔT d, entry delay time.

Screen shots (balloons added) of 2 displays with a snapshot of a system evaluation experiment.
The data were collected either using the support system or the conventional paper-based DCM against the videos, as follows: At most 3 mappers (subjects) mapped at one time. Each subject conducted mapping for 2 hours in total, either by the following 2 sequences:
Sequence 1: Mapping for video part 1 by conventional way, followed by mapping for part 2 with using the support system.
Sequence 2: Mapping for video part 1 with the support system, followed by mapping for part 2 by conventional way.
Subjects
Twenty-two mappers volunteered as subjects and were categorized into 3 mapper groups SA
, SB
, and SC
depending on the mapper level as follows:
SA
: High-level mapper group, consisting of advanced users or well-experienced basic users of DCM, who have conducted [B] + [M] + [F] on a regular basis (several times a year or more)
SB
: Mid-level mapper group, consisting of basic users of DCM with some mapping experience, who have conducted [M] + [F] on a regular basis (several times a year or several times in total so far)
SC
: Starter-level mapper group, consisting of basic users of DCM with little or no mapping experience, who have conducted at most [M]
where [B], [M], and [F] stands for Briefing, Mapping, and Feedback, respectively. Tables 2 and 3 show the characteristics of the subjects and their mapping assignation in sequence 1 and sequence 2, respectively.
Characteristics of Subjects.

Number of Subjects per Mapping Sequence and by Mapper Level.
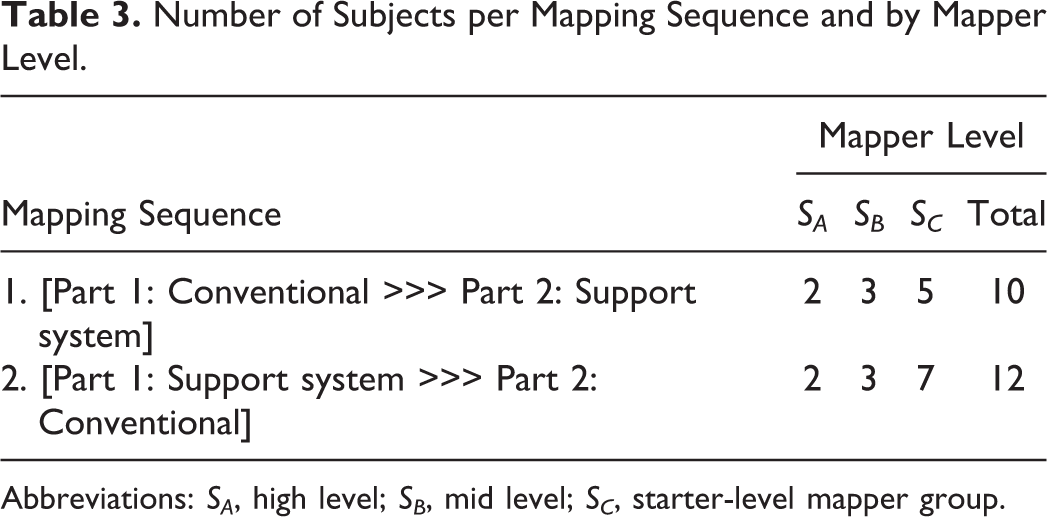
Abbreviations: SA , high level; SB , mid level; SC , starter-level mapper group.
Usefulness Evaluation of the Support System
We evaluated the usefulness of the support system as the decreased level of mapping difficulty using the support system, as follows: Ask a subject, concerning each item in Table 1, their usual feeling of level of difficulty (D) and level of help (H) that they have felt after using the support system:
(D) = {−3: difficult, −1: somewhat(s.wh.) difficult, +1: s.wh. easy, +3: easy}
(H) = {−3: unnecessary, −1: s.wh. unnecessary, +1: s.wh. helpful, +3: helpful}. Calculate the obtained easiness level (E) by the support system by equation (1):

where −6 ≤ (E) ≤ 6, and the more (H) exceeds (D), the larger (E) becomes. Calculate the obtained easiness level (E(j)i) concerning each item j (j = 1-17) for each subject i (i = 1-N, N: total number of subjects). If mean(E(j)i) > 0, then item j is considered to have become easier by the support system, where mean(E(j)i) is the average of (E(j)) of all subjects.
For evaluation of usefulness of the support system, we consider other positive effect utilizing the newly implemented functions, such as Reservation function and Alert function, as well.
Reliability Evaluation: Comparison of Mapping Accuracy
We evaluated the reliability of the support system by comparing the correctly answered rates of mapping conducted using the support system with that using the conventional paper-based method as follows: Obtain Cs
and Cc
, the concordance rates of mapping results over the model answers using the support system and conventional way, respectively. Let Csi
and Cci
be the concordance rates for each subject i (i = 1-N), and calculate the ratio of concordance rates (RC
i
) for each subject i by equation (2):

where k is the compensation coefficient for equalizing the difficulty level of the target videos for obtaining Cs and Cc .
If the average value of RC i ’s for every mapper-level group satisfies equation (3), then the reliability of the support system is validated:

We calculated the value k in equation (2) using the total average values of Cci ’s, that is, the concordance rates of mapping of all subjects conducted by conventional DCM, for videos part 1 and part 2.
Measures
DCM codes. The BCCs were assigned to participants in the role-play videos along with the ME values, both of which were recorded as per DCM 8 User’s Manual. 4
Ethical Issues
This is not a kind of human study that needs approval of an ethics committee but a system evaluation study using role-play videos. However, we explained to all of the subjects that (1) their mapping ability did not matter; that is, the experiment did not intend to measure the subjects’ mapping ability, and (2) subject anonymity would be preserved strictly, and we obtained consent of all subjects prior to conducting each experiment.
Results
Usefulness Evaluation
Decreased difficulty in mapping
Obtained easiness level (E) for each item in Table 1, estimated by equation (1), was all positive (Figure 7). Eight items were ranked quite high (+3.5 or above), 5 items (②, ⑦, ⑩, ⑫, and ⑬) among which were related to burdensome keeping track of time. Whereas 2 items, ⑭: easy notes taking and ⑯: easy correction of notes and codes, received a relatively low score of 1.3 and 1.0, respectively.

Obtained easiness level (E). Difficulty is indicated as “–2(D)”; twice of negated level of difficulty (D), for reference.
About making qualitative notes, total average numbers of handwritten items were slightly smaller using the support system than by conventional paper-based method (Table 4). While descriptions using the support system were more accurate and informative with time stamps.
Numbers of Handwritten Items Using the Support System and the Conventional Method.

Reservation function for BCC entry
Of 22 subjects, 18 utilized this function 161 times (around 9 times per subject on average). Number of cases in which compensated times are 10 seconds or longer, alongside the mean delay times (durations) for those cases, are shown in Table 5(a).
Usage of Reservation Function and Alert Function.

Abbreviations: BCC, Behavior Category Code; SA , high level; SB , mid level; SC , starter-level mapper group.
Alert function to prompt updating codes
Promptings were invoked 1297 times against all subjects (59 times per subject on average during 1-hour mapping), 14 times out of which ended up with Warnings. Numbers of cases in which mappers updated (changed) or continued the previously entered codes within 10 seconds after Promptings, alongside the average response times, are shown in Table 5(b1) and (b2), respectively. Numbers of cases in which Warnings emerged, alongside the average response times, are shown in Table 5(c1) and (c2).
Reliability Evaluation: Mapping Accuracy Using the Support System
The mean values of the compensated ratio of concordance rates RCs for sequence 1 and sequence 2 for subjects categorized by experience level, SA , SB , and SC , were 1.0, 1.1, and 1.1, respectively, as shown in Table 6. There were no significant differences in mapping accuracy using the support system against by conventional way depending on the subjects’ mapper level.
Mean Values of Cs and Cc and the Resultant Ratio RC Compensated by k, per Mapper Level.
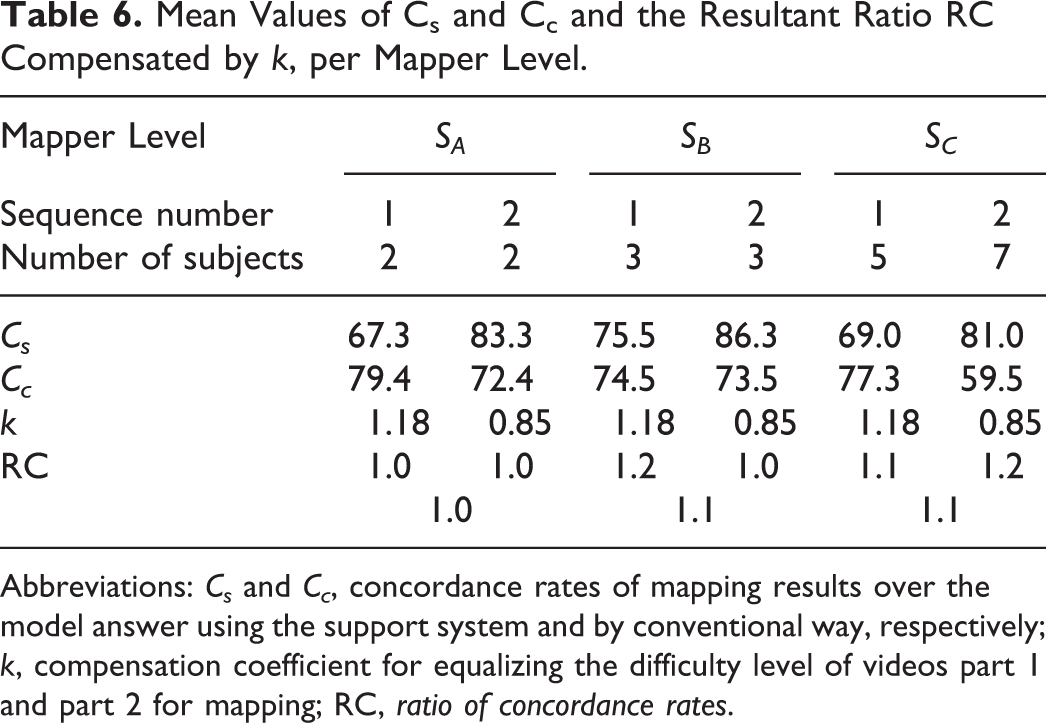
Abbreviations: Cs and Cc , concordance rates of mapping results over the model answer using the support system and by conventional way, respectively; k, compensation coefficient for equalizing the difficulty level of videos part 1 and part 2 for mapping; RC, ratio of concordance rates.
Discussion
The total number of 5-minute time frames for the collected mapping data was 1056, and each time frame contributed a BCC and ME value rating from each subject. The total time frames correspond to 88 hours of observation. However, it may be equivalent to twice as long as the period or even longer, since we made the role-play videos “dense”; that is, the events during 3 hours were crammed into 1 hour. Actually, some of the subjects remarked the video mapping to be much busier than usual mappings.
Usefulness of the Support System
Effects of basic functions and real-time recording function
As shown in Figure 7, despite some limitations, we received quite positive feedback from almost all of the subjects regarding burden reduction and easier operation of DCM. In addition, most subjects showed the willingness to apply the support system in practical use after the experiments. The results demonstrated that the Basic function that automatize the rules and the Real-time recording function worked effectively to support mappers.
Effects of Handwriting input function
Generally, it takes more time to take notes by digital devices than using paper and pen. Voice recording may be a good alternative, which is quite fast. However, it is not applicable to mapping because it is very likely to disturb the care environment. Hence, we implemented the Handwriting input function to address the issue. The relatively low ratings on items ⑭ and ⑯ (Figure 7) and slightly smaller amount of handwritten items (Table 4) imply, however, that the support system is not as flexible as the paper-based system concerning making and/or correcting notes. It is very important to record qualitative notes as much as possible in DCM; therefore, there needs some improvement on this point.
Instead, notes recorded with time stamps provided more accurate explanation of the activities/states of the participants alongside the entered codes (BCCs and ME values) with time stamps, which was advantageous over the conventional method.
Effects of Reservation function for BCC entry
A delay of BCC entry timing by ΔT d ends up with the duration error of 2ΔT d in total (Figure 5). Therefore, it is necessary to avoid BCC entry delays to ensure mapping accuracy. In practice, however, it is not necessary to be as precise as to a second, and 10 seconds may be a practically non-negligible amount of time. As shown in Table 5(a), those cases in which ΔT d ≧ 10 seconds were observed in all mapper levels, and quite significant delay times, for example, 28 and 75 seconds have actually been compensated. The results demonstrated that the Reservation function could potentially serve to increase the accuracy in actual mapping, regardless of the mapper level.
Effects of Alert function to prompt updating codes
It is not easy to keep one’s concentration during a long period (eg, a 6-hour mapping). Actually, it often happens that entries of some time frames be left blank by oversight in the conventional mapping. When using the support system, the entered codes may last beyond time frames by oversight, instead. The Alert function calls mappers’ attention by Prompting. The sooner a mapper responds to Prompting, the more accurate the recorded data will be.
The function was invoked quite frequently during the experiments. Among the cases in which the mappers responded to Prompting within 10 seconds, they continued the previous conditions in more cases than they updated to new BCCs and/or ME values. The numbers of cases updated versus continued are 76:340 and 79:426 for videos part 1 and part 2, respectively, as shown in Table 5(b1) and (b2). The average response time was slightly longer when codes were updated than continued in all mapper levels: 5.1:4.1 and 5.4:4.2 for videos part 1 and part 2, respectively. The results obviously demonstrated that continuing operation is simpler and easier than entering new codes. Warnings emerged also in all mapper groups, though the number of cases was small, as shown in Table 5(c1) and (c2). Thus, the periodic alert for preventing oversight seemed to have worked effectively, indicating the potential of the Alert function to increase mapping accuracy.
Reliability of the Support System
The mapping accuracy using the support system was equivalent or slightly higher than that by conventional way, as shown in Table 6. The results demonstrated that the developed prototype support system has already reached the level of conventional DCM in terms of mapping accuracy. The results may possibly imply that the support system is more helpful for less experienced mappers than experienced as intended, since the average RC values of mapper levels SB and SC were 1.1 while that of level SA was 1.0, though there was no statistically significant difference between them. In order to ensure the reliability of the system, further research is needed by conducting mapping at real care settings in a larger sample size. We think the support system is almost ready, with some improvements, for the use of this purpose.
Extendibility of the Support System
There have been published several studies so far that raised questions about the psychometric properties of DCM. 6,11,21 -23 For example, Thornton et al 21 assessed whether the 5-minute time frame was able to provide a meaningful representation of actual events. They compared the data obtained by 2 different methods, DCM mapping and continuous time sampling, to discuss the issue. Utilizing the Variable timeframe length function of the support system, it is possible to analyze the identical raw DCM data under different time frame lengths to compare the results, in line with the DCM rules. Actually, none of the rules is substantially restricted to “5-minute” and varying it may possibly bring different mapping results. Hence, the ICT-based support system has potential of solving some of the methodological issues by extending the paper-based method of DCM, together with the Multiple event recording function.
Limitations
Some of the limitations of this study are (1) the small sample size and (2) mapping data were collected only against role-play videos.
Sample size of 22 subjects (mappers) is quite small in general; however, as far as we know, it is the largest to date for a published study concerning DCM that has employed mappers, except for those on survey of mappers. The reasons may include that not so many mappers are readily available to cooperate in research besides their hectic normal daily duties. Moreover, even a relatively small number of mappers can undertake mapping of a large number of participants , as in most DCM relevant studies. Nonetheless, larger sample size with various mapper levels is needed to fully evaluate the DCM support system as well as to identify various support needs.
Video mapping is suitable in terms of repeatability of evaluation tests. In addition, we designed the video mapping to be compatible with real-life mapping in terms of attention demand. Nonetheless, we cannot guarantee the compatibility; therefore, actual mapping in different environments is indispensable for full evaluation of the support system. It is hoped that further studies will be conducted in real care settings and evidence be accumulated.
Conclusions
Dementia Care Mapping is a well-developed evidence-based observational method and has been widely used worldwide to implement Person-centred Care in dementia care settings for over 20 years. However, recent researches have reported mixed results on efficacy of DCM, and implementation issues arose as the contributing factors for the differences in the research results. Authors focused on the barriers to DCM implementation at the observer (mapper) level, where the complexity of the method makes mappers difficult to carry out DCM. To solve the problem, we have developed a new ICT-based DCM support system based on the investigation of mappers’ difficulty during mapping. We also developed a new test method using role-play videos and assessed the usefulness and reliability of the support system. We received quite positive feedback regarding burden reduction and easier operation of DCM and found out that the prototype support system has already reached the level of conventional DCM in terms of mapping accuracy, as well. In addition, the new functionality of the system indicated potential for increasing mapping accuracy. In order to put the support system into practical use, however, there still need further improvements in, for example, agile note-taking and flexible revision of mapping entries.
Future studies include reliability assessment of the system by actual mapping at various care settings, development of additional support functions for paper work (report writing), and validation and extension of current DCM method utilizing the advantages of the ICT-based system over the conventional paper-based method.
Footnotes
Authors’ Note
Development of the DCM support system was undertaken under a Research License Agreement with University of Bradford.
Acknowledgments
The authors thank the following for their contributions to this work: Dr Yutaka Mizuno, Strategic Lead of PCC/DCM in Japan, for his continuing support and encouragement for us. Dr Tetsuro Ishihara and all the volunteer mappers across the country for their support and participation in the evaluation tests. Special thanks to Yasuko Murata and Yuko Nakamura for their assistance, as accredited advanced trainers of DCM, to prepare model answers for the role-play videos, and to Satoshi Yoshikawa and his colleagues for providing us with the opportunity to run pilot tests in their facilities to finalize the system evaluation procedure. The authors also thank Dan, Meg, Michiko Yamamoto, and Emma Mori for making the role-play videos.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.