
Abstract
Diogenes syndrome refers to the combination of extreme self-neglect and excessive collecting with clutter and squalor, which is often present in patients with dementia. Diogenes syndrome may be particularly common in behavioral variant frontotemporal dementia (bvFTD), and the investigation of these patients may help clarify the nature of this syndrome. We describe 5 patients with bvFTD who exhibited a decline in self-care accompanied by hoarding behaviors. These patients, and a review of the literature, suggest a combination of frontal lobe disturbances: loss of insight or self-awareness with a failure to clean up or discard, a general compulsive drive, and an innate impulse to take environmental items. This impulse may be part of the environmental dependency syndrome in frontal disease, with specific involvement of a right frontolimbic–striatal system. Further investigation of the similarities and mechanisms of these symptoms in bvFTD could help in understanding Diogenes syndrome and lead to potential treatment options.
Introduction
Definition
Diogenes syndrome refers to the unique combination of severe self-neglect and excessive hoarding, often in the context of dementia. 1 Originally named for the Greek philosopher and cynic who chose to live in squalor as a rejection of the outside world, 2,3 Diogenes syndrome is accompanied by a lack of concern or awareness of their condition, a disheveled appearance, disregard of house and living environment, and overt clutter and disorganization. 4 Although the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), isolates hoarding disorder (“syllogomania”) as a distinct condition, 5 DSM-5 does acknowledge a potential association between self-neglect and hoarding behavior. 6
Clinical Features
Researchers have described Diogenes syndrome, previously referred to as “senile” or social breakdown 7,8 or “senile squalor,” 4 as occurring predominantly in older adults who live alone and who may have a detached or suspicious personality and a cognitive decline. 7 Diogenes syndrome has no clear socioeconomic or gender difference 3,9,10 and can occur in couples as “Diogenes à deux.” 4 Because individuals with this syndrome do not recognize their behavior as problematic, they are unlikely to seek help unless they require immediate medical attention or are referred by a neighbor or family member. 1,9 Hence, Diogenes syndrome is a serious condition with reported mortality rates of 47% to 50% within 1 to 4 years of diagnosis. 7 -9
The existence of a primary Diogenes syndrome is probably rare. In at least two-thirds of cases, Diogenes syndrome is associated with a comorbid neuropsychiatric condition. 3,10 Although secondary Diogenes syndrome occurs with obsessive-compulsive disorder, depressive or bipolar disorders, schizophrenia, personality disorders, and alcohol abuse, 1 -3 it is particularly associated with dementia. One report found Diogenes syndrome in about 15% of older adults with dementia, 11 and another describes clinical hoarding behavior, frequently associated with self-neglect, among 23% of patients with moderate or severe dementia. 12 Among the dementias, Diogenes syndrome may have a special relationship with behavioral variant frontotemporal dementia (bvFTD), 2 where it occurs in about 36% of patients. 13 Behavioral variant frontotemporal dementia involves medial “frontolimbic” and related areas and commonly presents with behavioral changes. 14 The International Consensus Criteria for bvFTD include 3 of the following: behavioral disinhibition; apathy or inertia; loss of sympathy or empathy; early perseverative, stereotypical, or compulsive/ritualistic behavior; hyperorality and dietary changes; and a neuropsychological profile with deficits in executive tasks and relative sparing of episodic memory and visuospatial skills. 15 These criteria for bvFTD encompass the essential elements of Diogenes syndrome: compulsive-like behaviors and the neglect of personal hygiene. 14,16
Diogenes and Frontotemporal Dementia
Behavioral variant frontotemporal dementia may offer a unique window into the neurobiological mechanisms for Diogenes syndrome. 3 The unique combination of behavioral symptoms of bvFTD may predispose to a high likelihood of developing Diogenes syndrome, suggesting that clinicians need to consider bvFTD when this syndrome occurs in middle or late life. We report and examine 5 patients with bvFTD and Diogenes syndrome, review the literature on this relationship, and discuss the potential insights to this syndrome afforded by patients with bvFTD. This study is part of an institutional review board approval from the David Geffen School of Medicine at the University of California at Los Angeles.
Case Presentation
Case 1
Initial presentation
A 48-year-old left-handed man presented with a 3-year history of a progressive personality change. It started with difficulty completing his work, following through on complex activities, managing his money, and initiating and maintaining positive productive interactions. The patient also exhibited disinhibited behavior, saying inappropriate things and touching others inappropriately. He became disheveled in his personal appearance and in the upkeep of his home, which was extremely disordered and cluttered from compulsive hoarding. He had amassed stacks of things, such as magazines, heaps of mail, and other items that he had previously deemed of value (See Table 1). Every surface in his home was covered with these items. He did not have insight into his hoarding behavior as a problem nor did he object to being prevented from accumulating items. He had other compulsive behaviors and repetitive pacing back and forth, as well as dietary changes including ice cream at breakfast and lunch, daily peanut butter and jelly sandwiches, and meat tacos (formerly a vegetarian).
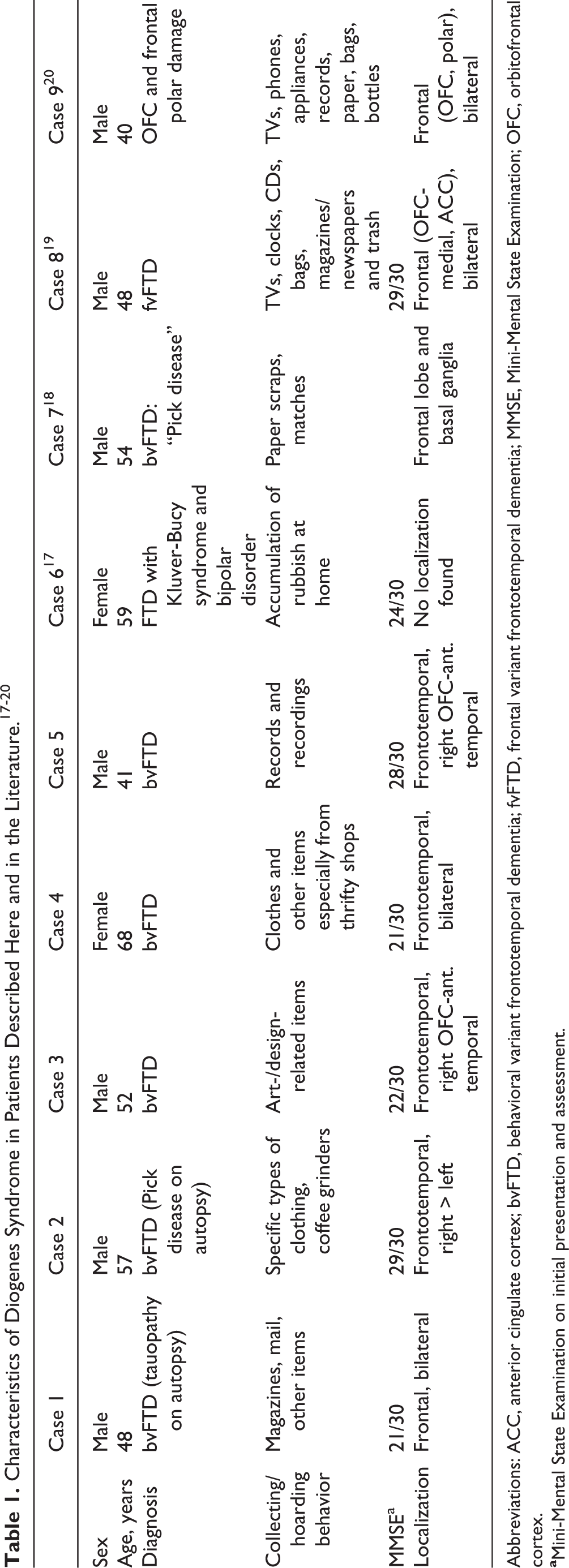
Abbreviations: ACC, anterior cingulate cortex; bvFTD, behavioral variant frontotemporal dementia; fvFTD, frontal variant frontotemporal dementia; MMSE, Mini-Mental State Examination; OFC, orbitofrontal cortex.
Cognitive evaluation
On examination, he sat quietly with little spontaneous verbal or physical activity and a flat affect. He was stimulus-bound on testing, did poorly on several frontal bedside tasks, but did not have utilization (tendency to use items within grasp) or imitation (tendency to mimic another’s actions) behaviors associated with frontal disease. He had neuropsychological testing which showed executive dysfunction including impulsivity and disorganization. Magnetic resonance imaging showed significant bifrontal encephalomalacia, and positron emission tomography (PET) of the brain showed bifrontal hypometabolism consistent with bvFTD.
Treatment, diagnosis, and outcome
His hoarding behavior did not respond to gabapentin (300 mg twice a day), bupropion (75 mg every day), aripiprazole (5 mg every day), lithium (300 mg twice a day), or memantine (10 mg twice a day). The patient eventually died, and autopsy was consistent with bvFTD with τ-immunoreactive neurons and astrocytes within frontal and temporal neocortex. There was no identified hereditary source for his tauopathy.
Case 2
Initial presentation
A 57-year-old right-handed man presented with a 3-year history of progressive behavioral changes. He had become disinhibited, saying or doing things that were inappropriate and demonstrating excessive familiarity with strangers. Without invitation, he would walk into his coworkers’ offices and defrag their computers and walk into a neighbor’s home and play their piano. He lost his job when he spontaneously blurting out that the workplace was “god-awful.” He also had a significant decline in his hygiene, claiming that it was not a problem. At 1 point, he was said to not have bathed for at least 6 weeks until he was asked to do so, and his response was that it was not necessary because he never had body odor. He developed new and prominent hoarding behavior, collecting items that he was known to value, such as dozens of coffee grinders and Hawaiian shirts, which accumulated in his home. Further changes included prominent compulsive behavior along with dietary changes where he would eat the exact same fast foods over and over again.
Cognitive evaluation and neuroimaging
On examination, he showed no insight into his disease or behavioral changes. There was no utilization behavior although he tended to echo the examiner’s comments. The rest of the neurologic examination was normal. Neuropsychological testing found executive deficits and decreased memory retrieval. Magnetic resonance imaging and PET imaging confirmed the presence of asymmetric frontotemporal atrophy, severe in frontal lobes and moderate in temporal lobes, affecting the right more than the left side.
Treatment, diagnosis, and outcome
During the course of his illness, several medications were tried with possible effects of sertraline (150 mg every day) in decreasing his collecting behavior. The patient eventually died, and his autopsy showed τ-positive Pick bodies consistent with bvFTD. There was no evidence of a genetic form of bvFTD.
Case 3
Initial presentation
A 52-year-old right-handed man presented with a 4-year decline in overall function and ability to understand instructions at work, leading to his dismissal. He had become disengaged and withdrawn from his usual activities of interest. His wife complained that he was no longer affectionate or concerned about her feelings and those of their children. Further history indicated a significant decline in self-care and hygiene involving dressing, grooming, and his environment, coupled with a paradoxical compulsion to shower. Indulging a long-standing appreciation of art, he became consumed with collecting and accumulating art and design-related items, frequently actively searching for these items in stores. This was coupled with the compulsion to check out every art-related store or second-hand store in the vicinity. The patient developed other compulsive-like behaviors and became fixated on eating only fish.
Cognitive evaluation and neuroimaging
On examination, he was detached during the interview and denied that anything was wrong with him. There was no utilization or imitation behavior and the rest of his neurological examination was normal. Neuropsychological testing showed executive deficits, decreased verbal fluency and disturbed memory, but spared visuospatial functions. Magnetic resonance imaging showed cerebral atrophy possibly more prominent in the frontotemporal regions, and PET confirmed bifrontal and right orbitofrontal cortex (OFC)-anterior temporal hypometabolism.
Diagnosis and outcome
His collecting and compulsive behaviors subsided as the disease progressed without drug intervention. There was no evidence of a genetic form of bvFTD, and the family declined autopsy on his death.
Case 4
Initial presentation
A 68-year-old right-handed woman with 12 years of education presented with a 5-year history of personality changes. She appeared to lose interest in everything, including self-care and paying her bills, and she became impulsive and disinhibited, at 1 point approaching overweight people and telling them that they were fat. The patient, who had previously enjoyed dressing well, began hoarding clothes, often compulsively going to thrifty shops to make multiple clothing purchases that she did not need. Despite an accumulation of clothes, the patient appeared poorly groomed and unkempt, and her living environment was cluttered and in disarray. She had other compulsive-like behaviors, such as going into the bathroom and repeatedly folding and unfolding toilet paper. She had a change in her dietary habits and would eat everything that was put in front of her.
Cognitive evaluation and neuroimaging
On examination, the patient was alert and cooperative. Her insight was limited because she denied any change in her behavior or personality when questioned. The patient had difficulty on memory and executive tasks, and her neurological examination was remarkable for a frontal grasp reflex, stereotypical movements, and akathisia-like restlessness. Magnetic resonance imaging showed frontotemporal atrophy, and PET showed frontotemporal hypometabolism.
Treatment, diagnosis, and outcome
The family history was negative for a familial bvFTD, and the family declined genetic testing. She was tried on multiple medications at different times by multiple providers (sertraline 200 mg every day, quetiapine 25 to 50 mg every day, lorazepam 0.5 mg, divalproex 250 mg twice a day, propranolol 10 mg twice a day, and risperidone 5 mg) without clear benefit of her compulsive-like behaviors.
Case 5
Initial presentation
A 41-year-old right-handed man had a 3-year history of an insidiously progressive change in his personality. He had a decline in his ability to follow-through on tasks and activities, yet he became very disinhibited, often making personal-referent comments to others and incessantly commenting and joking. His self-care declined prompting the need for his wife to remind him to maintain his hygiene and environment. A lover of music, he developed collecting behavior focused on old recordings, despite the fact that he would ignore them once collected. His wife had no trouble removing the accumulated items before it resulted in too much clutter. Additionally, the patient compulsively watched certain television shows, listened to specific radio programs, and became obsessed with eating carbohydrates. In general, he lacked insight regarding his illness and changes in behavior. The patient’s medical history and family history were negative for similar disease or behavioral changes.
Cognitive evaluation and neuroimaging
On examination, he continued to intrude comments and jokes. There was no utilization or imitation behavior or frontal grasp reflex. The rest of his examination showed executive deficits, including on neuropsychological testing, and a normal neurological examination. Magnetic resonance imaging showed bifrontal and right temporal volume loss, and PET had frontotemporal hypometabolism greater in right OFC-anterior temporal area.
Diagnosis and treatment
Sertraline (200 mg every day) had some effect in decreasing his compulsive-like behaviors.
Discussion and Conclusion
The spectrum of Diogenes syndrome in our bvFTD patients included a decline in self-awareness and self-care and collecting behavior leading to a tendency for clutter and a disordered environment. 14,21 Common to these patients, as well as cases in the literature, was a lack of insight and denial that their behaviors were problematic. Also observed in these patients were prominent compulsive behaviors. Distinct from hoarding syndrome, most patients displayed little interest in the accumulated items once collected and were able to allow others to discard them without distress. Additionally, none of our patients experienced anxiety or discomfort associated with hoarding or collecting or were driven by obsessions or preoccupations. These observations further suggest that Diogenes syndrome is facilitated by a pathological orientation to environmental items of interest in frontally diseased patients. 22
There may not be a pure form of Diogenes syndrome outside of dementia, schizophrenia, OCD, and other severe psychiatric illness. There is no consistent confirmation of Diogenes syndrome in otherwise normal individuals, most patients have had dementia or psychiatric conditions, and this syndrome may be most commonly secondary to specific symptoms of dementia. 9 The specific manifestations of this syndrome in dementia, in turn, argue for a distinct Diogenes syndrome, not explained by the coincident occurrence of hoarding and decreased personal hygiene, but by the interaction of these conditions along with an orientation to environmental items.
Diogenes syndrome in bvFTD appears due to the combination of 3 frontally mediated disturbances. First, these patients lack insight and are indifferent about maintaining their personal appearance, hygiene, environment, and avoiding clutter. 14,15 The lack of self-awareness results in a failure to discard collected items once they result in clutter and disorganization. Second, compulsive behavior is a prominent feature for bvFTD. Their collecting behavior occurs in the presence of additional “compulsive” behavior characteristic of bvFTD, which are more repetitive impulsions without obsessions, buildup of anxiety, or relief after the act. 14 Third, there is an orientation to environmental stimuli which may facilitate collecting behavior. 1 Many patients with frontal lobe deficits are drawn to visual stimuli or tactile perception of objects, which may activate prehension with grasping and groping behavior. These responses reflect an environmental dependency, which, in individual patients, can manifest in different ways, including utilization behavior, imitation behavior, echolalia, touching–handling, and reading outloud. 23 The environmental dependency spectrum may extend to collecting behavior, hoarding, and even pathological stealing or borrowing. 24,25
Previous neuroimaging and lesion studies have implicated abnormalities in the frontal lobe in association with decrease self-awareness and personal hygiene, compulsions, and the release of a need to accumulate objects. Neuroimaging studies of patients with bvFTD have shown that collecting behavior may be related to frontal hypoactivity 26 ; frontolimbic–striatal limbic hypometabolism 27 ; and abnormal activity in the anterior cingulate cortex (ACC), 26 its supervisory attentional system, 20 and adjacent insula. 26 Other reports have also associated collecting or borrowing behavior with lesions in the right ventromedial prefrontal cortex, right OFC, ACC, and adjacent white matter. 28,25 These specific frontolimbic regions may be important in regulating neurophysiological functions that, when deranged, may present with compulsive collecting behaviors. 29 Additionally, similar to OCD, some patients exhibit altered frontolimbic–striatal connectivity, 30 and bvFTD patients with specific gray matter loss in the basal ganglia (striatum) have had behaviors similar to OCD, including hoarding. 31 Together, our patients and this literature suggest that dysfunction of a frontolimbic–striatal system, predominantly in the right, causes release of an internal drive to collect external items. 32 This drive may have an evolutionary origin in a subcortical or mesolimbic mechanism for stockpiling or accumulating perceived important resources in case of scarcity. 28
Understanding Diogenes syndrome in bvFTD could lead to strategies for treatment and intervention. Many drugs were tried on the patients reported here, but only high-dose selective serotonin reuptake inhibitors (SSRIs), such as sertraline, seemed to have some improvement in reducing hoarding. Nevertheless, the effects of SSRIs were mixed in our patients. Others have reported benefit from other SSRIs and a combination of valpromide and quetiapine in treating patients with bvFTD and secondary Diogenes syndrome. 17 In other patients with this syndrome, previous studies show some improvement from the tricyclic clomipramine, paroxetine, and risperidone in some individuals. 2,3 Ultimately, providing individuals with a structured environment, with decluttering and cleaning, along with behavioral distraction and similar techniques, may be more effective than medications. 21
In conclusion, Diogenes syndrome may result from the combination of frontal lobe deficits resulting in decreased concern for personal care and decluttering their environment, compulsive behavior, and disinhibition of responsiveness to environmental items of interest. Moreover, patients with disease affecting a right frontolimbic–striatal system may be unable to inhibit a drive for collecting. Further research into this last frontal mechanism may help clarify collecting behavior and suggest treatment options for patients with dementia and others with Diogenes syndrome.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding National Institute on Aging R01AG034499.