
Abstract
Background:
The study aimed to compare neuropsychiatric symptoms (NPS) in people with early-onset Alzheimer’s disease (EOAD) and late-onset AD (LOAD).
Methods:
Fifty-six participants with LOAD and 24 participants with EOAD having mild dementia were assessed for NPS for their frequency, severity, and caregiver distress as measured by Neuropsychiatry Inventory (NPI) along with assessments of cognition and functional dependence.
Results:
Participants with EOAD and LOAD were not significantly different for total NPI score (P = .057). Early-onset Alzheimer disease had greater prevalence of all the NPS except apathy. Participants with EOAD were significantly worse on anxiety (P = .03), irritability (P = .01), and sleep (P < .01) subscales and their carers significantly more distressed by their irritability (P = .002) and sleeping patterns (P = .005). Regression analysis showed that higher NPI score was associated with longer duration of illness in EOAD and higher functional dependence in LOAD.
Conclusions:
The NPS severity was similar between EOAD and LOAD although EOAD had higher symptom prevalence and carer distress.
Keywords
Introduction
Dementia is a neurodegenerative disorder affecting over 46 million people worldwide, and Alzheimer’s disease (AD) is the most common form of dementia that typically occurs in late life, but in approximately 4% of cases it occurs in people younger than 65 years old (early onset). 1 –3 Although the underlying neuropathological hallmarks are the same, there is some evidence that there are differences in aspects of the disease between early-onset AD (EOAD) and late-onset AD (LOAD). Research has suggested that the rate of progression of the disease is more rapid in EOAD 4,5 and that there are differences in the distribution of atrophy in the gray matter 6 and genetic differences. 5 Other studies have shown differences in the initial clinical presentation of the illness 7 and the pattern of types of memory problems between EOAD and LOAD. 8 –11 Studies have demonstrated EOAD has greater behavioral problems, more rapid cognitive decline, and increased language difficulties. 12 In addition, the earliest symptoms of dementia in those younger than 65 years are typically nonamnestic 13 and may contribute to the delay in diagnosis.
Neuropsychiatric symptoms (NPS) in dementia have been found to complicate the course and management of the disease and has been associated with accelerated progression of cognitive decline 14 and an increased risk of early institutionalization. 15 Much research has identified the presence of NPS in late-onset dementia, 16 –21 and some previous studies found higher NPS in EOAD, mostly affective symptoms. 22 –25 However, there were variabilities in the 2 groups in terms of a difference in Mini-Mental State Examination score (MMSE) or disease severity and functional abilities between the groups. Presence of NPS in early-onset cases may delay the diagnosis, as it can often be misinterpreted as primary psychiatric condition rather than associated with neurodegenerative disorders. 26 A recent review 27 has called for studies using consistent measures of NPS, examining NPS individually and the distress caused to caregivers by them. Further clarifying these is important for clinical care, especially as little is known about caregiver distress in EOAD. This study aims to compare prevalence of individual NPS, severity, and impact on carers as indicated by carers’ distress between patients with EOAD and LOAD, as indicated by their scores on the Neuropsychiatric Inventory (NPI). 28
Methods
Participants
Participants with AD (with an MMSE of 15-25), LOAD (n = 58) who had onset after the age of 65 years, and EOAD (n = 24) who had onset of illness before 65 years of age were recruited from consecutive referrals from memory services of the South London and Maudsley NHS Foundation Trust, United kingdom, and Leicestershire Partnership NHS Trust, United Kingdom. Diagnosis of probable AD was made for all participants according to the National Institute of Neurological and Communicative Diseases and Stroke/Alzheimer’s Disease and Related Disorders Association criteria. 29 The exclusion criteria were dementia other than AD, history of neurological disorder, or major psychiatric disorder, including substance abuse and absence of a carer to provide information for NPI. Patients were excluded if they were between 65 and 70 years in order to ensure that individuals who were diagnosed with AD after 65 years of age had not developed symptoms before they were 65 years old but had delayed diagnosis. Two patients were excluded for this reason—67-year-old male (25/30 on MMSE, NPI score of 3, and 6 months of illness duration) and a 69-year-old female (13/30 on MMSE, NPI score of 7, and 24 months of illness duration).
All participants gave informed consent to participate in the study. The study had ethics approval from the regional research ethics committee.
Assessments
Assessments included cognitive testing with MMSE 30 ; noncognitive symptoms using NPI 28 which was completed with the carer, and daily activities with Bristol Activities of Daily Living Scale (BADLS). 31 Information pertaining to the participant’s family history of memory problems, duration of illness, and the number of years of education were elicited from the participant and their carer.
The NPI measures the frequency and severity of 12 psychiatric and behavioral symptoms/domains (NPS) on the basis of caregiver report 28 (delusions, hallucinations, agitation/aggression, depression/dysphoria, anxiety, elation, apathy/indifference, disinhibition, irritability/lability, aberrant motor behavior, sleep disturbance, and appetite and eating disorder). 32 For each domain, the NPI begins with a screening question (yes or no, to indicate presence vs absence of this symptom), followed by 7 to 8 more specific follow-up questions to determine the nature of the overall symptom endorsed (again, in yes/no format). The caregivers were asked to rate the overall frequency 1 to 4 and severity 1 to 3 of all the symptoms, thus providing an overall index of symptom severity. Test–retest reliabilities for this measure range from 0.64 to 0.71. 32,33 The caregivers also scored their own distress for the individual patient’s symptoms (scores range from 0 to 5), and the total caregiver distress score was calculated.
Statistical Analysis
Statistical analysis was performed using IBM SPSS statistics version 24. Nonparametric analyses were performed as the data showed nonnormal distribution. Chi-square tests were used to explore differences in categorical data (with Fisher exact test for multiple analyses) and Mann-Whitney U tests for continuous variables. Analyses were carried out to explore the differences between EOAD and LOAD groups in terms of family history of memory problems, duration of symptoms, and the number of years of education as well as total NPI (sum of frequency × severity subscale scores) and NPI-subscale scores (frequency × severity) and carer distress score (individual NPS and total). Linear regression analysis was carried out with NPI total as dependent variable and MMSE, age, gender, education, duration of illness, family history, and activities of daily living (ADL) entered as the predictive variables.
Results
There were 56 patients in the LOAD group and 24 patients in the EOAD group. Table 1 shows demographic data for each group. The EOAD group had significantly longer duration of symptoms at the time of assessment than the LOAD group (Mann-Whitney U test; P < .01) but were not significantly different in terms of gender, years of education, family history of dementia, MMSE or BADL score. The participants were mostly white British except 4 Asian in EOAD group and 3 Afro-Caribbean in LOAD group. The EOAD group had a higher proportion of individuals with a family history of dementia, but this was not statistically significant (χ2 = 2.23; P = .14).
Comparison of Sociodemographic and Clinical Parameters Between the Groups Early-Onset Alzheimer’s Disease (EOAD) and Late-Onset Alzheimer’s Disease (LOAD).a
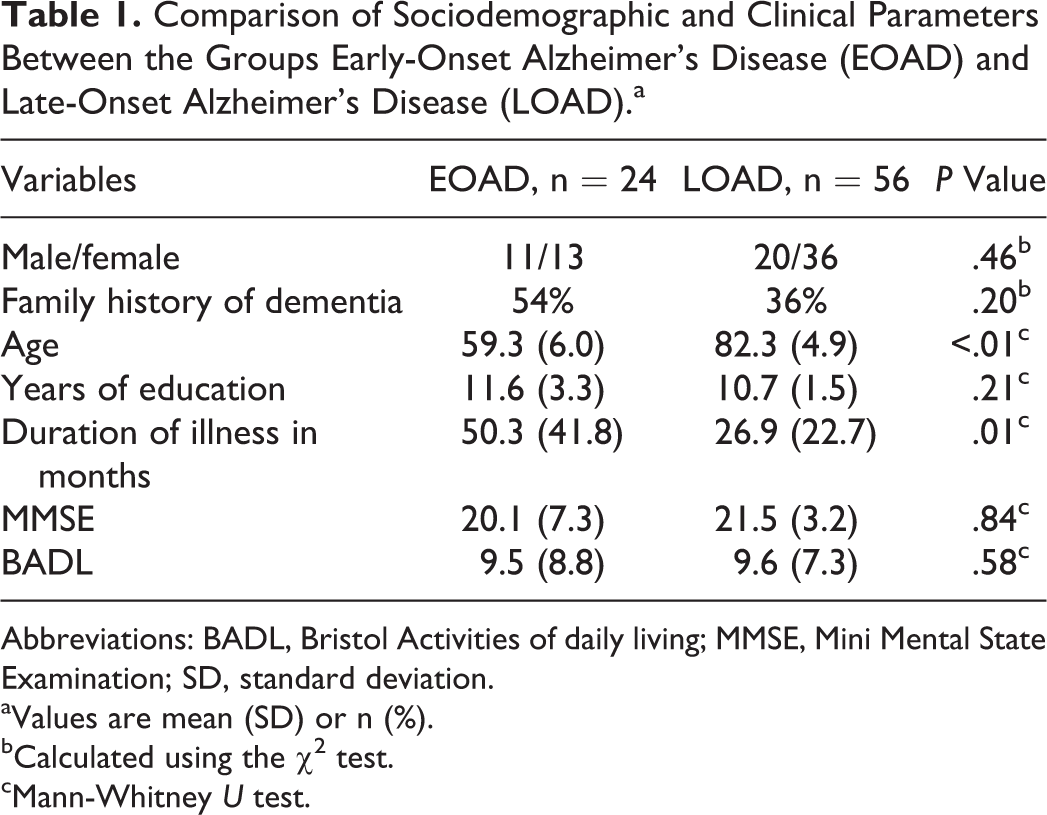
Abbreviations: BADL, Bristol Activities of daily living; MMSE, Mini Mental State Examination; SD, standard deviation.
aValues are mean (SD) or n (%).
bCalculated using the χ2 test.
cMann-Whitney U test.
The 2 groups were not different for previous psychiatry history (ie, depression or anxiety) or use of antidepressants. No patients had history of previous psychosis or substance-related disorder. None of the patients on the LOAD group had been commenced on antidementia medications at the point of assessments. Fourteen (58%) patients with EOAD were commenced on one or other of the antidementia medications (donepezil [10], galantamine [3], or memantine [1]). This was because interested participants with LOAD could be recruited soon after their clinical assessments and diagnosis; however, this was not possible for patients with EOAD due to unavailability of carers who were working or had child-care responsibilities, and some patients and carers needed more time to accept and adapt to the AD diagnosis before participation. However, there was no difference in total NPI scores (P = .141) or carer distress (P = .189) between patients with EOAD with and without antidementia medications.
The overall total NPI score was not significantly different for the EOAD group compared to LOAD (Mann-Whitney U test; P = .057). However, patients with EOAD had higher prevalence of all symptoms except apathy and scored higher (symptom frequency × severity) than the LOAD group on the anxiety, irritability, and sleep subscales (Table 2). Figure 1 shows the percentage of participants in each group who reported symptoms in each subscale. The total carer distress was higher for EOAD although not statistically significant. However, when tested for individual NPS, the carers’ distress was significantly higher in EOAD group for irritability (Mann-Whitney U test; P = .002) and sleeping patterns (Mann-Whitney U test; P = .005; Table 2).
Comparison of Neuropsychiatry Inventory Scores Between Early-Onset Alzheimer’s Disease (EOAD) and Late-Onset Alzheimer’s Disease (LOAD; Mean [standard deviation]).
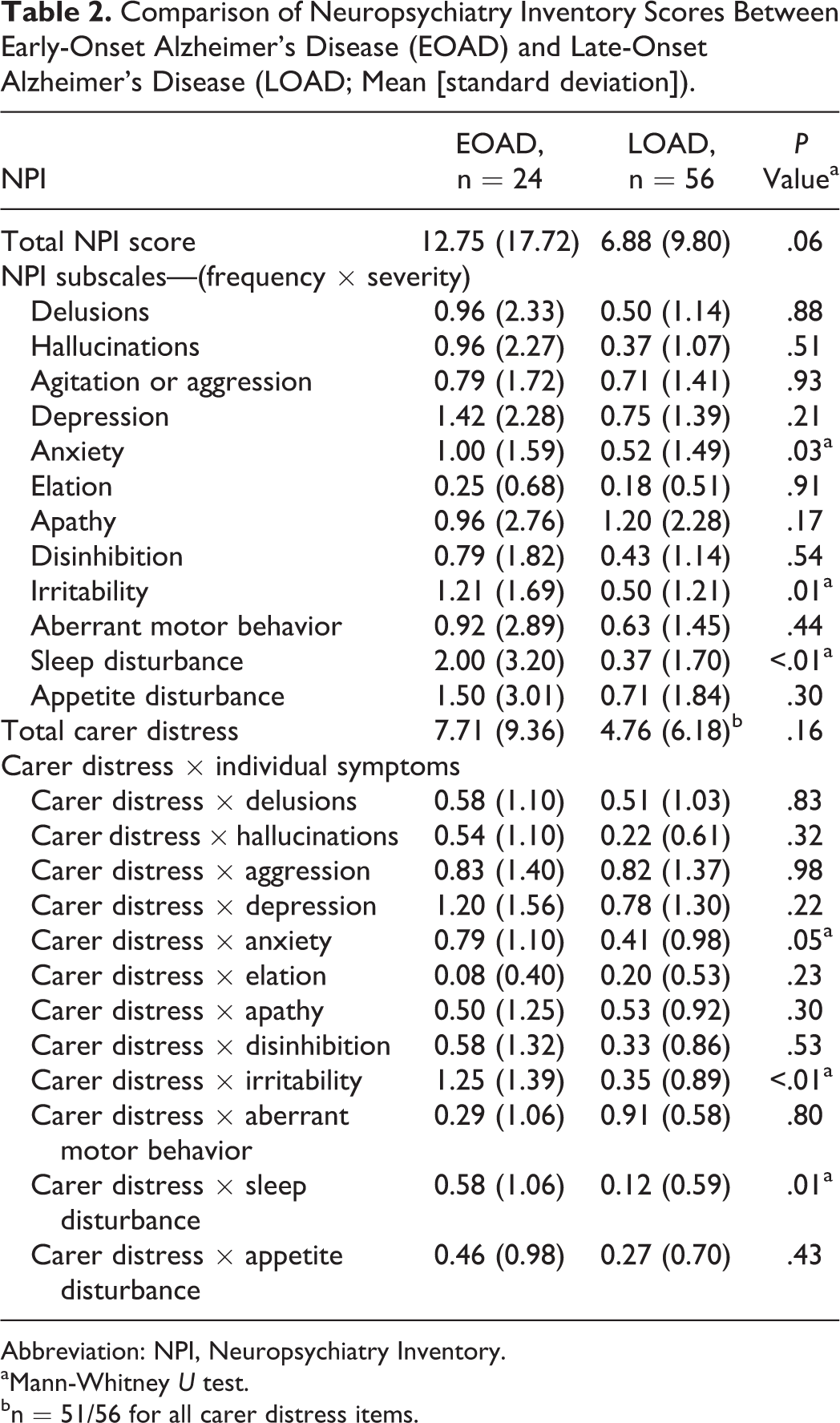
Abbreviation: NPI, Neuropsychiatry Inventory.
aMann-Whitney U test.
bn = 51/56 for all carer distress items.
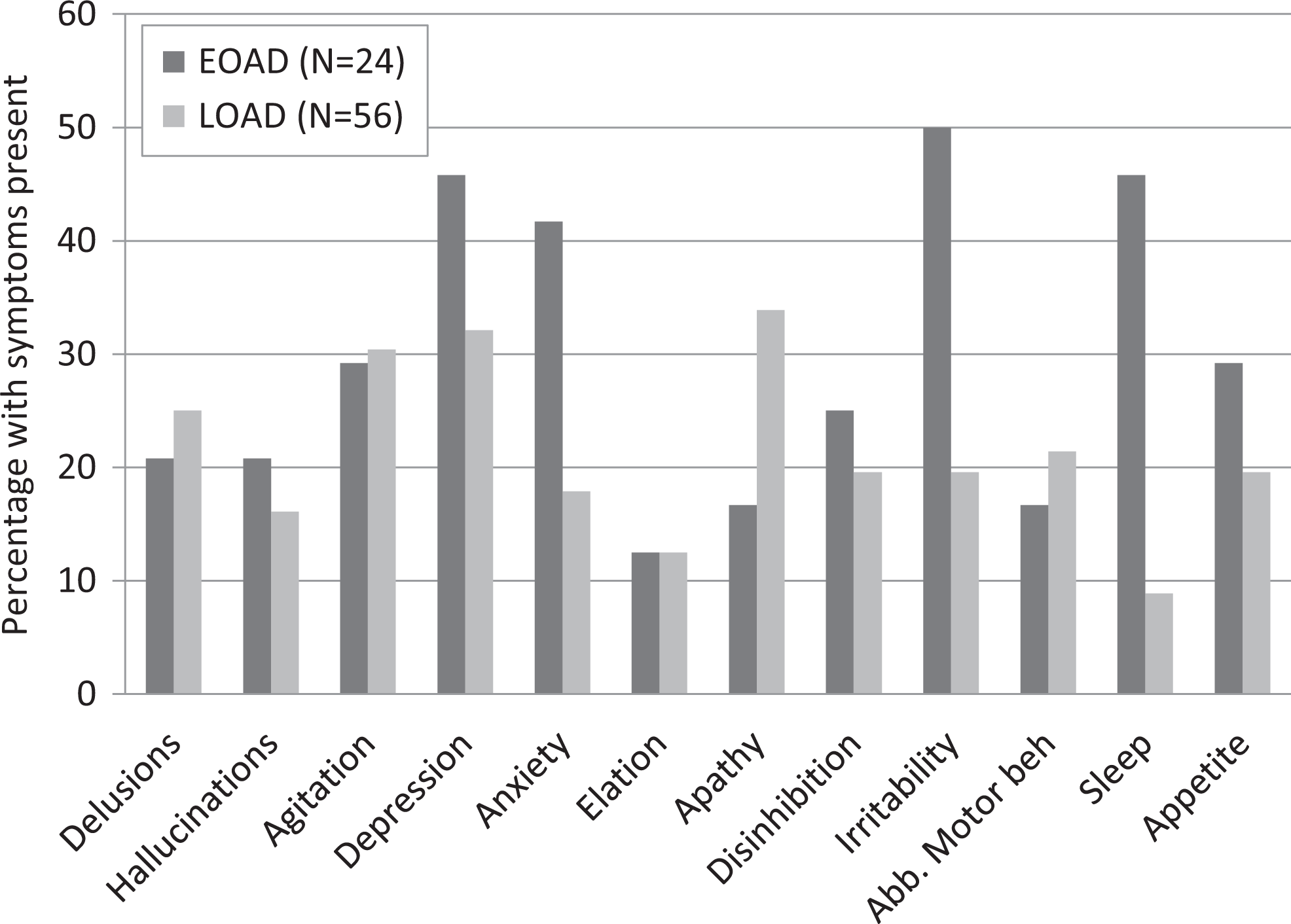
Percentage with 12 neuropsychiatry symptoms of Neuropsychiatry Inventory present for early-onset Alzheimer disease (EOAD) and late-onset Alzheimer disease (LOAD).
Linear regression analysis with NPI total as the dependent variable and MMSE, age, gender, education, duration of illness, family history, and ADL (Model 1) as independent variables showed longer duration of illness and higher ADL dependence as predictors for the whole cohort. In the LOAD group higher ADL dependence and in the EOAD group duration of illness predicted the total NPI score (Table 3).
Linear Regression Analysis With the Total NPI Scores as the Dependent Variable and Age, Gender, MMSE Scores, Duration of Illness in Months, BADL Scores, Education in Years, and Family History of Dementia Entered as Predictive Variables for the (a) Whole Alzheimer Disease Sample, (b) LOAD, and (c) EOAD Group.a
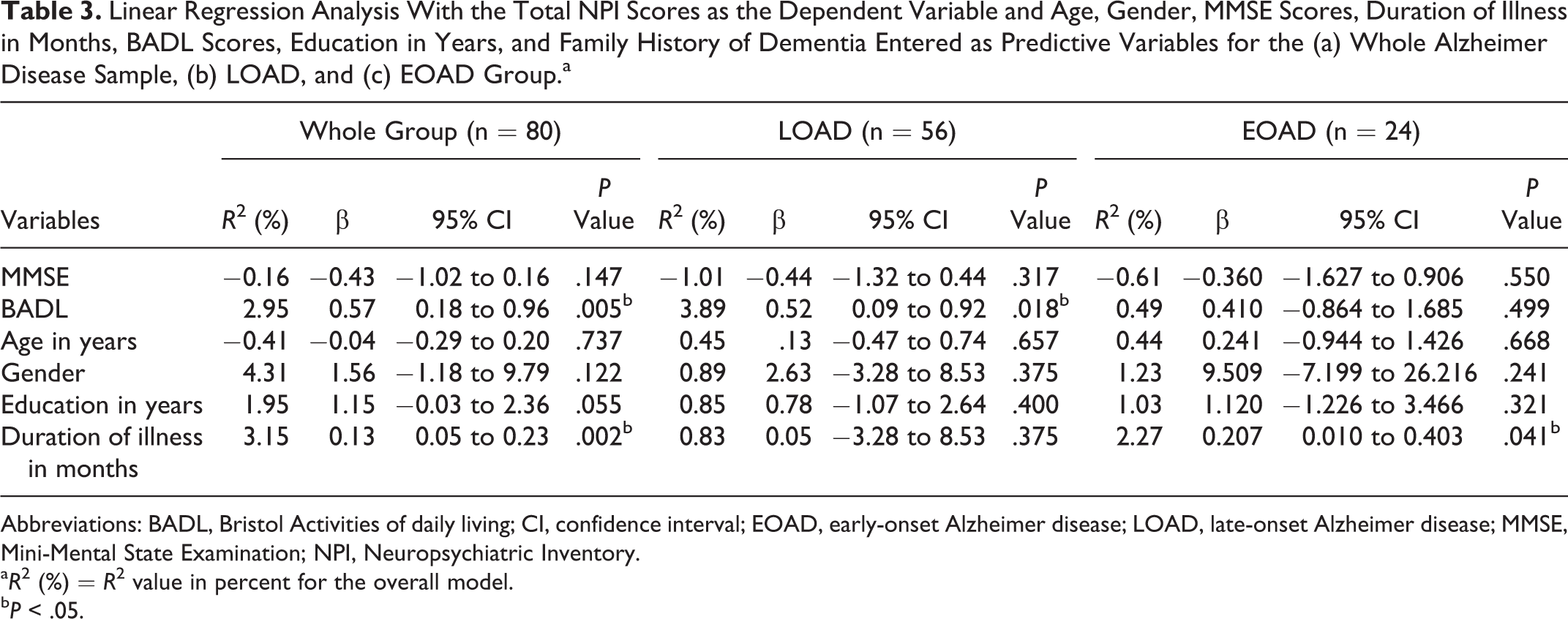
Abbreviations: BADL, Bristol Activities of daily living; CI, confidence interval; EOAD, early-onset Alzheimer disease; LOAD, late-onset Alzheimer disease; MMSE, Mini-Mental State Examination; NPI, Neuropsychiatric Inventory.
aR2 (%) = R2 value in percent for the overall model.
bP < .05.
Discussion
The study aimed to compare patients with EOAD and LOAD in terms of prevalence and severity of NPS as measured by the NPI. We found that the overall total NPS severity score was similar for the EOAD group compared to LOAD. The prevalence of 12 NPS as reported on the NPI was higher except for apathy in the EOAD group compared to the LOAD group and significantly higher for the anxiety, irritability, and sleep subscales. The EOAD group was comparable to the LOAD group except that they had longer illness duration. Our study demonstrated that longer duration of illness and greater ADL dependence affected the total NPS for the whole cohort. For people with LOAD, higher ADL dependence predicted NPI total score and for EOAD, longer duration of illness predicted NPI total.
Neuropsychiatric symptoms are common in AD although the prevalence and frequency vary across studies. Our findings are in keeping with previous studies that found higher NPS prevalence in EOAD. 22 –25 The prevalence of anxiety and depression has been reported to be greater in EOAD samples in various studies. 22,23,25 This is thought to be due to both the diagnosis and the subsequent changes in lifestyle, roles, and responsibility, 34 which are greater in EOAD than in LOAD. Another study reported that pattern of apathy, agitation, disinhibition, irritability and aberrant motor behaviour worsening with severity progression of dementia in patients with EOAD is similar to the patterns in late- onset AD, however hallucinations (occurring in milder stages due to brain damage), depression and anxiety (occurring throughout the course both due to brain damage and psychosocial factors) showed different patterns in EOAD. 35
Conversely, patients with LOAD have been reported with a higher NPI total score than the EOAD group, with higher scores on the delusion, hallucination, agitation, disinhibition, and aberrant motor behavior subscales and with similar duration of illness and measures of disease severity. 16 A 2-year longitudinal study of NPS in EOAD and LOAD found that the incidence and prevalence of NPS were lower in EOAD than in LOAD—in particular delusions, agitation, depression, apathy, anxiety, aberrant motor behavior, and irritability. 19 Another study 36 compared EOAD and LOAD groups with similar severity and found patients with LOAD had higher total NPI score and Delusion, Agitation, and Nighttime Behavioral Disturbance Subscale Scores. However, the EOAD group was less impaired in ADL and instrumental ADL. The authors suggested that patients with EOAD have greater cognitive reserve, associated with higher levels of education, which enabled them to compensate for cognitive deterioration, maintain levels of functioning, and reduce the impact of behavioral symptoms. A recent study found that the LOAD group scored higher on total NPI score but had lower MMSE scores than the EOAD group. 21 Other studies have found patients with EOAD and LOAD similar in total frequency and severity of NPS, although there seemed to be different symptom profiles in the 2 groups. 37
In keeping with previous studies, our patients with EOAD were treated with cholinesterase inhibitors to a higher extent than those with LOAD, 38 while there were no differences between the groups in antidepressant and antipsychotics use.
In our study, the EOAD group had longer duration of illness which may have contributed to the higher NPS prevalence, although they were similar in their NPS severity to LOAD. Patients with EOAD had functional dependence (ADL scores) similar to LOAD who had shorter duration of illness, indicating better reserve and compensatory mechanisms in patients with EOAD. Our cohort of EOAD had longer duration of illness compared to LOAD possibly due to the longer time taken to diagnosis which is known to occur in early-onset dementia. 39 Diagnosing young-onset dementia is challenging, and the range of possible presenting features is broad, encompassing behavioral, cognitive, psychiatric, and neurological domains, and symptoms are often subtle initially. 40 Since approximately one-third patients of younger age present with an atypical nonmemory phenotype 41 translating to delayed diagnosis and NPS are confounding factors, it is important that clinicians give importance to specific symptoms.
The carer distress was higher for EOAD and significantly so for irritability and sleep symptoms on NPI. Most of the studies that have reported carer distress associated with NPS have been for LOAD. A recent meta-analysis found irritability as one of the symptoms that most strongly correlated with distress. 27 Irritability was also reported to be significantly associated with caregiver burden. 42,43 To our knowledge, our study is the first one to compare the carer distress between the EOAD and the LOAD for individual symptoms. The early recognition and management of specific NPS by family members and health professionals may lead to better care and quality of life for both patients and caregivers. It is important to look further into caregiver factors and examine the causal mechanisms by which NPS impact caregiver well-being and burden so that interventions can be designed to target NPS more effectively and also support caregivers.
The strength of the study is that standardized measures were used for diagnosis and to evaluate NPS. We also excluded patients aged between 65 and 70 years, giving a “buffer” of 5 years between younger- and older-onset participants and excluded people with history of psychiatric disorder. The exclusion of participants with LOAD aged between 65 and 70 may potentially have been a source of bias, but it was felt that the benefit in terms of separating the 2 groups was greater. The small sample is the main limitation of the study, but nonetheless, the findings have implications for diagnosis and management of NPS in patients with AD. Although the 2 groups were comparable for MMSE, additional cognitive measures for severity assessment would have been useful. However, ADL were assessed, and both the groups were comparable for level of functional abilities. Analyses were carried out without controlling for multiple comparisons, and so results should be considered as preliminary until confirmed in a larger study.
In conclusion, the NPS severity was similar between EOAD and LOAD groups with similar dementia severity, although patients with EOAD had higher symptom prevalence and carer distress. Detection of NPS is important, as they impact negatively upon the ADL, cognitive functioning, and quality of life for patients and have been shown to increase caregiver stress and impact upon the likelihood of admission to institutional care. Understanding the pattern of NPS in AD is important when planning treatment, services, and care. Future research using larger samples and longitudinal study is needed in order to characterize the different reasons for NPS in EOAD and LOAD and mechanisms for alleviating it.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Alzheimer’s Research UK East Midlands Network Funding (Reference RM62G0546 and RM62G0700).