
Abstract
Objective:
To examine the patterns of statin use and determine the 3-year adherence and discontinuation rates among a cohort of Australians aged ≥65 years with dementia.
Methods:
The yearly prevalence and incidence of statin use were compared via Poisson regression modeling using 2007 as the reference year. People with dementia were identified according to dispensing of antidementia medications. A cohort of 589 new statin users was followed longitudinally. Adherence was estimated via the proportion of days covered (PDC). Discontinuation was defined as ≥90 days without statin coverage.
Results:
The annual prevalence of statin use among older Australians with dementia increased from 20.6% in 2007 to 31.7% in 2016 (aged-sex adjusted rate ratio: 1.51, 95% confidence interval: 1.35-1.69). Among the new users, the proportion adherent (PDC ≥ 0.80) decreased from 60.3% at 6 months to 31.0% at 3 years. During the 3-year follow-up, 58.7% discontinued their statin.
Conclusions:
Despite increased use of statins among older Australians with dementia, adherence is low and discontinuation is high, which may point to intentional cessation.
Background
Dementia is a medical condition of significant global importance, affecting more than 30 million people worldwide. 1 In Australia, there are over 400 000 individuals living with dementia. 2 This number is projected to grow as the population ages and is estimated to exceed 1.1 million by 2056. 3 Dementia, which is characterized by a cluster of symptoms including cognitive, behavioral, psychological, and muscular changes, is a progressive disease and usually leads to death 7 to 10 years after the onset of symptoms. 4
Dyslipidemia, especially when occurring during middle life, is associated with increased risk of dementia, particularly the cerebrovascular subtype. 5,6 Statins (3-hydroxy-3-methylglutaryl coenzyme A [HMG-CoA] reductase inhibitors) are one of the most commonly prescribed medications and are effective at reducing low-density lipoprotein cholesterol (LDL-C) levels. 7 Cohort analyses have reported that statins may reduce the risk of dementia, 5,8 but these benefits have not been observed in randomized clinical trials, with a recent Cochrane review concluding that statins are not effective at preventing or treating dementia. 9 Consequently, it has been recommended that statins be prescribed mainly for their known cardiovascular and metabolic indications. 10
In Australia, guidelines recommend that statins be prescribed for primary and secondary prevention of cardiovascular diseases. Guidelines highlight the need for clinicians to exercise clinical judgment to assess the balance between the benefits and risks of treatment. 11 In particular, among persons with vascular dementia, careful treatment of high cholesterol and other risk factors such as hypertension (while avoiding episodes of low blood pressure) and diabetes have been emphasized. 12 There is however paucity of evidence regarding the benefits of statins among older persons with life-limiting illness such as advanced dementia. 13 This creates a clinical conundrum. Statins have also been linked to cognitive impairment, although the evidence is weak and mixed. 14 Older people with dementia are at higher actual or perceived risk of statin-related adverse events (eg, muscle pain, falls). 15 These along with functional disability in those with dementia mean that adherence is often poor, which may further reduce any likely gains from statin treatment. 16 Yet past studies have reported high statin use among those with dementia. Among a cohort of older Americans with advanced dementia, around 1 in 6 used statins, 17 sometimes even up to the last weeks of life. 13
In Australia, little is known about the patterns of statin use among older persons with dementia. Thus, in this study, we aimed to (1) estimate the prevalence and incidence of statin use and (2) examine the patterns of adherence and discontinuation of statin therapy among a cohort of Australians aged 65 years and over with dementia.
Methods
Data Sources
We utilized pharmacy medication claims data from the Pharmaceutical Benefits Scheme (PBS) covering a 10% random sample of the Australian population. 18 The PBS is the part of Australia’s universal health coverage mechanism that subsides cost of prescription medications to residents of Australia and temporary visitors from countries with reciprocal health care with Australia.
Pharmaceutical Benefits Scheme data were supplied by the Australian Government Department of Human Services. The information contained in the PBS data sets included patient information (sex, year of birth, year of death), records of drugs dispensed (item number, name, quantity, and date of dispensing), prescriber details (eg, specialty), and concession status. Medical examinations and tests (eg, Mini-Mental State Examination) are not recorded in the PBS data sets. The PBS data are deidentified, with each person being assigned a unique identifying code. Statin scripts were identified by the relevant World Health Organization Anatomical Therapeutic Chemical Classification System (ATC) codes. Both single (ATC codes C10AA) and combination products (ATC codes C10 BX and C10BA) of 5 statins were included: atorvastatin, rosuvastatin, fluvastatin, simvastatin, and pravastatin. Cerivastatin and pitavastatin were excluded in the current analysis as the former was withdrawn from the market in 2001 and the latter is not listed on the PBS. 19 Lovastatin is also not available in Australia.
The statins were grouped according to intensity based on their capacity to lower LDL-C. As per their daily doses, statins that reduce LDL-C by <30%, 30% to 50%, and ≥50% were categorized as low, moderate, and high intensity, respectively (Supplemental Table S1). 20
Study Population
This study was carried out among older adults (aged ≥ 65 years) with dementia. As no diagnostic information is available in the PBS data sets, dementia was considered to be present in any person who was “ever” dispensed antidementia medication (ATC codes N06DA02, N06DA03, N06DA04, and N06DX01) 21 in the period between April 2005 and December 31, 2016. Persons were deemed to have dementia from the date of their first dispensing of antidementia medication. In Australia, cholinesterase inhibitors and memantine are subsidized via PBS only for Alzheimer’s dementia. Previous research has suggested that around 18 000 Australians were using medications indicated for dementia in 2004. 22 In the period 2005 to June 2012, statins that were priced below the “general patient copayment threshold” were not recorded in the PBS data sets. 23 Statins also became less expensive, and the general patient copayment increased over the study period, meaning that general patients may be likely to attract PBS subsidies over the study period. Therefore, our analysis was restricted to “long-term concession” individuals because complete records of their medications were available for the analysis period. 18 This restriction was consistent with previous analyses of PBS data. 23 Previous studies have suggested that long-term concession individuals constitute over 65% of all Australians receiving medications for chronic diseases. 23,24
Outcomes
The 1-year prevalence of statin use was calculated by dividing the number of persons with dementia who were dispensed ≥1 statin script during a calendar year by the total number of persons with dementia (study population) in the particular year. 25,26 The 1-year incidence of statin use was computed by dividing the number of new statin users in the particular year by the total number of persons with dementia in that year, excluding those who were dispensed statin or other lipid-lowering therapies in the previous year. 27 Medication records in 2006 were used as the control period to determine the number of new users in 2007. The certainty in the patterns of statin prevalence and incidence use were tested in a sensitivity analysis by varying the study population to include all persons who received ≥80% of medications under concession.
Among the persons with dementia, we selected a cohort of new statin users who commenced statin between January 1, 2007, and June 30, 2016. We defined a new user as any person with dementia dispensed statins but who otherwise had not been dispensed statins in the previous 12 months. 26 This new user cohort comprised of no-dementia medication group (those who had stopped taking antidementia medication at study entry, ie, at the time of statin initiation) and dementia medication group (those receiving dementia medication at study entry). This cohort was followed up to 3 years, until death or December 31, 2016, whichever came first. For those who died, only year of death is captured in the PBS data set. Thus, for the purposes of our analyses, we considered the month of death to be the month following their last dispensation (for all medications) in the data set.
We estimated statin adherence via the proportion of days covered (PDC). 28 By assuming a dosage of 1 tablet per day, we calculated the PDC for each period by dividing the number of days that was covered by a statin dispensation by the number of days in the period with necessary adjustments made if persons had early refills (ie, persons were deemed to start the new medication only after the estimated completion date of the current dispensation). In line with previous studies, we defined adherence as PDC ≥80%. 29 Adherence was calculated over a cumulative period of 6 months to 3 years. As the most regularly dispensed statin quantity in Australia is for 30 days, we considered discontinuation to have occurred if 90 or more days elapsed at the end of a statin dispensation without a new refill. In sensitivity analyses, the 90-day window was varied to 45 and 180 days. Persons who switched between different statins were deemed to be persistent with statins.
Statistical Analysis
Descriptive statistics were used to summarize the characteristics of older adults with dementia in each year. The prevalence and incidence of statin use were calculated for each calendar year, and the relative changes were compared via Poisson regression modeling using 2007 as the reference year. We adjusted for age and sex as well as the proportion of individuals who were active recipients of antidementia medications in the respective years. Age-adjusted gender differences were also determined as were sex-adjusted age differences in statin use. We estimated the probability of and time to discontinuation of statin therapy via competing risk proportional hazards regression model, death being the competing risk. 30 The variables included in the model were age, sex, statin type, intensity, and status of dementia medication use (ie, whether receiving antidementia medication or not). Analyses were performed with Stata software (Stata/IC v14.1; StataCorp, College Station, Texas).
Ethical Approval
Our study was approved by the Monash University Human Research Ethics Committee. The PBS data sets were provided by the Australian Government Department of Human Services that reviewed this report prior to submission.
Results
The number of older adults with dementia in the 10% PBS data set more than doubled from 2074 in 2007 to 4161 in 2016. Over 65% of the persons with dementia in each year were women. More than 80% of the older Australians with dementia in each year were also aged 75 years and over (Table 1). The mean age of the persons with dementia increased slightly from 81.7 (standard deviation [SD] ±6.9) years in 2007 to 83.0 (SD ±7.1) years in 2016 (P = .635). On average, 56% of the people with dementia in each year were being dispensed antidementia medications (eg, anticholinesterase inhibitors or memantine).
Characteristics of Older Australians With Dementia and Their Patterns of Statin Use From 2007 to 2016.a
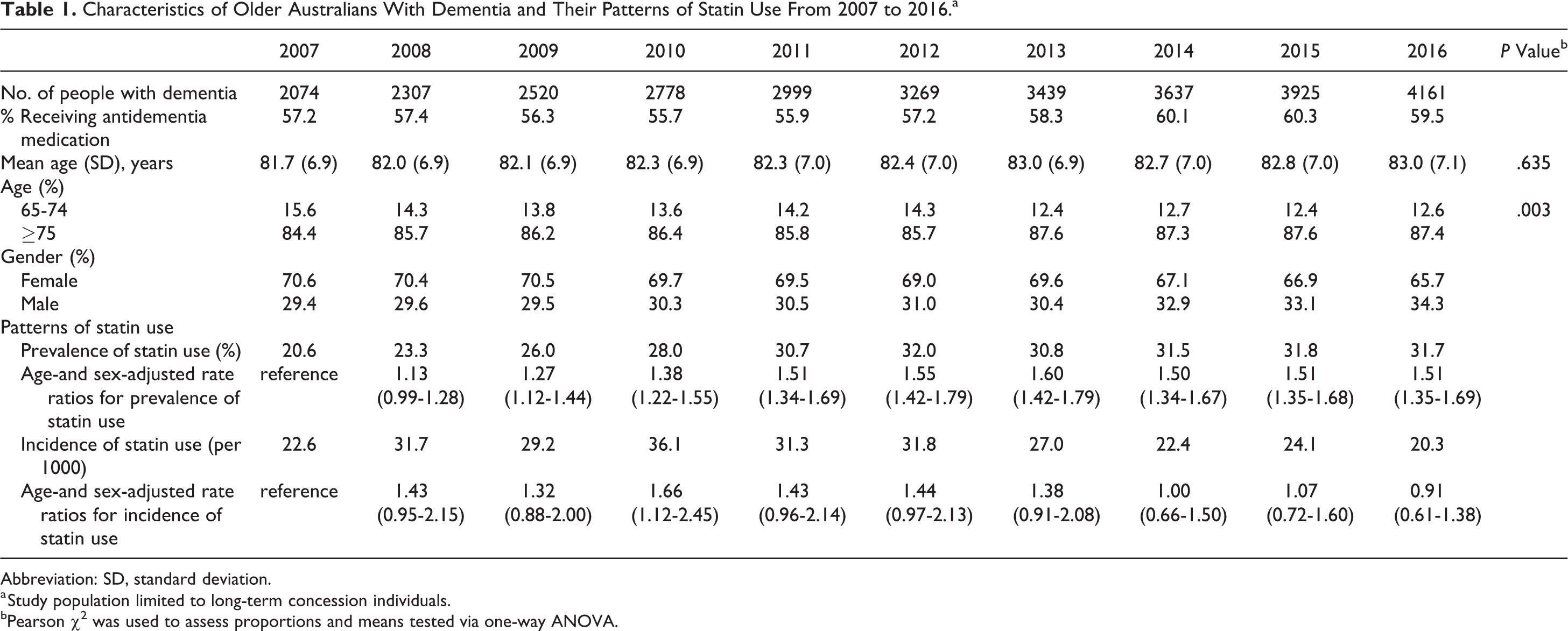
Abbreviation: SD, standard deviation.
a Study population limited to long-term concession individuals.
bPearson χ2 was used to assess proportions and means tested via one-way ANOVA.
The prevalence of statin use increased from 20.6% in 2007 to 31.7% in 2016 (age-sex adjusted rate ratio [RR]: 1.51, 95% confidence interval [CI]: 1.35-1.69). Compared to those currently dispensed antidementia medications, older adults with dementia not actively receiving anti-dementia medications were less likely to be dispensed statins (RR: 0.46, 95% CI: 0.44-0.49; Figure 1A). Among those who were currently receiving antidementia medications, the proportion of statins being dispensed increased from 25.7% in 2007 to 41.1% in 2016 (RR: 1.49, 95% CI: 1.32-1.69), whereas the proportion of persons no longer receiving antidementia medications who were dispensed statins increased from 10.1% in 2007 to 17.8% in 2016 (RR: 1.59, 95% CI: 1.26-1.99). There were no gender differences in the prevalence of statin use (age-adjusted rate ratio [aRR] for males compared to females: 1.03, 95% CI: 0.99-1.08). Similarly, those aged ≥75 years were no less likely to be using statins than those aged 65 to 74 years (sex-adjusted rate ratio [sRR] for ≥75 years compared to 65- to 74-year-olds: 0.98, 95% CI: 0.93-1.04).
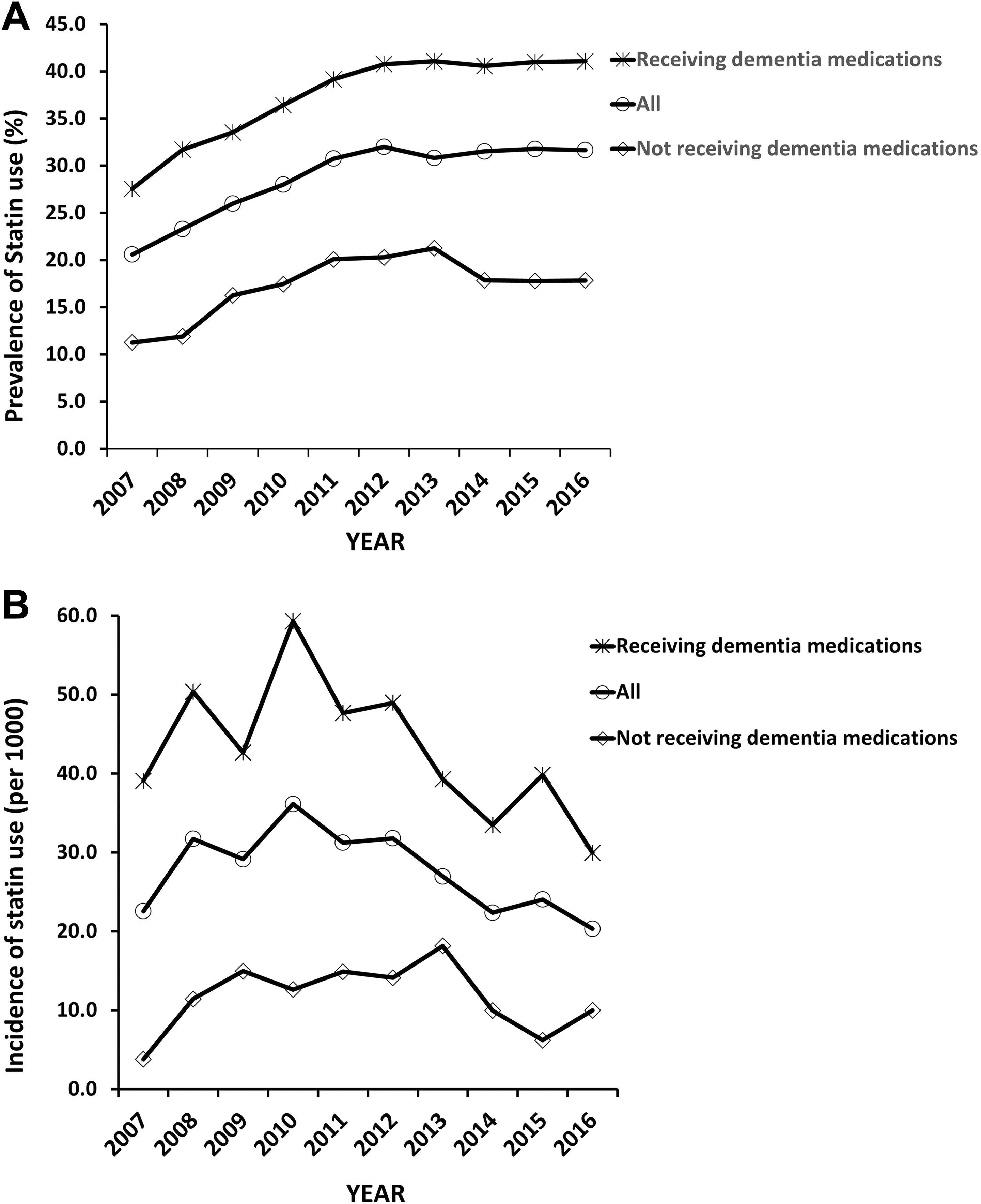
Trends in the (A) prevalence and (B) incidence of statin use among older adults with dementia who are receiving antidementia medications and those off dementia medications.
The incidence rate of statin use in 2007 was 22.6 per 1000. It then attained a peak of 36.1 per 1000 in 2010 (RR: 1.66, 1.12-2.45), before declining to 20.3 per 1000 in 2016 (aRR: 0.91, 95% CI: 0.61-1.38). Compared to those who were still dispensed antidementia medications, people with dementia no longer dispensed antidementia medications were less likely to be initiated on statin therapy (RR: 0.29, 95% CI: 0.24-0.35; Figure 1B). Among those who were currently receiving antidementia medications, the incidence of statin use in 2007 and 2016 was 39.1 per 1000 and 29.1 per 1000 (RR: 0.76, 95% CI: 0.48-1.18), respectively. Conversely, the incidence among persons no longer receiving antidementia medications was 3.8 per 1000 in 2007 and 10 per 1000 in 2016 (RR: 2.67, 95% CI: 0.77-9.3). There were no gender differences in the statin initiation rate (aRR for males compared to female: 1.16, 95% CI: 0.98-1.38). However, compared to those aged 65 to 74 years, persons with dementia aged ≥75 years were less likely to be initiated on statin therapy (sRR: 0.65, 95% CI: 0.54-0.79).
Varying our study population to include all persons who received ≥80% of their medications under concession resulted in similar patterns of prevalence and incidence of statin use (data not shown). A cohort of 589 older adults with dementia who commenced statins between January 2007 and June 2016 were assembled for the longitudinal analysis. The mean age of the cohort was 80.6 (±6.0) years, and 64.0% were females. Eighty percent were receiving antidementia medications at the time of statin initiation. Of the cohort, 4.7%, 70.7%, and 24.6% started on low, moderate, and high intensity statins, respectively. The proportion prescribed atorvastatin, rosuvastatin, simvastatin, and other statin (fluvastatin or pravastatin) was 54.9%, 24.8%, 16.8%, and 3.5%, respectively. Over the 3-year follow-up period, 18.4% of the older adults with dementia died.
The mean PDC of the cohort decreased from 0.73 at 6 months to 0.52 at 3 years. The proportion of people who were adherent to statin therapy was 60.3%, 51.2%, 40.4%, and 31.0% at 6 months, 1 year, 2 years, and 3 years, respectively. On the other hand, the proportion of statin users who had a very low PDC (<0.20) increased over time, being 16.3%, 18.8%, 21.7%, and 26.5% at 6 months, 1 year, 2 year, and 3 years, respectively.
Of the cohort of new statin users followed longitudinally for up to 3 years, 58.7% discontinued statins based on a 90-day gap criteria. The overall discontinuation rate was 38.1 events per 100 person-years. The likelihood of stopping statin medication within 6 months or 1 year after commencement was 22.9% and 36.9%, respectively. There were no significant gender differences in the likelihood of statin discontinuation (hazard ratio [HR] for males compared to females: 1.25, 95% CI: 0.99-1.56). Compared to people with dementia not receiving antidementia medications, people receiving antidementia medications were no more likely to discontinue their statin medication (HR: 0.88, 95% CI: 0.68-1.13). The overall proportion of the cohort discontinuing statins when 45- and 180-day gaps were applied was 71.0% and 47.4%, respectively. The likelihood of stopping statin medication within 1 year when using the 45- and 180-day gaps was 50.5% and 24.7%, respectively (Figure 2).
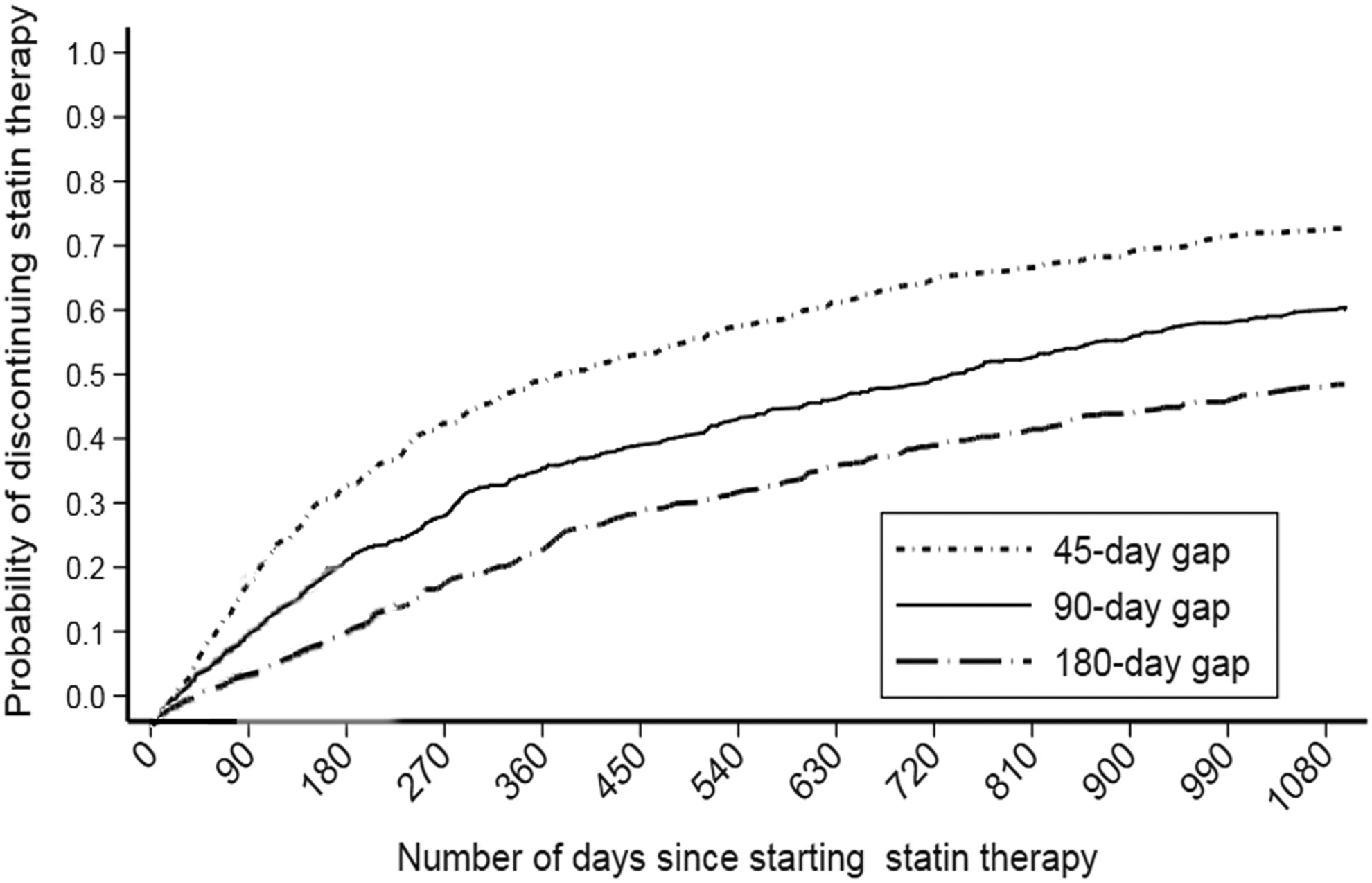
Cumulative incidence function (CIF) curves of the probability of discontinuing statin therapy in older adults with dementia in which stopping therapy was defined as a tablet-free period of at least 45, 90, and 180 days, respectively.
Discussion
Statin Utilization
Our analysis suggests increased use of statins among older adults with dementia over the 2007 to 2016 period. Compared to 2007, persons with dementia in 2016 were 51% more likely to be using statins, but the likelihood of initiating statin therapy remained largely stable. The increase in statin use is generally in line with overall increased utilization of statins among older adults, both in Australia and in most developed countries. 26,31,32 Persons who were no longer receiving antidementia medications were less likely to be using and/or initiate statin therapy. While we had no clinical data, we speculate that these persons may be those with advanced dementia among whom the benefits of statin therapy may no longer outweigh the risk of adverse events. 17
Statin Adherence
Statin adherence among the older adults with dementia was poor. Nearly 40% of persons were classified as nonadherent within the first 6 months and just 1 in 3 people were adherent at 3 years. These patterns are not surprising as poor adherence to statins and other medications have been reported among people with dementia. 33,34 Poor adherence to prescribed medication has been attributed to multiple factors, including challenges with memory and executive functioning. 16,35 Smith and colleagues 16 have noted previously that despite many interventions being implemented to improve medication adherence among the general older population, few have been tailored to people with dementia who have particular challenges with medication adherence. 16 Nonetheless, a recent systematic review that included 10 studies reported that frequent human reminders were more likely to improve adherence among patients with dementia than nonhuman reminders. 36 Additionally, interventions aimed at enhancing the knowledge of informal care workers may help to improve medication adherence in people with dementia. 37
Statin Discontinuation
In our study, over 47% discontinued statin therapy over a period of 3 years regardless of the gap length chosen. These rates are high when compared with statin discontinuation rates among the general older population, 38,39 as well as the statin discontinuation reported for people with dementia in other jurisdictions. 17 Our statin discontinuation rate is, however, comparable to those reported among those with other terminal illnesses such as advanced cancers 40,41 among whom deprescribing may be recommended. 42 Indeed, given the paucity of evidence to support the benefits of statins in persons with limited life expectancy, 17,40 the high discontinuation rate may reflect a conscious and legitimate decision to discontinue treatment in people for whom the likely benefits may no longer outweigh the risk of adverse events. 40,43 A recent meta-analysis that pooled data from over 13 countries found that those with dementia were about 18% more likely to discontinue statins than those without dementia. 34 Kutner and colleagues also reported that discontinuing statins in a setting of advanced life-limiting illness was not only associated with cost savings but also improved patients’ quality of life. 44
Methodological Considerations
We found that among our cohort prescribed antidementia medications at some point, only around half were actively taking antidementia medications at any one time. This pattern may be explained by the fact that antidementia medications may be discontinued when the disease is advanced. 45 Studies from Europe and North America have reported that around 20% to 40% of persons with dementia were using antidementia medications at any point. 46 –48 Comparisons of these estimates with our study results should be with caution as there are methodological differences. In particular, prior dispensing of antidementia medications was used to define our cohort in our analyses. Assessing the utilization of antidementia medications was not the aim of this study. In prior studies, clinical information was available; thus, persons with dementia could be identified whether they have ever been prescribed antidementia medications or not.
Strengths and Limitations
Our study has several strengths and limitations. To our knowledge, this is the first study to detail the patterns of statin use among older Australians with dementia, which should support future research into lipid-lowering medication use among persons with dementia. A limitation of our analysis is that we had no information as to why statin medications were discontinued and thus were unable to determine whether this was clinically appropriate or not. Additionally, due to the lack of hospitalization records in the PBS data sets, treatment gaps were likely to have been overestimated and adherence underestimated among patients who were hospitalized (those in residential aged care are likely to have been also excluded). Also, because we use only drugs to identify persons with dementia, we most likely capture only Alzheimer’s dementia due to the PBS subsidy rules. Furthermore, as is typical of medication claims-based research, we were unable to ascertain whether people actually took the dispensed statins. Our study population was defined only on the basis of medication records, and thus, we may have excluded some persons with dementia who were never prescribed antidementia medications. Finally, restricting our sample to only long-term concession patients meant that we had smaller number of individuals to follow-up longitudinally, and a larger sample-based analysis may be required.
Conclusion
Statins use among older Australians with dementia has increased, although incidence has remained stable. Adherence is also low, which will need to be addressed particularly if statins are deemed to be clinically necessary. Statin discontinuation rates are high, which may also point to intentional cessation.
Supplemental Material
Supplementary_Material - Prevalence and Incidence of Statin Use and 3-Year Adherence and Discontinuation Rates Among Older Adults With Dementia
Supplementary_Material for Prevalence and Incidence of Statin Use and 3-Year Adherence and Discontinuation Rates Among Older Adults With Dementia by Richard Ofori-Asenso, Jenni Ilomaki, Mark Tacey, Andrea J. Curtis, Ella Zomer, J. Simon Bell, Sophia Zoungas, and Danny Liew in American Journal of Alzheimer"s Disease & Other Dementias
Footnotes
Authors’ Note
The data underlying this paper can be accessed via direct application to the Australian Government Department of Human Services.
Acknowledgments
The authors would like to acknowledge the Australian Government Department of Human Services for the provision of the data.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Sophia Zoungas reports past participation in advisory boards and/or receiving honoraria from AstraZeneca/Bristol-Myers Squibb Australia, Janssen-Cilag, Merck, Sharp, Dohme (Australia), Novartis Australia, Novo Nordisk, and Sanofi and Servier Laboratories for work unrelated to this study. Danny Liew reports past participation in advisory boards and/or receiving honoraria from Abbvie, Astellas, AstraZeneca, Bristol-Myers Squibb, Novartis, Pfizer, and Sanofi and Shire for work unrelated to this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Richard Ofori-Asenso is supported by a Monash Graduate Scholarship and Monash International Postgraduate Research Scholarship for his doctoral studies. Jenni Ilomaki is funded by a National Health and Medical Research Council Early Career Fellowship. J Simon Bell is funded by a National Health and Medical Research Council Dementia Leadership Fellowship. Sophia Zoungas is funded by a National Health and Medical Research Council Senior Research Fellowship.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.