
Abstract
Background:
The most common type of dementia is an Alzheimer’s disease which is a major concern in growing chronic diseases in the geriatric society, and its connection with biochemistry has not been sufficiently understood.
Objective:
This study aims to evaluate the effects of blood biochemistry on Alzheimer’s disease.
Method:
Eight participants aged 55+ with Alzheimer’s disease were analyzed. A cross-sectional work has conducted. Eighty patients have been divided into 2 groups as group A and group B according to laboratory findings including glycosylated hemoglobin, high-density lipoprotein (HDL), low-density lipoprotein (LDL), total cholesterol (TC), triglycerides (TGA), vitamin D, folic acid, and vitamin B12. Mean Mini-Mental State Examination scores between these different 2 groups have been compared.
Results:
High levels of HDL, vitamin D, and folic acid correlate with cognitive scores, whereas high levels of total cholesterol, HbA1c, LDL show a negative effect on cognition scores.
Conclusion:
High-density lipoprotein, vitamin D, folic acid, cholesterol, HgA1c, and LDL have an effect on dementia.
Introduction
Alzheimer’s disease (AD) is the most common type of dementia as it occurs in 60% to 70% of cases, 1 and it is associated with neurodegeneration resulting from astrogliosis, microglial cell proliferation, amyloid plaques, and neurofibrillary tangles. 2 Even though there are currently treatments that remove one or several symptoms of dementia, there is no treatment that cures or slows the progression of the disease. 3,4
As AD is usually due to aging, morphological and physiological changes that occur in older people play an important role in the course of the disease. Total body water diminishes with aging and the fat compartment roughly doubles to 30% of one’s body weight. Fat becomes more centrally distributed adding to adipose tissue. Major organ systems also begin to change both in function and morphology. 5 Absorption of some micronutrients degenerates, motility is decreased, and hepatic size, mass, and blood flow are decreased. The cardiovascular system changes dramatically, including increases in atrium size, thickening and calcification of heart valves, decreased gas exchange, and increased blood pressure. 5 Changes to the kidney and bladder include decreased kidney size, a decline in creatinine clearance, loss of nephrons, decreased ability to handle sodium and potassium loads, and a decrease in function of the glomeruli. 5 Given the number of these “normal” changes that occur with age, it is not surprising that some changes are seen in blood chemistry in older adults. For instance, glycosylated hemoglobin (HbA1c%) and folic acid levels increase, while vitamin D and vitamin B12 levels decrease. 6 The changes in these parameters have the potential to affect the development and progression of dementia. Thus far, few studies have investigated the connection between AD and biochemistry. 7 –10 These studies are usually focused on one parameter and the dementia level comparisons are mostly performed through Aβ and amyloid precursor protein (APP) expression levels. We utilized a cross-sectional study to evaluate the association between polypharmacy and AD, taking into account the interaction among Mini-Mental State Examination (MMSE) scores and biochemical data.
Methods
Study Design
This study has been approved by ethics noninvasive Clinical Research Ethics Committee of Bezmialem Vakif University, Istanbul, Turkey, with decision number of 2/4 on January 24, 2017. A cross-sectional study was conducted at the Bezmialem Vakif University Hospital, Istanbul, in March 2017. Patients with AD who contacted neurology clinic at Bezmialem Vakif University Hospital have been included in the study. Inclusion criteria were being in similar sociodemographic level, being older than 55 years, and being diagnosed with the AD. Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition) and Alzheimer's Disease and Related Disorders Association (ADRDA) criteria were used in diagnosing AD. Biochemical data have been collected from all patients, including HbA1c%, high-density lipoprotein (HDL), low-density lipoprotein (LDL), triglycerides (TGA), total cholesterol (TC), vitamin D, folic acid, and vitamin B12. Also, gliotic focuses have been assessed based on magnetic resonance (MR) imaging findings. All procedures involved in this study were explained to the participants. Patients’ caregiver took an informed decision to consent on behalf of patients in instances where they lacked capacity to consent themselves due to severe dementia.
Eighty patients have been divided into 2 groups, group A and group B, according to laboratory parameters. For each parameter, a reference point 6,11 has been assessed. Group A represented below the reference point, while group B represented above the reference point. In other words, patients of group A and B with indicative unique hospital numbers have been assessed for each laboratory parameter. Mean MMSE scores between patients in group A and group B have been compared.
Statistical Analyses
For the statistical analysis, IBM SPSS Statistics version 22.0 (Statistical Package for Social Sciences) for Windows 10.0 program was used. Distribution status of variables have been analyzed with Kolmogorov-Smirnov test; the result showed that variables are not distributed normally. Mann-Whitney U and Wilcoxon signed rank tests were used in the comparison of descriptive statistical methods (mean, standard deviation, minimum, and maximum) as well as quantitative data when study data were evaluated. The results were evaluated in a confidence interval (CI) of 95% and a significance level of P < .05.
Results
The sociodemographic features of the 80 participants have been summarized in Table 1. The mean age of participants was 76.71 ± 0.89 years and 40% of them were male and 60% were female. The averages of measured weight and height were 70.61 ± 12.04 kg and 158.58 ± 9.72 cm for all participants, respectively. The ratio of smoking participants was 5% and alcohol was 10% among all patients. According to data, 40% of the patients have no education, 20% have graduated only elementary school, 38% have graduated from middle school, and the remaining 2% have higher education.
Sociodemographics Features of Participants.
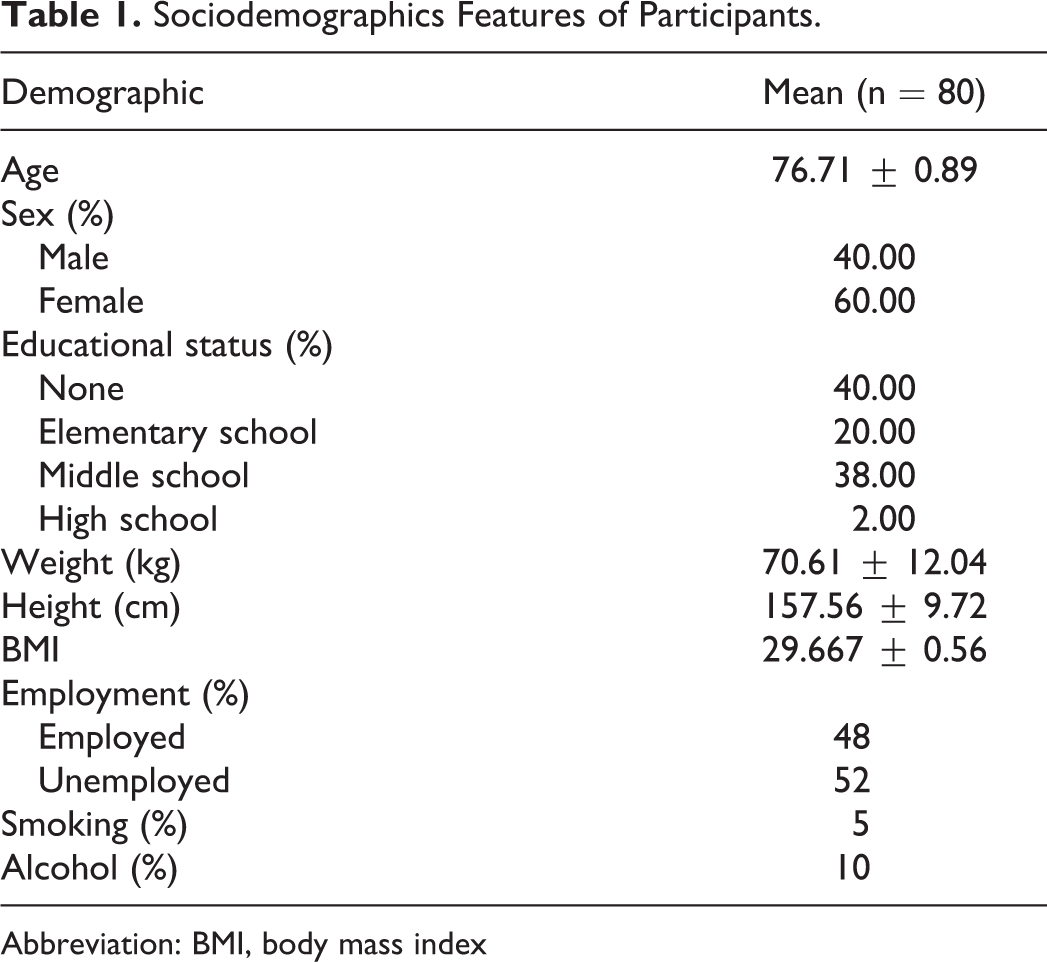
Abbreviation: BMI, body mass index
The mean serum levels of HbA1c% of all patients were 6.024 ± 0.10% (Table 2). As shown in Table 3, group AHbA1c consisted of 34 patients and the mean MMSE score was 17.6 ± 5.40. Group BHbA1c consisted of 46 patients and mean MMSE score was 16.9 ± 5.54 (Table 3). Also, there was no statistical significance between group AHgA1c and BHgA1c (Mann-Whitney U test; U = 671 500; P = .585; P > .05).
Mean Biochemical Results of Participants.
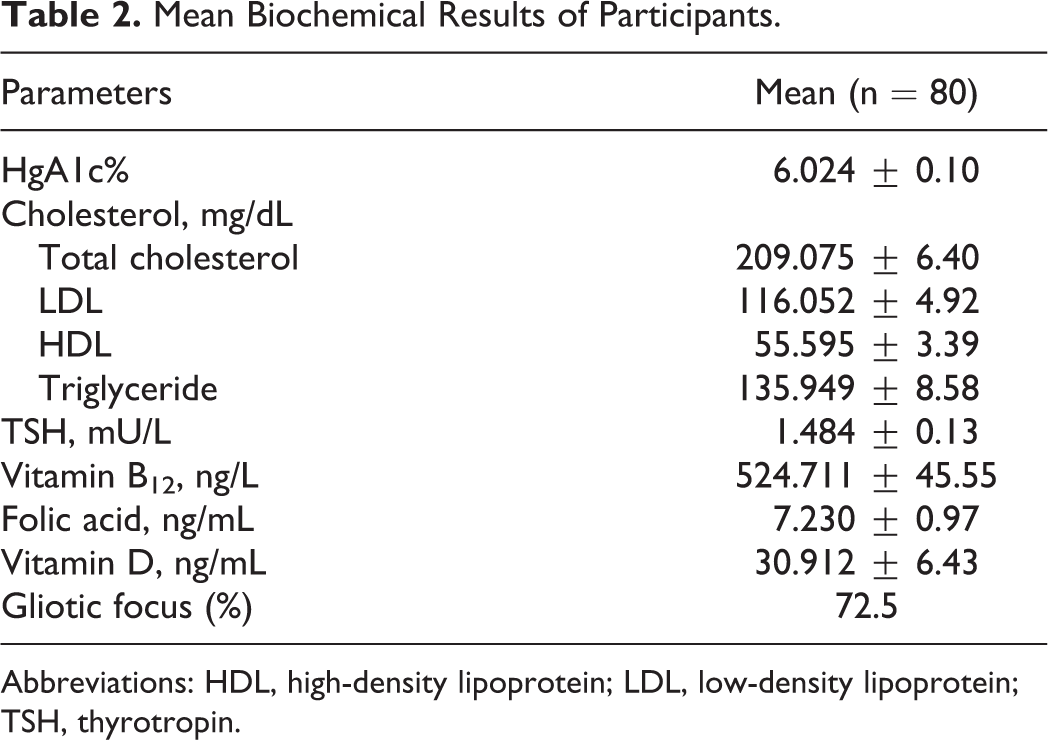
Abbreviations: HDL, high-density lipoprotein; LDL, low-density lipoprotein; TSH, thyrotropin.
Comparison of Median MMSE Scores of Groups A and B According to Biochemical Parameters Including Referece Intervals.
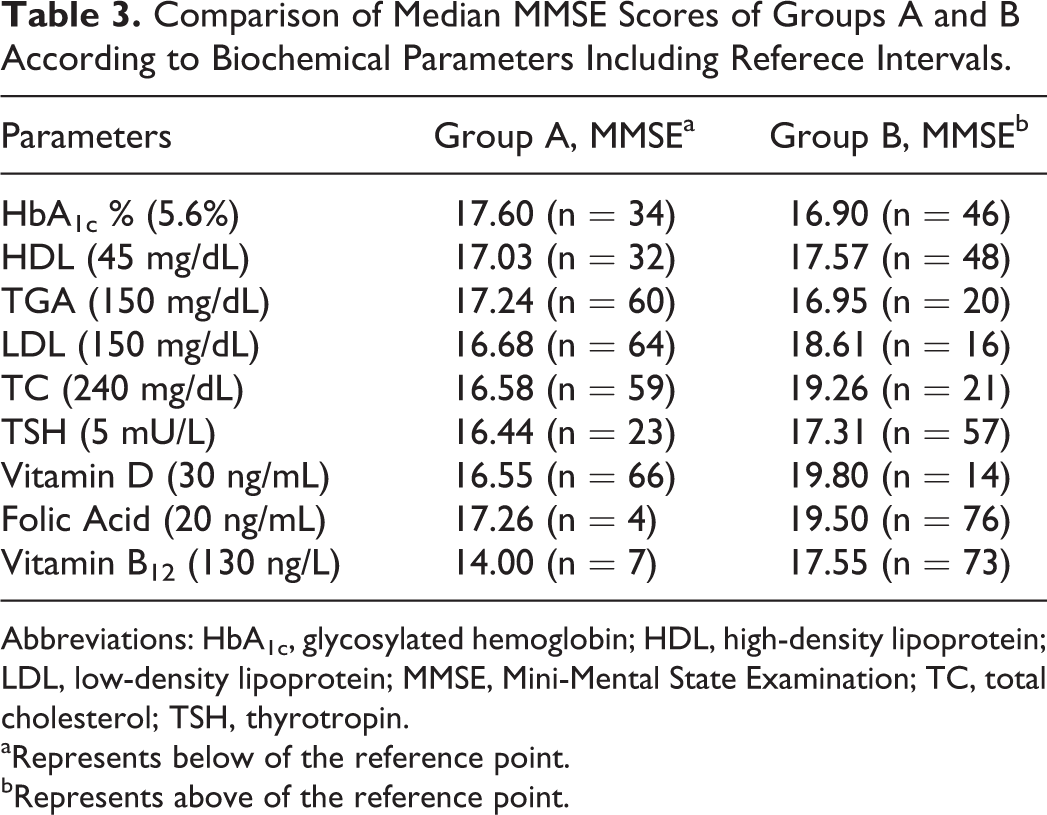
Abbreviations: HbA1c, glycosylated hemoglobin; HDL, high-density lipoprotein; LDL, low-density lipoprotein; MMSE, Mini-Mental State Examination; TC, total cholesterol; TSH, thyrotropin.
aRepresents below of the reference point.
bRepresents above of the reference point.
The mean serum levels of HDL of all patients were 55.595 mg/dL (Table 2). As shown in Table 3, group AHDL consisted of 32 patients and the mean MMSE score was 17.03 ± 5.18. Group BHDL consisted of 48 patients and mean MMSE score was 17.57 ± 5.59. There was no statistical significance between group AHDL and BHDL (Mann-Whitney U test; U = 777 500; P = .988; P > .05).
The mean serum levels of TGA of all patients were 135.949 mg/dL (Table 2). As shown in Table 3, group ATGA consisted of 60 patients and the mean MMSE score was 17.24 ± 5.44. Group BTGA consisted of 30 patients and mean MMSE score was 16.95 ± 5.66. There was no statistical significance between group ATGA and BTGA (Mann-Whitney U test; U = 581 500; P = .760; P > .05).
The mean serum levels of LDL of all patients were 116.052 mg/dL (Table 2). As shown in Table 3, group ALDL consisted of 64 patients and the mean MMSE score was 16.68 ± 5.30. Group BLDL consisted of 16 patients and mean MMSE score was 18.61 ± 5.49. There was no statistical significance between group AHDL and BHDL (Mann-Whitney U test; U = 447 500; P = .684; P > .05).
The mean serum levels of TC of all patients were 209.075 mg/dL (Table 2). As shown in Table 3, group ATC consisted of 59 patients and the mean MMSE score was 16.58 ± 5.14. Group BTC consisted of 21 patients and mean MMSE score was 19.26 ± 5.69. There was no statistical significance between group ATC and BTC (Mann-Whitney U test; U = 556 500; P = .564; P > .05).
Even though both the ATSH and BTSH groups showed the normal range of thyrotropin (TSH) levels, ATSH including 23 patients had a mean MMSE score of 16.44, while BTSH including 57 patients had an MMSE score of 17.31. There was no statistical significance between group ATSH and BTSH (Mann-Whitney U test; U = 667 500; P = .687; P > .05).
In Table 3, vitamin D and folic acid were evaluated. Group AvitD consisted of 66 patients and mean MMSE score was 16.55 ± 5.41. Group BvitD consisted of 14 patients and mean MMSE score was 19.80 ± 5.06. There was statistical significance between group AvitD and BvitD (Mann-Whitney U test; U = 457 500; P = .035; P < .05). Group Afolic acid consisted of 4 patients and mean MMSE score was 17.26 ± 5.45. Group Bfolic acid consisted 76 patients and mean MMSE score was 19.50 ± 4.80. There was no statistical significance between group Afolic acid and Bfolic acid (Mann-Whitney U test; U = 123 500; P = .567; P > .05).
Group AB12 consisted of 7 patients and mean MMSE score was 14.00 ± 6.58. Group BB12 consisted of 73 patients and mean MMSE score was 17.55 ± 5.34. There was no statistical significance between group Afolic acid and Bfolic acid (Mann-Whitney U test; U = 100 500; P = .267; P > .05; Table 3). According to the MR imaging, 73.42% of the participants had ischemic gliotic focuses on their brain imaging.
Discussion
The results of this study have shown that biochemical parameters have an effect on cognitive levels. In regard to the MR imaging, cerebrovascular pathology has revealed gliotic focus in AD patients’ autopsies with a ratio of 60% to 90%; cerebral amyloid angiopathy, endothelial degeneration, periventricular white matter lesions, and cerebral ischemia have been observed in many of them. 12
Glycosylated hemoglobin is a blood test used as diagnostic and monitoring factor for type 2 diabetes mellitus. Ramirez et al states that patients with HbA1c levels of 6.5% or higher have an increased risk to develop AD by 2.8 times. 13 We have evaluated the risk of an incident of AD according to this referenced parameter and observed an increased risk of the incident of dementia by elevated HbA1c% concentration. In a study that shows evidence to support the connection of diabetes with the subsequent cognitive decline, findings show a linear correlation between circulating HbA1c levels and cognitive decline, in any case of the diabetic condition. 14 Jana et al show in participants with hyperglycemia the rate of self-perceived cognitive blackouts were elevated and it was positively associated with the HbA1c levels higher than confirmed those correlations. 15 On a quantitative level, mainly HbA1c levels higher than 5.6% confirmed those correlations. 15 A small rise has been observed between HbA1c levels of groups. Our results showed that 12 patients (body mass index [BMI] > 30.06) with elevated levels of HbA1c are using combined therapy for the AD.
Gamba et al’s study has provided evidence linking altered cholesterol metabolism and hypercholesterolemia to amyloid plaque formation and tau hyperphosphorylation. 16 According to Hall et al, individuals with high TC had lower MMSE and significantly more neuropsychiatric symptoms (NPS) and more symptoms of psychosis. 17 Inconsistently with these results, in our study, the group A (lower TC group) scored significantly lower on MMSE. Considering that many more patients have been evaluated in these studies in comparison to ours, results can be reasonable. According to Proitsi et al, genetic inclination to increased blood cholesterol and triglyceride lipid levels is not associated with elevated late-onset AD risk. The observed epidemiological associations between abnormal lipid levels and late-onset AD risk could, therefore, be attributed to the result of biological pleiotropy or could be secondary to late-onset AD. 18 Since our results and other studies were unconvincing, the relationship among total cholesterol and dementia risk needs more investigation.
In aging and age-related neurodegenerative diseases, HDL plays an important role. 19 Khalil et al indicated that HDL from patients with AD is less able to control cholesterol efflux than HDL from healthy participants and that the decrease is substantially related to the state of the cognitive decline. 20 Since HDL from healthy participants and patients with AD were used at the same concentrations (denoted as total protein content), the diminish in the capacity of HDL to control cholesterol efflux is unlikely to be caused by an attenuation in HDL concentrations in patients with AD but rather by a reduction in their functionality. 20 Apart from this, a research showed that lower HDL-C is a risk factor for dementia for those who don’t have any other comorbidities, and lower HDL-C levels are seen among patients with AD compared to patients without AD. 21
According to Zheng et al, high levels of LDL values and low levels of HDL may cause worsening of the AD. 14 Kerrisk et al demonstrated that very-low-density lipoprotein (VLDL)-receptor polymorphism correlated with dementia risk, particularly with mixed and vascular dementia. 22 The LDL levels were observed to be significantly high both in the AD and ischemic stroke. 23 In our study, MMSE scores elevation correlates with LDL values. Usage of many antihyperlipidemic medications could be effective for these results because LDL levels of all groups are found in normal range. Keeping lipid level in the range could be another important factor for AD prognosis. Our results were similar with study carried out by Tynkkynen et al. 21,24 They pointed out that cholesterol-lowering medication affects lipoprotein levels, and these associations with incident dementia were weakened after regulating for BMI and cholesterol-lowering medication. 21,24 Association of total cholesterol in small VLDL (S-VLDL-C) with incident dementia can be largely clarified by elevated selective mortality. 24 Since our results and other researches fall satisfying, the relationship among HDL lipoprotein and LDL lipoprotein and dementia risk needs more investigation.
In our study, the group B (higher TC group) scored slightly lower on MMSE. Ohnuma et al states that effects of a medium-chain triglyceride were investigated, and as a result, it did not improve cognitive function in a sample of patients with AD, even in those patients without the ApoE4 allele. 25 In a single case observation, after 109 days treating with caprylic triglyceride, Montreal Cognitive Assessment (MoCA) scores changed from a baseline value of 24 to 28 and MMSE scores changed from 23 to 28. No changes were observed on 2-Deoxy-[18F]fluoro-D: -glucose positron emission tomography (FDG-PET) scans. The results suggest that, in a case of mild AD, caprylic triglyceride may have affected cognitive function, assessed by means of MMSE and MoCA, although glucose uptake and metabolism remained unchanged. 26
Even though all groups showed the normal range of TSH levels, 18 individuals with 2 mU/L had an MMSE score of 16.44, while other 57 individuals had an MMSE score of 17.31. Increased levels of TSH have destructive effects on the AD. Especially women are prone to be affected by raised levels of TSH. 15 Considering folic acid levels, 13 individuals with lower than 4 ng/mL had increased severity of AD with MMSE mean values of 14.07. For the remaining 62 patients, the MMSE mean score was 17.14. Folic acid has been associated with increased cognitive functions and significantly decreased inflammation. 27
In our study, we have demonstrated that almost all of our participants had low levels of vitamin D. Mann-Whitney U test was preferred for analyzing difference for groups analyses between MMSE scores and vitamin D levels (P < .035). Patients with vitamin D levels higher than 30 ng/mL had an MMSE score of 19.80 ± 5.06. On the other hand, patients with vitamin D levels less than 30 ng/mL had an MMSE score of 16.55 ± 5.41, as given in Table 3. According to research conducted by Miller et al, low levels of vitamin D lead to impaired episodic memory, semantic memory, visual perception, and motor functions. The study has shown that vitamin D levels have a direct impact particularly on cognitive functions and episodic memory. 28 Our results were similar with literature.
As to vitamin B12, several studies have consistently reported that there was no significant association between vitamin B12 level and the risk of AD. 29,30 In spite of the cross-sectional analysis results suggesting that low vitamin B12 level may correlate with decreased risk of the AD (Table 3), the association between vitamin B12 and AD risk was not conclusive and more studies are warranted on this issue. In our study, we have demonstrated that the mean MMSE score of group A of folic acid was lower than group B (Table 3). In a study that investigates 6 studies covering 2070 participants were included in the meta-analysis of the association between folic acid level and risk of the AD. The risk ratio (RR) was calculated to be 2.11 (95% CI: 1.51-2.71), which suggests that low folic acid level may correlate with increased risk of AD. 31
In conclusion, this study demonstrates that biochemistry has an effect on the course of the AD. High levels of HDL, vitamin D, and folic acid correlate with cognitive scores, whereas high levels of total cholesterol, HgA1c, and LDL show a negative effect on cognition scores. There is an enormous need for more detailed and larger clinical studies about the relationship between biochemistry and AD.
Footnotes
Acknowledgments
The authors of this study are thankful to Bezmialem Vakif University for the opportunities given. Settlement of study has been provided by Bezmialem Vakif University.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.