
Abstract
The World Health Organization (WHO) has called for the development and adoption of national plans or strategies to guide public policy and set goals for services, supports, and research related to dementia. It called for distinct populations to be included within national plans, including adults with intellectual disability (ID). Inclusion of this group is important as having Down’s syndrome is a significant risk factor for early-onset dementia. Adults with other ID may have specific needs for dementia-related care that, if unmet, can lead to diminished quality of old age. An International Summit on Intellectual Disability and Dementia, held in Scotland, reviewed the inclusion of ID in national plans and recommended that inclusion goes beyond just description and relevance of ID. Reviews of national plans and reports on dementia show minimal consideration of ID and the challenges that carers face. The Summit recommended that persons with ID, as well as family carers, should be included in consultation processes, and greater advocacy is required from national organizations on behalf of families, with need for an infrastructure in health and social care that supports quality care for dementia.
Introduction
Many nations are experiencing a significant increase in the proportion of aging persons in their populations along with corresponding increases in age-related conditions. This includes dementia stemming from neurodegenerative conditions such as Alzheimer’s disease. 1,2 Such demographic shifts and disease contingencies apply also to aging adults with lifelong intellectual disability (note 1). Overall, some 24 million adults are projected to be affected by dementia worldwide; of these, there are at least 225 000 older adults with intellectual disability (ID), with 10% to 20% having Down’s syndrome. Due to the high risk of Alzheimer’s disease, adults with Down’s syndrome represent a large segment of the ID population with early-onset dementia. 3,4 An International Summit in Scotland (note 2) considered a range of critical and emerging issues in the field of ID and dementia, including areas of convergence and divergence, some of which are addressed elsewhere. 5,6 In this article, we specifically explore strategies for advocating and working toward including people with ID within national dementia strategies and plans.
The World Health Organization’s (WHO) report on Dementia: A Public Health Priority 1 called for the development and adoption of national dementia plans or strategies to guide public policy and set development goals for services, supports, advocacy, and research related to dementia. While there are 30 such plans in existence or in development across Europe, the total figure of only 81 worldwide suggests many countries have not yet adopted their first plan. 7 Where these national plans are in place, they address diverse issues such as encouraging research into the causes and eventual prevention of dementia, establishing early diagnosis and treatment programs, undertaking surveillance efforts, promoting the support of treatment strategies and managing supports for caregivers, setting up public education programs, integrating pathways of care, and enhancing the capabilities of workers to care for and support adults affected by dementia. 8,9 In fact, many national dementia plans additionally focus on the social care aspects of helping people with dementia, including promoting the importance of individuals remaining at home for as long as possible: making more services dementia-capable, supporting carers to delay the move of individuals with dementia to long-term care, and giving individuals living with dementia as much control over their care as possible. However, challenges remain, often due to increasing cognitive impairment (eg, in relation to having the capacity to make informed choices), equating service provision with need, promoting early diagnosis, coordinating services at the local level, and making long-term care environments as home-like as possible. 10
The WHO’s report also called upon countries to address the needs of diverse groups within the scope of these national dementia plans, such as minority ethnic groups, persons with early-onset dementia, and adults with lifelong disabilities (such as ID). 1 Within this context, Alzheimer’s and other dementia associations around the world have been advocating for the adoption of comprehensive national and subnational Alzheimer/dementia plans as a means to gain attention and focus on the social, health, and economic issue that dementia is becoming and to define solutions and mobilize resources. These plans also call attention to smaller subsets of the dementia community and have been a vehicle for persons affected by dementia and their supporters to speak out about living with dementia.
One such subset is adults with lifelong disabilities, such as ID. Inclusion of this population in national dementia plans is imperative, as research shows that adults with an ID generally experience dementia at a similar or higher rate than do other adults. For the most part, primary carers are home-based parents and other relatives who have been carers over extended periods. Further, as having Down’s syndrome is a major risk factor for Alzheimer’s disease, many such adults are at risk of early-onset dementia leading to a shortened life and diminished quality of old age. 11,12 Some studies suggest that some 50% to 70% of adults with Down’s syndrome will be affected by dementia by the age of 60. 13 -15 For other types of ID, studies point to prevalence rates for this population as equivalent to or greater than the general population. Both Janicki and Dalton 16 and Zigman et al 17 using large populations reported prevalence in line with the general population. Other reports, such Strydom et al 15 and Cooper, 18 noted higher prevalence in limited populations of adults with ID other than Down’s syndrome. The WHO recognized this phenomenon and included people with ID among those who should be specifically addressed in national dementia plans. 1
Given the abovementioned findings, the convergence of interests among dementia services and advocacy planning bodies, public health authorities, ID services, and advocacy organizations should work to assure the inclusion of this focal area within such national strategies and plans. These interests converge around meeting mental and physical health and social care needs as well as providing for long-term care when a neuropathological disease becomes prominent. Where they might diverge is with respect to service specialization, with special housing and family supports having prominence within ID services in older age.
National Dementia Strategies and ID
Defining Service Needs
The core principle guiding services for adults with ID is that any service should be aimed at meeting each individual’s needs—this principle is summarized in the concept of “person-centered planning” which has been widely promoted as an effective framework for service delivery. 19 Decision-making should be focused on each individual’s strengths, capabilities, skills, and wishes, and each individual’s family, relatives, and closest friends should be engaged with the person in all decisions with the aim of helping the person remain in his or her chosen home and community. These notions are encapsulated in the Edinburgh Principles, which are seven statements identifying a foundation for the design and support of services to people with ID affected by dementia and their carers. 20
Summit participants recognized that some of the services needed to help adults with ID are the same as are needed by other adults with dementia. The underlying assumption is that as dementia progresses, it lessens an individual’s ability to be left alone—thus, living without supervision is progressively less of an option. The core need is provision of safe adapted housing, continued engagement, and safety monitoring, as well as assistance with personal care, the nature of which will be dependent upon the degree of dysfunction experienced by the adult. Supports related to dementia care fall into several categories, 21 typically following a time line toward decline. 22 -24 Generally, this starts with pre- and peridiagnostics and involves the screening for and early detection of cognitive problems potentially transitioning into dementia; included here are assessment and diagnostic services and related follow-along services that track the progression of the dementia. It is followed by postdiagnostic supports, such as nonpharmacological interventions, personal care, day services and diversion programs, and community-based housing (ie, group homes). In parallel are supports designed to address health status and comorbidities, dental, mental and physical health care, and related needs. 25 An ancillary support area also addresses aid for the carers of the person, including carer respite, enrollment in support groups, advice for advanced planning for alternative care, and advice on end-of-life supports. Many of the abovementioned requirements for care and support are given within the ID system, whereas these are not implicit concerns in the general population until after the onset of dementia. Our focus here is to highlight the importance of this distinction and of including this population in the development of future plans and strategies, with some pertinent sources of information to support this included in Table 1.
Dementia Plan Functions Related to Intellectual Disability.
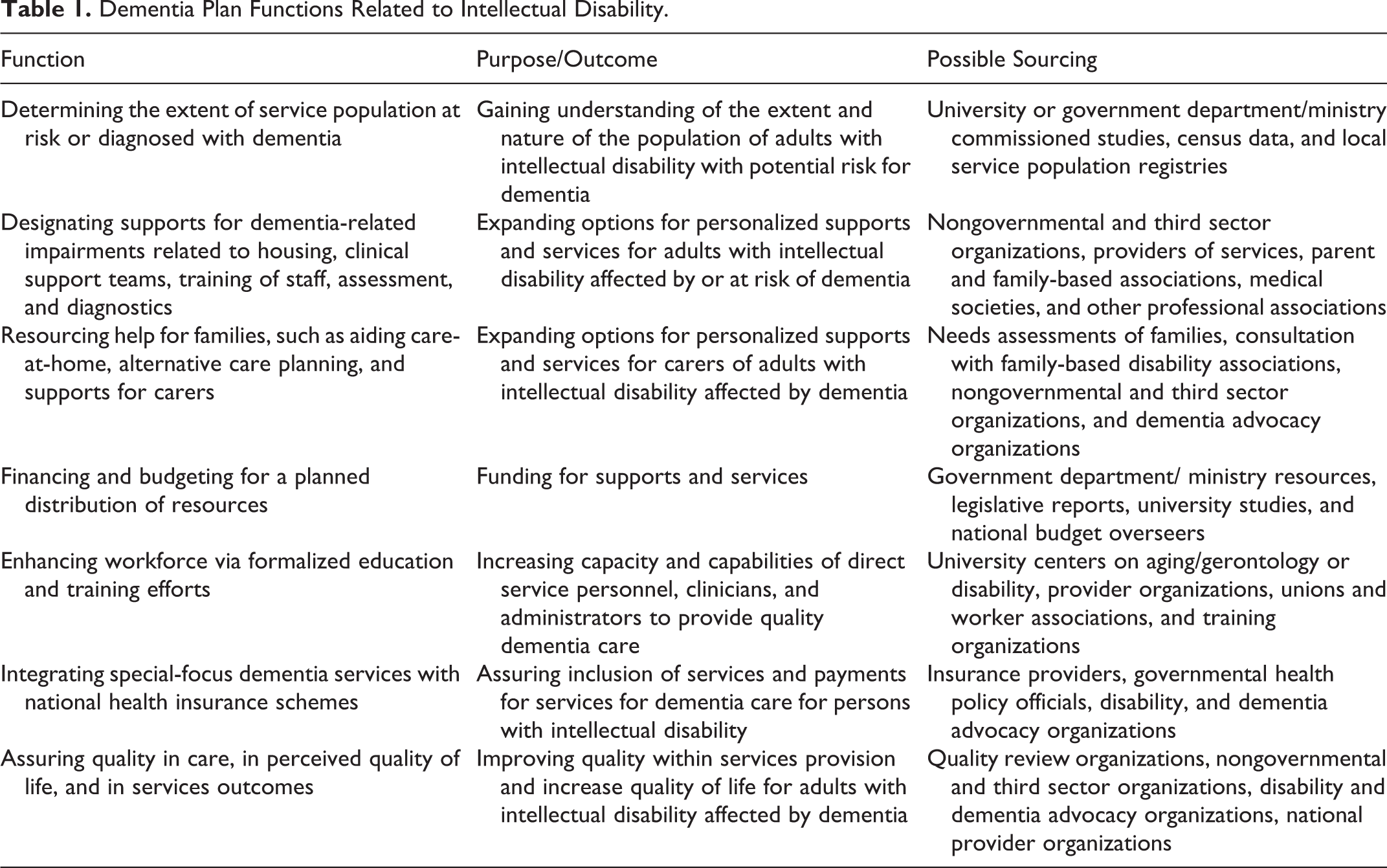
As highlighted in Table 1, the Summit notes that to put these service needs in a planning perspective for national plan inclusion would require addressing the following: determining the extent of the number of people with ID (especially Down’s syndrome), at-risk or diagnosed with dementia, defining their needs, and identifying what gaps in services exist. Elaborations are needed on designating supports for dementia-related impairments, dementia-capable housing, training and making available clinical support teams, providing a program of training for staff carers, defining resources for assessment and diagnostics, identifying health and other clinical resources, and sourcing help for families, such as aid with care at home, alternative care planning, financial aid, and other carer supports.
The Impact of ID
Although the absolute numbers of adults with ID nationally or locally may not be great, their numbers still pose a significant challenge due to the greater impact on long-term caregiving families and specialized public services. In England, for example, about 0.15% to 0.25% of the population are older adults with ID, but they consume up to 5% of the total public personal care budget. 26 Many older adults with ID live in the family home with parents who are themselves older or with a sibling. Others are supported by social care providers either in their own home or in shared accommodation supported by staff who are often the primary carers and who may need information and specialized input. Often the onus falls on organizations, such as national Alzheimer’s societies, to respond to inquiries, yet many by their own admission are not equipped or informed enough to do so. 27 Older persons’ services typically have a fixed requirement of 60 or 65 years of age for access to their services, leaving persons with ID who may have an earlier age of onset (particularly those with Down’s syndrome), and often their families, with unmet needs.
Linking to Services
A key consideration is how national organizations devoted to advocacy on behalf of people affected by Alzheimer’s disease and related dementias address the needs of people with ID and dementia and the needs of their carers, whether paid staff or family members, whose main difference, in many instances, is a lifelong dependency status. One survey 28 of Alzheimer’s Disease International’s (ADI) 77 national affiliates organizations revealed that there was resistance in their constituents to bridging the dementia and disability agenda. This was evident from the perception of their government’s lack of financial support, resistance from within their organization’s administration, or a belief that their services were inappropriate to the needs of people with intellectual disabilities and dementia. Such difficulties were amplified by a lack of understanding of key issues affecting people with ID and their families; by not having an established linkage with a national Down’s syndrome group; low awareness of risk of people with Down’s syndrome developing dementia; lack of support to offer service to this group (although typically a willingness existed to co-operate with parents’ association of persons with ID); and lack of appreciation of the longevity of people with ID. These findings showed that there was disconnect between the daily demands on the Alzheimer’s organizations for more services and the low awareness on the part of governmental agencies or ministries about people with ID or their families. Given that most of the organizations reported a very low rate of involvement or support from public authorities, it would appear that inclusion in national plans would be a challenge; yet, such inclusion would be an optimal way to raise awareness, commit resources, include adults with ID within general dementia services, and support both formal (paid) and informal (family) carers.
Some countries have begun to include consideration of ID within national or regional strategies and plans. Splaine Consulting conducted a survey 27 of 79 national and subnational dementia plans and found that approximately 37% mentioned adults with intellectual/learning (note 3) and/or developmental disabilities, with variation in how this was included. For example, some presented information about ID and dementia, while others presented actions that are taking place. It should be noted that although some countries are yet to develop a national plan or strategy, a small number are onto their second or in the case of Scotland, their third. Attention should be paid to changes in second and subsequent plans that recognize this development with an increased recognition, albeit in a limited manner, of the needs of marginalized populations in relation to dementia care. For example, in Norway’s first dementia plan, Dementia 2015, people with ID were omitted entirely, yet in the second, Dementia 2020, there is a distinct section related to ID with the clear recommendation that support models identified in national dementia plans should also be adapted to people with ID. 29 In Scotland, the first dementia plan 30 —Scotland’s National Dementia Strategy—made reference to the link between Down’s syndrome and dementia, while the second 31 —Scotland’s National Dementia strategy 2013-2016—made a specific commitment to seek further information that will inform the third strategy due in 2017. In the United States, the annual updates to the National Plan to Address Alzheimer’s Disease 32 which has a time line of 2025 progressively have increased mention of ID, since the Plan’s first iteration in 2012. 33,34 This is a productive progression, perhaps indicative of increased recognition not only of the incidence and prevalence but of the supports available recognizing the unique characteristics of this population. Such inclusion in national plans serves to make the document immediately relevant for staff of intellectual organizations as do any recommendations for dementia-related training and awareness raising.
Plan Information
Summit attendees considered what aspects needed to be considered when addressing ID in national strategies or plans. One would be demographics; it is useful to report the number or percentage of the population that this group represents. If epidemiological data are absent, then an estimate of the number of persons potentially affected can be ascertained by identifying the number of adults aged 60 and older with ID and assume that a minimum 6% of this group may be affected by dementia. However, it is also necessary to factor in an estimate of those adults aged 45 to 59 (due to health implications associated with premature aging and early-onset dementia). Second, derive a figure for home-based caregivers. To do this, estimate, or ascertain from government departments, the numbers of families throughout the country who may be home-based carers of older adults with ID, and in particular those with Down’s syndrome, so as to identify the risk population for home-based support services. Third, determine the number of persons currently being supported. To do this, ascertain the numbers of older adults in formal services within the country and derive an estimation of the risk for dementia—so as to plan for out-of-home care. The assumption is that demand for out-of-home care may increase as the primary carers age. In many instances, this is the result of the additional stress experienced by families, where the primary carer may be an older parent who is experiencing health or cognitive changes.
The degree of specificity of inclusion of dementia-related services for persons with ID in national plans may be driven by the availability of mandated services for persons with ID within a country. Specialized dementia-capable services adapted to persons with ID are already in prevalent use in those countries with established formal life-span support schemes for persons with lifelong special needs. 33,34 In these instances, plan consideration may be on recognizing the utility of such services and advocating for their expansion. In countries with informal and less established or undeveloped services for persons with ID, adaptation of foundational models applicable to dementia care that may be in use with the general population would be appropriate. In these instances, the plan consideration may be on advocating for adapting such generic services to the care of persons with ID. Such foundational process models widely used in generic dementia services, and which also may be appropriate for use with persons with ID, typically include those that focus on person-centered care. Examples of these include, the VIPS framework model of person-centered care, 35 dementia care mapping, 36 and the Marte Meo method with application to dementia. 37 There are also specialized delivery models that can apply to both persons with ID and the general population. Such specialty delivery models already in prevalent use within ID services include use of small, community-centered group homes (which offer an alternative to institutional congregate care), and enrollment in day support services, which provide a nurturing environment for persons with dementia and respite for carers. 33,34
Another plan consideration would be directed toward raising public awareness. This can work on two levels. The first is a focus on the general public and the second on the aging and disability-related services’ workforce. Raising general awareness within the public can further advocacy goals and gain support from voters for legislation-enhancing services or the channeling of public funds. With respect to the personnel employed in dementia-related support functions, workforce capacity enhancement should target all levels of workers, including administrators and clinicians, so that they become more proficient in understanding and identifying dementia. Workforce enhancement should also include gaining familiarity with dementia-capable care and environments. 38 Including this aspect in plans can further the goal to enable early identification of adults with ID showing symptoms so as to facilitate engagement in the diagnostic process and enable them and their carers to begin to plan for additional care and health intervention as appropriate when dementia progresses. 39 Equally important is ensuring that the need for medical screening, assessment, and diagnostic resources are stated in the plan and then pursued in order to identify dementia in adults with ID. This can serve several purposes, one is to identify the nature of the dementia (and its etiology) and another is to conduct a differential diagnosis and eliminate other neuropathological causes for behavior change (such as depression, adverse drug reactions, or thyroid conditions). Additional benefits include having a workforce with a stronger grounding in dementia and an understanding of the services and approaches that work best when supporting persons with ID affected by dementia. Finally, focal areas in the plan should address practices enhancing the quality of life of adults with ID affected by dementia. 40,41
Further plan considerations can include the bridging of care supports within the ID system with those of providers whose primary goal is to serve persons with dementia. Nakanishi and Nakashima 42 noted the importance of cooperation among “silos” as a feature to be encouraged in national plan efforts. This could involve inclusion within efforts to plan housing, homecare supports, medical reviews and treatment, palliative care and hospice teams, and end-of-life care activities. The plan development may also consider how to form and support voluntary advocacy groups who can help input into the plan and serve as a “watchman” or “overseer” over the delivery of public services which may be a first step toward the voice of people with ID being heard in focus groups for new policy development. 33,34 Finally, the plan should incorporate the requirement to include ID in any research related to dementia being undertaken, whether basic or remedial (ie, medical or social). Also, any research focusing on prevention should give due consideration to ID and include persons with ID as participants.
In summary, the Summit proposes that national dementia strategies or plans minimally include, but preferably go beyond, passive functions, including description and relevance of this group, and notations of the higher risk factor recognition. This should extend to proactive functions including recognition of the need for access to specialized diagnosis resources, maintaining quality of care and quality of life as dementia progresses to advanced stage, recognizing complexities with recognizing end of life, increasing capacity of the workforce via training and education for service providers, supporting (unpaid) carers of persons with ID and dementia, enabling adaptation of existing ID services to accommodate dementia; proposing reviews of health-care schemes and public funding programs so that ID providers can receive payments or reimbursements commensurate with costs of dementia care, instituting healthy brain and physical health initiatives (to promote prevention), and undertaking government-supported research activities in both the underlying etiological factors and best practices in providing quality care.
Strategies for Inclusion in Dementia Plans
One consideration is the extent to which persons with dementia are involved in existing national plan development or implementation. Alzheimer Disease International commissioned a study 28 that looked at 20 extant national plans to ascertain whether persons with dementia in general were involved with plan development and found that persons with dementia fell into two main categories. They were either included as members on a task force, working group, or committee or were involved in a public comment period or consultation process; others had no involvement at all. Of the 20 national plans examined, they found that only one country stated persons with dementia were included in its working groups, another included two Alzheimer’s patient advocates on a national advisory council which helped create and annually updated the national plan, and five countries involved persons with dementia in workshops or consultation/dialogue/ questionnaire processes or mentioned that their plan was informed by the views of persons with dementia. The study found that the other 14 countries did not specifically mention the involvement of persons with dementia in the development of their national plans but that this does not necessarily correlate with no involvement of persons with dementia. The “take-away” from this analysis is that while not many adults with dementia are involved in the national plan development and oversight process, even less involvement may be of adults with ID or their advocates.
We know of no instances in which persons with ID (who are conceivably at risk of dementia and capable of personal involvement in planning groups) have had a role in the task forces/work groups that have developed national dementia plans; rarely also are their advocates included in their working groups. Thus, public testimony and advocacy by surrogates and concerned government agencies seem to be the sources of influence. Given that we know very little about this, the Summit working group recommends investigating to what extent there is any involvement by adults with ID in dementia plan development groups. Another investigation should examine to what extent national voluntary or third sector organizations are devoting efforts to advocacy on behalf of people with ID affected by dementia. Anecdotally, there seems to have been little pressure from third sector organizations on issues around aging in general among people with ID. The ID organizations are more likely to have input into disability-specific policy rather than dementia-related policy, despite the known incidence and prevalence. Among ID organizations, parents are the largest group of members, and it seems that most have a primary focus on the challenges their children face when they are younger, with far fewer engaged in these organizations when their children are older adults. It may be that when there are few relatives who engage in this type of advocacy, there is also no pressure on the national dementia organizations and governments. 33,34 Also, at the time of highest risk for dementia, parents may themselves likely be aging, affecting their continued engagement.
A resource for information on the inclusion of people with ID within a national plan is to draw upon other reports or pressure presented by national advocacy organizations. Examples of such national reports/plans are the “My Thinker’s Not Working” document issued by the National Task Group on Intellectual Disabilities and Dementia Practices in the United States 43 and “Dimentica la Disabilità e Guarda alla Persona” issued by a consortia of organizations in Italy. 44 Both of these documents provide a wide-ranging analysis of the needs of adults with ID affected by dementia and include goals and plans for the development of services and addressing of needs (note 4). Another example is “Dementia and Equality—Meeting the Challenge in Scotland,” a report that followed Scotland’s second National Dementia Strategy 2013–16 identifying 17 national commitments underpinned by a human rights approach. 45 This strategy highlights five particular population groups with characteristics protected by the Equality Act 2010, 46 where challenges might arise in the context of dementia, one of which is ID. Also, the Norwegian Dementia Plan 2020 recognized the absence of minority groups, including people with ID and affirmed that all strategies and measures in the plan must be adapted to people with ID. 29 It does not need to be only a national or local plan that informs inclusion in general dementia plans; the Convention for the Rights of Persons with Disabilities 47 can be drawn upon to infuse consideration of the perspectives of persons with dementia (including those with ID) into the national public policy and planning discourse. 48
Thus, strategic initiatives may have to be undertaken to actively promote the inclusion of ID in national plans. These efforts may include any or all of the following: (1) ensuring that adults with ID with knowledge of dementia are invited onto planning groups or working parties providing contributions to national plans and related policy; (2) contributing to issue briefs and policy letters on dementia and ID by national or other self-interest groups within the intellectual disability field; (3) requesting inclusion of representatives of national intellectual disability organizations onto national councils, boards, or planning bodies creating or monitoring national dementia plans; (4) advocating and raising awareness among governmental officials and bodies of the public policy issues related to dementia and intellectual disability; (5) advising on how dementia-capable care environments can be further adapted to meet the particular needs of adults with ID; and (6) creating public awareness by assisting the press and other media to develop and present human interest stories about carers and persons with ID affected by dementia.
Recommendations
Noting the issues and problems related to gaining attention for adults with ID affected by dementia, the Summit recommended that: Advocates and self-advocates, including ID or Down’s syndrome specific organizations, mobilize to make their issues known to authorities responsible for the development, or redevelopment/update of national dementia plans Forums, meetings, and consultations held in advance of national plans being developed or modified should ensure appropriate representation; these should include alternate and accessible methods of communication as required to ensure inclusion of people with intellectual disability and families Government representatives be drawn into the process and requested to provide demographic, services, and financial data related to ID for use in the plan Discussions be held at a policy level to determine what laws or existing policies may need to be instituted or altered/updated to facilitate the inclusion of ID in national dementia strategies or plans Involve self-advocates or persons authorized to speak on behalf of adults with an ID, in the development or review of documents produced related to a national dementia strategy and make available the documents in accessible formats
Summary
Governments have had a major role in providing for the health, welfare, economic, and social stability for persons with ID. Over the past 60 years, the interpretation of this role has changed considerably, from a focus on a responsibility for remedial and custodial care to one on various supports, social inclusion, and autonomy. With increased longevity, adults with ID, like other persons, now face the prospect of having a neuropathology in old age. 49 This risk is especially acute for persons with Down’s syndrome. This means there is a need for inclusion of ID issues in national dementia planning. To effect inclusion, active advocacy needs to be undertaken to involve individuals and groups representing people with ID on planning bodies and those constructing national plans.
The Summit proposes that inclusive and thoughtful planning on dementia must include people with ID; recognized by the WHO as a “group having additional needs.” In addition to the topics noted earlier, plans should designate a consistent policy home for persons dually affected, accurate census/surveillance of the numbers of affected persons, and possible policy changes to empower the carers and services’ staff in becoming advocates in address barriers to health care. 39 To make this happen, it is incumbent on ID organizations to prepare background material, personal stories, and rationales for inclusion. This is in addition to working with policy officers to raise awareness and promote inclusion of their concerns and needs in national dementia service delivery efforts and national and regional plans.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The contents of this statement and preceding International Summit, were partially developed under a grant from the United States Department of Health and Human Services, Administration for Community Living (ACL), National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR) Grant # 90RT5020-03-00. Additional support was provided by grants from RS MacDonald Charitable Trust, Edinburgh; Alzheimer Scotland, and the Scottish Government.