
Abstract
Scripted-IMPROV (SI) is a nonpharmacological (ecopsychosocial) intervention that consists of semi-improvised drama performances specifically designed for persons with dementia (PWD). In this 12-site study, 178 PWD took part in the SI intervention. Levels of engagement/affect were assessed at baseline and again during SI performances; quality of life (via the Dementia Quality of Life scale) and depression (via the Geriatric Depression Scale-Short Form [GDS-SF]) were assessed at baseline and post-treatment. Positive forms of engagement/affect increased, while negative forms of engagement decreased. Regarding depression, for a subsample of 29 participants who scored in the depressed range on the GDS-SF at baseline, depressive symptoms were reduced at post-treatment. Although overall quality of life did not change, the increase in positive affect during SI suggests that quality of life was higher during the intervention itself. In conclusion, SI possesses the characteristics of a high-quality intervention for PWD and seems worthy of further investigation in future research.
Introduction
There is a strong public health need for cost-effective ecopsychosocial interventions 1 —formerly called nonpharmacological treatments—that can reduce the behavioral symptoms, exhibited by up to 90% of persons with dementia (PWD). 2 –4 Such interventions are often disregarded or overlooked, because evidence of their effectiveness is based on studies involving small sample sizes, that rely primarily on qualitative data, or employ primarily anecdotal evidence. This study involved the development and evaluation of an innovative ecopsychosocial intervention aimed to overcome these limitations.
The goal of the present study was to examine the effects of the Scripted-IMPROV intervention (described below) on engagement, affect, and depression in PWD. The study also serves as a test of what the authors are calling the Engagement Replacement Model (ERM). The Engagement Replacement Model purports that PWD who take part in engaging activities that allow them to succeed exhibit fewer behavioral disturbances because engagement takes the place of these behaviors in the person’s attention. An “engaging activity” is one in which “participants are engaged with each other in a socially appropriate and/or altruistic manner. Examples include a long-term care resident making eye contact with peers, saying ‘hello’ to peers, and reading aloud to a resident who is blind.” 5 According to the ERM, if a person is taking part in an engaging activity, they cannot at the same time exhibit apathy (lack of interest, concern, or emotion), aggression (verbal or physical behavior that harms others), nor any other challenging behavior, such as agitation, anxiety, and wandering.
The ERM is not a model explicitly espoused by a specific researcher or group of researchers. Nevertheless, the ERM underlies many ecopsychosocial interventions for PWD developed and studied over the past decades. 6 –14 As Cohen-Mansfield, Dakheel-Ali, and Marx state, “The study of engagement is a necessary foundation for the development of nonpharmacological interventions for persons with dementia, whether the interventions address depression, agitation, apathy, loneliness, or boredom.” 15 Kolanowski, Litaker, and Buettner claim that activities “tailored to meet individual needs…improve behavioral symptoms associated with dementia.” 16 Camp, Skrajner, and Gorzelle have stated that “if a person with dementia is positively engaged, he or she will not carry out unacceptable responsive behaviors, such as attempting to escape or repetitive actions.” 5
Intervention
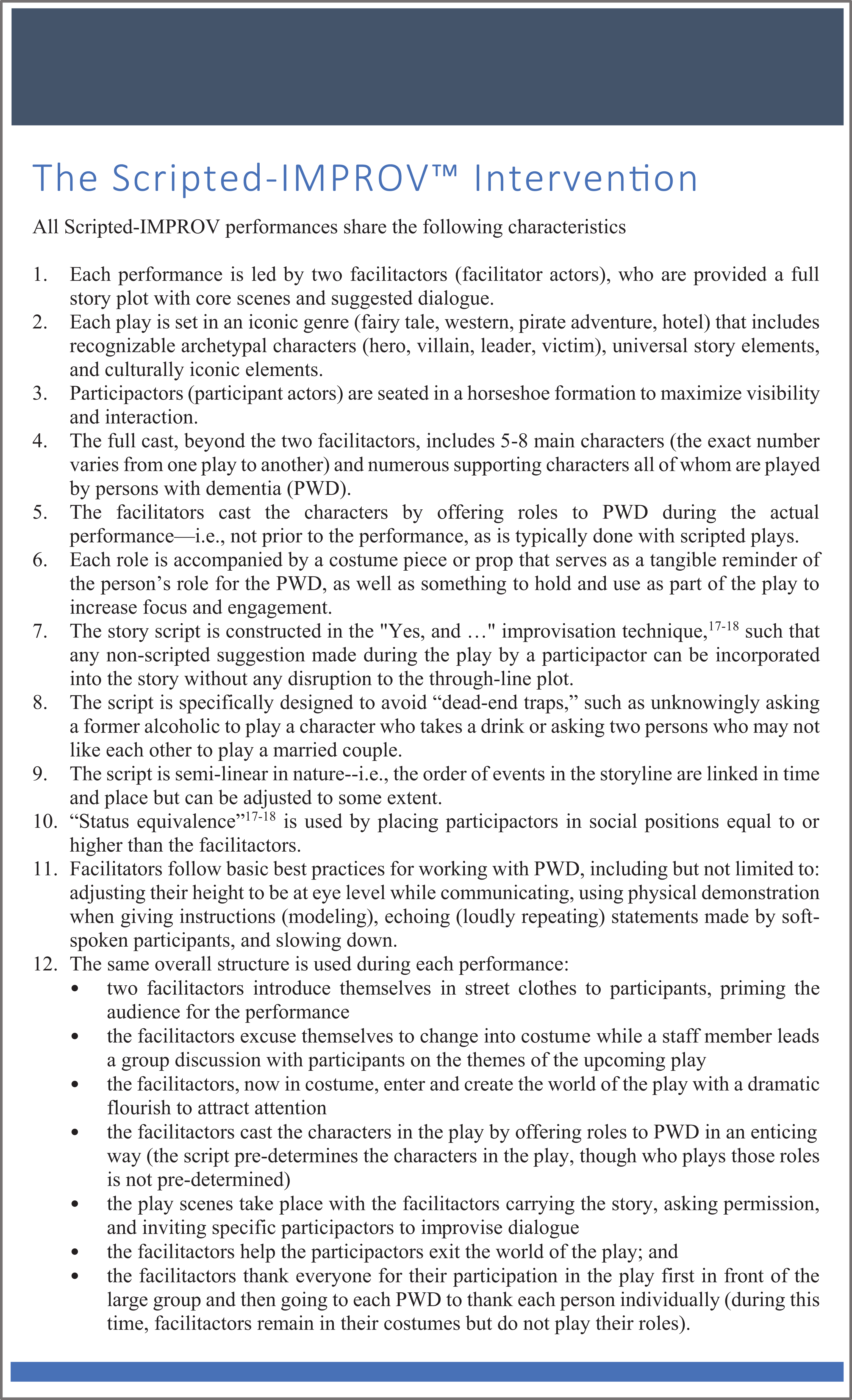
The Scripted-IMPROV intervention consists of semi-improvised drama performances specifically designed for PWD. In a Scripted-IMPROV performance, the narrative of a loosely scripted play is carried out by two “facilitactors”—that is, staff and/or actors who facilitate the performance. In the present study, two New York-based actors (Evan Bass Zeisel [stage name Evan Bass] and Miranda Noelle Wilson) served as facilitactors for all performances (nonactors/site staff have successfully served as facilitactors for Scripted-IMPROV performances after the completion of the present study). Facilitactors are provided with a full script, indicating core scenes and suggested dialogue. During the performance, participants with dementia, called “participactors” (participant actors), take on main character roles in the story, such as the captain of a pirate ship, the deputy of a town in the Old West, or the Elephant Wizard in a fantasy tale. Other PWD engage with facilitactors and fellow participactors by improvising in other ways—for example, by creating “waves” when the pirate ship goes out to sea, dancing during a birthday celebration for a character, helping to identify clues for the deputy and sheriff, and so on. All contributions by participactors are improvised: they do not need to read or remember lines, and plays are specifically designed so that any improvisation a PWD contributes is always appropriate and can be integrated into the ongoing story.
Scripted-IMPROV performances are designed to take place at nursing homes (NHs), assisted living facilities (ALFs), and adult day centers (ADCs). In other words, participactors are not expected to travel to a theater or other performance space to take part in a performance. In pilot work conducted prior to the present study, the authors found that an appropriate group size for a Scripted IMPROV performance lies in a range from 15 to 25 participants. However, for reasons explained below, group sizes were sometimes larger in the present study (with no apparent negative outcomes).
In an effort to offer a variety of storylines for study participants (and for future Scripted-IMPROV users), four plays were written and performed: Ahoy, Me Pirate Tale! (a swashbuckling pirate adventure), Dream Hotel (a choose-your-own adventure story set at the luxurious Hotel Rêve), The Land of Wondermore (a fantasy tale inspired by the Wizard of Oz), and The Brute of Brut 33 (a murder mystery set in the Old West).
Since there are four different plays, and since the intervention is semi-improvisational in nature, each Scripted-IMPROV performance is unique. However, as shown in Figure 1, all Scripted-IMPROV performances share a variety of important characteristics. Plays are designed to give all participants an opportunity to be in a judgment-free zone where whatever character they decide to create is acceptable and validated. Each potential participactor is offered a choice to participate or not, and the choice remains available to join the fully interactive performance at any time throughout the performance or to leave. No one is forced to participate in any way. Performances typically last approximately 75 minutes, inclusive of the time that facilitactors spend introducing themselves in street clothes and thanking people individually at the end of the play.
Key Characteristics of the Scripted-IMPROV Intervention
The goal of the study was to determine whether the Scripted-IMPROV intervention increases the levels of positive engagement/affect, reduces levels of negative engagement/affect, and whether engagement/affect levels produced by Scripted-IMPROV differ between various types of sites (NHs, ALFs, and ADCs). The study also examined the effect that the intervention has on symptoms of depression and overall quality of life.
Methods
Design
The study employed a between-groups quasi-experimental pre-test–post-test design, with data gathered at baseline (preintervention) and again at treatment (measurement of engagement/affect) or post-treatment (measurement of depression and quality of life indicators).
Settings
The study was conducted at 12 research sites: four ADCs, four ALFs, and four NHs, half of which were in the Boston, Massachusetts area, and half in and around New York City, New York.
Participants
Inclusion criteria were as follows: Diagnosis of dementia (as recorded in medical records) and/or a Mini-Mental State Examination (MMSE)
19
raw score of 20 or lower, and The ability to speak English.
A raw score of 20 was chosen as the MMSE cutoff score for the presence of dementia, rather than a cutoff based upon education- and age-based norms, for two reasons. First, the authors were unable to obtain the level of education for some participants (especially ADC participants); second, a score of 20 is generally accepted as an indication of dementia for all age/education levels. 20 The MMSE total score was used in this study as an inclusion criterion and to estimate the level of dementia—it was not used as an outcome measure, as the authors did not expect the Scripted-IMPROV intervention to impact cognition.
To test the intervention with a wide variety of participants with different backgrounds, facilities of various sizes took part in the study. Some facilities housed only 20 participants, all of whom had dementia, while others housed more than 300 residents, only some of whom were diagnosed with dementia. Regardless of the size of the facility, to ensure an adequate sample size, every resident/client at each site with a diagnosis of dementia was invited to participate via a recruitment mailing sent to responsible family members. The total number of participants invited to participate at any single site ranged from approximately 20 to 150, while the final number of participants in each intervention session ranged from 14 to 55. In addition to sending recruitment packets, activity staff at the sites contacted family members by phone to recommend enrollment in the study. Family members responsible for the medical decisions of PWD enrolled the participants by reviewing and signing an informed consent form. Enrollment rates varied considerably between sites, with smaller sites generally having higher rates of enrollment (approximately 50%-70%) than larger facilities (approximately 25%-35%). After obtaining consent from family members, researchers obtained assent from PWD both by asking them whether they wanted to participate and by respecting their right to withdraw at any time. An external Institutional Review Board (IRB) approved all recruitment and study procedures.
To prevent a situation where only “ideal” candidates for the Scripted-IMPROV intervention would be enrolled in the study (eg, participants who regularly attend activities might be more likely to enjoy Scripted-IMPROV), the authors instructed staff to recommend the study equally to all family members, regardless of the level of dementia, type of dementia, and whether the person normally attends activities. In other words, the authors were interested in examining the effect of the intervention on a wide variety of PWD. Because of these attempts to enroll a wide range of participants, the study technically employed a convenience sample, since the sample consisted of all participants whose family members agreed to enroll them in the study.
Procedures
Researchers were extensively trained on data collection procedures for the study and were blind to the specific engagement, quality of life, affect, and depression hypotheses. However, by virtue of observing participants in the target intervention, they were not blind to the nature of the intervention itself. All study data were gathered initially via pen and paper and later entered into SPSS.
At baseline, a variety of measures were collected via chart review, direct interview with PWD, and/or proxy interview one to four weeks prior to the intervention period. In addition, four distinct five-minute observations of each participant were taken during standard, regularly scheduled activities using the six-item Menorah Park Engagement Scale (MPES). 5 All of these measures are described in detail below.
Since baseline data were collected over the course of four weeks, researchers had time to collect all baseline observations “live”—that is, video recording of PWD taking part in activities was not required. For each participant, two observations were taken during morning activities and two during afternoon activities. Researchers observed participants in a variety of activities, including but not limited to bingo, discussion groups, exercise programs, arts and crafts, balloon toss, sing-along, and reading groups. The goal was to randomly sample a wide variety of existing activities at each facility. In addition, the order of observations for a given activity was randomly chosen ahead of time by using a random number generator. The objective was to randomize the timing of observations as much as possible since it is possible that always taking observations for one participant in the early (or later) part of an activity could impact engagement levels.
After the baseline period, which took approximately one month, participants entered the treatment phase. During the treatment phase, each study participant took part in two different Scripted-IMPROV plays over the course of one week, one in the morning, and the other in the afternoon. Half of the sites/participants took part in The Land of Wondermore and The Brute of Brut 33, while the other half took part in Dream Hotel and Ahoy, Me Pirate Tale! Plays occurred at least two days apart (eg, on a Tuesday morning and a Thursday afternoon) to avoid as much as possible contamination of the second drama experience by the first.
As was the case during baseline, four MPES observations were taken on each participant during the treatment period (ie, during the Scripted-IMPROV performances). Two observations were taken on each participant during the morning play, and two were taken during the afternoon play. Again, each observation lasted five minutes.
Researchers implemented post-treatment measures two to four weeks after the Scripted-IMPROV plays were performed. The two-week variation in completion of the post-treatment measures was due to scheduling considerations (eg, some participants were unavailable during initial visits, so research staff had to return at different times).
Measures
Baseline
Diagnoses and type of dementia as well as demographics (age, gender, marital status, ethnicity, and education level) were collected via chart review. The MMSE 19 , the Geriatric Depression Scale-Short Form (GDS-SF), 21-22 and the Dementia Quality of Life scale (DEMQOL) 23 were conducted with each study participant via direct interview. The GDS-SF is a 15-item scale used to measure depression in older adults. Scores range from 0 to 15, with higher scores indicating more depressive symptoms. The DEMQOL is a 29-item scale designed to measure the quality of life of PWD. Scores range from 28 to 112, with higher scores indicating higher quality of life. If participants were unable to respond to questions on the DEMQOL, the proxy version of the DEMQOL was employed with caregivers.
As noted previously, four observations of participants attending standard, regularly scheduled activities at each site were taken at baseline using the MPES. 5 The MPES is an observational scale that measures four distinct types of engagement: constructive engagement (CE): motor or verbal behavior exhibited clearly in response to the target activity; passive engagement (PE): listening or watching the target activity; distracted engagement (DE): motor or verbal behavior exhibited in response to something other than the target activity; and nonengagement/apathy (NE): outward signs/indicators of apathy, such as sleeping, closing one’s eyes, and staring into space. The MPES also measures two types of affect: pleasure (PL): clearly observable smiling or laughing, interpreted as an observable indicator of higher quality of life; and anxiety/sadness (AS): tearfulness or clearly observable depressed affect (sadness), and/or hand wringing, rocking, anxious vocalizations, or other psychomotor activity in combination with an anxious facial display (anxiety). Anxiety/sadness is considered an observable indicator of low quality of life. Successful activity programs result in relatively high levels of CE, PE, and PL and relatively low levels of DE, NE, and AS. The “target activity” for the MPES was defined as the activity being implemented by staff (during baseline) or a Scripted-IMPROV performance (during treatment).
Each MPES observation period lasts five minutes. During this time, a researcher standing or sitting in an inconspicuous area of the activity room observes a single participant, then continues observing participants until all participants have been observed in either the baseline activity or the treatment intervention. At the end of the five-minute period, the researcher records the length of time that a participant exhibited the specific type of engagement/affect. For each MPES item, there are three options: not observed (coded as “0”), observed for up to half of the activity (coded as “1”), or observed for more than half of the activity (coded as “2”). For each participant, the MPES values for each item across all four observations are summed, and then a mean is calculated for that item. For example, if a participant scored 0, 2, 2, 1, for CE at baseline, then the mean baseline CE score for that participant would be 1.25 ((0 + 2 + 2 +1) / 4). This approach of analyzing MPES data has been used in previous research. 24
Extensive training ensures a high level of reliability across observers, with interrater reliability at approximately 90% for each MPES item. Periodic retraining on the MPES is conducted with researchers to maintain interrater reliability.
After the four baseline observations were completed for each participant, a mean for each of the six MPES items was calculated for that person. Taken together, the MPES means represent a “snapshot” of each person’s engagement levels during typical (non Scripted-IMPROV) programming and served as points of comparison for the Scripted-IMPROV intervention.
Treatment
As noted previously, four MPES observations were taken on each participant during the Scripted-IMPROV performances. Whenever possible, these treatment observations were taken “live”—that is, while a researcher stood or sat in an inconspicuous area of the room. However, due to the relatively large number of participants taking part in each Scripted-IMPROV performance, and the limited amount of time and number of researchers, some MPES observations were recorded via video and ranked afterward. (Only participants whose family members had given consent for video recording were observed in this way.) As with baseline, the order of observations was randomly selected ahead of time using a random number generator.
As was the case for baseline observations, a mean for each of the six MPES items was calculated for each participant. These means represent a “snapshot” of each person’s engagement levels during Scripted-IMPROV programming.
Post-treatment
At post-treatment, researchers interviewed participants to collect GDS-SF and DEMQOL data. The DEMQOL-proxy was used for participants who were unable to respond to the DEMQOL.
Results
Participants
A total of 178 PWD took part in the study. This included 46 ADC clients, 61 ALF residents, and 71 NH residents. Table 1 summarizes the characteristics of participants at baseline. Across all sites, the mean age was 85.5 (standard deviation [SD] = 7.5). The majority of participants (82%) were white. Seventy-five percent of participants were female. The sample was relatively well educated, with 38% of participants having at least a bachelor’s degree. It should be noted that these education data are based on participants for whom education information was available, as there were missing data for some participants, especially those from ADCs.
Characteristics of Scripted-IMPROV Participants at Baseline.
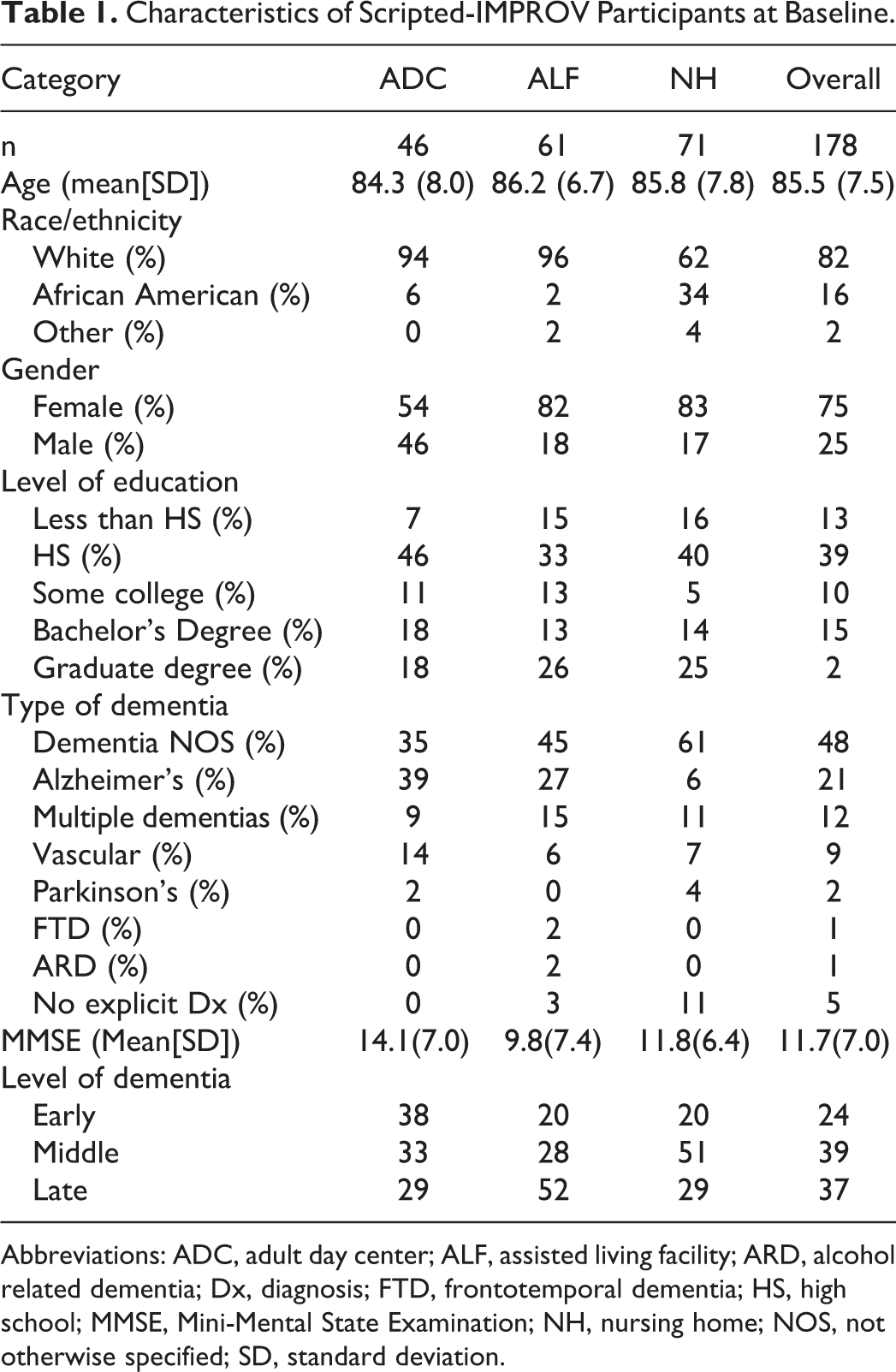
Abbreviations: ADC, adult day center; ALF, assisted living facility; ARD, alcohol related dementia; Dx, diagnosis; FTD, frontotemporal dementia; HS, high school; MMSE, Mini-Mental State Examination; NH, nursing home; NOS, not otherwise specified; SD, standard deviation.
The overwhelming majority of participants—that is, 169 (95%) of 178 —had a documented dementia diagnosis listed in their medical records. For the nine participants who did not have a documented diagnosis, nursing staff were surprised that the diagnosis was not recorded in their records and verbally indicated that the person did have dementia, despite the lack of a diagnosis listed in their medical records. For these participants, the mean MMSE score was 10.9 (SD = 6.1), with a range of 2 to 18. A considerable percent (48%) of participants had an unspecified form of dementia, typically referred to as “Dementia NOS (not otherwise specified).” Alzheimer’s disease was the second most common form of dementia (21%), followed by multiple dementias (12%) and vascular dementia (9%). For the 21 participants with multiple dementias, two had a dual diagnosis of Alzheimer’s disease and Parkinson’s Dementia, and 19 had dual diagnosis of Alzheimer’s disease and Vascular Dementia. The mean MMSE score for all participants was 11.7 (SD = 7.0), with scores ranging from 1 to 27. (It should be noted that participants who scored above 20 on the MMSE had documented dementia diagnoses.) The following MMSE total score ranges were used to estimate the level of dementia for each participant; late-stage dementia = 0 to 9; middle-stage dementia = 10 to 17; early-stage dementia = 18 or higher. Based on these ranges, 24% of participants were in the early stages, 39% in the middle stages, and 37% in the late stages.
The site categories (ADCs, ALFs, and NHs) did not differ in age, gender, or level of education. However, there were significant differences between the site categories on other items. In particular, there were significant differences between site categories on race/ethnicity (P < .01), type of dementia (P < .01), MMSE total score (P < .01), and level of dementia (P < .01). Regarding race/ethnicity, a higher percentage of African American participants were enrolled at NHs, as compared to the other site categories. Regarding the type of dementia, there was a higher percentage of NH residents with dementia NOS, and a lower percentage with Alzheimer’s disease, as compared to the other two sites. Regarding MMSE scores, ALF participants had significantly lower MMSE total scores than ADC participants (P < .01). Regarding the level of dementia, ALFs had the highest percentage of participants with late-stage dementia (52%), while ADCs had the highest percentage with early-stage dementia (38%).
Outcomes
Engagement/affect outcomes are shown in Table 2. Positive forms of engagement/affect increased from baseline to treatment in the overall sample, including all sites and all levels of dementia: Constructive engagement increased by 31% (P < .01, d = .52), PE increased by 13% (P < .01, d = .26), and PL increased by 100% (P < .01, d = .82). Negative forms of engagement decreased from baseline to treatment: levels of DE decreased by 79% (P < .01, d = .96) and NE decreased by 41% (P < .01, d = .36). Anxiety/sadness did not change significantly from baseline to treatment. Cohen’s d scores reflect large effect sizes for PL and DE, medium effect sizes for CE and NE, and small effect sizes for PE. 25
Scripted-IMPROV Engagement/Affect Outcomes, Baseline Versus Treatment: Means (Standard Deviations) on the Menorah Park Engagement Scale (MPES).
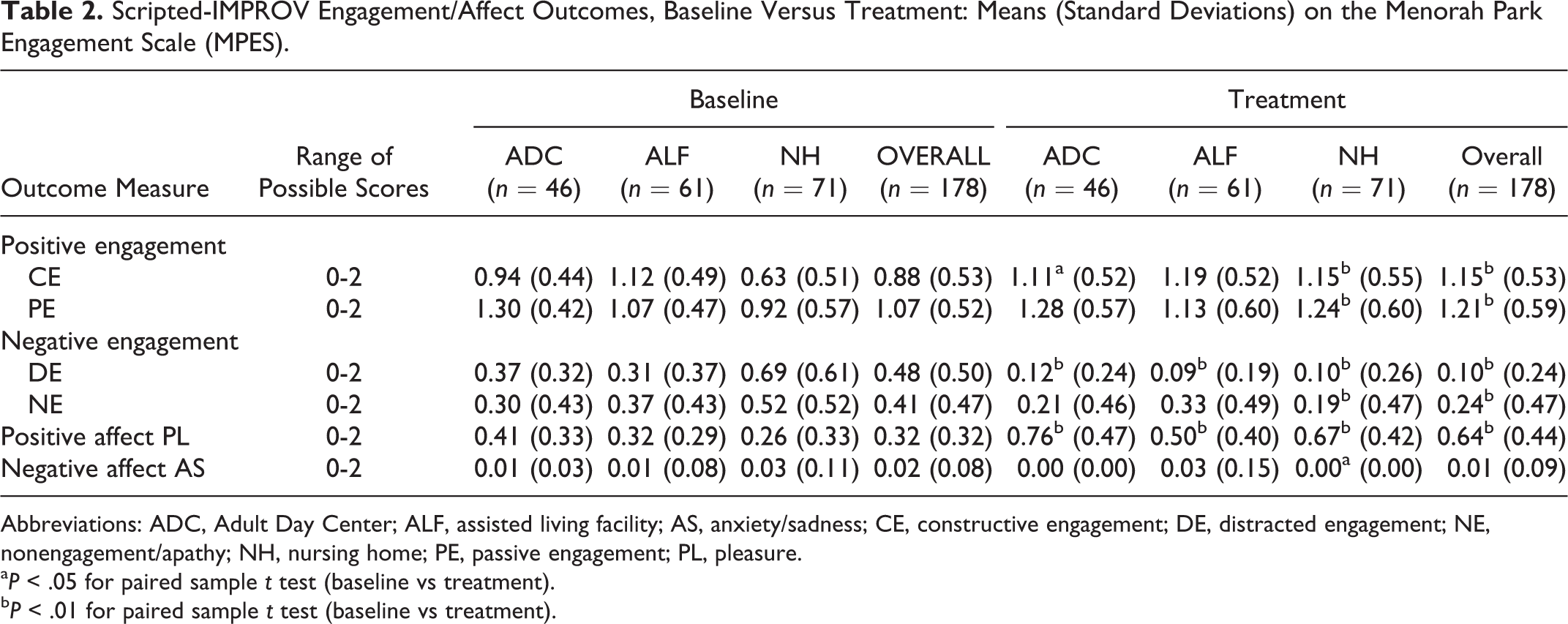
Abbreviations: ADC, Adult Day Center; ALF, assisted living facility; AS, anxiety/sadness; CE, constructive engagement; DE, distracted engagement; NE, nonengagement/apathy; NH, nursing home; PE, passive engagement; PL, pleasure.
a P < .05 for paired sample t test (baseline vs treatment).
b P < .01 for paired sample t test (baseline vs treatment).
At baseline, MPES scores differed significantly between the three site categories. For instance, NHs have significantly lower levels of CE in comparison with ALFs and ADCs (0.63, 1.12, and 0.94, respectively, with P < .01). Despite these between-site differences at baseline, MPES scores during the Scripted-IMPROV intervention were similar in all three site categories, with the one exception of PL, which was lower at ALFs during intervention, compared to ADCs and NHs (0.50, 0.76 and 0.67, respectively, with P < .01 for both comparisons). However, in ALFs, the data reflect the same basic trend seen in the other two site categories, an improvement from baseline to intervention—that is, from 0.32 to 0.50.
Study participants in all three site categories experienced statistically significant, positive changes from baseline to intervention. For ADCs, CE increased by 18% (P < .05), DE decreased by 68% (P < .01), and PL increased by 85% (P < .01). For ALFs, DE decreased by 71% (P < .01) and PL increased by 56% (P < .01). NH residents experienced the most profound changes, with CE increasing by 83% (P < .01), PE increasing by 35% (P < .01), DE decreasing by 86% (P < .01), NE decreasing by 63% (P < .01), and PL increasing by 158% (P < .01). Additionally, at NHs, AS decreased from 0.03 to 0.00 (P < .05). It should be noted that changes from baseline to treatment for each site category not mentioned here were not significant.
As noted previously, pilot work conducted prior to the present study suggested that groups of between 15 and 25 appeared to work best for Scripted-IMPROV performances. Most sites did, in fact, utilize groups of this approximate size. However, four of the sites exceeded this recommended group size. For example, at one NH, approximately 45 residents attended the Scripted-IMPROV performances. There were two main reasons for the large group sizes at these sites. First, there was a strong interest by residents/clients at these facilities, each of which housed more than 150 residents. Second, site staff could not devise a practical and/or ethical way to disallow interested residents/clients from attending a play. After all, the performances needed to take place in an easily-accessible area at each facility, and all residents/clients had the right to be in these places, should they so desire. We anticipated that such larger group sizes (ie, groups larger than 15-25) would negatively impact levels of engagement/affect, since each participant would have a reduced opportunity to engage with the two facilitactors. However, the data suggest that larger group sizes improved levels of engagement/affect. Larger group sizes produced significantly higher levels of PE (P < .01) and PL (P < .01), and significantly lower levels of NE (P < .05). Larger group sizes did not impact CE or DE.
Although we were primarily interested in examining the impact that site category had on engagement/affect levels, we were aware that other factors could affect engagement levels as well. Two relevant factors we considered were age and level of dementia. One might hypothesize that participants who are older and/or more impaired might not experience positive trends from baseline to treatment, when compared to younger and less impaired participants. To test this hypothesis, we conducted a multivariate analysis of covariance on the factors of age and the level of dementia. The multivariate test indicated that age and level of dementia did not have an impact on observed engagement trends from baseline to post-treatment.
As shown in Table 3, when the entire sample is analyzed, GDS-SF, and DEMQOL scores did not change significantly from baseline to post-treatment. The mean DEMQOL score was 94.40 (SD = 11.77) at baseline and 94.70 (SD = 12.45) at post-treatment; the mean GDS-SF score was 2.82 (SD = 2.68) at baseline and 2.66 (SD = 2.98) at post-treatment. However, as shown in Table 4, for the 29 participants who scored in the clinically depressed range (≥6) on the GDS-SF at baseline, there was a statistically significant reduction in symptoms of depression at post-treatment (P < .01, d = 0.62). The mean baseline GDS-SF score of 7.24 decreased at post-treatment to 5.07, which is below the GDS-SF cutoff for clinical depression. With a Cohen’s d of .62, the effect size was in the medium/large range. The characteristics of the clinically depressed subsample are shown in Table 5. Although the differences were not statistically significant, the clinically depressed subsample compared to the nondepressed participants in the full sample included a higher percentage of NH residents, had a slightly lower level of education, and included a lower percentage of persons with Alzheimer’s type dementia.
Scripted-IMPROV Depression and Quality of Life Outcomes, Baseline Versus Posttreatment: Means (Standard Deviations).
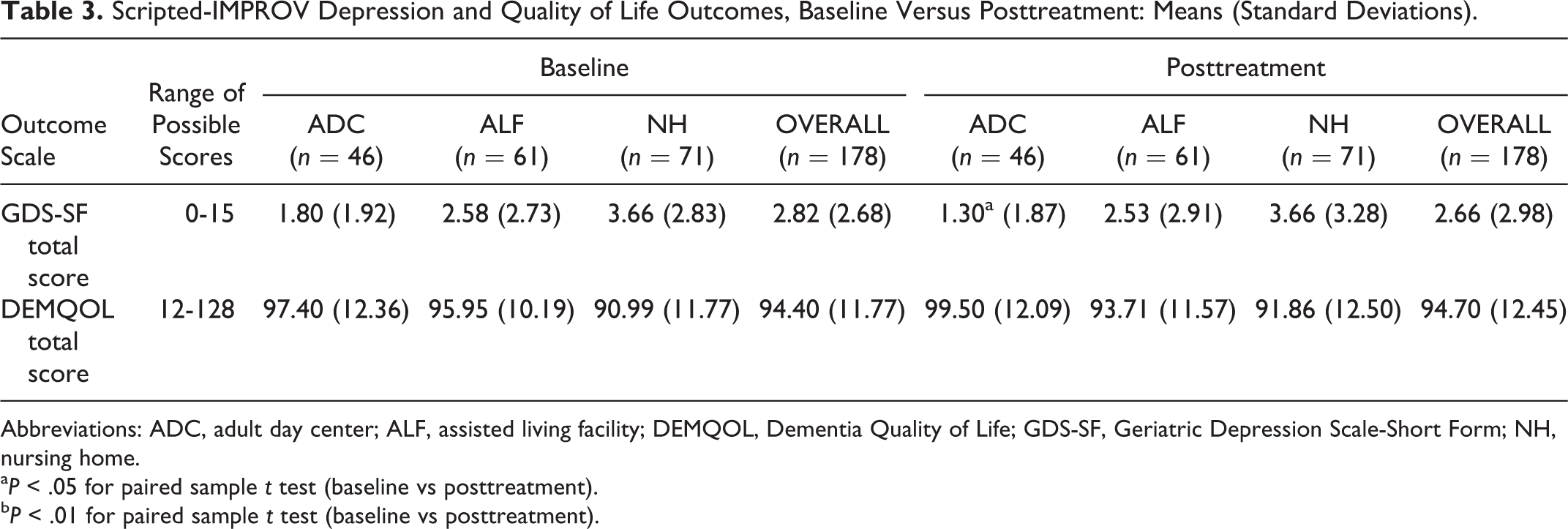
Abbreviations: ADC, adult day center; ALF, assisted living facility; DEMQOL, Dementia Quality of Life; GDS-SF, Geriatric Depression Scale-Short Form; NH, nursing home.
a P < .05 for paired sample t test (baseline vs posttreatment).
b P < .01 for paired sample t test (baseline vs posttreatment).
GDS-SF for Participants With Baseline GDS-SF ≥ 6. Baseline Versus Posttreatment.a,b.
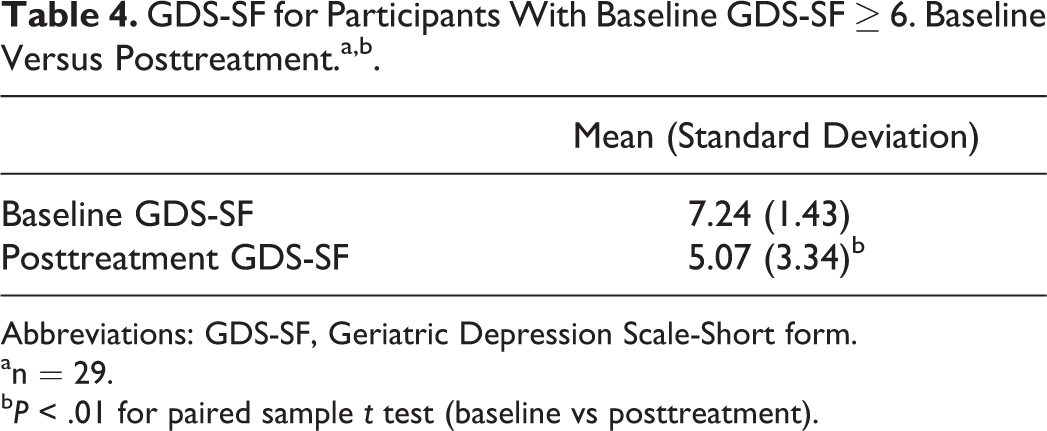
Abbreviations: GDS-SF, Geriatric Depression Scale-Short form. an = 29.
b P < .01 for paired sample t test (baseline vs posttreatment).
Characteristics of the Clinically Depressed Subsample.
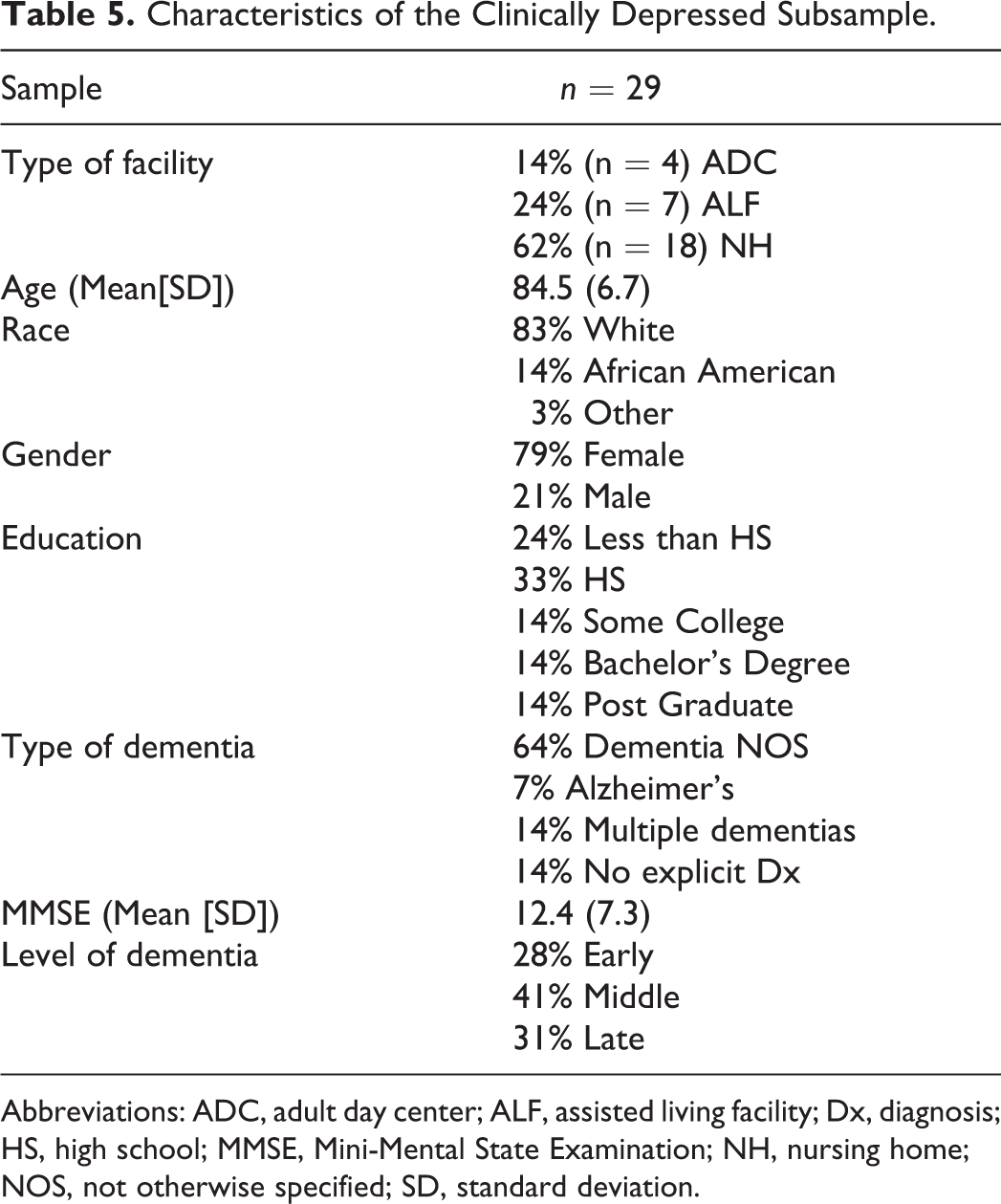
Abbreviations: ADC, adult day center; ALF, assisted living facility; Dx, diagnosis; HS, high school; MMSE, Mini-Mental State Examination; NH, nursing home; NOS, not otherwise specified; SD, standard deviation.
It is important to point out that most of the positive results (except for the changes in depression for the depressed subsample) were restricted to the time at which the intervention occurred. This is not necessarily surprising because the intervention was implemented only twice over the course of a one-week period.
Discussion
One goal of this study was to determine whether the Scripted-IMPROV intervention increased the levels of positive engagement/affect and reduced levels of negative engagement/affect in comparison with standard programming. With significant increases in CE, PE, and PL, and significant decreases in DE and NE, there is clear evidence that Scripted-IMPROV did produce these effects during the treatment period.
A second goal was to determine whether levels of engagement/affect produced by Scripted-IMPROV differed between the different site categories (NHs, ALFs, and ADCs). Although the sites differed significantly at baseline, there were only minor differences between sites at treatment—namely, PL was lower and NE was higher at ALFs during intervention, as compared to ADCs and NHs. However, ALFs did still see an increase in PL and a decrease in distracted engagement from baseline to treatment, which was in line with the trend observed at the other sites. The data, therefore, suggest that Scripted-IMPROV produced high levels of positive engagement/affect and low levels of negative engagement, which were somewhat dependent upon the site category.
A third goal of the study was to examine whether the intervention influenced depression and overall quality of life. Changes in depression for the overall sample were not detected, but for those participants who met the criteria for clinical depression at baseline, a reduction in depressive symptoms was observed at the postintervention period. A substantial increase in PL during the actual performances was not accompanied by significant changes in overall quality of life over time in any setting.
In sum, the results suggest that Scripted-IMPROV is an intervention which may be worthy of dissemination, as well as an intervention which is worthy of further research. The present observations indicate that the intervention seems to be effective across all dimensions examined in NH settings, in half of the MPES measures in ADC, and on two of the six MPES measures in ALFs. The MPES results appear to be independent of age and magnitude of dementia.
Returning to what the authors have termed the ERM, discussed at the beginning of this publication, the authors ask: does Scripted-IMPROV provide additional support for this model? The authors believe it does, because the negative behaviors that were relatively common at baseline (ie, NE and DE) were seemingly replaced by positive behaviors at treatment (ie, CE, PE, and PL) during Scripted-IMPROV programming.
An important unanswered question regarding the ERM is: Does an engaging program/intervention have a lasting impact on symptoms or only an immediate impact? If the effect is lasting, such interventions may be needed only intermittently. If the effect is immediate, such interventions must continuously be made available to PWD to meet the goal of reducing challenging behaviors. Data from the present study suggest that improvements in depression were not present initially, but emerged over time. However, there is no clear evidence that improved engagement/affect levels were sustained after the intervention had ended. This question of how often a “dose” of ecopsychosocial (nonpharmacological) intervention is needed has been asked by researchers examining ecopsychosocial interventions for many years.
It is evident that watching a comedic film can influence a person’s affect and mood while one is watching the movie. However, the PL derived from such an event does not necessarily last weeks or even days. No one critiques comedic films on this basis. Similarly, when someone takes a dose of simvastatin to maintain low cholesterol levels, it is accepted by patients that the effects only last 24 hours. So, one might argue that nonpharmacological interventions, just like a comedy film or a pill for cholesterol, cannot reasonably be expected to create long-term changes whether implemented infrequently and/or sporadically. To derive the full benefit of an ecopsychosocial intervention, it might be necessary for it to be implemented regularly over a long period of time.
There is, in fact, evidence that long-term, regular implementation of ecopsychosocial interventions is likely to have a lasting impact on participants. In a recently completed study of the Hearthside Book Club® intervention, participants took part in a specialized reading group four times per week for four weeks. 26 Participants exhibited a statistically significant increase in overall quality of life based on the DEMQOL, a reduction in apathy based on the Neuropsychiatric Inventory Nursing Home Version, 27 –29 and a reduction in symptoms of depression based on the GDS-SF. It remains to be determined whether these types of longer term results would have been observed in participants if they had participated in Scripted-IMPROV programming regularly for a long period of time. It is a question worthy of future research. In the interim, the authors have created a 70-page Scripted-IMPROV Drama Club Facilitation Guide, which provides descriptions and templates enabling staff to hold four full months of Scripted-IMPROV programming. This facilitation guide is currently being used by nonactors at various communities. Anecdotal evidence is promising; however, a formal research study has not yet been initiated.
Limitations and Directions for Future Research
One limitation of this study is its quasi-experimental design. Since the investigators did not use a control group, but rather compared intervention results to the same participant sample engaged in standard, regularly scheduled activities, it is possible that the results were due to the novelty of the intervention, rather than the specific nature of the intervention. Future research, using an alternative, novel intervention, conducted to explore this question in more detail might provide useful answers. Although the reduction in depressive symptoms is promising, it is possible that this outcome was caused by “regression to the mean.” 30 To examine the precise impact of Scripted-IMPROV on depression, a randomized controlled trial with only PWD who also had depression would be needed. Since researchers were not fully blinded to the study, it is possible that bias was introduced into data collection, despite the investigators’ best efforts to maintain objective data collection. In the authors’ view; however, some of the outcomes are so robust that it is unlikely that bias alone would account for the changes.
An additional limitation of the study relates to the outcomes we detected in relation to group size. Although the present data suggest that a large group size had a positive impact on engagement/affect, this was a post hoc analysis without any a priori prediction, and the present study does not have the statistical power to probe this result further with the study’s small group size. A separate study controlling for group size would be needed to determine the precise effect of group size on engagement and affect.
Barriers to Dissemination of the Intervention
Actors implemented the Scripted-IMPROV intervention in this study. However, the ultimate goal of the Scripted-IMPROV project is to enable nonactors such as facility staff to implement the intervention. To date, approximately 13 facilities have implemented the Scripted-IMPROV intervention. Feedback has been overwhelmingly positive. The greatest challenge experienced at the present time involves convincing sites/staff that they are capable of successfully implementing a program such as Scripted-IMPROV that involves “performance.” The investigators have identified a several barriers in the early stages of disseminating the intervention and various approaches which they have been using to overcome them.
First, implementing Scripted-IMPROV takes both staff time and energy. In order for staff to be willing to assign resources to the program, the effects of Scripted-IMPROV and the unique nature of the intervention must be understood by both facility staff and management. For this reason, the authors have created a brief staff in-service program that describes the key aspects of Scripted-IMPROV and provides an overview of some of the outcomes seen in this study.
Second, some staff have told the authors that “they are not actors” and “could never put on a play” with participants. A related concern is that some staff members are afraid even to attempt to act. To address this concern, the authors have created a training program that attempts to motivate staff and help the staff observe that nonactors are capable of putting on a Scripted-IMPROV play, even though the staff may believe they cannot. The authors have also posted video clips of nonactors implementing Scripted-IMPROV on their website, so that prospective Scripted-IMPROV staff members can see other nonactors succeeding. Finally, as noted previously, the authors created a 70-page facilitation guide, which can assist staff to gradually prepare for a performance, so they can over time become accustomed to acting in front of their clients and residents.
Third, many staff are extremely fearful of needing to memorize lines for a performance. To allay this concern, the authors initially remind staff that there is no need to memorize lines, given the semi-improvisational nature of the intervention. The authors emphasize in the training that the “Yes, and…” improvisation principle allows the staff member to take whatever a client says or does and run with it—without the need to follow the script precisely. In addition, the authors created “cheat sheets” for staff who would like to be reminded of key plot points around which to improvise—cards with the main actions stated briefly rather than as whole parts to learn. For staff members who like the idea of using the sample dialogue in the full scripts, we tell them that it is completely fine to do a rehearsal while holding the script or even hide their script inside a prop their character carries around. The important point is getting the staff members in front of participants and having fun with the intervention.
In the future, the authors plan to continue to develop additional Scripted-IMPROV content, including additional scripts, training programs, and facilitation guides. The goal is to amass a legion of brave staff members, volunteers, and family members who are excited to engage participants in meaningful semi-improvisational drama performances.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Institutes of Health / National Institute on Aging: Project #5 R44 AG035404 (Zeisel, Principal Investigator).