
Abstract
We aim to investigate whether a popular hand exercise could be used to improve the action of eating in patients with Alzheimer’s disease (AD). A 6-month intervention was conducted in 60 patients with AD who live in a nursing home. They were divided into hand exercise and control groups. Patients of the control group maintained their daily routine. The improvement of Edinburgh Feeding Evaluation in Dementia scale in hand exercise group was significantly greater than in the control group (P = .003). Significant differences in time of autonomous eating and time of simulated eating between patients in the hand exercise and control groups (P < .05) were noted. The improvements in accuracy of eating action and coordination of eating action from baseline were significant in hand exercise group compared to the control group (P = .020 and .014, respectively). Hand exercise is a safe and effective intervention to improve the feeding and eating of people with AD.
Introduction
Because of the increasing global life expectancy, the world’s population is aging rapidly. Between 2015 and 2050, the proportion of adults aged 60 years and older is estimated to be between 12% and 22% worldwide. By 2050, there will be almost 120 million older people living in China. 1,2 Alzheimer’s disease (AD) is the most frequent cause of dementia in the older population. In China, the number of people with AD was estimated as 5.69 million in 2010. 3 During the aging process, due to metabolic changes and loss of appetite, the amount of food intake was largely decreased and resulted in malnutrition and weight loss in the older population. 4,5 This may be more important for patients with AD. Weight loss is observed in 40% of patients with AD. 6 In addition to changes in metabolic and appetite, the possible explanations include impaired cognitive function and behavioral and psychological symptoms. 7 Many intervention approaches were applied as attempts to improve the nutrition intake of patients with AD, including oral nutritional supplementation, diet modification, and eating assistance 8,9 ; however, methods with definite effectiveness are still lacking. We aim to investigate whether a popular exercise program in China, the hand exercise, could be used to improve the eating action in patients with AD as well as their nutrition status.
Background
Dementia is one of the most common neuropsychiatric disorders in the world’s older population. 10 The burden of dementia seems to be increasing faster than is generally assumed. The dementia burden may have been underestimated in China. For example, the number of people with dementia in China was 9.19 million (5.92-12.48), and the number of people with AD was 5.69 million (3.85-7.53) in 2010. 3 In order to develop the proper support system for older people, efficient techniques for care of older people with dementia is timely needed. Hand movement has been widely used to activate several brain areas, for example, the prefrontal cortex which is involved in cognition, particularly executive function. 11,12 Furthermore, diminishing the activity of this area leads to the activation of the hypothalamo–pituitary–adrenal axis, which may be the cause of the depression in AD. 13 Both cognition and mood condition are the possible effectors of difficulty with self-feeding in patients with AD. 14 –16 A hand exercise program may be worthy of being evaluated as an intervention for improving the feeding and eating of people with AD.
Methods
Patients with AD were recruited from residents of a nursing home in Fuzhou, China, from September 2016 to March 2017 for participation of the 6-month program of hand exercise. Inclusion criteria were (1) diagnosis of AD consistent with the International Statistical Classification of Diseases and Related Health Problems, Tenth Edition issued by the World Health Organization and (2) the Mini-Mental State Examination (MMSE) scores was estimated after the patients or their family agreed for eligibility. Patients with MMSE scores between 10 and 26, defined as mild to moderate, were included. The cutoff scores classified whether or not individuals with dementia are >17 for illiterate patients, >21 for patients with primary school education, and >24 for patients with higher degree of education 17 ; (3) ability of oral communication; (4) ability to take food by mouth; (5) 60 years and older; and (6) informed consent provided by the patient or family members. Exclusion criteria were (1) severe pathologies of the liver, kidneys, blood, or primary disease of the endocrine system; (2) other past or current diseases that may have affected swallowing function, such as tumors of the head or neck, tumors of the esophagus, or cranial injury; (3) depending on gastric tube or feeding tube for nutrition; and (4) unstable vital signs. Demographic and comorbidity information were collected from their medical records.
Ethical Approval
The internal review board of Fujian Medical University, School of Nursing approved the study protocol (IRB No.: K2014-027-01). All enrolled patients were provided informed consent to participate after fully understanding of the purpose and methods of this study. For patients who cannot fully understand, the study were estimated by the physicians, and the consents were provided by their family members who were also explained completely.
Study Design
Enrolled patients were randomly divided into hand exercise group and control group by envelope method. Two nurses with a master’s degree were trained by investigators using videos, practical exercises, and participating in lessons to fully understand the study protocol before starting. They have to pass the examinations to be sure they were qualified. The one-on-one intervention was conducted from 09:30 to 10:00, Half an hour in the morning, 3 times per week for 6 months. Patients of the control group maintained their daily routine. Their daily activities include basic living and daily recreational activities such as eating, chatting, walking, and sleeping. No specific recommendations to engage in cognitive or physical activities were made during the 6 months intervention. Intervention was implemented in nonroutine periods of time. The assessors were blinded to the assignment of the groups.
Hand Exercise Program
The hand exercise was modified based on Wang’s design 18 for patients with diabetes mellitus but removed the overly complicated parts due to muscle skeleton degeneration of most older people. The exercise included 10 steps: (1) rub: rub the palms for 30 seconds, rub the back of both hands by placing your one palm on the back of the other hand for 10 times, alternate the hands and repeat; (2) claw: raise arms in front of the body with palms facing down and retract arms with hands like a claw, repeat 30 times; (3) fist and extend: fist the hands and then extend the fingers as widely as possible for 15 times; (4) tap: palm to palm with 1-cm distance apart, use right thumb to tap on the left thumb, then right index finger to tap on left, right middle finger to tap on the left, continue on to the right little finger, and back from little finger to thumb, then alternate the hands and repeat; (5) split: raise arms in front of the body with palm facing down, open the arms to the sides with split thumb, then pull the arms back to the initial position, fingers together. Repeat the movement but split the thumb and index finger, and next repeat but split the fingers between index finger and ring finger, final split between ring finger and litter finger. Repeat for 3 times; (6) clasp, fingertip: squeeze both tips of thumbs by opposite thumbs and index finger and interlace the fingertips, squeeze. Repeat 3 times; (7) clasp: purlicue to purlicue and press, then clasp hands and squeeze. Repeat 3 times; (8) snap: raise arms from stomach to over your head as high as possible, and back to stomach, all the while keep on doing fingers snap. Repeat 10 times; (9) pull: pull each finger by opposite thumb and index finger, interlace the fingers with palms facing out in front of the body, stretch for 20 times; and (10) rub and swing to relax. One nurse guided one patient to complete the whole program, mainly the nurse demonstrated and patient followed independently, when the patient had difficulty completing some steps, the nurse could provide suitable adjustments carefully.
Assessment Measures
Amount of food intake
The Nutrition Society of Taiwan recommends that older people who engage in light work should receive a daily caloric intake of 2000 to 2200 kcal for men and 1800 to 1900 kcal for women; 2000 kcal of food was represented as 1 unit in this study. This study employed fractions of this unit to calculate patients’ food intake during their 3 daily meals, and intake was recorded as 0, 1/4, 1/2, 3/4, and 1. The caloric value of each meal was controlled by the dietitian of the nursing home according to the food exchange list. Data of 3 meals for 3 days were recorded for analysis.
Time of autonomous eating
Autonomous eating was defined as the patients could hold their cutleries and eat without any assistance from the nurses. The total length of time during 1 meal was recorded by the investigators when the patients picked up and put down their cutleries. Data of 3 meals for 3 days were recorded for analysis.
Time of consecutive self-feeding
The investigators recorded the total time during one meal when the patients begin to hold their cutleries and successfully feed themselves for 5 consecutive times. Data of 3 meals for 3 days were recorded for analysis.
Accuracy of eating action
The investigator estimated the accuracy by 4 rating scores: excellent, good, normal, and bad. Excellent: never fail to put food into the mouth during one meal. Good: fail to put food for 1 to 2 times during one meal; normal: fail to put food for 3 to 5 times during one meal; and bad: >5 times of failures during 1 meal. All assessments were performed by the same investigator. Data of 3 meals for 3 days were recorded for analysis.
Coordination of eating action
The investigator estimated the coordination by 4 rating scores: excellent, good, normal, and bad. Excellent: never drop or spill the food, or any tremors of the arm or fingers during one meal; good: 1 to 2 times of each one of above during one meal; normal: 3 to 5 times during one meal; and bad: >5 times during 1 meal. All assessments were performed by the same investigator. Data of 3 meals of 3 days were recorded for analysis.
Upper arm circumference
Two investigators measured independently, and the mean values were recorded and used for analysis.
Eating compliance
The Edinburgh Feeding Evaluation in Dementia (EdFED) scale has 11 items encompassing eating behavior, nursing intervention, and eating difficulties. 19 The simplified and validated Chinese version of EdFED was used in this study to evaluate the eating compliance before and after the completion of the 6-month hand exercise program. 20
Statistical Analysis
Continuous variables were represented as mean and standard deviation, and categorical data were represented by number (n) and percentage (%). For continuous variables, the changes before and after intervention within the groups were analyzed by paired sample t test, and the differences between the groups were sought by independent t test. For categorical data, the differences between the groups were evaluated using χ2 or Fisher’s exact test. All P values were 2 sided, and <.05 were considered statistically significant. Statistical analyses were performed using the statistical software package SPSS version 22 (IBM, Armonk, New York).
Results
There were 87 patients who were asked the will to participate this study. Of these, 76 patients or their family members provided the signed informed consents, and 14 patients were excluded due to the criteria. In each group, 1 patient was discontinued the intervention due to the leave from the nursing home (the hand exercise group) and the worse heath condition (the control group), respectively. The data from 60 patients with mild-to-moderate AD who fulfilled all inclusion/exclusion criteria and completed the intervention were analyzed. A total of 30 patients were allocated in the hand exercise group and another 30 patients in the control group. There were 9 males (30%) and 21 females (70%) with an average age of 82.7 (8.4) years in the hand exercise group, and 8 males (26.7%) and 22 females (73.3%) with an average age of 81.0 (8.1) years in the control group. The demographics and baseline characteristics of the patients in both the hand exercise group and control group are shown in Table 1. There were no significant differences in age, gender, MMSE, comorbidity, EdFED, time of autonomous eating, amount of food intake, upper arm circumference, time of consecutive self-feeding, accuracy of eating action, and coordination of eating action between the 2 groups (Ps > .05).
Demographics and Baseline Characteristics.a
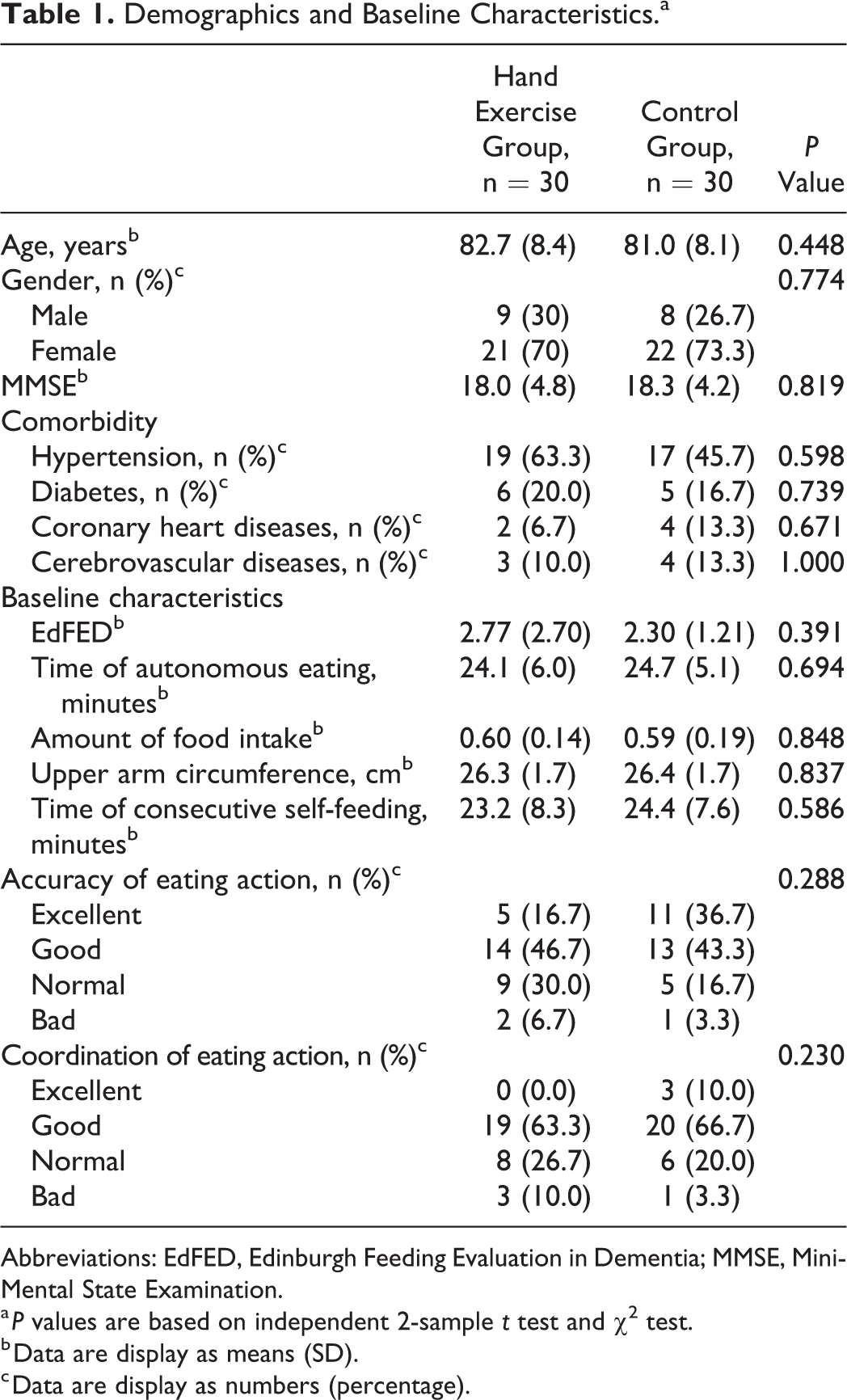
Abbreviations: EdFED, Edinburgh Feeding Evaluation in Dementia; MMSE, Mini-Mental State Examination.
a P values are based on independent 2-sample t test and χ2 test.
b Data are display as means (SD).
c Data are display as numbers (percentage).
Table 2 presents the change in outcomes from baseline after 6-month intervention in both the groups. A statically significant reduction of EdFED at 6 months after intervention in the hand exercise group (−0.63 [0.81], P < .001) was found; however, there was a slight decreased EdFED at 6 months after intervention in the control group and it did not meet the significant level (−0.10 [0.48], P = .264). In addition, the improvement of EdFED in hand exercise group was significantly greater than in the control group (P = .003).
Changes in Outcome Measurements From Baseline at Month 6 After Intervention.
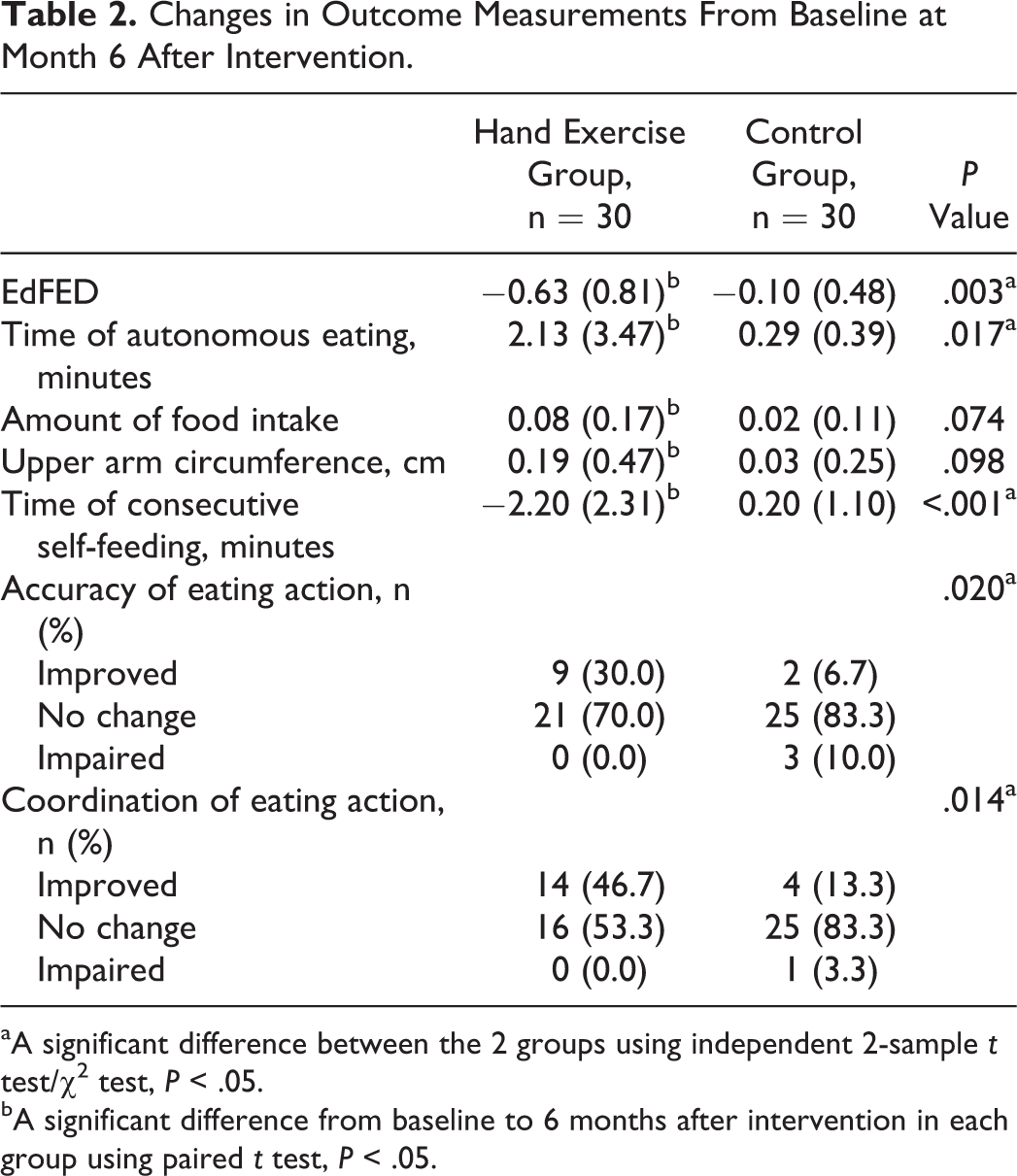
aA significant difference between the 2 groups using independent 2-sample t test/χ2 test, P < .05.
bA significant difference from baseline to 6 months after intervention in each group using paired t test, P < .05.
Statically significant increase in time of autonomous eating, amount of food intake, and upper arm circumference at 6 months after intervention in hand exercise group was found (P < .05). However, there was no significant change in terms of time of autonomous eating, amount of food intake, and upper arm circumference in the control group (P > .05). There were significant differences in time of autonomous eating and time of consecutive self-feeding between patients in the hand exercise and control groups (P < .05). The changes in amount of food intake and upper arm circumference from baseline were not significantly different between 2 groups after intervention (P = .074 and P = .098, respectively). Moreover, at 6 months after intervention, there were significant improvements of accuracy of eating action and coordination of eating action from baseline in hand exercise group compared with control group (P = .020 and P = .014, respectively; Table 2).
Discussion
Our results indicated that the hand exercise intervention improved the feeding and eating of people with AD, shown by the reduction in EdFED after 6 months of hand exercise. Compared to the control group, the time of autonomous eating increased significantly after intervention. In addition, the time of consecutive self-feeding decreased. Abovementioned changes reflected the improvement of the accuracy and coordination of eating actions, that is to say, the techniques of self-feeding were enhanced by the gentle physical exercise.
Physical and cognitive degeneration lead to increase feeding dependence and eating skills regress gradually in aging, and thus the disease progress of AD become even severe. 14 These could relate to that patients with AD have poor nutrition commonly and that malnutrition may also hasten the loss of cognitive function. 21 Intervention for decelerating the progress is of clinical importance to control the deterioration of eating capability due to aging and AD and reduce the burden of caregivers.
Positive effects of physical exercise intervention on cognition function in older people with dementia have been demonstrated in many studies. 22,23 But after taking the frailty and limited mobility of older people into consideration, a subgroup of patients with AD were not able to engage in the gentle physical exercise intervention for general population, such as walking and coordination exercise, which have been reported benefit on cognition function in older people. 24,25 Hand exercise may be safer and have better compliance. In addition, performing this intervention does not require large space, or special instrument, and therefore may be more convenient for the patients with AD to comply as a routine activity.
Hand exercise we introduced in this present study is well known in China. From children to older people, every age-group can learn and be familiar with it quickly, indicating that this is a simple intervention for improving the feeding and eating in patients with AD, with no restriction bounded by professional knowledge and skillset. Chen and the colleagues reported an effective intervention for patients with AD, including preparation of environment, preparation of food, preparation of utensils, appropriate assistance, patient monitoring, psychological care, and nursing care after eating. 26 All of them require intensive training, careful planning, and sufficient resource from professional caregivers with solid knowledge in nursing. This is a financial burden as well as a burden of caregivers. In fact, in China, family members (eg, spouses, children) remained to be the major caregivers for patients with AD 27 ; thus, some interventions which are designed for nursing home residents are not applicable. Our study was conducted in a nursing home, too, but we believe these results can be generalized to family caregivers under the supervision of professional nurse. A major difficulty is the compliance of patients. Some of our patients were low compliance at the initial stage of the intervention of the hand exercise. We tried to improve by increasing the familiarity between the patients and the nurses, including increasing the contact time, caring for the other needs of the patients, aiming to understand the habits and the meaning of their behaviors of the patients, and providing more appropriate care. We believed the efforts can develop the trust between the patients and the nurses. This experience encourages our belief that family caregivers may have good contributions which are comparable to professional nurses.
The limitation of our study is the small sample and short evaluation period, and the results may not apply to all patients in other geographical areas and cultural background. All participants were recruited from a single institution, which may caused site bias. Larger prospective multicenter studies with longer period of intervention are needed. In addition, the evaluation of the accuracy/coordination of eating action and eating compliance was developed by us. But a new study shows that the EdFED-I includes 10-item version works equally well on the basis of their correlation with related measures of cognitive status and nutritional status. 28 Improvement in these evaluation methods or more incorporated established indicators for food intake and eating behaviors, and nutrition status are required in the future work to confirm our results. Also, training plans for family caregivers could be designed according to the experiences of professional nurses and thus can optimize our study aim.
Conclusions
Hand exercise is a safe and effective intervention to improve the feeding and eating of people with AD. Since specific instrument and technique are not required, a better compliance and generalization could be expected.
Relevance to Clinical Practice
The significant improvements in eating and feeding suggested this intervention is workable. A training course could be designed and conducted by professional nurses to teach the nursing staff and family caregiver, to reduce the care burden and help the patients with AD with good physical and psychological status.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Fujian Provincial Medical Innovation Project (No. 2015-CX-3).