
Abstract
Few neuropsychological tests are available to assess executive dysfunction in low-educated and multicultural populations. To address this issue, the TFA-93, a switching verbal fluency test to assess cognitive flexibility, was administered to 70 healthy controls, 57 patients with a clinical diagnosis of Alzheimer’s disease, and 21 with a clinical diagnosis of a neurodegenerative disease associated with frontal disorders. Most of the participants were low-educated and nonnative French speakers. The TFA-93 comprises 2 categorical fluency tasks (animals and fruits) and a fluency task in which participants have to switch between animals and fruits. Correct responses and errors were collected, and a flexibility index expressed the switching cost. Results showed that correct responses were lower, and the switching cost was greater in both patient groups. In low-educated and multicultural populations, the TFA-93 seems to be a good alternative to assess flexibility compared to the standard neuropsychological tools based on academic abilities.
Keywords
Introduction
Despite the fact that neuropsychological examination contributes to detecting dementia, in some cases of low-educated or multilingual patients, the usual tools are not reliable, and as a result, this assessment is a real challenge. Most standard neuropsychological tools require reading or writing capacities and educational knowledge. When patients are illiterate or have a low level of education, suitable tools are lacking. 1 -3 Yet, such cases cannot be considered as rare in clinical routine, as the proportion of people with no schooling and/or a low level of literacy still remains quite high. Data from 146 countries indicate that 14.8% of individuals worldwide do not receive any formal schooling, and this number increases to 40% when including individuals who only attended primary school. 4 Moreover, in a context where societies are becoming increasingly multicultural, it should be kept in mind that cultural background also influences cognitive performance, 5,6 and that among the patients referred to a memory clinic, some of them are older immigrants who have moved from their country of birth. Again, few cognitive tests are available in a context of cross-cultural assessment, and difficulties with language barriers and cultural differences lead to over- (false positives) or underdiagnosis of dementia. 7,8 Thus, it is crucial to develop specific tools for these populations.
Most of the previous studies have proposed standards of existing global scales or slightly modified existing global scales for low-educated people in their country (eg, the Mini-Mental State Examination [MMSE] 9 -11 ; the Montreal Cognitive Assessment 12 ). Few studies have specifically created and validated global scales for low-educated populations. 13,14 The same situation holds for tests investigating one specific cognitive function, such as episodic memory. 15,16 To fill this gap, we previously created, normalized, and validated 2 memory tests for dementia detection and Alzheimer’s detection in illiterate and low-educated patients, respectively, (1) the Nine Images Test of the district of Seine-Saint-Denis—TNI-93 17 and (ii) the Memory Associative Test—TMA-93. 18 The question of neuropsychological tools specifically assessing other cognitive domains such as executive functions has been poorly investigated, despite the fact that the assessment of executive functions is essential in the field of dementia. These high-level functions governing goal-directed action are highly vulnerable in neurodegenerative diseases, 19 -23 and their impairment impacts patients’ daily life. 24,25 Based on a large cohort of patients, Godefroy and colleagues reported that the dysexecutive syndrome is a significant predictor of loss of autonomy. 19 Executive impairments have been described in several neurodegenerative diseases involving the frontal lobes and/or the striatofrontal circuits, such as frontotemporal dementia, 26 -28 Parkinson’s disease, 29,30 Lewy body dementia, 31 progressive supranuclear palsy, 32 corticobasal degeneration, 33,34 or vascular dementia. 35,36 Furthermore, although memory deficit is considered as the main cognitive symptom in Alzheimer’s disease (AD), it is now well established that executive disorders are also frequently associated. 37 -41 Godefroy et al reported that more than 87% of patients with AD showed a dysexecutive syndrome with prominent impairments of planning, inhibition, flexibility, and generation executive processes. 42 These executive impairments may even be observed in prodromal AD 43 and may have a prognostic value in the nondemented elderly individuals by predicting cognitive decline and conversion to AD. 44,45
Among executive functions, the assessment of cognitive flexibility may be particularly relevant 43 -45,46 even in low-educated people or for cross-cultural dementia screening. 14,47 One of the most common neuropsychological tests used to assess cognitive flexibility is the Trail Making Test (TMT 48 ). However, its validity is questionable in the assessment of low-educated people and/or in a multicultural population. First of all, the TMT requires a perfect knowledge of the letters of the alphabet, thereby excluding people with a low level of literacy (or with a low level of literacy in the language of the host country). Second, Fernandez and Marcopoulos 49 showed a wide variability in TMT norms across several Western culture countries, even for reaction times on part A. This suggests an impact of culture or at least that norms are not interchangeable across different cultural groups. As suggested by Diamond, 50 cognitive flexibility can also be assessed by verbal fluency tasks. Verbal fluency tasks might be a good alternative for low-educated people, since reading skills are not required, and these tasks are less sensitive to educational level, school experience, or cultural background. 51 This might be particularly the case when using ecological fluency such as a supermarket fluency task or an animal fluency task. 52 However, in the above cited studies, participants were assessed in their mother tongue. In France, a substantial proportion of low-educated people are nonnative French speakers. Despite the fact that their level of French is variable, the neuropsychological examination is conducted in French, probably decreasing de facto their abilities to produce a large number of words regardless of the semantic category considered. Furthermore, the use of a timed verbal generation test with nonnative French speakers is likely to underestimate their true ability due to a possible lower overall speed and ease in generating words in a nonnative language. 53,54
In order to increase the cognitive flexibility demands in these fluency tasks, Diamond 50 proposed to add a switching condition between different categories (eg, objects and food), requiring greater recruitment of flexibility rather than semantic knowledge. Using a switching verbal fluency test, previous studies showed that this test (1) is more highly associated with executive functions than classical semantic verbal fluency tasks 55 and (2) is valid in groups of patients with executive disorders. 56,57 This switching condition could also enable cognitive flexibility to be more appropriately assessed in nonnative speakers by controlling the potentially low number of words generated within the time frame during classical semantic verbal fluency tasks. We therefore sought to examine whether a switching verbal fluency test might assess cognitive flexibility in a sample of neurodegenerative patients, most of whom had a low level of education and came from a multicultural background. Based on previous results, it was hypothesized that the switching cost observed by comparing classical fluency tasks and the switching condition would be higher in patients than in healthy controls (HCs).
Methods
Population
A total of 148 participants (HCs: n = 70; patients: n = 78), aged older than 50, were included. According to the Helsinki Declaration, 58 all participants gave their full informed consent.
Overall, the sample was composed of 37% native French speakers with different levels of education (51% without a formal degree or with the lowest secondary school degree, from 0 to 7 years of education; 49% with a higher degree from 8 to 19 years of education) and 63% of multicultural participants with an immigrant background, mainly low educated (82%: 0-7 years of education; 18%: 8-15 years of education), with variable levels of French language skills, especially in its written form.
Patients attending the Memory Clinic at the Neurology Department of Avicenne Hospital (Assistance Publique des Hôpitaux de Paris) with the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V) clinical criteria of major neurocognitive disorders 59 were included. The clinical diagnosis was characterized by a neurologist and a multidisciplinary discussion. We selected patients with a clinical diagnosis of AD 60 (n = 57) and patients who received a clinical diagnosis of a neurodegenerative disease known to be associated with frontal disorders (frontal group; n = 21). This group included frontotemporal dementia (n = 6), Lewy body dementia (n = 6), Parkinson dementia (n = 2), vascular dementia (n = 4), corticobasal degeneration (n = 2), and supranuclear palsy (n = 1). When the patient’s level of French permitted (91% of the patients), the French version of the MMSE 61 was administered. Demographic characteristics are summarized in Table 1.
Participant Characteristics.a
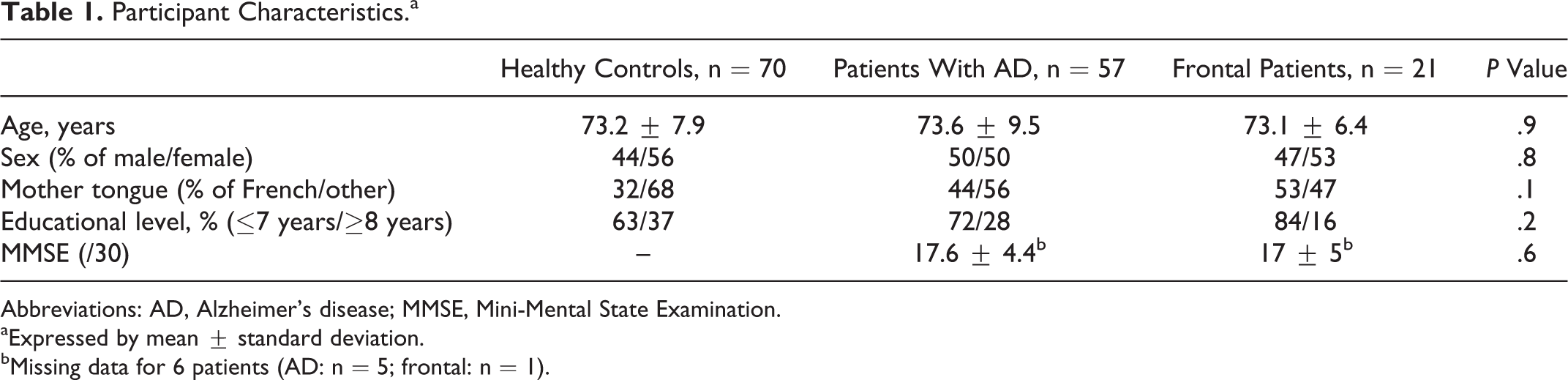
Abbreviations: AD, Alzheimer’s disease; MMSE, Mini-Mental State Examination.
aExpressed by mean ± standard deviation.
bMissing data for 6 patients (AD: n = 5; frontal: n = 1).
Healthy controls were included at the Centre d’Examen de Santé (Center of Health Exams) in Bobigny (Seine-Saint-Denis district, France). They were recruited on a voluntary basis during a free health checkup proposed by the French National Health Service. During the checkup, they were examined by a neurologist who, based on DSM-V criteria, excluded a diagnosis of major neurocognitive disorder or psychiatric illness. When memory disorders were suspected, the participant was systematically excluded and addressed to the Memory Clinic for further investigations. A total of 235 healthy participants were recruited, but to match with the demographic characteristics of the patient groups, a subsample of 70 was selected for the present study.
The 3 groups did not differ in terms of age, F(2,143) < 1; P = .9), sex distribution χ2 (2;N=146) = .5; P = .8, proportion of French native speakers, χ2 (2;N=146) = 3.9; P = .15, and proportion of low-educated people, χ2 (2;N=146) = 3.5; P = .17. Patients with AD and frontal patients did not differ in global cognitive performance assessed with MMSE scores, F(1,65) < 1; P = .6).
Material and Procedure
Executive functioning was assessed using the switching verbal fluency test of the district of Seine-Saint-Denis (TFA-93). The TFA-93 was based on a switching verbal fluency test previously proposed in the Delis-Kaplan Executive Function System (D-KEFS 62 ).
First, 2 classical categorical fluency tasks were proposed. Participants were asked to orally produce as many names of animals as they could during 1 minute and then to orally produce as many names of fruits as they could during 1 minute. As previous studies found that performance on phonemic fluency tasks is more impacted by educational level than performance on semantic ones, 63,64 and considering our low-educated and/or multicultural population, semantic fluency tasks were preferred to phonemic ones. In common with the D-KEFS battery, we included the fruit category, but we chose to replace the furniture category proposed in this battery by animals, consistently with the version previously proposed by de Paula et al, 55 in view of the higher lexical frequency of items in the animal category. The whole test was administered in French, and participants were asked to accomplish the 3 fluency tasks in French, even when they were not native French speakers. Pretested instructions were short and easily understandable, including for participants with a low level of French: “Could you say as many names of animals (/fruits) as possible in 1 minute. Any questions? You can start.” The timer was started immediately after instructions. No example or strategy was given to the participants. When participants produced no words or produced errors during the first 15 seconds, the instructions were repeated (without stopping the timer). The number of correct responses, repetitions, and intrusions was recorded for each semantic fluency task. Considering that restrictions concerning the production of variants or derived words were not imposed (no restrictions were given by the way), all the names of animals/fruits produced were counted as correct responses.
After having administered the 2 semantic fluency tasks, the switching task was proposed to increase the demands on cognitive flexibility. In this task, participants were asked “to say as many words as possible in 1 minute, but this time you have to say one animal then one fruit, then one animal, then one fruit, and so on. You can start.” The timer was started immediately after the instructions. When participants produced no words or produced errors (repetitions; intrusions; perseverations) during the first 15 seconds, the instructions were repeated (without stopping the timer). One point was given for the first correct response (animal or fruit), then for the following word if (1) the switching instruction was respected and (2) the word had not already been given during the switching condition (however, participants could use the names of animals or fruits produced earlier during the semantic fluency tasks). Consistent with the procedure used by de Paula and colleagues, 55 the switching task used the same categories as those proposed during the first 2 conditions. This point was crucial in the present study, as the task was highly demanding for nonnative French speakers. It was therefore important to take into account their performance on the 2 semantic fluency tasks to interpret their performance in the switching condition. In order to investigate more specifically their cognitive flexibility, an index was calculated by dividing the number of correct responses given in the switching condition by the sum of correct responses given in the 2 semantic fluency tasks. To facilitate its interpretation, the result was finally multiplied by 200. The higher the index, the lower the switching cost, and an index below 100 means that the number of correct responses given in the switching condition is lower than the sum of correct responses produced for animals and fruits (ie, showing a switching cost).
Statistical Analyses
We first conducted analyses of variance (ANOVAs) with group (HC, patients with AD, and frontal patients) as between-group factor and fluency condition (animals, fruits, and switching) as a within-group factor separately on each score (correct responses, repetitions, and intrusions) to investigate the effect of pathology on classical lexical evocation tasks and to test the presence of an interaction suggesting that the switching task particularly decreases performance in patient groups and especially in the frontal group. To check whether flexibility is impaired in patient groups, we then compared patients’ performances to those obtained by HC on the flexibility index and perseverations using univariate ANOVAs with group (HCs, patients with AD, and frontal patients) as between-group factor. Finally, Pearson correlation analyses were conducted between the flexibility index and the other cognitive scores (MMSE; TNI-93).
Performances are expressed by mean ± standard error of the mean. Analyses were performed using SPSS version 18.0 (SPSS Inc, Chicago, Illinois), and the threshold for statistical significance was set at P < .05. Power analyses were performed for main between-group comparisons.
Results
Effect of Pathology on TFA-93 Performances
A first ANOVA with group (HC, patients with AD, frontal patients) as between-group factor and fluency condition (animals, fruits, switching) as within-group factor was performed on correct responses. The main effect of group, F(2,143) = 63.3; P < .001; η2 = .47, was due to the higher performance in HC (11.9 ± 0.3) than in patients with AD (6.9 ± 0.4; P < .001) and frontal patients (5.8 ± 0.6; P < .001), whereas the 2 patient groups did not significantly differ (P = .1). The main effect of condition was also significant, F(2,286) = 52.1, P < .001; η2 = 0.27, due to higher correct responses in the animals fluency task (9.9 ± 0.4) than in the fruits category (7.8 ± 0.3; P < .001) and the lowest performances obtained in the switching condition (6.8 ± 0.3; both P < .001). The group × condition interaction was significant, F(4,286) = 2.9; P = .02; η2 = .04 (Figure 1). Univariate ANOVAs were conducted to investigate the condition effect in each group separately. In HC, F(2,144) = 36.8, P < .001, η2 = .34, it appeared that they performed better in the animals fluency task than in the fruits (P < .001) and switching conditions (P < .001), whereas the latter 2 did not differ (P = .8). In frontal patients, F(2,36) = 15.9, P < .001, η2 = .47, as in patients with AD, F(2,106) = 37.8; P < .001; η2 = 0.42, all paired comparisons were significant, meaning that performance during the switching task was lower than the 2 simple fluency conditions (all P < .02), suggesting a switching cost in patient groups that was not observed in HCs.
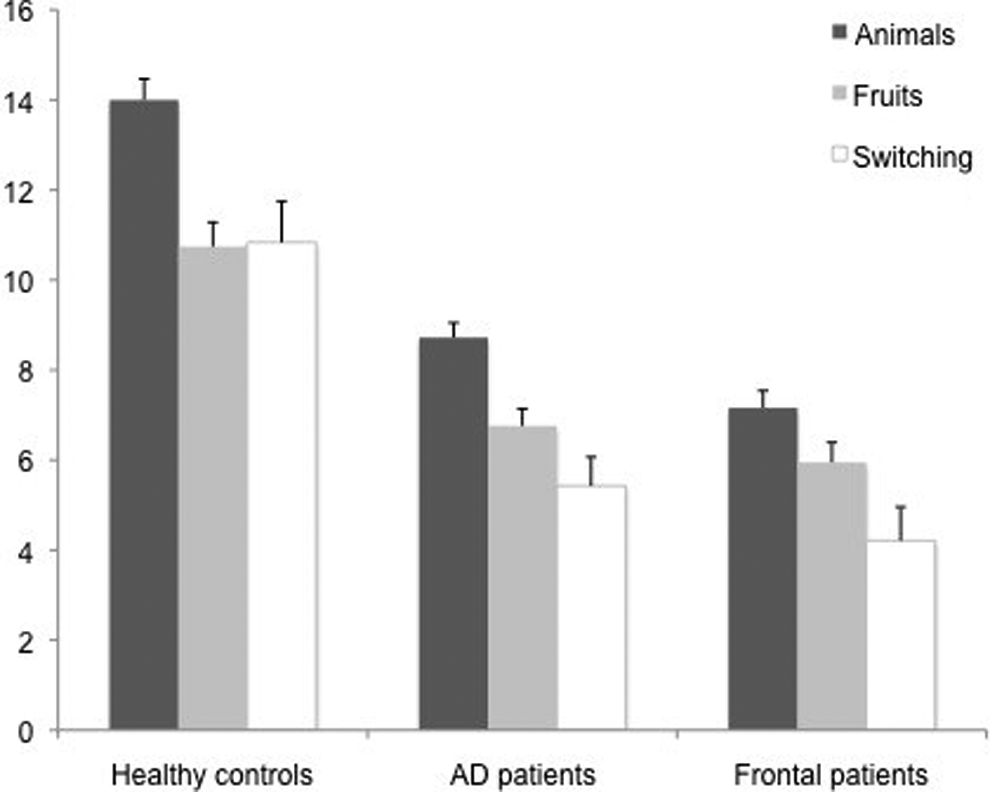
Number of correct responses given according to the task condition in each group. Bars represent the standard error of the mean.
A second ANOVA with group (HC, patients with AD, frontal patients) as between-group factor and fluency condition (animals, fruits, switching) as within-group factor was performed on repetitions produced during the task. The main effect of group was significant, although weaker, F(2,143) = 3.6, P = .03, η2 = 0.05, due to more repetitions given by patients with AD (0.7 ± 0.1) than by frontal patients (0.3 ± 0.1; P = .01) and a trend to produce more repetitions in patients with AD than in HC (0.5 ± 0.07; P = .09). The effect of condition and the group × condition interaction were not significant, respectively, F(2,286) = 2.2, P > .1, η2 = .01; F(4,286) = 2, P = .1, η2 = 0.03.
Another ANOVA with group (HC, patients with AD, frontal patients) as between-group factor and fluency condition (animals, fruits, switching) as within-group factor was performed on intrusions produced during the task. The effect of group was not significant, F(2,143) < 1, P > .5, η2 = 0.008, suggesting that the number of intrusions did not significantly differ between groups (HC: 0.2 ± 0.05; AD: 0.2 ± 0.06; frontal: 0.3 ± 0.1). The main effect of condition, F(2, 286) = 6.6, P < .01, η2 = 0.04, was due to more intrusions during the fruits (0.4 ± 0.1) and switching conditions (0.3 ± 0.07) than during the animals condition (0.03 ± 0.02; both P < .001), while fruits and switching conditions did not differ (P = .4). The group × condition interaction was not significant, F(4,286) < 1, P > .6, η2 = 0.009, suggesting that the same pattern was observed regardless of the group considered.
This unexpected result could be explained by the fact that illiterates have different categorization strategies than literates. 5 Semantic categorization is acquired throughout schooling. However, for illiterates or our multicultural population, it is possible that in their functional categorization based on daily life, fruits and vegetables belong to the same category, since they can be bought from the same place. To test this hypothesis, we checked the nature of intrusions produced by all participants and applied a new scoring by accepting vegetables as correct responses (during the fruits condition). We also consistently revised the number of intrusions produced when the remaining intrusions were terms unrelated to the categories of fruits and vegetables. The new ANOVA with group (HC, patients with AD, frontal patients) as between-group factor and fluency condition (animals, fruits, switching) as within-group factor conducted on the remaining intrusions (when considering vegetables as correct responses) showed that the condition effect previously found disappeared, F(2,286) = 2.2; P = .1, η2 = 0.01 (the group effect and the group × condition interaction were still not significant, respectively: F(1,143) < 1, P > .5, η2 = 0.008; F(4,286) < 1, P = .7, η2 = 0.008). We also checked whether this new scoring changed effects previously observed on the first ANOVA conducted on correct responses with group (HC, patients with AD, frontal patients) as between-group factor and fluency condition (animals, fruits, switching) as within-group factor. All the effects previously described remained significant.
Effect of Pathology on the Flexibility Index
A univariate ANOVA conducted with group (HC, patients with AD, frontal patients) as between-group factor performances on the flexibility index showed a main effect of group, F(2,143) = 11.4; P < .001; η2 = 0.14, due to a higher flexibility index in HC than in patients with AD (P = .001; Table 2) and frontal patients (P = .001), whereas the 2 patient groups did not differ (P = .29). The same analysis was conducted on the number of perseverations produced during the switching task. The main effect of group was significant, F(2,143) = 3; P = .05; η2 = 0.04, suggesting that the frontal group produced significantly more perseverations than HC did (P = .04), and there was a trend of more perseverations produced by patients with AD in comparison to HCs (P = .07; see Table 2). The 2 patient groups did not differ (P > .4).
TFA-93 Performances on the Switching Task in Healthy Controls Versus Patients With Alzheimer’s Disease and Frontal Patients.a

aExpressed by mean ± standard error of the mean.
We checked whether the results changed using the flexibility index calculated based on the second scoring (considering vegetables as correct answers). All the effects previously described remain significant. We also computed a post hoc power analysis to analyze the power of our study to document group differences on the flexibility index and the number of perseverations. With an α = 0.05, our proposed sample size was large enough to detect significant differences between HC and patients with AD (power > 0.9 for the flexibility index and power = 0.77 for the number of perseverations). However, the power to detect significant differences between patients with AD and frontal patients was lower (flexibility index: power = 0.55; perseverations: power = 0.32).
Correlation Analyses
To verify the added value of the TFA-93 during a neuropsychological evaluation with low-educated and multicultural patients, we studied correlations between performances on the TFA-93 switching task and performances on the widely used MMSE or performances on the TNI-93 (that was specifically normalized and validated to assess episodic memory in this kind of population). The flexibility index was positively correlated with the MMSE total score (r = .57; P < .001), suggesting that the higher the global cognitive functioning is, the lower the cost of the switching task in comparison with the categorical fluency tasks. However, no correlation was found between the flexibility index and recall performances on the TNI-93 (TNI-93 free recall: r = .1; P > .2; TNI-93 total recall: r = .09; P > .4). A similar pattern of results was obtained with the number of perseverations produced during the TFA-93 switching task that was correlated with the MMSE score (r = −.38; P < .001), whereas no correlation was found with the TNI-93 scores (free recall: r = .06; P = .6; total recall: r = −.05; P > .7). The higher the global cognitive functioning, the lower the number of perseverations produced during the switching task.
Discussion
The present study aimed to examine whether the switching verbal fluency test of the district of Seine-Saint-Denis (TFA-93) might assess cognitive flexibility in a low-educated and multicultural population. Based on previous results, it was hypothesized that the switching cost observed by comparing traditional fluency tasks and the switching condition would be higher in both patient groups than in HCs.
When looking at the number of correct responses, results showed that patients’ performances were lower than HCs’ performances regardless of the condition considered and without distinction between patients with AD and frontal patients. This means, first of all, that the ability to generate information in semantic fluency tasks is impaired in both patient groups. This result is consistent with previous studies showing (1) that verbal fluency is impaired in AD 65,66 due to reduced executive abilities involving search and retrieval processes and reduced availability of semantically related words 67 but also (2) that words generated in verbal fluency did not differ between patients with AD and those with frontal lobe dementia. 68 Second, when comparing the number of correct responses across conditions, it appears that—by contrast with HC—the performance of patient groups in the switching condition was lower than in the 2 simple fluency conditions. This result suggests a switching cost in patient groups that was not observed in HC. This point is confirmed by analyses conducted on the flexibility index and perseverations produced during the switching condition, where we found that the flexibility index was lower in both patient groups, supporting the hypothesis of a greater switching cost in patients in comparison with HC. Consistently, the frontal group produced more perseverations than HC did. Although patients with AD showed a tendency to produce more perseverations than the HC group, again there was no difference between the patient groups. It has to be emphasized that these results cannot be explained by a low level of education or a multicultural background, since the 3 groups did not significantly differ on these characteristics. These findings confirm the impairment of cognitive flexibility in patients with AD and in frontal group patients that was well described in previous studies using standard neuropsychological tools such as the TMT or the Wisconsin Card Sorting Test 19,20,42,69 and extend them to a low-educated and multicultural population. From a clinical point of view, these results indicate that the TFA-93 can be useful to assess cognitive flexibility when investigating potential cognitive decline in low-educated patients but also in nonnative French speakers. In this case, the flexibility index and the number of perseverations seem to be interesting clinical indicators. The former is crucial considering our specific sample. The use of classical semantic verbal fluency tasks would have been likely to underestimate participants’ true ability, since these tasks are highly demanding for nonnative French speakers (ie, it is more difficult for them to generate words in a non-native language, and their lexical stock in French is probably poorer). It is therefore important to use the flexibility index rather than the number of words generated during the switching task condition, since this index takes into account participants’ performance on the 2 semantic fluency tasks to interpret their performance in the switching condition (ie, as a ratio).
It is also interesting to underline that, considering correct responses on the TFA-93, patients with AD and frontal patients did not differ, suggesting that this test might not be useful to distinguish the 2 patient groups. Is it the same when looking at the errors produced? Three different kinds of errors can be made during the TFA-93: (1) repetitions (eg, when a participant names the same fruit twice during the verbal fluency task in the fruits category); (2) intrusions (or rule violation errors; when a participant gives a word that does not belong to the category); and (3) perseverations (when a participant does not alternate during the switching condition; eg, successively naming two animals). Our results showed that patients with AD and frontal patients did not differ in either intrusions or perseverations. However, patients with AD produced more repetitions than frontal patients did. Yet, these 3 kinds of error might differ in their underlying mechanisms. While rule violation errors and perseverations may be explained by a deficit in executive functioning (respectively, an inappropriate maintenance of a category and a deficit of cognitive flexibility 70 ) related to degeneration of the frontal lobes, repetitions could arise from language and memory deficits in relation to left temporal lobe atrophy. 71 -73 Following this hypothesis, our results suggest that the severity of executive disorders is quite similar between our patients with AD and frontal patients, whereas memory disorders are greater in the AD group. An alternative hypothesis is that patients with AD and frontal patients did not differ because of a lack of statistical power, as suggested by the power analysis we conducted. It is noteworthy that, despite a lack of power, the number of repetitions was helpful to distinguish patients with AD from frontal patients, arguing in favor of a rather similar severity of executive disorders in both patient groups rather than a lack of power. Nevertheless, future studies on the TFA-93 are needed to disentangle these 2 hypotheses and to further explore its potential interest to help distinguish patients with AD from other neurodegenerative diseases. 74
Also arguing in favor of an added value of the TFA-93 in the neuropsychological evaluation of low-educated and multicultural patients, we found no correlation between the cognitive flexibility indices (flexibility index and perseverations in the switching condition) and the TNI-93—an episodic memory test specifically developed and normalized in the same kind of population. 17 By contrast, both cognitive flexibility indices correlated with the MMSE total score. This may be surprising since the MMSE does not assess executive functions. 75 However, the MMSE score decreases with dementia severity. Thus, with increasing dementia severity, the probability of observing executive disorders (eg, cognitive flexibility deficits) or their severity increases.
With the first analysis on intrusions, an unexpected result was observed: Participants produced more intrusions in the fruits condition, without any differences between the 3 groups. On checking the nature of these intrusions, it appeared that this effect was driven by the propensity of participants to name vegetables in addition to fruits. It suggests that, in our mainly low-educated and multicultural population, the semantic organization might be different. Luria already reported several decades ago that illiterates—from Central Asia—did not make classifications based on semantic categories but rather on associative or functional properties. 5 Consistently, previous studies showed that illiterates performed more poorly than literates on classical semantic fluency tasks, for example, for the animal criterion, 1,76 -78 whereas no difference was found when using a more ecologically relevant criterion such as market foods. 52 Similar results were reported in an immigrant population by Nielsen and Waldemar. 79 It can be hypothesized that our participants responded to the fruits criterion in a concrete situational way (eg, things that can be bought at the greengrocer’s). This consideration will be particularly relevant when studying the educational and cultural effects on the TFA-93 in a normative data perspective.
To sum up, the TFA-93 seems to replicate the results of previous studies highlighting the cognitive flexibility impairment in neurodegenerative diseases. Furthermore, the test was easily understandable, even when participants had no schooling, a poor level of spoken French, and/or presented cognitive disorders. Added to the fact that this is a short test with no required reading and writing skills, these results indicate that the TFA-93 might be a good alternative to the traditional neuropsychological tools used to assess flexibility abilities (eg, TMT) when the patient has a low level of education and/or when he or she has to be assessed in another language than his or her mother tongue (eg, in an immigrant population). Our results also suggest that the TFA-93 might be an interesting complementary test in the neuropsychological examination of low-educated and multicultural people, since no correlation was found with the TNI-93, which assesses episodic memory. However, some limitations have to be mentioned. First, our sample of frontal patients is quite small and heterogeneous. It is possible, as argued by the power analysis, that this limitation contributes to explaining why frontal patients did not perform worse than patients with AD. Second, although the involvement of flexibility abilities in a switching verbal fluency task has been previously shown (eg, de Paula et al, 2015), the good construct validity of the TFA-93 was not checked in the present study. This was not done due to the lack of available normalized executive tests adapted for our specific population. Further studies are needed (1) to propose traditional executive tests to French native speakers in order to verify this psychometric property and (2) to increase the sample size, especially in the HCs, in order to study the effects of demographic variables and to propose normative data before using the TFA-93 in clinical practice. Finally, as our 3 groups were comparable in educational level and proportion of nonnative French speakers, we cannot claim that the TFA-93 can be considered as a culture-free test. 80 Again, this point will be crucial with a view to elaborating normative data for its clinical use according to—or regardless of—the patients’ cultural background.
Footnotes
Acknowledgments
The authors thank Philippe Laboulaye, Karema Soufi, Valérie Haziza, and Sarra Le from the CES of Bobigny who contributed to the data collection for healthy controls and also Magalie Cordel, Claire Messaoudi, and Marta Sanchez Ortiz who contributed to the data collection and data verification during their master’s theses in psychology. The authors also thank Elizabeth Rowley-Jolivet for English language editing of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.