
Abstract
Background:
Older adults with Alzheimer’s disease (AD) may be unable to perform treadmill testing due to balance issues. We investigated whether older adults with AD could successfully complete a peak cycle ergometer test.
Methods:
Peak oxygen consumption (peak
Results:
All participants completed the cycle ergometer test successfully. Peak
Conclusion:
Older adults with AD are able to safely complete a peak cycle ergometer exercise testing protocol. We provide an individualized cycle ergometer test for determining aerobic capacity in older adults with AD who may be unable to perform treadmill testing due to balance or gait issues.
Introduction
Aerobic exercise and aerobic capacity have been associated with improved or maintained brain structure and cognitive function in healthy individuals and in people with mild cognitive impairment.
1
-5
Recent studies found associations between aerobic capacity and cognitive and cerebral structural changes in persons with Alzheimer’s disease (AD) as well, suggesting that aerobic exercise training may play a therapeutic role in AD through biologically sound pathways, although this remains to be fully elucidated.
6,7
However, the current understanding of aerobic capacity in persons with AD is limited to a few studies that have investigated peak oxygen consumption (
Methods
Of the first 57 participants who completed all screening tests in the FIT-AD trial, 44 who met the eligibility criteria were included for this study. The FIT-AD trial is an ongoing exercise intervention study that aims to enroll a total of 90 participants and its protocol and inclusion/exclusion criteria have previously been described in detail. 17 Briefly, English-speaking older (>66 years) community-dwelling adults with diagnosed mild to moderate AD (defined as 0.5-2 on the Clinical Dementia Rating [CDR] scale and a score of 15-26 on the Mini-Mental State Examination [MMSE]) were enrolled in the study. Participants were recruited via a variety of methods including mailings, advertisements, and clinical referrals. Potential participants who have a resting heart rate of <50 or >100 beats/min, cardiac ischemia, significant arrhythmias, neurological/psychiatric disorders other than AD, chemical dependency, inability to cycle, or any contraindications to exercise per American College of Sports Medicine (ACSM) guidelines were excluded. 18 This study was approved by the local university’s institutional review board, and informed consent or surrogate consent/participant assent was obtained during an in-person screening visit. All testing procedures took place at the University’s Clinical Translational Science Institute and the School of Nursing Laboratory of Clinical Physiology.
Outcome Variables and Their Measures
All assessors were trained and certified by the investigators. The training included 3 months of readings, lectures, demonstration testing, practice testing, and supervised test runs with the initial participants. All assessors participated in ongoing training to maintain proper procedures. Fidelity checks were conducted on a regular basis and assessors were briefed and debriefed to ensure compliance with the study protocol. All peak exercise testing was conducted by a team that consisted of a trained exercise technician, study staff, and a physician coinvestigator. All physical function tests were conducted by trained research staff.
Aerobic capacity and fitness levels were measured by a peak cycle ergometer test, the incremental shuttle walk test (ISWT),
19
and the 6-minute walk test.
20
Peak cycle ergometer test: Participants began pedaling at a speed comfortable to them (40-60 rpm). The intensity of cycling was then increased every 3 minutes by increasing the watt to achieve an increase in energy expenditure of 1 metabolic equivalent (MET; 1 MET = 3.5 mL oxygen/kg body weight/minute: estimated resting oxygen consumption). The Borg rating of perceived exertion (RPE) was used to assess the perceived level of exercise exertion based on participant’s report during the last minute of each stage and at peak exercise. The participants continued to exercise until meeting one of the predefined stopping criteria or reaching volitional fatigue/asked to stop or had symptoms that indicated test termination as outlined by the ACSM.
18
The predefined stopping criteria were: (a) inability to maintain the required 40 to 60 rpm with increasing exercise intensity above ventilatory threshold; (b) achieving an RPE (Borg RPE) of ≥17/20; or (c) no increase in oxygen consumption or heart rate with increasing exercise intensity. The test was performed in the postabsorptive state with no tobacco or caffeinated beverages in the previous 8 hours. Heart rate and blood pressure were assessed at rest, during the last minute of each stage, at peak exercise, immediately after cessation of exercise, and every 3 minutes until return to baseline levels. Heart rhythm was continuously monitored via electrocardiogram. Expired gases were measured continuously by mouthpiece and nose clip using breath-by-breath analysis averaged by 5 to 7 seconds. The metabolic cart was calibrated prior to each testing session using known precision calibration gases according to manufacturer’s instruction. Peak oxygen consumption was defined as the median oxygen consumption during the last 30 seconds before cessation of exercise. Outcome variables of interest obtained from the cycle ergometer tests were peak
Shuttle walk test, an externally paced incremental test that stresses participants to peak performance, was conducted as following: Participants walked a circuit around a pair of markers placed 9 m apart while being paced by a recording of beeps. The participant had to arrive from one marker to another marker at the time of the beep (1 shuttle). Failure to arrive at a marker by the time of the beep 2 consecutive times marked the end of the test. Verbal cues “stop” and “walk” were given to coincide with the beeps. The distance walked in meters was considered the outcome variable. 19
The 6-minute walk test was conducted according to standard guidelines. The distance covered in 6 minutes a walking speed intended to cover as much distance as possible was the used as the outcome variable. The distance walked in meters was considered the outcome variable. The 6-minute walk test has a reported 0.58 to 0.96 validity and 0.65 to 0.92 reliability.
20
We have previously tested the symptom-limited peak cycle ergometer test without measuring
Physical function was measured by the Short Physical Performance Battery (SPPB), which has 3 subscales: balance, gait speed, and sit to stand (each scored 0-4) with a sum score of 0 to 12 (higher score = better performance). The test–retest and interrater reliabilities are both >.90 in older adults. 23 The subscores and total scores on the SPPB were considered the outcome variables of interests in this study.
The AD stage was assessed using the CDR during the in-person interview. The AD stage was used as a measure of dementia severity.
Cognition was measured using the MMSE. The MMSE assesses orientation, memory, recall, constructional praxia, and language with a total score of 30. Higher score indicates better global cognition. The MMSE has a reliability of .98. 24
Demographics of interest included age, gender, race, education level, comorbidities, and anthropometrics since these covariates have been linked to exercise capacity.
Statistical Analysis
Continuous variables were summarized by means and standard deviations (SDs) and categorical variables were summarized by frequency and percentage and were used to describe the sample. Pearson bivariate correlation was used to assess simple association between variables for the entire sample. Correlational analyses for CDR were conducted by point biserial correlation due to low distribution (see “Results” section). One participant, an avid cyclist, achieved a substantially higher
Results
Demographics are presented in Table 1. Of the 59 participants screened in person, 10 participants were excluded and referred for evaluation due to abnormal stress test response and 3 were further excluded due to not meeting the AD criteria on magnetic resonance imaging (also known as having a non-AD dementia) and 2 were excluded due to an inability to bend the knees. The final sample consisted of 44 participants (mean age 78.4 [SD 6.8], 55% male, 98% white), with a CDR range of 0.5 to 2 and a mean MMSE score of 21.6 (SD 3.3). The CDR 0.5 (n = 19), CDR 1 (n = 24), and CDR 2 (n = 1) are considered mild–moderate AD, and the majority of the sample was treated pharmaceutically for AD (70.5%).
Demographics and Health Characteristics.
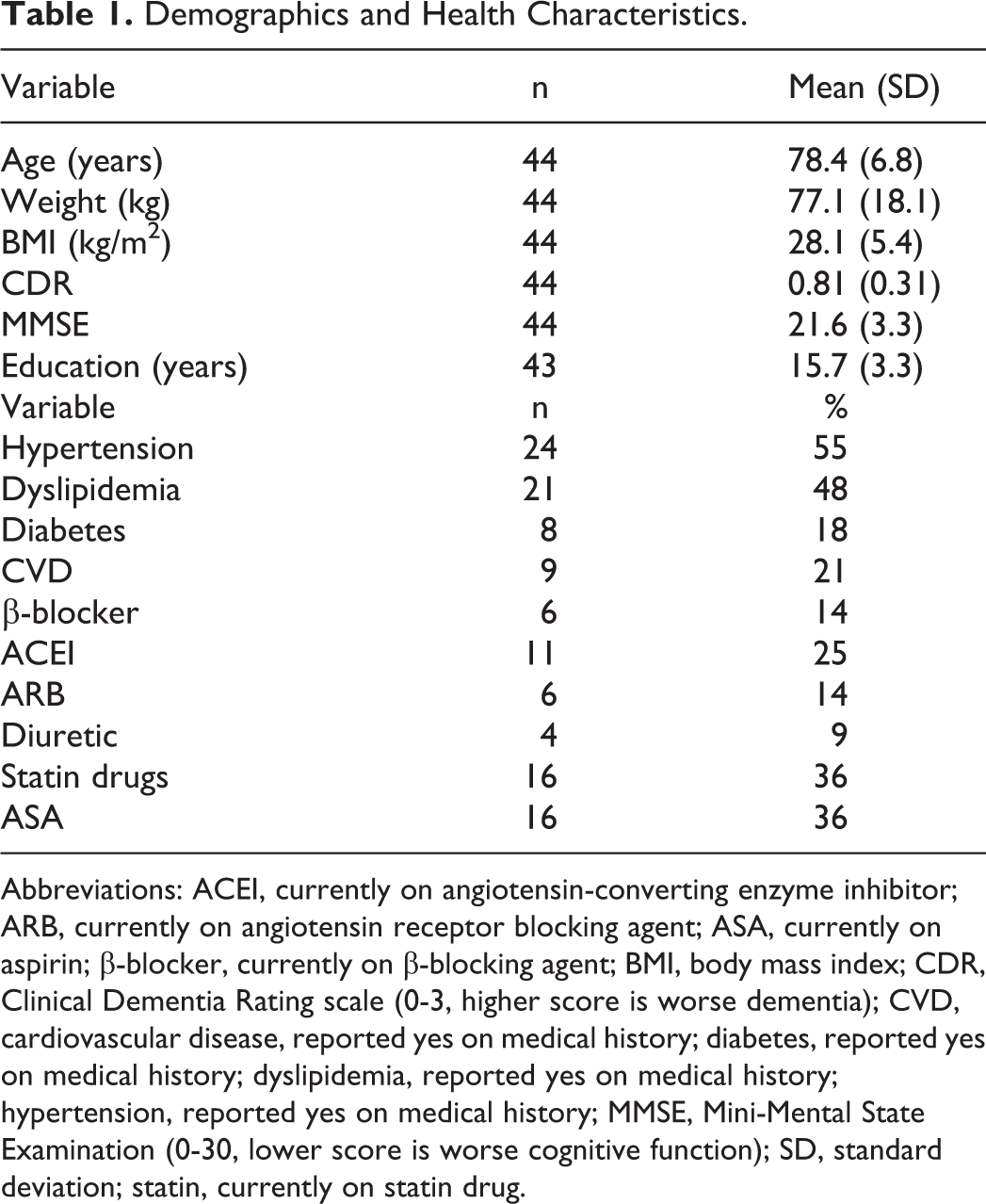
Abbreviations: ACEI, currently on angiotensin-converting enzyme inhibitor; ARB, currently on angiotensin receptor blocking agent; ASA, currently on aspirin; β-blocker, currently on β-blocking agent; BMI, body mass index; CDR, Clinical Dementia Rating scale (0-3, higher score is worse dementia); CVD, cardiovascular disease, reported yes on medical history; diabetes, reported yes on medical history; dyslipidemia, reported yes on medical history; hypertension, reported yes on medical history; MMSE, Mini-Mental State Examination (0-30, lower score is worse cognitive function); SD, standard deviation; statin, currently on statin drug.
Success of Cycle Ergometer Test Completion
There were no unanticipated adverse events related to exercise testing procedures. We were unable to obtain
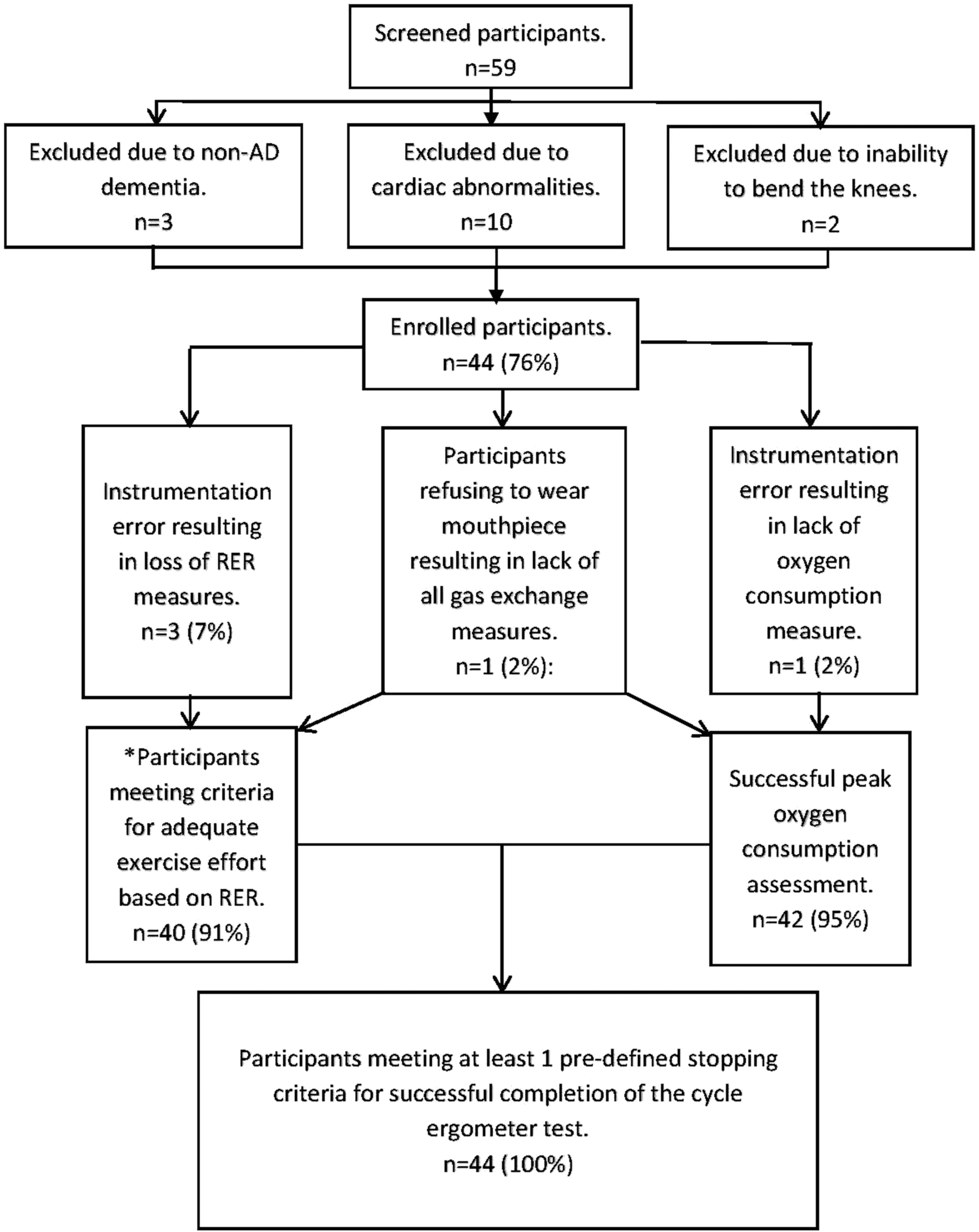
Flow diagram of success rate of the cycle ergometer test. *All participants with reliable respiratory gas exchange measures were able to reach adequate work effort for determining
Descriptives of Exercise Capacity and Physical Function Measures
The mean aerobic capacity (peak
Physical Fitness and Physical Functioning Measures.a
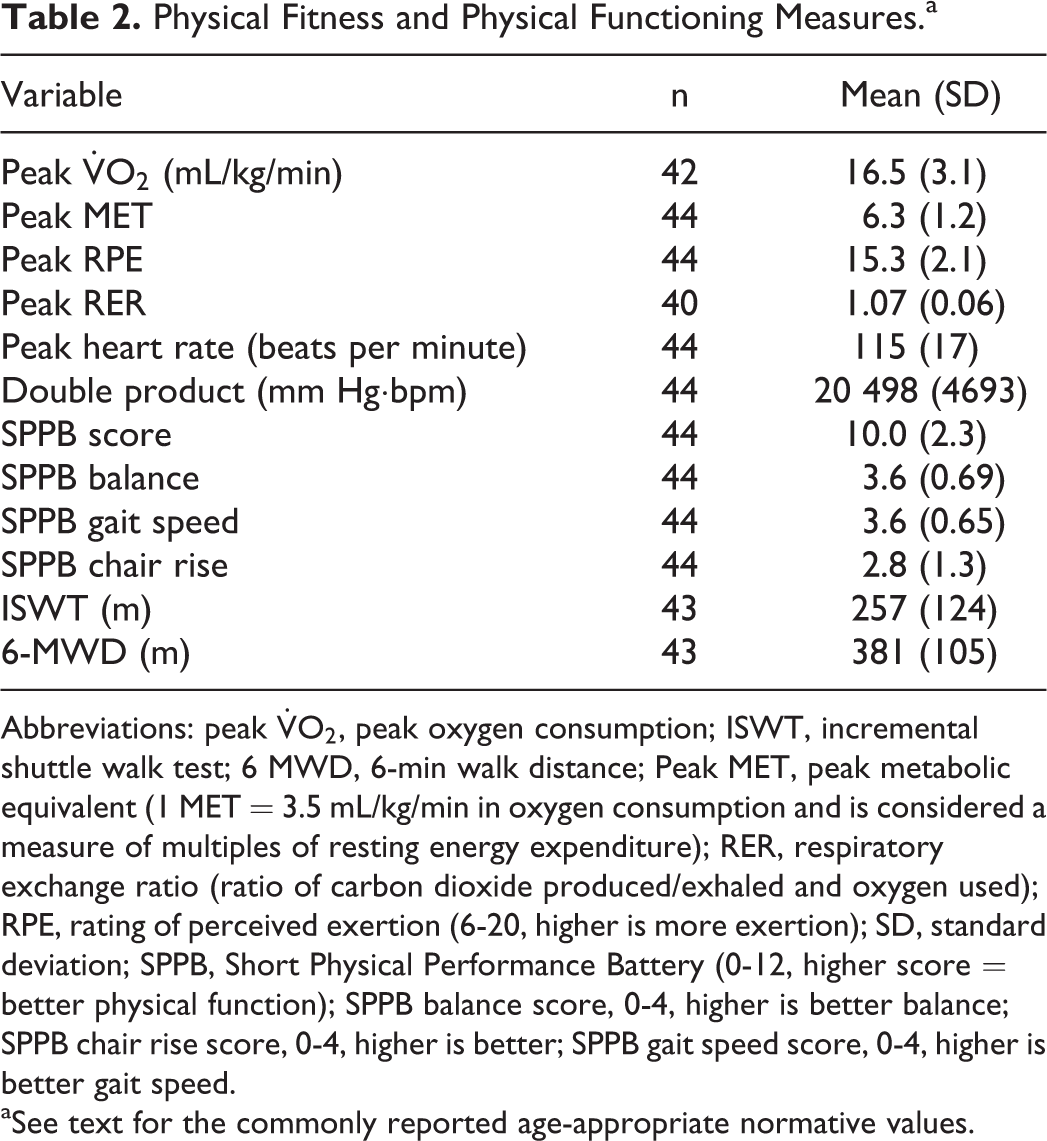
Abbreviations: peak
aSee text for the commonly reported age-appropriate normative values.
Associations of Aerobic Capacity With Physical Functioning and Cognitive Functioning
Peak
Correlational Analyses.
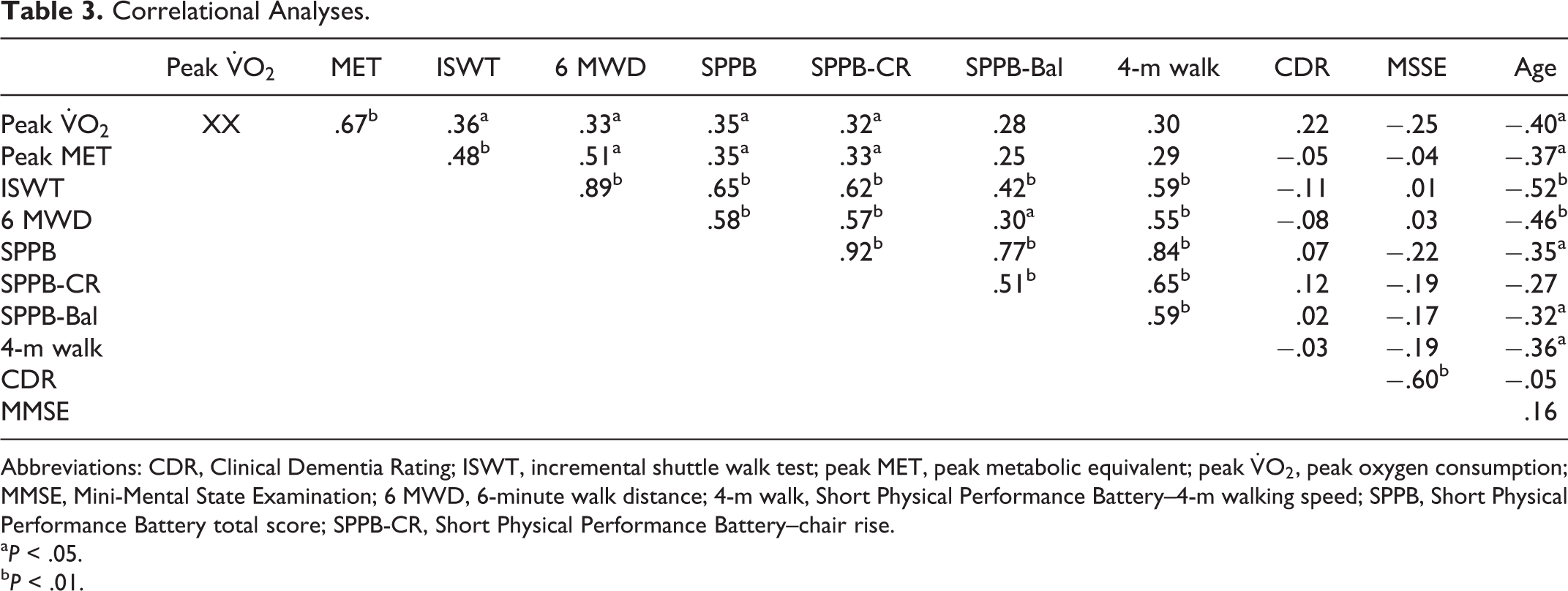
Abbreviations: CDR, Clinical Dementia Rating; ISWT, incremental shuttle walk test; peak MET, peak metabolic equivalent; peak
a P < .05.
b P < .01.
Associations between aerobic capacity and physical function measures are presented in Table 3. The SPPB score was inversely correlated with age and strongly correlated with peak heart rate during the cycle ergometer exercise test, shuttle walk distance, and 6 MWD. The shuttle walk distance was inversely correlated with age, moderately correlated with peak MET achieved during the cycle ergometer exercise test, and strongly correlated with 6 MWD. The 6 MWD correlated moderately with peak MET achieved during the cycle ergometer exercise test and inversely correlated with age. Age remained the only variable that consistently correlated with physical functioning variables and aerobic capacity, with the exception for the SPPB subscale score on chair rise.
Correlational analyses between aerobic capacity and AD severity and cognition indicated no significant correlations for the entire sample (Table 3). The CDR score was inversely correlated with peak RPE (r = −.32, P = .035). Analysis controlling for age did not change outcomes between AD severity, cognitive function measures, and physical function and fitness variables.
Participants with a
Demographics of Participants With a Peak
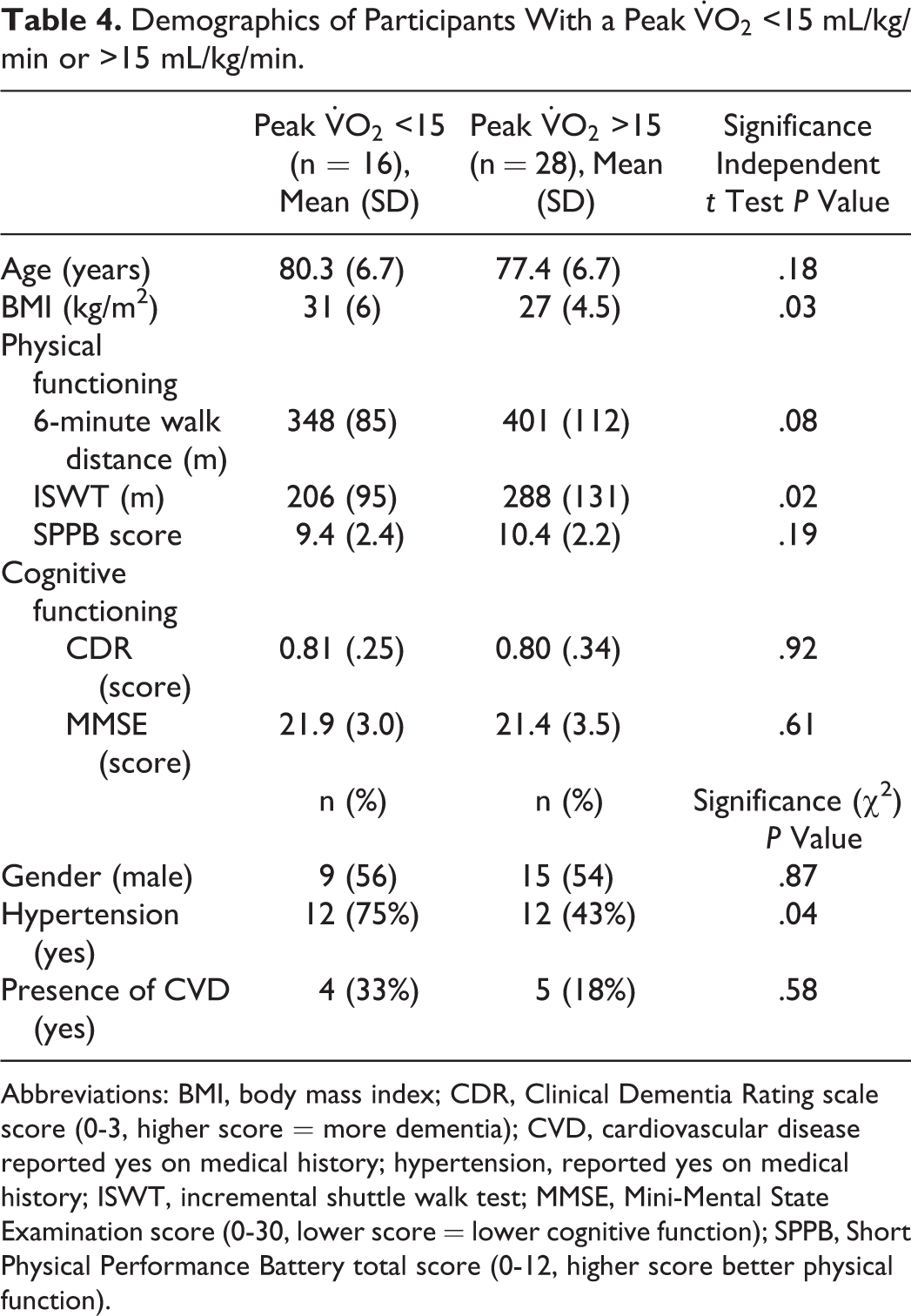
Abbreviations: BMI, body mass index; CDR, Clinical Dementia Rating scale score (0-3, higher score = more dementia); CVD, cardiovascular disease reported yes on medical history; hypertension, reported yes on medical history; ISWT, incremental shuttle walk test; MMSE, Mini-Mental State Examination score (0-30, lower score = lower cognitive function); SPPB, Short Physical Performance Battery total score (0-12, higher score better physical function).
Discussion
The results demonstrate that older adults with mild to moderate AD can successfully and safely perform a peak cycle ergometer test for determination of peak aerobic capacity, shuttle walk test, 6-minute walk test, and the SPPB. All participants (100%) met at least one of the predefined stopping criteria for successful completion of the test. This finding meets our consensus a priori criteria that at least 80% of enrolled participants would be able to successfully complete the cycle ergometer test. All participants with reliable respiratory gas exchange measures were able to reach an RER of >1.0, suggesting that adequate work effort was reached for determining
We also experienced an unanticipated problem with participants’ range of motion preventing them from completing a full revolution, related to participants being poststatus total knee replacement and an inability to keep feet firmly on the pedal and in the pedal straps. We addressed this problem by allowing slower rpms (40 rpm) than initially anticipated and adjusting the cycle ergometer to allow for less than optimal knee flexion and by adjusting the pedal straps to allow unusually large footwear and ankle angles to fit securely in the pedal straps.
18
Despite these adjustments, we were unable to test 2 participants due to an inability to perform sufficient knee flexion to allow for cycle ergometer testing or training; these participants were subsequently excluded from the study and not counted as part of the study sample. Our findings that people with AD can safely and successfully perform the SPPB, 6-minute walk test, and the ISWT are supportive of previous reports. However, to our knowledge, this is the first study that have compared peak
Aerobic capacity and physical function in our study sample were all below age- and sex-matched normative levels, suggesting that older adults with AD have reduced physical fitness levels contributing to early loss of independence. 28 -30 Normative values at the study sample mean age of 78 are commonly considered to be 514 m on the 6-minute walk test, with the 10th percentile reported at approximately 334 to 361 m. 28,29 The 25th percentile is commonly reported as <430 for women and <470 for men. 29 Importantly, any score lower than the 25th percentile is considered as low functioning status. 18 Our mean 6-minute walk test was substantially lower than the 25th percentile, suggesting low physical functioning status with only 17% of men and 40% of women scoring over the 25th percentile. The normative values for the ISWT in healthy adults over age 70 has been reported to be 633 m. 30 The mean of our sample was 59% below the ISWT normative value, with all participants scoring well below the normative value of 633 m, further underscoring the reduction in the physical fitness levels in older adults with AD. Moreover, 36% of the study sample scored <10 on the SPPB and would be considered at moderate risk of functional disability. 31,32 However, the range of SPPB scores was large with participants ranging from a score of 4 to 12 (total score possible = 12), suggesting that physical functioning varies substantially in this population and according to our data is mostly related to age. The SPPB scores were similar to the Finnish Alzheimer disease exercise trial (FINALEX) study. 33
Aerobic capacity that is adequate to allow individuals to perform ADLs is essential to maintain independence. A large subgroup (37%) of older AD patients were not able to achieve a cardiorespiratory fitness level above the minimum of 15 mL/kg/min required for maintenance of independent ADLs, suggesting that more effort should be placed on maintaining physical fitness levels via exercise training.
25
Moreover, only 15% of participants were able to achieve a peak
The significant correlations between aerobic capacity and physical function suggest that the SPPB, 6-minute walk test, and the shuttle walk may be useful in identifying individuals who have low aerobic capacity in a clinical setting. Determination of
Contrary to our hypothesis, there were no significant correlations between aerobic capacity and cognition, possibly due to the small sample size and limited range of AD severity. Our findings are in support of previous studies that have shown no correlations between cardiorespiratory fitness and CDR.
1,2
However, other studies have indicated a moderate correlation between cognitive function measures, brain structure, and aerobic capacity in healthy persons and persons with AD.
1,3,5,36,37
One possible explanation of our finding may be related to the use of a cycle ergometer test instead of treadmill testing. Treadmill testing is known to result in higher
The observation of a significant correlation between peak MET level and CDR in the low fitness group suggests that the association between AD severity and aerobic capacity may not become apparent until aerobic capacity has deteriorated below levels required for meaningful work to be performed. This is in support of previous studies that suggest that aerobic capacity is related to cognitive function and that an increase in physical fitness levels may moderate age-related brain changes and possible AD-related brain changes, the so-called cardiorespiratory fitness hypothesis. 36,38,39 It is also possible that people with AD subconsciously reduce usual physical activity levels, which results in lower aerobic capacity and physical fitness levels. This in turn increases the risk of frailty and loss of independence. The results from this study do not support this hypothesis for the entire sample, but rather only in the low fitness sample. It is also plausible that patients with AD are unwilling to reach uncomfortable levels of effort and thereby artificially reduce peak aerobic capacity levels. A large group of participants in this study did not reach a peak RPE >15 (n = 11), and we observed a moderate correlation with RPE and AD severity as measured by CDR score. This suggests that AD severity may affect peak testing outcomes due to apathy or an inability or unwillingness to perform exercise at an uncomfortable effort level or an inability to cognitively understand peak effort. 40 This finding is different from Burns et al who did not find a correlation between RPE and dementia. 1 This difference was likely due to our study sample having a larger range of AD severity and included participants with more severe AD. Researchers should take these considerations into account when designing exercise testing and training programs 40 and possibly use criteria other than RPE for determination of exercise intensity (eg, heart rate or metronome pacing).
Although much research is needed, there is evidence suggesting that the AD disease process follows a biological pathway (the biological hypothesis) that contributes to a reduction in aerobic capacity. Specifically, there appears to be a reduction in both peripheral and central mitochondrial capacity in AD, which may result in low aerobic capacity. 41 Moreover, animal and human studies have shown that an increase in fitness levels leads to enhanced survival of brain neurons following neuronal insults and that exercise training increases brain vascularization and growth factors and thereby stimulates hippocampal and cortical neurogenesis as reviewed by Paillard et al 6 and Bherer et al 42 Future studies should focus on these areas of research.
Strength and Limitations
We enrolled a sample consisting of older adults with AD that has been largely neglected in the majority of published AD studies and we introduced a battery of testing procedures not performed in previous studies in order to fully investigate aerobic capacity and physical function in this population. We present the first study comparing peak
Conclusions
This is the first study to our knowledge that have investigated
Footnotes
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Institutes of Health National Institute on Aging award number R01AG043392 (Yu). Trials registration (NCT01954550). The CTSI were supported by the National Institutes of Health National Center for Advancing Translational Sciences (UL1TR000114).