
Abstract
Objectives:
This study assessed a smartphone-based program to promote practical and mildly demanding arm responses and personal satisfaction and increase physical exertion (heart rates) in people with advanced Alzheimer’s disease.
Methods:
The program relied on a Samsung Galaxy A3 smartphone with Android 6.0 operating system. Two groups of 10 and 11 participants, respectively, were assigned different responses (ie, placing cards into an elevated box and moving bottles with water from a table into a container). Responses activated the smartphone, which produced brief periods of preferred stimulation. Lack of responding led the smartphone to produce a verbal prompt.
Results:
All participants had significant increases in independent response frequencies, level of personal satisfaction, and heart rates during program sessions as opposed to baseline or control sessions.
Conclusion:
A smartphone-based program may help people with advanced Alzheimer’s disease increase independent occupation with possible benefits in terms of satisfaction and physical condition.
Keywords
Introduction
Alzheimer’s disease is a neurodegenerative condition which has an increasingly larger incidence among older people (ie, people older than 65 years of age) with extremely serious personal and social consequences. 1 -4 In fact, people affected by the disease experience a progressive deterioration in their cognitive and behavioral functions, which eventually leads them to total dependence. 5 -7 Accordingly, their families as well as treatment and care centers in charge of their positive occupation and well-being are required to provide progressively higher levels of support, with growing emotional, practical, and economical costs. 2,3,8,9
At present, the disease is neither preventable nor curable. 10 -13 Pharmacological and behavioral interventions are being applied as ways to slow down the progress of the disease; alleviate some of the related functional, emotional, and physical drawbacks; and provide some respite to the persons affected and their staff and caregivers. Pharmacological interventions (eg, use of acetylcholinesterase inhibitors, antioxidants, and memantine) are typically combined with behavioral interventions. 10,14 Behavioral interventions can vary widely based on the stage of the disease. 10,15 -17
Behavioral interventions available for persons in the mild or early moderate stages of the disease may include (1) traditional approaches, such as reality orientation training, memory exercises, and reminiscence therapy, aimed at fostering cognitive functioning and communication 18 -21 and (2) technology-aided programs aimed at supporting different types of functional engagement concerning, among others, daily activities, leisure/entertainment, communication, and reminiscence. 22 -28 A technology-aided program for supporting engagement in daily activities, for example, may involve the use of a tablet that reminds the participants of the activities to carry out (ie, at the appropriate times of the day) and presents them with the instructions for the activity steps. 26
Behavioral interventions available for persons in the low moderate, or severe stages of the disease may include (1) various forms of environmental stimulation (eg, music stimulation, snoezelen, and aromatherapy) 29 -34 aimed at reducing problem behavior (eg, agitation) and improving general mood and (2) technology-aided programs aimed at promoting simple responses (eg, arm or leg movements, supported ambulation steps, and basic occupation). 35 -38 Within those programs, responses are automatically followed by preferred stimuli aimed at motivating their repetition and thus bringing about periods of potentially beneficial engagement with minimal staff supervision. Within a program for promoting leg movements, for example, a microswitch (sensor) may be used to monitor those movements and trigger computer delivery of preferred stimuli in relation to their occurrence. 36
In light of the relatively limited behavioral intervention data available with regard to the latter group of individuals, and the condition of passivity, detachment, and sadness that these individuals often experience, new research with them seems warranted. An immediate research objective might be to extend the assessment of technology-aided programs to determine their level of effectiveness in (1) supporting basic forms of occupational engagement (eg, use of different objects), which might also represent mild forms of physical exercise and (2) promoting individuals’ satisfaction with the engagement situation. 36,37,39,40
This study was an effort to advance research on technology-aided programs and, in particular, to address the aforementioned questions. The responses available for the participants to perform (1) were functional for them (ie, allowed them to access brief periods of preferred stimulation) and (2) consisted of practical, mildly demanding arm movements (ie, placing cards into an elevated box and moving bottles with water from a table into a container). The new program relied on the use of a smartphone, which was set up to monitor the responses and deliver stimulation and prompts. To determine the effects of the program, the participants’ independent responses, indices of personal satisfaction (eg, smiling and singing), and level of physical exertion (ie, heart rates) were measured during the program/intervention sessions as well as baseline or control sessions. 36,41,42
Method
Participants
Twenty-six individuals attending residential social–medical centers were recruited for the study according to purposive sampling. 43 Five criteria were used for their selection. First, the individuals were considered to be functioning in the low moderate, or severe stages of the disease. Second, the individuals tended to be inactive and disengaged unless directly supervised. Third, observations had shown that the individuals responded to (1) environmental stimulation such as popular songs and religious hymns (eg, by orienting or smiling) and (2) simple verbal prompts/encouragements (eg, by engaging in the task on hand). Fourth, observations had also indicated that the individuals were capable of performing the responses selected for the study. Fifth, families and staff supported a technology-aided program such as that planned for this study (ie, with simple activities and positive stimulation). Families had also signed a written consent form to authorize the individuals’ inclusion in the study. The study had been approved by the ethics committee of the Alzheimer Association, Bari, Italy.
The individuals were divided into 2 groups based on a convenience criterion. The 12 individuals of the first group were to perform the response of placing cards into an elevated box. The 14 individuals of the second group were to perform the response of moving water bottles. Two of the individuals included in the first group and 3 of those included in the second group left the program prematurely (ie, due to practical issues, health problems, or severe behavior deterioration). The remaining 10 individuals of the first group (referred to from here onward as participants 1-10) were between 74 and 93 (mean [M] = 83) years of age and had scores on the Mini-Mental State Examination 44 ranging from 9 to 14 (M = 11). The remaining 11 individuals of the second group (referred to from here onward as participants 11-21) were between 73 and 96 (M = 85) years of age and had Mini-Mental State Examination scores ranging from 6 to 14 (M = 10).
Setting, Sessions, Responses, and Stimuli
The setting for the study was a quiet area of the social–medical centers that the participants attended. The study included baseline, control, and intervention sessions. Sessions lasted 5 minutes and were carried out for each participant individually. Mostly, there were 3 to 5 sessions per day. During baseline and intervention sessions, the participant sat at a desk with cards or water bottles that they were to use for their responses. Figures 1 and 2 illustrate the position of the participants and the responses they were to perform (ie, placing cards into an elevated box and moving bottles from a table into a container). Those responses were selected in cooperation with physiotherapists based on the fact that they were feasible for the participants and their execution required the participants some physical effort (ie, their execution could represent a mild/beneficial form of physical exercise for the participants). During the control sessions, the participants sat quietly with no activity material available.
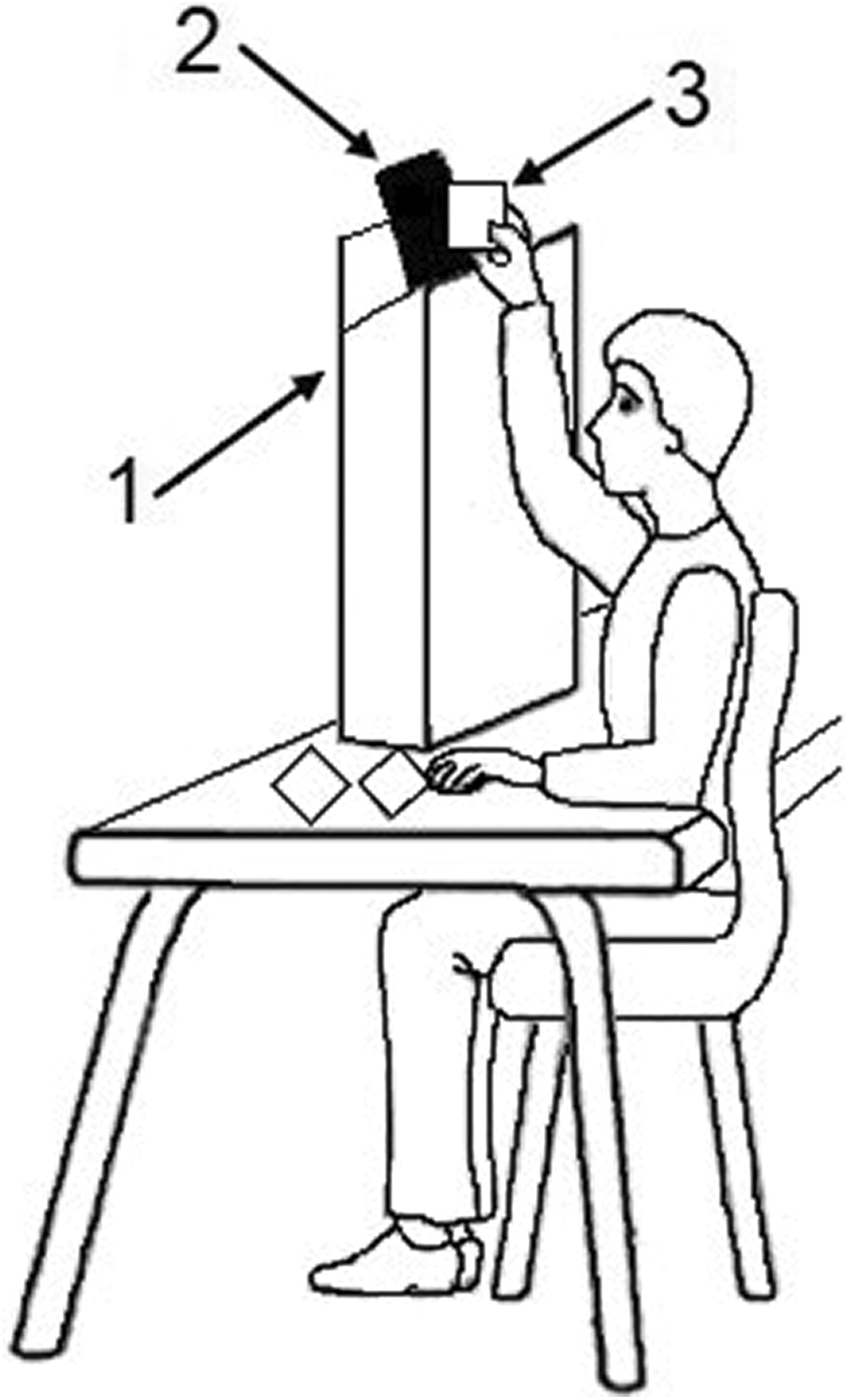
The drawing represents a participant sitting at a table with cards, in front of an elevated box (1), with a smartphone (2) attached to the box’s opening, and placing a card (3) into the box, thus activating the smartphone.

The drawing represents a participant sitting at a table with bottles, next to a container (1), with a smartphone attached to the container’s opening (2), and placing a bottle (3) into the container, thus activating the smartphone.
Popular songs or popular songs and religious hymns were the stimuli used contingent on the participants’ responses. Those stimuli were recommended (ie, were deemed preferred by the participants) by families or staff and were selected for the study after a brief preference screening. The screening consisted of presenting each participant with two 10-second segments of the single stimuli being screened, for about 10 nonconsecutive times over several assessment sessions. 31,45 A stimulus was used during the intervention if the research assistant and staff member involved in the screening agreed that the participant exhibited forms of orientation or indices of satisfaction (see above) during about or more than 50% of the stimulus segments’ presentations.
Smartphone and Wristwatches
The program version available for the first group of participants who placed cards into an elevated box relied on a Samsung Galaxy A3 smartphone with Android 6.0 operating system, near-field communication function, and WPC-Walden Personal Communicator and MacroDroid applications. The smartphone was supplied with a large variety of audio files containing the participants’ preferred songs and could be linked to a mini speaker. The cards available to the participants for the responses showed the images of their preferred singers and were fitted with special radio frequency code tags. Usually, a participant had about 30 cards concerning a few singers and songs. The tags differentiated the cards regarding the singer they represented. Placing the cards in the elevated box made the cards touch the back of the smartphone positioned there (ie, before falling into the box; see Figure 1) and activate its near-field function. This function together with the WPC application allowed the discrimination of the code tags attached to the cards and led the smartphone to open the files corresponding to those tags and thus play 10-second segments of preferred songs of specific singers. The MacroDroid application was set to ensure that a smartphone verbal prompt/encouragement occurred if the participant did not have a new response within 10 to 15 seconds from the end of the previous stimulation (ie, during intervention). The same application was also set to ensure that responses and prompts were automatically recorded.
The program version used for the second group of participants, whose response consisted of moving bottles into a container, relied on the Samsung Galaxy A3 smartphone with the MacroDroid application. This application ensured the delivery of a 10-second stimulation segment for each response as well as the delivery of prompts and the recording of responses and prompts (ie, see above). The responses were detected by the light sensor of the smartphone, which was fixed at the opening of the container.
Wristwatches with built-in heart rate monitor (ie, Garmin Vivosmart HR or TomTom Runner Cardio) were used to record the participants’ heart rates during intervention and control sessions. The wristwatches were considered to be reliable in recording heart rates based on previous checks carried out with research assistants. 41
Measures and Data Recording
Four measures were recorded, that is, card or bottle responses, smartphone prompts, heart rates, and indices of satisfaction. The frequencies of cards placed into the box, bottles moved into the container, and prompts occurred were recorded automatically by the smartphone during (1) the baseline and intervention sessions (card and bottle responses) or (2) the intervention sessions (prompts). Heart rates were recorded as mean rates per session via a wristwatch with heart rate monitor, which the participants wore. Recording was carried out for each participant over 21 to 38 pairs of sessions. Each pair included a control and an intervention session. The intervention session always occurred immediately after the control session. Indices of personal satisfaction (ie, smiling, singing, moving parts of the body with music, or making positive verbal statements 37 ) were recorded by research assistants during the baseline and intervention sessions. Recording occurred according to a partial interval system, in which 10-second observation intervals were followed by 5-second scoring periods. 46 Interrater agreement on this last measure was assessed in more than 20% of the single participants’ sessions, with a research assistant and a reliability observer involved in data recording. The percentages of agreement computed for the single sessions (by dividing intervals with identical scores by the total number of intervals and multiplying by 100%) were normally within the 80 to 100 range, with means greater than 90 for all participants.
Experimental Conditions and Data Analysis
A nonconcurrent multiple baseline design across participants 47 was used for each group of participants. The participants started with 4 to 10 baseline sessions, according to design requirements. Then, they had 64 to 120 intervention sessions (with differences in the number of sessions largely due to participants’ availability). The participants’ baseline and intervention data for card and bottle responses and indices of satisfaction were summarized as means per session (with session ranges) for the single participants of each group and reported in tables. An identical approach was used for the control and intervention data on heart rates, that is, the data collected over 21 to 38 pairs of sessions (see Measures and Data Recording).
The percentage of nonoverlapping data (PND) method 48 and paired t tests 49 were used to determine the effect size of the intervention. The PND was calculated for the single participants of the 2 groups by comparing the baseline and intervention session values on card or bottle responses and indices of satisfaction. Paired t tests were used to assess the differences between the participants’ heart rates in the control sessions and in the subsequent intervention sessions (ie, the differences across the multiple pairs of control and intervention values of each participant of the 2 groups).
Baseline Sessions
During the baseline sessions, the participants had the cards with the smartphone placed in the elevated box or the bottles with the smartphone placed inside the container. The smartphone recorded the participants’ card or bottle responses but did not provide stimulation or prompts. Prior to the start of the sessions, a research assistant used verbal and physical guidance to help the participants produce a response (ie, place a card in the elevated box or a bottle in the container).
Intervention Sessions
During the intervention sessions, conditions were as during the baseline except that the smartphone (1) presented a 10-second stimulation segment after each card or bottle response, (2) provided a prompt to respond if the participant did not have a new response within 10 to 15 seconds from the end of the previous stimulation segment, and (3) recorded the responses and prompts. During 21 to 38 intervention sessions, which were distributed across the intervention phase and were preceded by control sessions, heart rates were also recorded (see Measures and Data Recording). The intervention phase was introduced by 4 to 6 practice sessions, during which the research assistant used verbal and physical guidance to help the participants perform the responses and experience music stimulation independent of and following smartphone prompts.
Control Sessions
The control sessions served to determine the participants’ heart rates immediately before the start of intervention sessions. The participants sat at a desk without cards/bottles, smartphone, or stimulation.
Results
Tables 1 and 2 report the participants’ numbers of sessions and their mean frequencies of card or bottle responses and mean percentages of intervals with indices of satisfaction per session (with session ranges) during the baseline and the intervention. During the baseline phase, the participants’ mean frequencies of responses per session varied between 0 and 1 for the first group and 0 and 3 for the second group. During the intervention phase, the mean frequencies of responses per session varied between about 11 and 15 for the participants of the first group and between about 8 and 16 for the participants of the second group. Comparisons of the baseline and intervention data, according to the PND method, showed indices of 1.0 for all participants (ie, the participants’ intervention data values always exceeded their baseline data values), implying a strong effect of the program. The mean frequencies of smartphone prompts, which are not reported in the tables, varied between less than 1 and about 3 (with an overall mean of less than 2) for the participants of the first group and between close to 0 and about 6 (with an overall mean of about 3) for the participants of the second group.
First Group: Participants’ Number of Sessions (Sessions), Mean Frequencies of Card Responses (M Freq CR), and Mean Percentages of Intervals With Personal Satisfaction (M % PS) With Related Session Ranges, During Baseline and Intervention.a
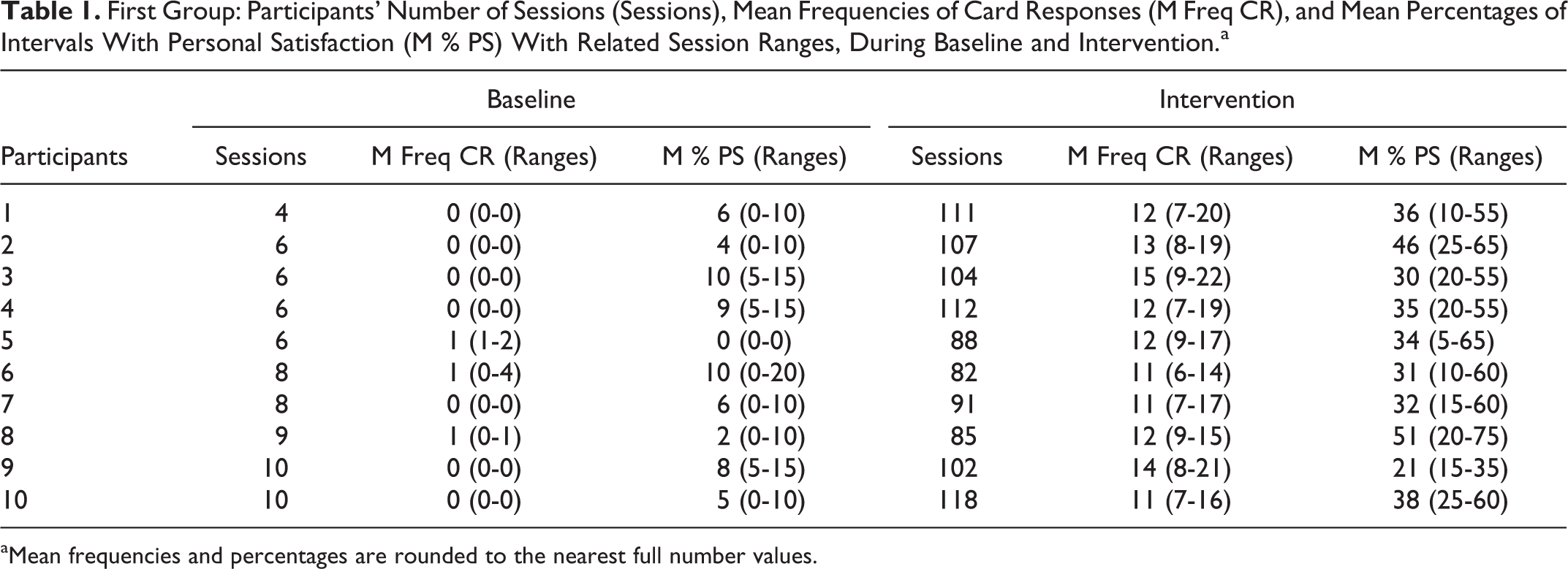
aMean frequencies and percentages are rounded to the nearest full number values.
Second Group: Participants’ Number of Sessions (Sessions), Mean Frequencies of Bottle Responses (M Freq BR), and Mean Percentages of Intervals With Personal Satisfaction (M % PS) With Related Session Ranges, During Baseline and Intervention.a
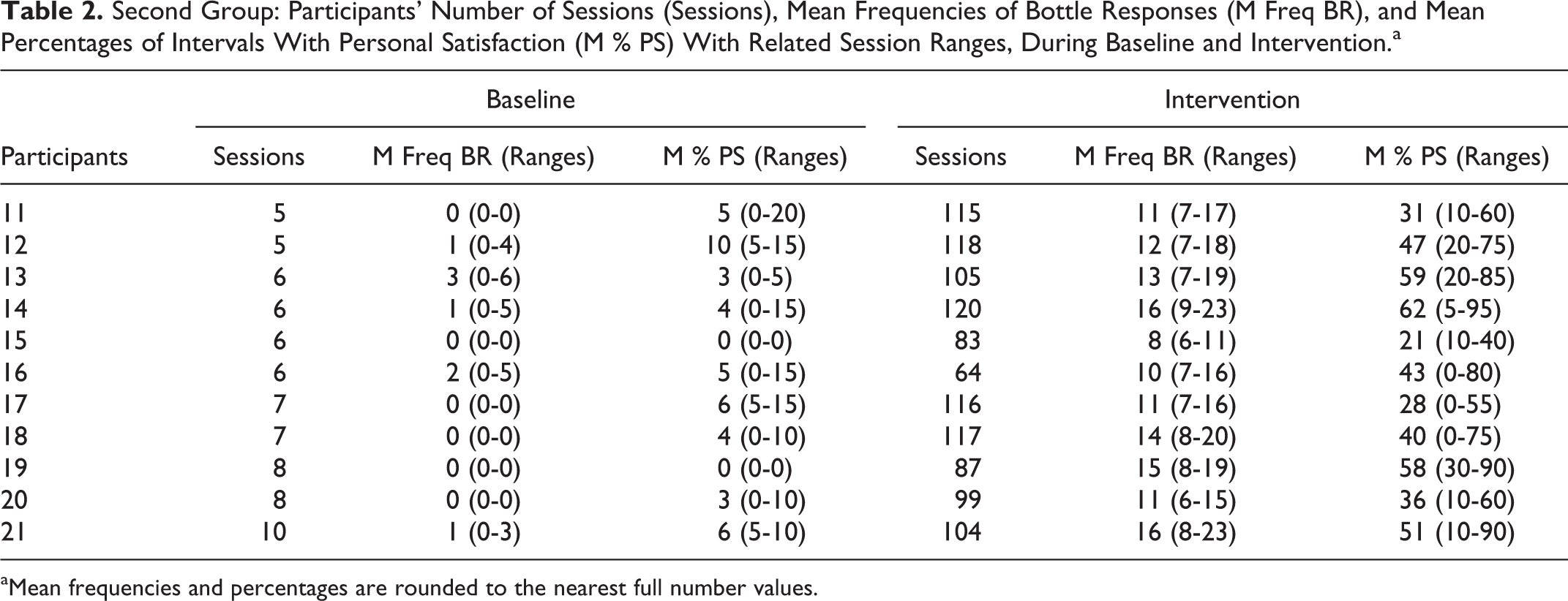
aMean frequencies and percentages are rounded to the nearest full number values.
The participants’ mean baseline percentages of intervals with indices of satisfaction varied between 0 and 10 for both groups. The mean intervention percentages varied between about 20 and 50 for the participants of the first group and between about 20 and 60 for the participants of the second group. Comparisons of the baseline and intervention data via the PND method showed indices ranging between 0.9 and 1.0 (ie, indicating strong effect of the program) except for participant 6 of the first group and participants 11 and 17 of the second group. Their indices were 0.83, 0.86, and 0.82, respectively (still indicating a fairly positive effect of the program).
The control and intervention heart rates for the 2 groups of participants are reported in Tables 3 and 4, respectively. The participants’ mean heart rates during the control sessions varied between 72 and 79 and between 56 and 84 for the 2 groups, respectively. The participants’ mean heart rates during the intervention sessions varied between 79 and 84 and between 68 and 95 for the 2 groups, respectively. The mean rate increase from control to intervention sessions was about 7 for the participants in the first group and about 9 for the participants in the second group. The paired t tests carried out for the single participants showed that the differences between control and intervention heart rates were significant (P < .01) in each case, with t values ranging from 3.72 to 14.48.
First Group: Participants’ Mean Heart Rate Values (and Ranges) Across the Control and Intervention Sessions Whose number (No.) Is Specified.a
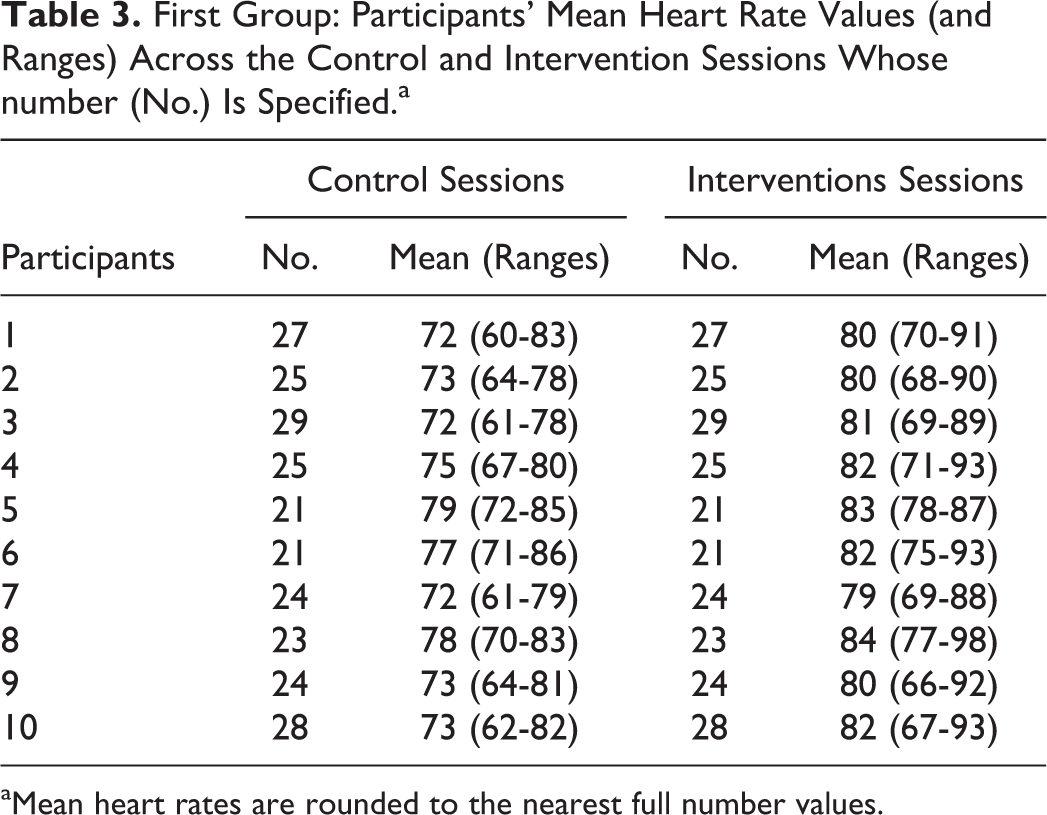
aMean heart rates are rounded to the nearest full number values.
Second Group: Participants’ Mean Heart Rate Values (and Ranges) Across the Control and Intervention Sessions Whose Number (No.) Is Specified.a
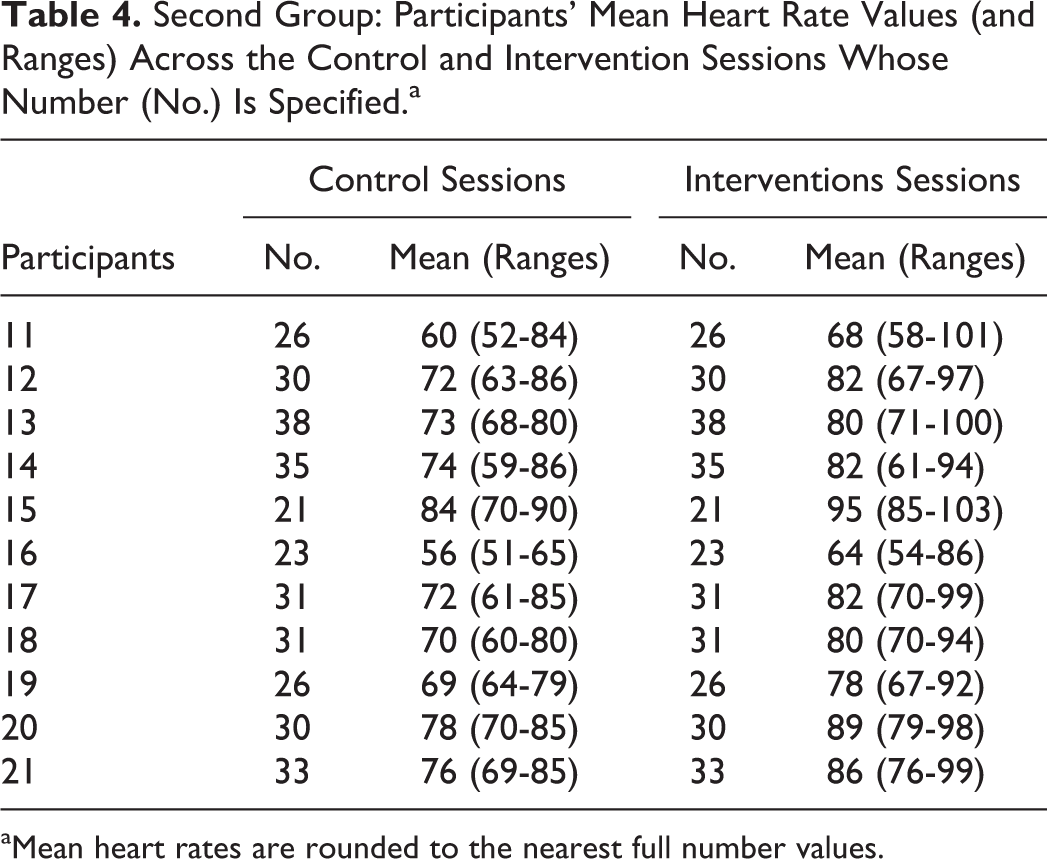
aMean heart rates are rounded to the nearest full number values.
Discussion
The results of this study seem to provide encouraging evidence regarding the issues addressed. Specifically, they (1) indicate that the smartphone-based program was effective in fostering activity engagement and personal satisfaction in participants with advanced Alzheimer’s disease (thus supporting/strengthening preliminary data in the area) 35 -37 and (2) show that functional and slightly demanding response engagement, particularly the engagement concerning the manipulation/moving of bottles, could represent a form of mild physical exercise with potential benefits for the participants’ general condition. 39,40 In light of these results, a few considerations can be made.
First, the positive results obtained with the smartphone-based program suggest that such program may easily replace previous ones based on more complex technology (ie, on computer systems and microswitches). 36 This evidence is practically relevant, since a smartphone is rather easily accessible and affordable compared to the technology used before. In spite of its accessibility, however, the smartphone requires a certain amount of preparation before it can be used for the program. Indeed, one needs to fit the smartphone with a variety of files concerning the participants’ preferred stimuli as well as the prompts. Moreover, the WPC and/or MacroDroid applications are to be arranged properly to automate the functioning of the smartphone according to the intervention conditions.
Second, the use of brief periods of preferred stimulation contingent on the responses was probably critical to motivate the participants to engage in such responses and maintain their independent engagement over time. 50 The use of prompts automatically delivered by the smartphone seemed also to have an important role in promoting the participants’ independence. In fact, prompts may have curbed interruptions in performance, which are fairly common at a late stage of the disease, and thus ensured a sustained level of engagement and stimulation. 50 The participants’ independent engagement may be considered a critical achievement (1) underlining the effectiveness of the program and (2) suggesting its apparent suitability for daily contexts where human resources are often limited. 9,51,52
Third, the responses used in this study may be helpful to increase the participants’ level of attention to and interaction with the immediate surrounding (ie, more helpful than responses that are not related to specific objects within the context). Object-related functional responses could also be more easily appreciated by staff and caregivers and promote their positive opinion about and consequent support for the program. 9 This aspect together with the fact that participants had a significant increase in the level of personal satisfaction during the intervention sessions may have important implications. On the one hand, the participants’ involvement in the program could be viewed as a constructive and enjoyable experience that (1) is likely to have an impact on their general mood and quality of life 9,52 and (2) fully justifies and encourages efforts to foster the use of basic activity in individuals with advanced Alzheimer’s disease. 37,53 On the other hand, the participants’ positive engagement and satisfaction could help staff and caregivers accept the program more easily and arrange favorable conditions for its use. 54
Fourth, the heart rate data represent preliminary evidence in this area and suggest that simple and fairly viable activities such as those included in this study may represent forms of mild physical exercise for participants with advanced Alzheimer’s disease. 37,39,55 While it is difficult to judge the beneficial impact of the heart rate increases reported in this study (ie, due to the absence of reference/interpretation criteria), it seems reasonable to believe that involving the participants in several activity sessions per day may produce meaningful physical benefits. 40,56,57
Fifth, a main limitation of this study is the failure to include a social validation of the program through interviews of staff and caregivers. A social validation would have identified the opinion of staff and caregivers about the impact, practicality, and applicability of the program in daily contexts. 58,59 A second limitation concerns the inability to draw conclusions from the heart rate data, as there are no clear parameters or scales for interpreting them. While they appear encouraging, new research efforts are needed to help clarify the value and implications of the rate increases obtained in this study and set parameters for new work in the area. 57 A third limitation concerns the relatively small number of participants included and, even more importantly, their use of few, fairly short intervention sessions per day. To determine the program’s potential contribution within daily contexts, new research should assess whether longer sessions and/or larger numbers of sessions per day can be profitably implemented. 60,61
In conclusion, the results of this study provide encouraging answers with regard to the possibility of (1) supporting independent activity engagement and fostering personal satisfaction in people with advanced Alzheimer’s disease and (2) using relatively purposeful and mildly demanding responses that can represent a form of gentle physical exercise for a number of those people. New research will need to address the limitations of this study and also investigate new forms of activity and new responses that could extend the range of engagement options available for the participants.
Footnotes
Authors’ Note
The ethics committee of the Alzheimer Association, Bari, Italy, approved the study. Families provided written informed consent for the participants’ involvement in the study. All procedures performed were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.