
Abstract
Objectives:
These 2 studies assessed a technology-aided program to support mild physical exercise or simple occupational activity in participants with moderate to severe Alzheimer’s disease.
Methods:
Study 1 included 11 participants who were to perform a leg-raising response. Study 2 included 10 participants who were to sort objects into different containers. The program ensured that they received positive stimulation contingent on the responses and reminders/prompts after periods of nonresponding. Each study was carried out according to a nonconcurrent multiple baseline design across participants.
Results:
The program was successful in supporting mild physical exercise and activity with objects in the 2 groups of participants, respectively. The participants also showed signs of positive involvement (eg, smiles and verbalizations) during the sessions. Moreover, staff personnel rated the program and its impact positively.
Conclusion:
The program may be considered a practical resource for supporting positive engagement in persons with moderate to severe Alzheimer’s disease.
Introduction
Alzheimer’s disease is a neurodegenerative disorder that causes a progressive decline in the conditions of the persons affected. 1 –8 These persons gradually lose their abilities to deal with time, space, and money; to perform relevant tasks (ie, from vocational, recreational, and self-care tasks to simple occupational tasks); and to walk. Although the disease is the focus of extensive research, no treatments exist to stop or effectively modify its course, and potentially decisive (disease-modifying) drugs are still under investigation. 9 –11 Available pharmacological interventions, such as the use of acetylcholinesterase inhibitors and memantine, serve mainly to counterbalance the neurotransmitter disturbance and improve the behavior and/or slow down the decline in the persons treated. 12 –15 Similarly, behavioral interventions, such as those used for supporting the performance of daily tasks or verbal reminiscence and promoting mild physical activity/exercise, provide the persons extra opportunities of positive engagement that temporarily curb the disease’s symptoms and degenerative process. 16 –23
Research has shown that behavioral interventions can also be delivered by means of technology-aided programs, which may be (1) advantageous in terms of procedural accuracy and reliability as well as in terms of staff costs and thus (2) plausible and affordable within daily contexts. 19,22,24,25 For example, Lancioni and colleagues 19,26 –28 used multiple versions of a technology-aided program to (1) present persons with mild and moderate Alzheimer’s disease verbal or visual instructions for the single steps of functional daily tasks (eg, preparing tea or coffee) and (2) regulate such presentation based on the participant’s performance and preset time criteria. Similarly, Lancioni and colleagues 21 –23 used a technology-aided program to support mild physical activity/exercise (ie, arm raising or leg–foot movement) in persons with advanced (ie, moderate to severe) Alzheimer’s disease who were sedentary and inactive. The program involved the delivery of brief periods of preferred stimulation after each arm or leg response and verbal reminders/prompts when the participants failed to respond for a preset period of time.
The results obtained using the aforementioned technology-aided programs were quite encouraging, indicative of the programs’ potential for supporting the participants’ positive engagement (ie, multistep daily tasks or mild physical activity/exercise). 23,24,28 In spite of that mentioned earlier, one needs to be cautious in drawing conclusions and making recommendations. In fact, the first type of program was assessed with a relatively small number of daily tasks (ie, a total of 9) and required special arrangements of the objects involved in the tasks. 19,26 The second type of program was assessed with a relatively small number of participants (ie, a total of 25) and with only one form of activity (ie, arm or leg movements). 22,23 Given this situation, new research efforts seem warranted with regard to both types of programs and particularly in connection with the second one. For this program, one could envisage replication and extension trials, that is, (1) a further assessment of the program with the form of activity (ie, basic arm or leg responses) previously used and (2) an assessment of the program (or an adapted version thereof) with different forms of activity (eg, occupational activity with simple use of objects). 29 –32
These 2 studies represent the aforementioned replication and extension trials in participants with general passivity. Specifically, study 1 assessed the effects of the program in promoting leg-raising responses in 11 new participants diagnosed with moderate to severe Alzheimer’s disease. The participants’ levels of positive involvement (eg, smiles and vocalizations) during the program sessions and the rating of the program by staff personnel were also recorded. Study 2 assessed the effects of an adapted version of the program in promoting simple occupational activity (ie, sorting objects into different containers) in 10 participants diagnosed with moderate Alzheimer’s disease. As in study 1, the participants’ positive involvement during the program sessions and the rating of the program by staff personnel were also recorded. Positive results in terms of participants’ activity engagement in the 2 studies would confirm the efficacy of the program or adapted version thereof across different activity conditions. 31,32 Positive results in terms of participants’ involvement and staff rating would provide the evidence required for (1) recommending such a program to daily contexts and (2) envisaging a favorable response by those contexts. 33,34
Study 1
Method
Participants
Thirteen persons were initially selected for this study. Two of them left the program early or after sporadic attendance (due to health or practical reasons) and were thus dropped. The other 11 received more than 75 intervention sessions and are here indicated as the participants (ie, participants 1-11). The participants, who represented a convenience sample, 35 were considered to function at the lower half of the moderate or at the severe level of Alzheimer’s disease and attended centers for people with Alzheimer’s disease and other dementias. Table 1 reports the participants’ sex, age, and scores on the Mini-Mental State Examination. 36 Their selection was based on 3 basic criteria. 23 First, they were sedentary and generally passive and withdrawn but could perform the leg-raising response targeted in this study and deemed beneficial for them. 37 –39 Second, they seemed to enjoy stimulation events, such as music and videos, and responded to verbal reminders/prompts for the performance of arm or leg movements. Third, staff and families had expressed support for the program considering it beneficial and enjoyable (due to the stimulation opportunities available) for the participants. 40 –42 Given their condition, the participants could not provide formal consent for their involvement in the study. Their families provided such consent. The study complied with the 1964 Helsinki declaration and its later amendments and was approved by the Ethics Committee of the Alzheimer Association, Bari, Italy.
Participants’ Characteristics (Study 1).
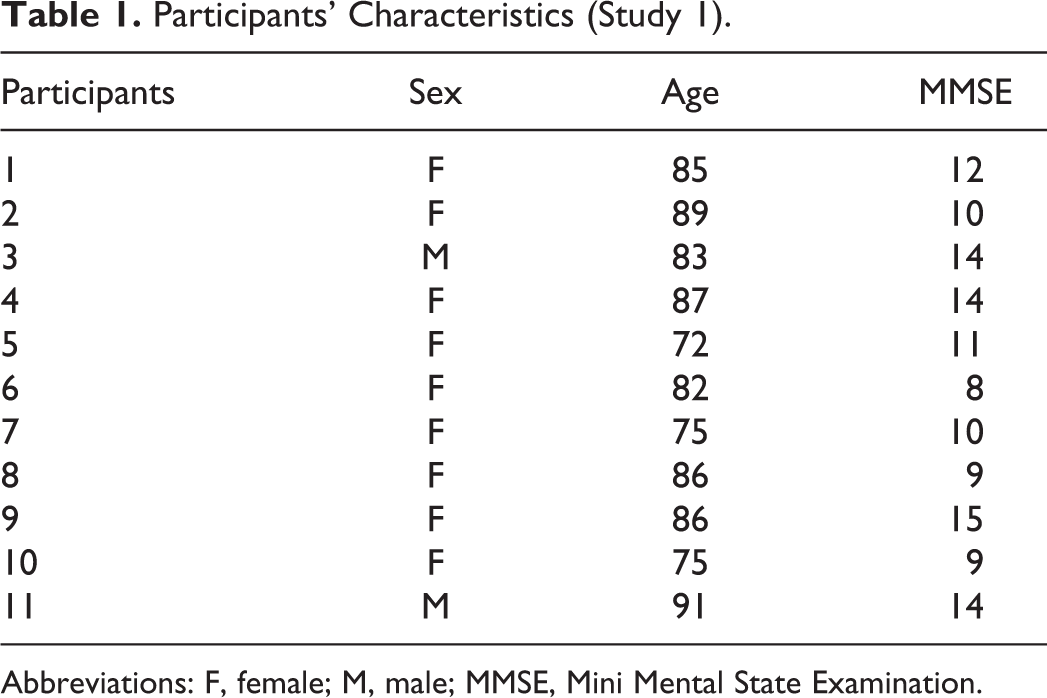
Abbreviations: F, female; M, male; MMSE, Mini Mental State Examination.
Sessions, Leg Responses, Technology, Stimulation, Reminders, and Indices of Positive Involvement
Sessions lasted 5 minutes and were carried out on an individual basis in a quiet area of the center that the participants attended (typically 2-5 times a day). Leg-raising responses consisted of the participants lifting the right or left leg (ie, according to their motor conditions). The technology included a microswitch, a computer with sound amplifier, and basic software. 22 The microswitch included 1 or 2 tilt devices fixed to the participant’s leg(s) or foot/feet and detected the leg responses. 43 The computer, which was linked to the microswitch, served to (1) record the leg responses (ie, throughout all sessions of the study) and (2) deliver stimulation events and verbal reminders and record them (during the intervention sessions). Stimulation events lasted 10 seconds and followed the performance of the leg responses. Different events (eg, different segments of a song) would be delivered for different responses so as to ensure stimulus variation. Reminders (ie, calls to lift the leg) occurred if they failed to respond for about 15 seconds after the start of the session or the end of a stimulation event.
Stimulation events included segments of old songs, religious hymns, prayers, and matching videos, which were considered preferred for the participants by staff and in light of direct screening. Screening entailed at least 10 nonconsecutive presentations of brief segments of various stimuli of the aforementioned categories. A stimulus was selected for use during the intervention sessions if the 2 research assistants who conducted the screening agreed that it produced positive reactions, such as orienting, smiling, or verbalizations, in 60% or more of the presentations. 23,44
In addition to the aforementioned leg responses, stimulation events, and reminders, data recording also involved the participants’ indices of positive involvement (ie, singing, music-related body movements, positive verbalizations, and smiles). 22 These indices, contrary to the other measures, were recorded by research assistants. Recording was carried out for each participant during 2 or 3 baseline sessions and 20 to 25 nonconsecutive intervention sessions using a partial interval system, in which 10-second observation intervals were followed by 5-second scoring periods. 45 Interrater agreement was checked in more than 50% of the aforementioned sessions (with 2 research assistants involved in the recording) and was computed by dividing the intervals with matching scores by the total number of intervals and multiplying by 100%. Session agreements were within the 80% to 100% range, with means exceeding 90% for all participants.
Experimental Conditions and Data Analysis
A nonconcurrent multiple baseline design across participants was used to assess the effects of the program on leg responses and indices of positive involvement.
29
The baseline phase included between 2 and 4 sessions for the different participants. The number of sessions was decided in advance. Yet, a participant would receive extra sessions if his or her response frequency was above 5 and showed an increasing trend. (This condition never materialized.) The intervention phase included between 81 and 127 sessions, with the differences among participants largely due to their availability. During the sessions, the participants sat in their wheelchair or a regular chair and were provided with the technology. Prior to each baseline session and the initial 30 intervention sessions, they were also guided to perform the target response. After the end of the intervention, staff personnel were asked to rate the program (see below). The baseline and intervention data on leg responses and indices of positive involvement of each participant were (1) summarized/reported in terms of mean values per session and (2) analyzed through the percentage of nonoverlapping data (PND) method, which allowed to determine the percentage of intervention data points exceeding the baseline levels.
46,47
Baseline: During the baseline sessions, the technology did not provide stimulation or reminders but simply recorded the leg responses.
Intervention: During the intervention sessions, the technology provided stimulation and reminders. Four or 5 introductory sessions were conducted prior to the start of the intervention. During these sessions, the research assistants ensured that the participants practice responding to the reminders and experience the stimulation for their responses.
Staff Rating
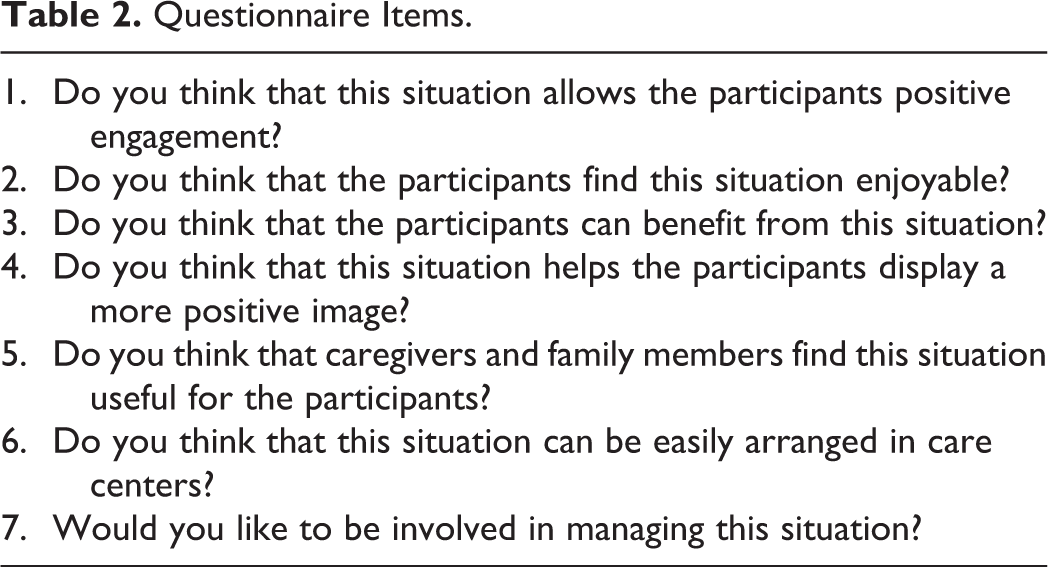
Twenty-two staff persons working with people having Alzheimer’s disease (ie, nurses, physiotherapists, physicians, and occupation/education therapists) participated in rating the program. They were between 24 and 52 (mean = 36) years of age, represented a convenience sample, 35 and were divided into 2 groups of 11. The groups watched videos containing six and five 1.5-minute segments, respectively. Those segments were related to the first 6 and the last 5 participants, respectively. Research assistants had selected those segments on the agreement that they were representative of the participants’ behavior during the intervention sessions. After watching the allotted video, staff provided their rating using a 7-item questionnaire (see Table 2). Item scores could vary from 1 (ie, least positive value) to 5 (ie, most positive value).
Questionnaire Items.
Results
Table 3 reports the participants’ mean frequencies (and frequency ranges) of leg-raising responses per session during the baseline and intervention phases of the study. During the baseline, the participants’ mean frequencies of leg-raising responses per session were between 0 and 4. During the intervention, the mean frequencies of leg-raising responses per session varied from about 10 (participant 8) to about 20 (participant 7). The mean frequencies of computer reminders (available only during the intervention phase) varied among participants from slightly above 0 to near 8 per session, with an overall mean across participants of about 3. Comparisons of the intervention and baseline’s session response frequencies, according to the PND method, showed indices of 100% for all participants (ie, all their intervention data points exceeded their baseline levels), thus indicating that the program was highly effective. 47
Number of Sessions, Mean Frequencies of Responses Per Session, and Frequency Ranges During Baseline and Intervention (Study 1).a
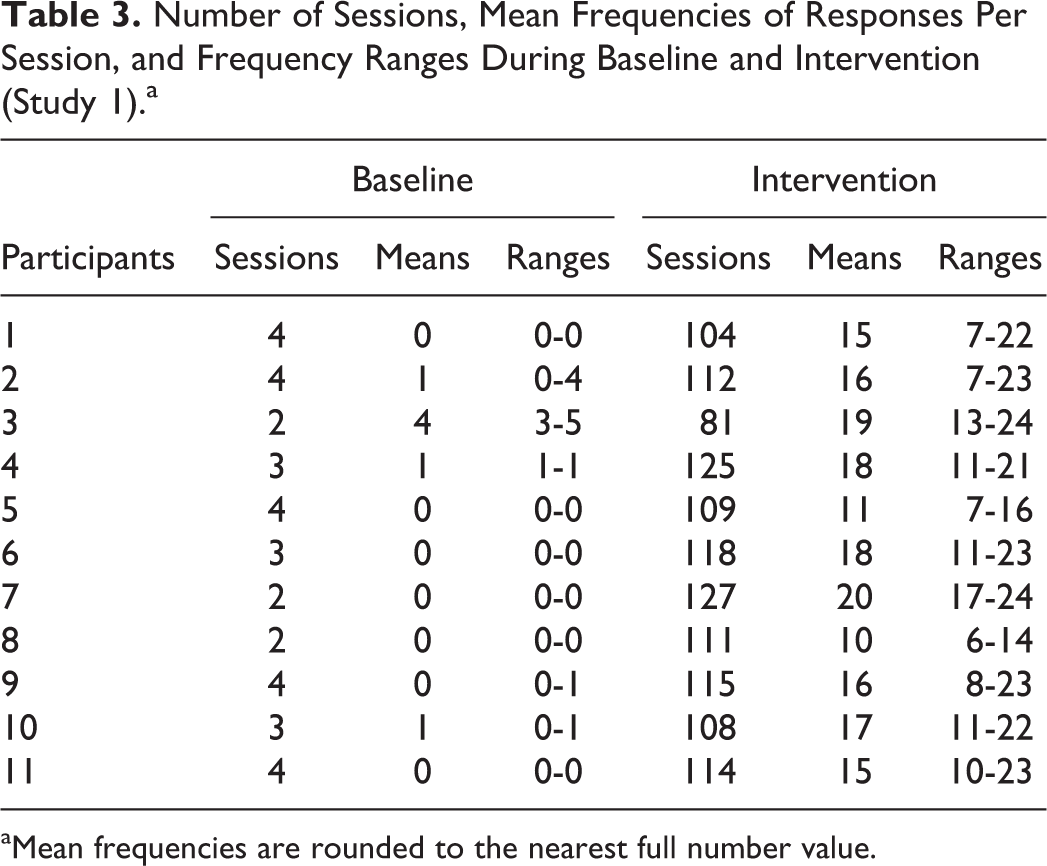
aMean frequencies are rounded to the nearest full number value.
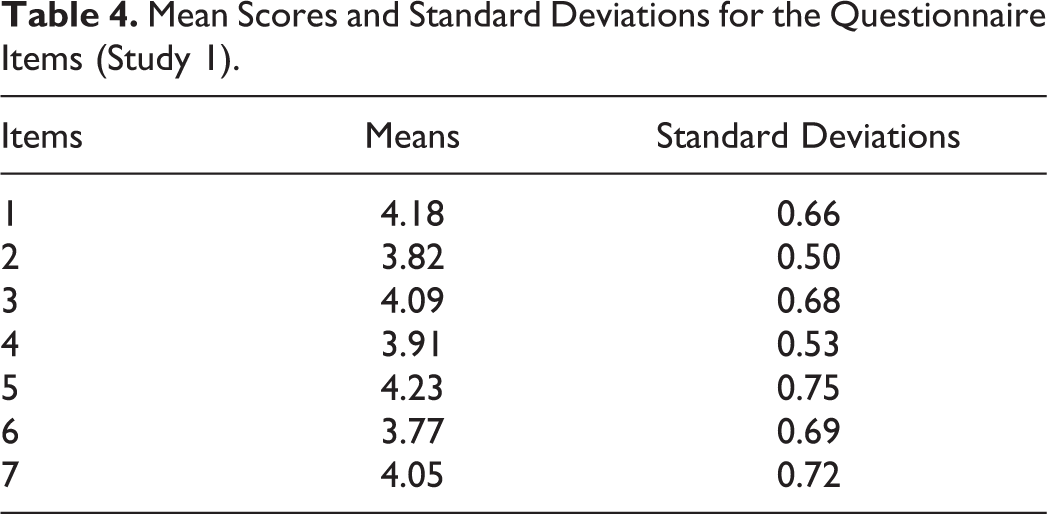
The mean percentages of intervals with signs of positive personal involvement were between 0 and about 15 during the 2 or 3 baseline sessions and increased to between about 30 (participant 4) and over 70 (participant 6), with an overall mean exceeding 45, during the 20 to 25 intervention sessions (see above for the recording of this measure). Comparisons of the intervention and baseline’s session data for the single participants, according to the PND method, showed indices ranging from 90% to 100% (indicating strong effects of the program), except in the case of participants 2, 4, 10, and 11. These participants had indices varying between 72% and 88% (ie, indices that were still sufficiently high to stress the impact of the program). 47 The staff’s mean scores and standard deviations for the single questionnaire items are summarized in Table 4. As shown in the table, the mean scores exceeded 3.5 for each of the items, suggesting fairly positive rating.
Mean Scores and Standard Deviations for the Questionnaire Items (Study 1).
Study 2
Method
Participants
Eleven persons were selected for this study, but 1 left the program after a few days (for practical reasons) and is not included here. The 10 included (ie, participants 1-10) were diagnosed with moderate Alzheimer’s disease, attended centers for people with Alzheimer’s disease and other dementias, and represented a convenience sample. 35 Table 5 reports their sex, age, and Mini-Mental scores. Three basic criteria were followed for their selection. First, they tended to be sedentary and passive and were unable to perform complex tasks but could manipulate and differentiate objects and put them away (ie, sort them into different containers). Second, they responded to verbal reminders concerning the sorting of those objects and were interested in environmental stimulation events, such as music and videos. Third, their families and staff supported the use of a technology-aided program for fostering positive engagement in simple occupational activity through preferred stimulation for appropriate responses and reminders. Participants seemed keen to be involved in the study but could not provide a formal consent. Their families provided such consent. The study complied with the 1964 Helsinki declaration and its later amendments and had been approved by the same ethics committee as study 1.
Participants’ Characteristics (Study 2).
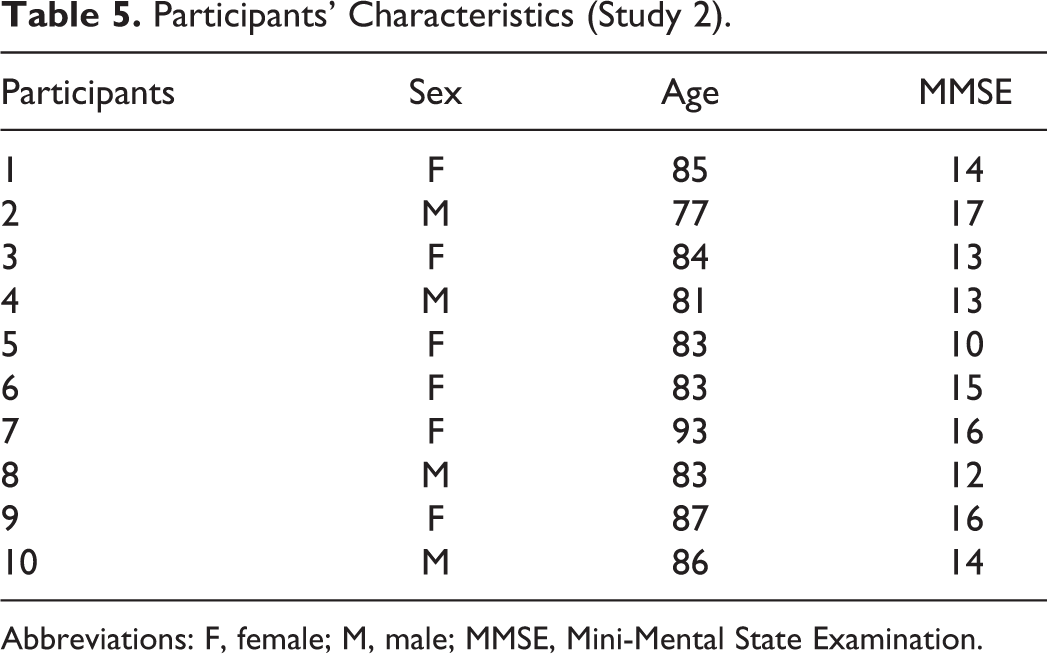
Abbreviations: F, female; M, male; MMSE, Mini-Mental State Examination.
Sessions, Activity Responses, Technology, Stimulation, Reminders, and Indices of Positive Involvement
Sessions were conducted on an individual basis and lasted 5 minutes as in study 1. The participants sat at a desk and had 2 or 3 containers of different colors and series of objects of matching colors (eg, cups, booklets, boxes, or brushes) in front of them. The activity consisted of putting the objects into the containers (possibly the containers of matching colors). Putting an object into a container was recorded as a response and was followed by positive stimulation during the intervention sessions (see below). The technology included optic microswitches, 43 a computer with sound amplifier, and basic software. The microswitches were fixed to the containers and detected the participants’ responses. The computer, which was linked to the microswitches, worked as described in study 1, that is, it (1) recorded the participants’ responses (during all sessions) and (2) delivered stimulation events and verbal reminders and recorded them (during the intervention sessions). Conditions concerning stimulation events, reminders, and indices of positive involvement as well as the recording of these indices and interrater agreement on them were comparable with those described in study 1.
Experimental Conditions and Data Analysis
As in study 1, a nonconcurrent multiple baseline design across participants was used to determine the effects of the program.
29
The baseline phase included between 2 and 6 sessions. The intervention phase included between 89 and 116 sessions, except for participant 9 who had only 50 sessions because of health problems. At the end of the intervention, staff rated the program (ie, the adapted version used in study 2).
Baseline: During the baseline sessions, the technology served only to record the responses.
Intervention: During the intervention sessions, the technology provided and recorded stimulation and reminders in addition to recording the responses. Introductory sessions were available as in study 1.
Staff Rating
Twenty-two staff persons (other than those involved in study 1), who worked with people with Alzheimer’s disease and represented a convenience sample, 35 participated in rating the program. They were between 25 and 56 (mean = 37) years of age and were divided into 2 groups of 11. Each group was to (1) watch a video containing five 1.5-minute segments related to 5 participants (ie, the first or last 5) of study 2 and (b) score it on the 7-item questionnaire used in study 1.
Results
Table 6 reports the participants’ mean frequencies (and frequency ranges) of responses per session during the baseline and intervention phases. During the baseline, the participants’ mean frequencies of responses per session were between 0 and 5. During the intervention, the mean frequencies of responses per session varied from about 9 (participant 5) to about 15 (participants 1 and 6). The mean frequencies of computer reminders (available only during the intervention phase) varied for the single participants from below 1 to about 7 per session, with an overall mean frequency across participants exceeding 3. Comparisons of the intervention and baseline response frequencies for the single participants, according to the PND method, showed indices of 100% (ie, with all intervention data points exceeding the baseline performance). 47
Number of Sessions, Mean Frequencies of Responses per Session, and Frequency Ranges During Baseline and Intervention (Study 2).a
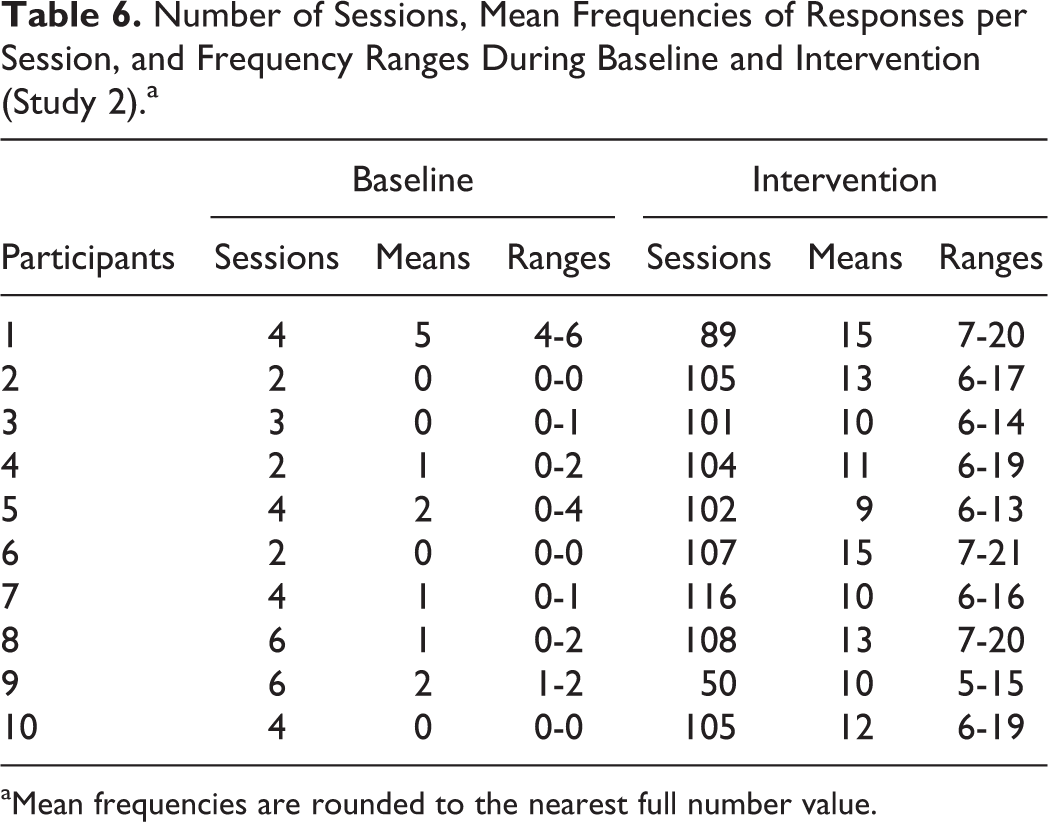
aMean frequencies are rounded to the nearest full number value.
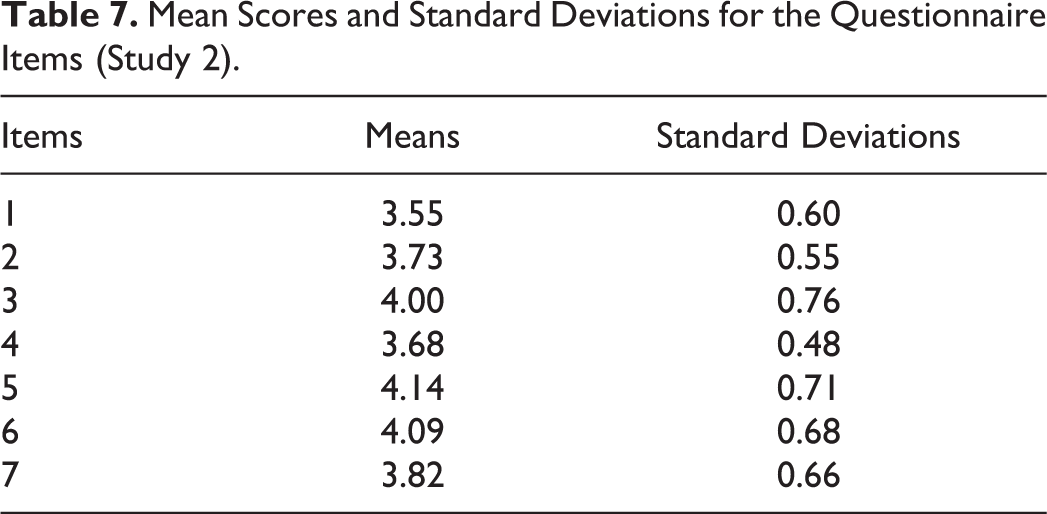
The mean percentages of intervals with signs of positive personal involvement were between 0 and about 7 during the 2 or 3 baseline sessions and between about 15 (participants 1 and 9) and above 50 (participants 8 and 10), with an overall mean exceeding 35, during the intervention sessions (ie, 14 for participant 9 and 20-25 for the other participants). Comparisons of the intervention and baseline’s session data for the single participants, according to the PND method, showed indices between 90% and 100% (ie, strong effects of the program), except for participants 1 and 9. These participants had indices of 82% and 57%, indicating certain and questionable effects of the program, respectively. 47 The staff’s mean scores and standard deviations for the questionnaire items are summarized in Table 7. As shown in the table, the mean scores exceeded 3.5 for each of the items, suggesting fairly positive rating.
Mean Scores and Standard Deviations for the Questionnaire Items (Study 2).
Discussion
The results of study 1 support preliminary evidence on the positive impact of a simple technology-aided program for promoting and sustaining mild physical activity/exercise in persons with moderate to severe Alzheimer’s disease who are generally inactive and withdrawn. 22,23 The results of study 2 show that an adapted version of the program could also be used to promote and sustain simple occupational activity with similarly passive participants diagnosed with moderate Alzheimer’s disease. Nearly all participants of the 2 studies had a clear increase in indices of positive involvement (eg, smiles and music-related movements) parallel to their increase in leg responses or responses with objects. Staff personnel with work experience in the area rated the program versions used in the 2 studies and their impact on the participants favorably. In light of that mentioned earlier, a number of considerations may be put forward.
First, the data of study 1 represent a direct replication of previous findings concerning the impact of the program on leg responding and positive involvement. 31,32 The levels of responding observed in the study can be taken as a sign of the participants’ comfortableness with the response requirements and possible enjoyment of the intervention sessions. The reason for such an enjoyment was almost certainly the stimulation available for the responses. This stimulation, which was preferred by the participants (ie, as noted during the preliminary screening), apparently contributed to motivate their responding and improve their general involvement and mood. 42,48 –50
Second, while the use of stimulation contingent on leg responses might have been critical in supporting the response engagement of all participants, the reminders might also have had an important role at least for the participants receiving the higher frequencies of these events. 45,49 With regard to the reminders, 2 general points should probably be made here. The first point is that some of the aforementioned participants could be expected to continue their successful leg responding within the program even without reminders, while others might definitely need reminders. The second point is that the reminders are most likely to become necessary also for those participants who presently do not need them, given that their disease will progress and their ability (1) to keep track of stimulus and response events and (2) to make connections between those events will grow increasingly weaker. 2,4,6,21,40,41
Third, the positive results of study 1 may gain extra relevance if one considers that they were obtained with a program relying on rather simple and easily affordable technology. 22,51 Indeed, the hardware components (ie, microswitch with related interface and portable computer) are commercially available and can be readily assembled. The software is specific for the program, but it is quite plain and can be developed by anyone who possesses basic concepts of software engineering. The final cost of the program components would be around or slightly above US$1000. In light of this, one could view the program as a realistic and beneficial tool within daily contexts for people with Alzheimer’s disease and other dementias. Such tool could help staff provide the participants with extra opportunities of positive engagement, thus countering conditions of extended passivity and related physical and psychological risks (eg, reduced body fluids regulation, limited alertness/attention, low environmental stimulation, and poor general mood). 25,52 –58
Fourth, the positive results of study 2 indicate that the technology-aided program used in study 1 could be successfully adapted with new microswitches to help another group of participants engage in activity with objects. These participants could differentiate objects (by shapes or colors) and manipulate them successfully and thus appeared suitable for such type of activity. The successful performance and generally positive involvement of these participants suggest that a fairly simple and affordable technology-aided program ensuring contingent stimulation and response reminders can be used to foster different types of activity across different persons with Alzheimer’s disease characterized by passivity and withdrawal. 23,24,59,60 Future research should continue the assessment of the program with new participants and new activity situations so as to determine its range of applicability. 27,29
Fifth, the positive activity engagement outcomes described earlier, although highly encouraging as to the potential impact of a technology-aided program in daily contexts, could hardly be considered sufficient to guarantee its adoption within those contexts. 32,42 In fact, such an adoption might be based not only on the general effects of the program but also on the way the program is perceived. 42,61 In light of this, the staff rating (ie, social validation assessment) 62 of the program versions used in the 2 studies was viewed as a critical component of the research process. The positive evidence emerging from staff (ie, their relatively high scores across the questionnaire items) could be taken as a sign of the acceptability and possible applicability of both program versions. 61 –63
Sixth, a limitation of the 2 studies reported concerns the exclusive use of 5-minute sessions. In daily contexts, it might be more convenient for caregivers to have longer sessions. One could think of 10- or 15-minute sessions, in which the reminders are presented after 20 to 30 seconds of no responding so as to avoid a large frequency of those events with the risk of them becoming less effective in fostering responding. 45 In those sessions, participants who rely only moderately on reminders may continue to display rather consistent responding. Participants who are more dependent on reminders may have lower, nonetheless relevant, responding rates. Given the practical implications of longer sessions, new research will need to assess their impact and compare it with the impact of shorter sessions such as those used in the present studies. 59 –61
In conclusion, the 2 studies showed that a basic technology-aided program (1) could support mild physical activity/exercise in a group of participants and (2) could be adapted to support simple occupational activity in a second group of participants. The participants’ levels of positive involvement during the intervention sessions and the staff’s favorable scoring of the program were 2 additional, practically relevant, findings. New research needs to confirm all these findings in daily contexts with regular care personnel in charge of the technology and the sessions. 30 –33 New research will also need to (1) evaluate the possibility of using longer sessions, (2) inquire about possible (positive) spillover effects of the sessions, and (3) determine ways of upgrading the technology so as to make it more easily applicable within daily contexts. 48,49,64 –66
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.