
Abstract
Background:
Several recent studies have examined the positive effects of physical exercise and equilibrium on individuals with neurodegenerative diseases.
Objectives:
In this sense, this study based on an experimental design, tested whether global postural reeducation (GPR) can affect equilibrium and cognition, life quality, and psychological symptoms of patients with Alzheimer’s disease (AD).
Methods:
One hundred thirty-five participants with mild and moderate AD diagnosis were assigned to 2 groups: experimental group (EG, n = 90) and control group (CG, n = 45). The GPR therapy was implemented in the EG for 6 months, while both groups underwent neuropsychological assessments prior and after the 6-month period.
Results:
According to the repeated measures of analysis of variance, significant differences between groups were found at the 6-month follow-up period, in benefit of the EG such as Mini-Mental State Examination (P = .000), Geriatric Depression Scale (P = .000), Neuropsychiatric Inventory (P = .000), quality of life in AD/patient (P = .000), quality of life in AD/caregivers (P = .000), Barthel index (P = .000), and Tinetti Scale (P = .000), while the CG showed a low performance in the neuropsychological tests.
Conclusions:
We suggest that GPR is a therapeutic option, which can improve the psychological, physical, and cognitive aspects of patients with AD.
Introduction
Alzheimer’s disease (AD) was first described in 1906, after Alois Alzheimer’s evidence, hence its name, but it took about 70 years until it was known as a common case of dementia and one of the deadliest causes. 1 In respect to the clinical outlook, the way of presentation, natural history, symptoms, the interaction of cognitive and noncognitive factors, and the duration of the disease, it represents the possibility of individual alterations that complicate the prototype clinical framework of the disease. 2
The origin of the disease is characterized by unclear symptoms that are recognized only retrospectively once the clinical outlook is clearly manifested. 3 Despite the progressive loss of cognitive functions, dementia, in its clinical setting, is a disorder of the motor system. Therefore, individuals with AD present alterations in the step plan, decrease in walking speed, and an average increase in limb support time, in comparison to healthy elderly individuals. 4,5 Meanwhile, the loss of locomotor efficiency increases the falling and the balance hub risk. 6,7
It has been widely reported in the literature that executive dysfunctions contribute to the instability of gait and balance, and this increases the falls in patients with AD. 8 Moreover, elderly patients with AD are 3 times more prone to falls when compared with elderly individuals without dementia. Consequently, it is necessary to develop strategies that might reduce the deterioration of the executive functions and the one of components of functional capacity in the elderly patients with AD. 9 In this merit, some researchers showed that physical activity can indeed reduce the decline in executive functions and the loss of functional capacity components, such as balance, in elderly patients with AD, thus contributing to the reduction of fall risk. 10,11 Rolland et al 12 showed that by implementing a therapy with a noncontrolled design through a 7-week program of endurance training and exercise (walking and cycling) led to a decrease in the nutritional and behavioral complications as well as the risk of falls in patients with AD. On the other hand, it was observed that a structured physical activity during a 12-week program greatly improves muscle tone, flexibility, alertness, dynamic balance, posture, and walking and decreases the risk of fall. 13
In fact, the mechanisms through which physical activity provides benefits to cognitive functions might be explained, according to some authors, 14,15 for example, by the increase in the supply of oxygen and other energy substrates during the regular practice of physical activity. This increases the use of neurotransmitters and also provides the release of brain-derived neurotrophic factor, a substance responsible for the process of neural regeneration. Other authors 16 observed improvement in the motor function of patients with AD, after 3 months of aerobic exercise and training of strength, balance, and flexibility.
Given the abovementioned facts regarding the benefits of physical exercise and the importance of improving gait and balance in patients with AD, this pioneer study explores the global postural reeducation (GPR) method effects in patients with AD. Comparatively, the literature review shows that this method turns out to be effective in the treatment of many pathologies and muscle–skeletal disorders such as back pain, rheumatoid arthritis, ankylosing spondylitis, disc hernias, cystic fibrosis, respiratory obstruction, and so on. 17 -20
The GPR is a method that mainly involves global stretching, breath control, and manual control by the therapist in order to provide proprioceptive information to the patient. Therefore, it is considered an intermediary approach between active techniques, such as stretching, and passive techniques and manual therapy. Breath control plays an important role during the exercises and may be proposed as one of the beneficial mechanisms of action. 21,22
The GPR’s specific aim is to prolong muscle relaxation and contraction of antagonistic muscles by avoiding postural asymmetry. Treatment postures of GPR especially affect the balance of 2 major chains, usually called anterior chain and posterior chain. Thus, the mechanism of action of GPR is the re-equilibration effect of the different treatment postures on areas of motor cortex that control muscles belonging to the posterior or anterior chains. 23 -25 The GPR maneuver, applied in standing patients, increases inhibition in cortical areas by controlling flexor muscles, which increases the even excitation of cortical areas that control extensor muscles. However, when GPR maneuver is applied in patients in supine position, increased inhibition in cortical areas controlling flexor muscles is not extended in the excitation of the extensor ones. 26
Indeed, the GPR technique is intended to act on the muscle-tendinous system by achieving the body harmony by stretching. 27 This is accomplished by working on the kinetic muscular chains organized according to a structure. 28 According to Souchard, the good body morphology is indispensable for life. In this context, the purpose of the study is to verify whether GPR can affect equilibrium, cognition, life quality, and psychological symptoms of patients with AD, through postural treatment.
Methods
Study Design and Participants
This pilot clinical trial was carried out simultaneously between 2 countries, Albania and Spain, for 6 months. Patients were recruited from senior residences of Tirana (Albania), Murcia, and Malaga (Spain) according to the National Institute of Neurological and Communicative Diseases and Stroke/Alzheimer’s Disease and Related Disorders Association criteria 29 with a clinical diagnosis of AD allocated into 2 groups.
A total of 135 patients participated in this study and 90 out of them pertain to an experimental group (EG) and 45 control group (CG). The inclusion criteria for the present study were patients with a probable AD diagnosis in mild–moderate stage, live in the community such as residence, able to autonomously perform daily activities, and show no presence of any other neurological and psychological disease. Participants not within the target age range (67-92 years), those with severe dementia or those who presented vertigo, visual impairment, previous back surgery, vertebral fracture, presence of brain tumors, presence of psychiatric disease, ictus, or other limitations that made the ambulation difficult were excluded.
A simple random sampling was used. The allocation was performed by an external scientific researcher, who was not involved in the assessment or treatment of the participants, and used a computer random number generator from Excel 2016 software program. The GPR therapy lasted 6 months with pre–post tests (T0-T1) carried out before and after 6 months of treatment.
The data were provided by the professional GPR treatment physiotherapists for each center that was in charge of including or excluding patients who performed the abovementioned technique. The collected results were given to a single external evaluator who provided the study “data pool.” The study was approved by the ethics Committee of Catholic University of Murcia, in full compliance with ethical standards of the Committee on Human Experimentation of the institution, in which the examinations were done, as well as in compliance with Helsinki Declaration of 1975. All participants signed the informed consent, and their family members were also informed concerning the purpose of the study.
Assessment of Cognition
– Mini-Mental State Examination (MMSE) 30 : The version of 30 elements was used to obtain a global measure of cognitive function and dementia. This test was chosen to be implemented with reference to its practicality, use, and recognition in all residences analyzed.
– Quality of Life in AD (QoL-AD) 31 : It consists of 13 elements referring to the perception that patients have concerning various aspects of their life such as mood, health, cognition, environment, and functional capacity. There were separately analyzed as QoL/AD caregivers (QoL-AD/C) and QoL/patients (QoL-AD/P) with the aim of verifying whether there were correlations in what patients and caregivers reported for the same test.
– The Geriatric Depression Scale (GDS) 32 : The version of 15 elements was used, which given its length can be validly and reliably resolved by patients themselves in the quality of a self-report questionnaire, in order to investigate the possible presence of depressive symptoms.
– Neuropsychiatric Inventory (NPI) 33 : This test includes 12 symptoms scored according to severity and frequency phenomena. It is an instrument specifically designed for the assessment of psychobehavioral disorders in individuals with cognitive impairment.
Additional Assessments
– Barthel index (BI) 34 : It is used to measure performance in the basic activities of daily life. It refers to the patient’s independence in all basic daily living activities, and the maximum score used is 100 points.
– Tinetti Scale (TS) 35 : The equilibrium subscale has been applied, which consists of 7 elements and with a score between 0 and 13. Highest scores indicate a better balance.
Intervention
The intervention implemented to the EG with AD was the GPR, which lasted about 30 to 40 minutes in repeated individual sessions of 2 meetings per week, in 6 months, respectively, by making 48 sessions in total, under the implementation guidance of different certified postural therapists for each residence. All participants received the intervention in the same time period. During each treatment session, the tight muscles related to the postural misalignment were smoothly and progressively stretched into a particular position (treatment postures), followed by the active contraction of the antagonist muscles. Hence, the therapist and the patient were able to control and harmonize compensatory movements along with a 3-dimensional global alignment of body segments and joints. 23,36,37
The treatment posture consists of a global neck pompage, relaxed lying patient associated with deep diaphragmatic breathing, and legs in shape of frog during the first period, with the aim of lengthening the anterior muscular chain, lying posture with progression of the extension of the legs. During the second treatment period, the posture of patients with AD changed, with the aim of posterior muscle chain stretching, lying posture with hip joint flexion progression. It is addressed by changing the position of the legs (tied with a rope in the angle with pelvis 90°), and in the last period of therapy, the position changed again, with the aim of giving major importance to the specific rehabilitative technique of deep diaphragmatic breathing, with legs relying on pelvis approximately 90° and the knees in 70° on pillows, as auxiliary; the patient lying always supine in bed therapy (Supplemental Material).
Meanwhile, the same residential conventional exercises were performed, such as 30 to 40 minutes of physical exercise, aerobic, and walking activity, referring to the therapeutic intervention of CG.
Statistical Procedure
A comparative study of an exhibition consisting of 2 groups (experimental and control) was carried out. The statistical analysis was performed using Statistical Package for the Social Sciences—SPSS 21 for Windows. In the first moment, the variables treated were established. Thus, a descriptive statistical analysis (frequency, mean, and standard deviation) was performed for clinical, neuropsychological, functional, and psychobehavioral variables at baseline and at the end of the study. Quantitative variables were expressed as mean ± standard deviation. Furthermore, the variables normality diagnosis has been performed with the Kolmogorov-Smirnov test for n > 50. In addition, a repeated-measures analysis of variance (ANOVA) was used to compare the continuous variables, while χ2 test was used for dichotomous ones. The significance value was corrected according to the Bonferroni analysis for multiple comparisons of the multivariate general linear model. Effect sizes are reported as partial η2, with cutoff values of 0.01, 0.06, and 0.14, respectively, for small, medium, and large effects. 38 Pearson coefficient was used to test the correlations between variables. The statistical examinations were performed at 95% confidence level.
Results
Only 160 patients out of the 180 patients with AD contacted fulfilled the study eligibility criteria and were randomly allocated into 2 groups (EG, n = 90 and CG, n = 70). In total, 25 participants from the CG were excluded from the analysis considering that 9 patients changed residence, 5 patients died, other 5 lost to follow-up, and 6 withdrew. Participant flowchart is shown in Figure 1.
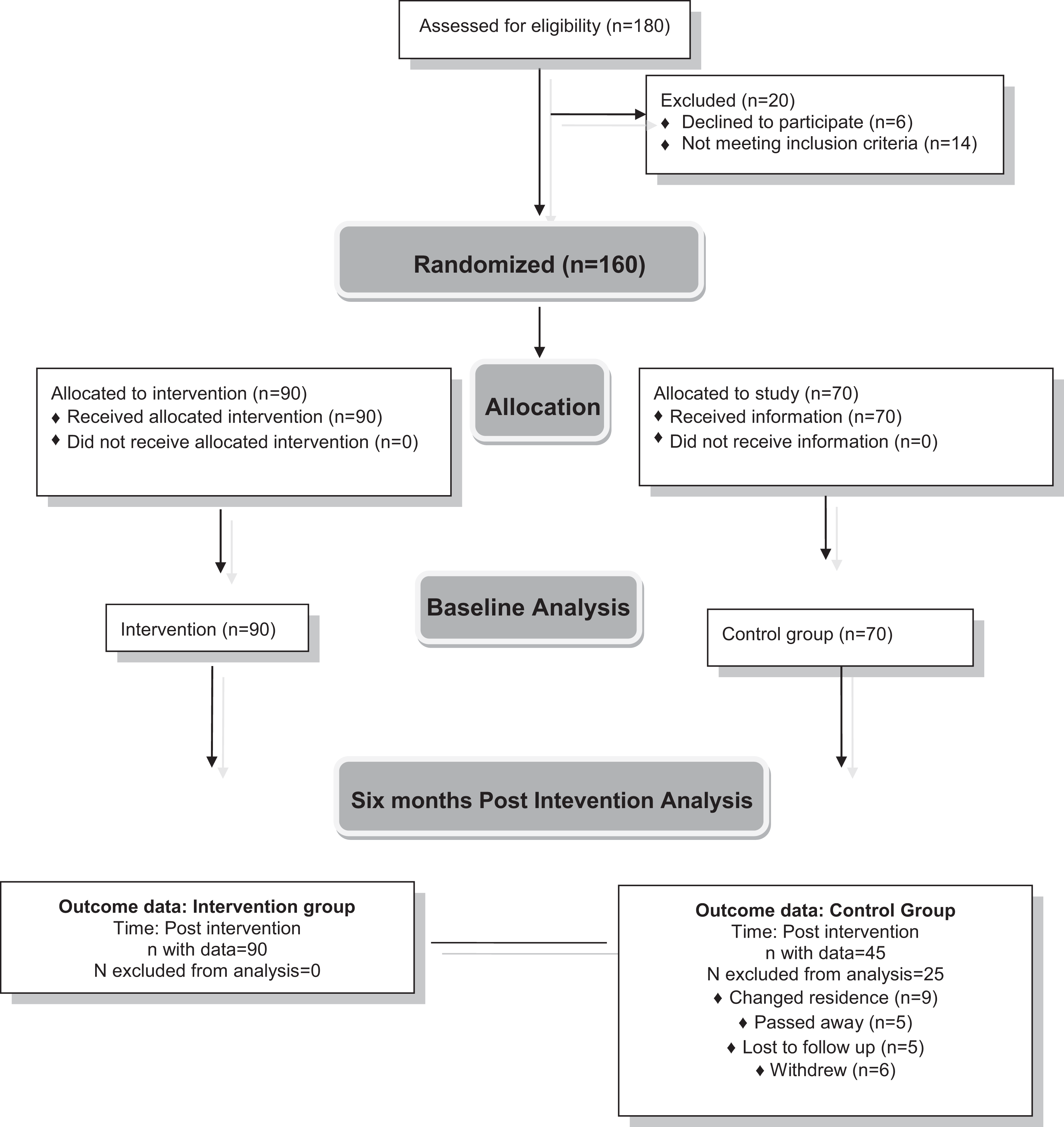
Flowchart of participants.
As a consequence, 135 elderly people were analyzed, of which 45 belonged to the CG. The sample consists of 34% male (n = 46) and 66% female (n = 89) with average age between 67 and 92 years (mean age = 80.76, standard deviation [SD] = 5.32). Specifically, the CG consists of 38% male (n = 17) and 62% female (n = 28) aged 73 to 92 (mean age = 81.87, SD = 4.83). At baseline, the individuals of both groups were homogeneous concerning the age and Alzheimer phase. Characteristics of participants are presented in Table 1.
Baseline Demographic and Clinical Characteristics of Participants.

Abbreviations: CG, control group; EG, experimental group; M, men, Min, minimum; Max, maximum; N, participants; SD, standard deviation; W, women.
As shown in Table 2, at baseline, EG and CG did not show statistical differences in MMSE (P = .053), QoL-AD/C (P = .503), QoL-AD/P (P = .101), and NPI (P = .093). The exceptions were in the GDS in which the CG had 2.39 more points than the EG; in the BI in which the EG had 14.04 more points than the CG; and in the TS, in which the EG had 1.68 more points than the CG.
Baseline Characteristics of Participant Outcomes.

Abbreviations: BI, Barthel Index; CG, control group; EG, experimental group; GDS, Geriatric Depression Scale; MMSE, Mini-Mental State Examination; N, number of participants; P, significance; QoL-AD/C, quality of life in Alzheimer’s disease/caregivers; QoL-AD/P, quality of life in Alzheimer’s disease/patients; SD, standard deviation; NPI, Neuropsychiatric Inventory; TS, Tinetti Scale.
Table 3 shows means and SDs for each group at baseline and postintervention and the interaction effects from repeated measures of ANOVA, which revealed a statistical significant difference between groups, concerning the majority of the outcomes such as MMSE (F 1,133 = 9.28, P = .003, η2 = .065), QoL-AD/C (F 1,133 = 7.53, P = .007, η2 = .054), GDS (F 1,133 = 95.72, P = .000, η2 = .419), BI (F 1,133 = 8.67, P = .004, η2 = .061), NPI (F 1,133 = 5.73, P = .018, η2 = 0.041), and TS (F 1,133 = 9.89, P = .002, η2 = 0.069). The exception was represented from the QoL-AD/P (F 1,133 = 2.26, P = .135, η2 = 0.017) outcome, which did not revealed statistical significance between groups. This was separately analyzed on purpose, aiming to report and compare the mean and SD differences of QoL-AD/C, where participants reported 1.71 more points than caregivers in the sixth month at CG and 0.21 points more at EG.
Means and SDs, for Each Group at Baseline and Postintervention, and Interaction Effects From Repeated-Measures ANOVA.

Abbreviations: ANOVA, analysis of variance; BI, Barthel Index; CG, control group; EG, experimental group; F, frequency; GDS, Geriatric Depression Scale; N, number of participants; P, significance; QoL-AD/C, quality of life in Alzheimer’s disease/caregivers; QoL-AD/P, quality of life in Alzheimer’s disease/patients; MMSE, Mini-Mental State Examination; NPI, Neuropsychiatric Inventory; SD, standard deviation; TS, Tinetti Scale; T0, pretest; T1, six months posttest; η, partial η quadrate value.
It is also important to mention the significance of the depressive and neuropsychological symptoms of the sample; thus, the mean difference (SD) of GDS test shows an increase of 5.12 (0.22) points at CG, and mean difference (SD) of NPI shows an increase of 5.89 (2.46) points at CG. Hence, the lower is the total scored, less depressive and neuropsychological symptoms present in the patients. The repeated measures of ANOVA yielded a significant mean difference in time interaction between groups for MMSE (P = .000, η2 = 0.120), BI (P = .000, η2 = .433), and TS (P = .000, η2 = 0.383). However, the outcomes such as QoL-AD/C (P = .104), QoL-AD/P (P = .265), GDS (P = .124), and NPI (P = .078) did not present significant mean difference in time interaction between groups (refer to Table 4).
Mean Difference Interaction Between Intervention and Control Group at 6-Month Follow-Up.

Abbreviations: BI, Barthel Index; CG, control group; CI, confidence interval; EG, experimental group; F, frequency; GDS, Geriatric Depression Scale; MMSE, Mini-Mental State Examination; P, significance; η, partial η quadrate value; QoL-AD/C, quality of life in Alzheimer’s disease/caregivers; QoL-AD/P, quality of life in Alzheimer’s disease/patients; NPI, Neuropsychiatric Inventory; TS, Tinetti Scale.
Nonetheless, regarding the group × time interaction, significant improvements were found in all variables without any exception such as MMSE (1.71% for the CG and 0.66% for the EG): F 1,133 = 94.29, P = .000, η2 = 0.415; QoL-AD/C (2.28% for the CG and 1.57% for the EG): F 1,133 = 79.41, P = .000, η2 = 0.374; QoL-AD/P (2.13% for the CG and 1.63% for the EG): F 1,133 = 71.10, P = .000, η2 = 0.348; GDS (0.8% for the CG and 1.22% for the EG): F 1,133 = 54.98, P = .000, η2 = 0.292; BI (3.33% for the CG and 1.33% for the EG): F 1,133 = 47.20, P = .000, η2 = .262; NPI (4.13% for the CG and 3.36% for the EG): F 1,133 = 302.4, P = .000, η2 = 0.695; and TS (0.44% for the CG and 0.96% for the EG): F 1,133 = 72.22, P = .000, η2 = 0.352.
In Table 5, the relationship between all the outcomes analyzed as MMSE (P = .000), QoL-AD/C (P < .05), QoL-AD/P (P < .05), BI (P = .000), GDS (P < .05), NPI (P = .000), and TS (P = .000) is shown.
Relationship Between Outcomes.
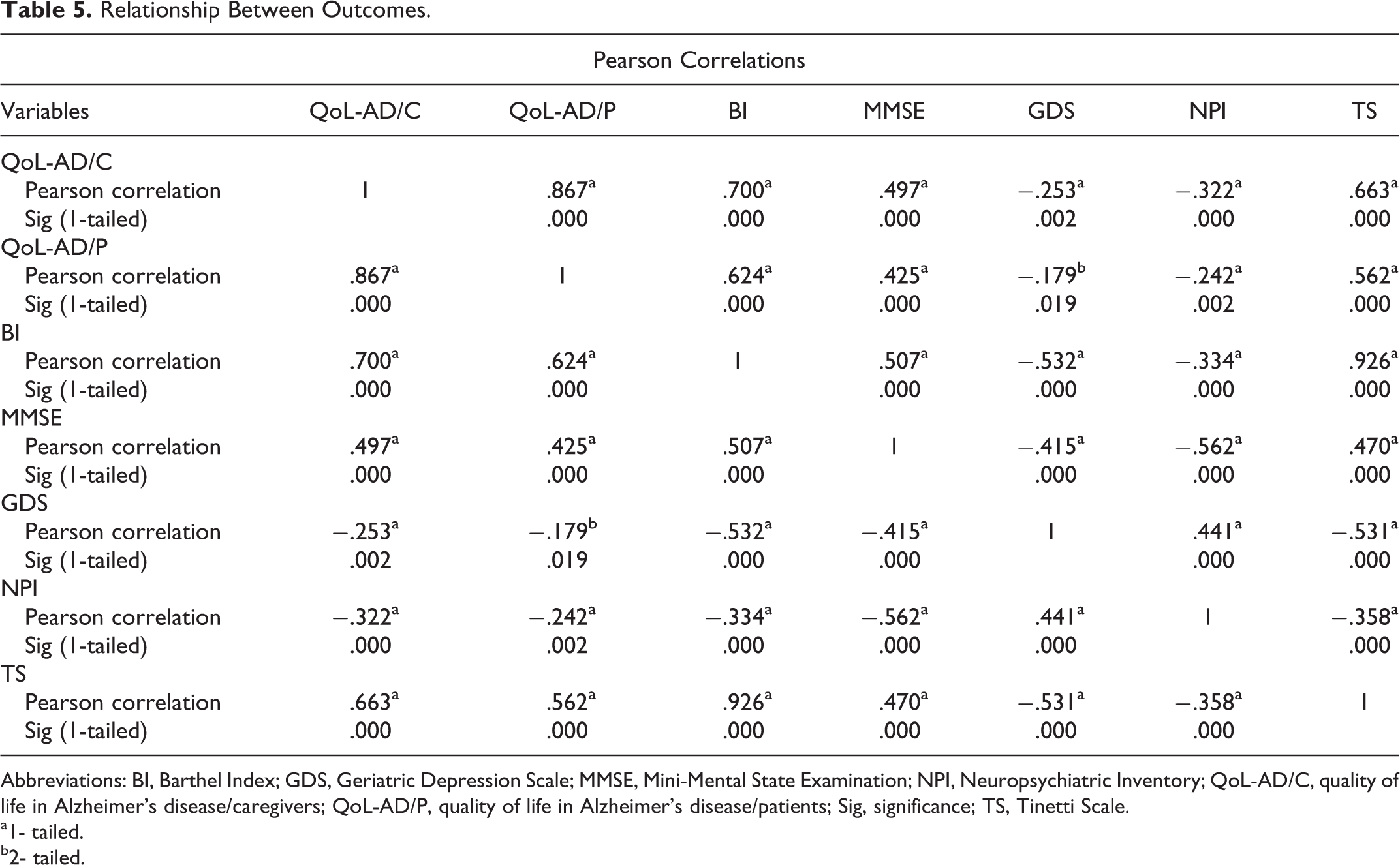
Abbreviations: BI, Barthel Index; GDS, Geriatric Depression Scale; MMSE, Mini-Mental State Examination; NPI, Neuropsychiatric Inventory; QoL-AD/C, quality of life in Alzheimer’s disease/caregivers; QoL-AD/P, quality of life in Alzheimer’s disease/patients; Sig, significance; TS, Tinetti Scale.
a1- tailed.
b2- tailed.
Discussion
The 6-month follow-up results in this study showed that GPR technique was effective in individuals with AD, as helped in the improvement of their cognitive, autonomy, balance, neuropsychological, and depressive symptoms. With special regard to the latter, which is assessed with GDS test, the difference between baseline groups was significant. Experimental group represented 2.39 points less than CG. Experimental group had a depression average of 1.22 points compared with an average increase of 1.51 points in CG symptoms, as shown in the results after the GPR implementation. Concerning BI results, it can be affirmed that at baseline, EG had an average of 14.04 points more than CG. After the 2 groups’ assessment of 6-month period, EG had an average increase of 1.34 points compared to CG, as the latter marked a 12.96 points decrease in the score. This average difference can be explained even by the difference in the number of participants, considering that in the sixth month of the study, the CG was reduced with 25 participants (see Figure 1).
The same situation was presented even for TS, where at baseline, the difference between groups represented an average of 1.68 points more for EG. While in the sixth month after GPR implementation, there was a surge in balance with a mean of 0.97 points in EG compared to CG, which marked a 1.8 average decrease.
The explanation for the significance of all results produced by GPR intervention is that this procedure is based on the globalism (physical strategy designed to improve static and dynamic stability) of the individual and not only the fact that it takes into account all kinetic chains. It is important to treat the whole musculoskeletal structure including the upper and lower limbs, in order to reach the balance, without forgetting the individual’s global influence and the psychomotivational aspects. 27 In fact, the main goal is to improve the progressive reeducation of normal body functioning. 39 In addition, GPR has also been suggested with the aim to exert physiological effects at cortical level by increasing the amount of intracortical inhibition and reducing intracortical excitation, or both. 26 Hence, the pilot randomized study of Agosti et al demonstrated that significant improvements in temporal gait parameters of patients with Parkinson disease can be obtained through a 4-week GPR program. 40 Furthermore, in the randomized controlled trial (RCT) study of Pillastrini et al with a 6-month follow-up period of the GPR implementation in patients with neck pain, 18 it is proposed to discuss the matter in a broader context, as it takes into consideration some psychosocial components of the chronic pain. Therefore, this study highlights that GPR may be a gentle option to propose movement without pain, enhance relaxation via respiratory rhythm, and offer a positive experience of body posture modification. Moreover, this clinical encounter approach can influence not only the “posture” but also the negative feelings and beliefs that are frequently associated with chronic pain. Nonetheless, these findings can be discussed in a wider context by also taking into consideration the treatment of psychosocial components and the fact that no previous controlled study investigated the efficacy of GPR in patients with AD.
Meanwhile, the current study is analyzed through a midterm follow-up therapy focused on 2 weekly sessions. It was also noted that the EG compared to the control one had a notable symptomatic improvement and dominance of the AD symptoms.
Maybe, the presence of the physiotherapist in an individual session of EG can cause the positive results and, in addition, it should be added that it was the first time that patients had experienced a completely individual postural therapy for about 40 minutes. Previously, they were mostly organized in residences and in psychological and cognitive therapy groups.
Another positive element in the GPR implementation technique, which may have positively impacted the study, is the proactive patients’ cooperation during the treatment, as it should be all the time, in order to autocorrect the wrong postures during the treatment combined with postural harmonious breathing cycles. A good postural control allows the patient’s motor control, balance, and breakdown of the wrong postural schemes. In this regard, other studies suggest that intensive postural treatment improves significantly functional performance, which is a distinctive sign of life quality and independence associated with mobility. 41,42
Referring to the epidemiological studies, concerning AD incidence among women, 43 -45 it can be said that 135 elderly patients with AD participated in this study, and the examined sample consisted of almost 66% females (n = 89). In this regard, epidemiological studies 23 confirm that women live longer and perhaps this fact mostly brings the appearance of AD to them. Against the epidemiologically references in the review of statistical data on individuals with AD, it can be evidenced that the major factor causing the decline in cognition is not yet studied. 46 However, another important result is that around the first half of the 20th century, women had a lower level of education than men in the same examination period. 47
It can be confirmed that the sample average age was about 80 years by comparing these interesting data with our study. It is worth mentioning that this fact leads to cognitive deterioration from the aging process and consequently to the appearance of a multitude of cognitive pathologies. According to the World Health Organization projections, in recent years, there are more cases of dementia, of which two-thirds are revealed with AD. 48 Not disconnected from our descriptive analysis, the sample’s major part (n = 108) consisted of individuals with an average education, not low. Therefore, our results do not confirm the above data considering that the analyzed sample is small (n = 135) in confront to the entire population. From the other hand, it can be affirmed, closely referring to this research results, that all variables explored were correlated between each other (see Table 5 data). This important fact demonstrates that cognition affects the psychological, depressive, autonomy, and quality of life of the individuals with AD; and a meaningful interaction of all study variables approves the hypotheses raised correspondingly.
Thus, a further correlation between the improvement in depression and neurological symptoms was observed (refer to Table 5). In addition, the evidences prove that the correlation between functional and cognitive improvement exists, and the effect on the functional state is likely to precede global cognitive improvement. In fact, it has been reported that the elderly confinement, as well as the simultaneous reduction in mobility and independence, limits their social relationships and accelerates the progression of cognitive impairments. 49 -51
The magnitude of the effect on these improvements is considerable, and thus, it can be said to have a clinical significance, although it would be necessary to develop longer term studies in order to validate these results.
However, our findings are supported by previous studies, which also reported improvement in quality of life after GPR due to changes in the corporal representation and increased self-perception, which are associated with well-being and better postural conscience. 17,21
Limitations
Since this pilot study was designed and specifically focused on the treatment of patients with AD, the limitations were associated not only with the difference in the number of study groups but also with the difficulties encountered in providing information on this technique. The further limits consisted in identifying the residences where the certified therapists for the GPR performed their work; this was closely related to the distances among the residences where the study took place, which was directly connected to the fulfillment of the questionnaires. Moreover, the tests used fit within the ones applied in the residences such as MMSE and TS.
The equilibrium was evaluated only through TS, as the only degree applied to those centers without the presence of stabilometry, which would best suit the study. The lack of funds was of major importance in this study, as the geriatric centers do not have rehabilitation technology to assess equilibrium, walking measures, and so on, correctly.
Conclusions and Future Recommendations
The research results prove that GPR therapy does not only provide benefits in cognitive and neuropsychological aspects but also helps to enhance the autonomy of the participants and consequently the quality of their lives.
In this context, we suggest to use GPR as a slight therapy for painless movements, aiming to increase relaxation through breathing rhythm and to provide a positive experience in modifying the bodily behavior. The therapeutic session approaches can modify not only “postural attitude” but also the negative feelings of patients’ confidence, often associated with insecurity up to psychosomatic pain. Moreover, the abovementioned noninvasive procedure could be autonomously applied at patients’ home in accordance with the therapist’s recommendations.
A special attention should be paid to the further GPR implementation, through RCT examinations, concerning the randomization of participants, which would lead to homogenization in the number of participants. Moreover, it would be interesting to study even the comparison of patient pathways, depending on the different treatment centers.
It should also admit that the implementation of spirometry could also be very useful to measure the breath of air, in the inhalation–exhalation process with a maximal effort at the movement speed, as this examination could represent an assessment of breathing in the other RCT. The measurement of muscular strength through the electric digital dynamometer could also be useful, in order to obtain an interesting analysis concerning the implementation of an RCT study. Finally, it can be affirmed that this is a preliminary open study with severe limitations. Further validation should be investigated in the context of a RCT with a larger population.
However, the results of the current study should encourage the further exploration of experimental trials of stretching exercises, equilibrium, or GPR with the aim to preserve and potentially improve cognition, life quality, autonomy, performance, and relaxation in patients with AD. In this regard, future studies can verify the effects on the cognitive abilities obtained from the practice of a longer postural treatment by considering a follow-up period from 1 to 3 years.
Supplemental Material
Supplemental_materialTreatment_postures_new_(2) - An Experimental Pilot Study of Global Postural Reeducation Concerning the Cognitive Approach of Patients With Alzheimer’s Disease
Supplemental_materialTreatment_postures_new_(2) for An Experimental Pilot Study of Global Postural Reeducation Concerning the Cognitive Approach of Patients With Alzheimer’s Disease by Jasemin Todri, Orges Lena and José Luis Martínez Gil in American Journal of Alzheimer's Disease & Other Dementias
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.