
Abstract
Caring for people with dementia in acute settings is challenging and confounded by multiple comorbidities and difficulties transitioning between community and acute care. Recently, there has been an increase in the development and use of integrated care pathways (ICPs) and care bundles for defined illnesses and medical procedures, and these are now being promoted for use in dementia care in acute settings. We present a review of the literature on ICPs and/or care bundles for dementia care in the acute sector. This includes a literature overview including “gray literature” such as relevant websites, reports, and government publications. Taken together, there is clearly a growing interest in and clinical use of ICPs and care bundles for dementia. However, there is currently insufficient evidence to support the effectiveness of ICPs for dementia care in acute settings and limited evidence for care bundles for dementia in this setting.
Background
The incidence of dementia is increasing worldwide and there is an international call for integrated dementia care pathway development. 1,2 “Integrated care pathways (ICPs) are instruments designed to map out the direction of clinical and administrative activities for all care professionals working with a diagnostic specific group.” 3 Individuals with dementia and their family members require access to a number of health-care services. An ICP for dementia could therefore potentially assist in streamlining a system of care to ensure patients with dementia receive equal, effective, evidence-based treatment, and support which is timely and responsive to their individual needs.
Care bundles are a composite of synergistic interventions to improve clinical outcome for a condition, containing a few essential, well-accepted components selected based on best evidence, local considerations, and open to change with time and experience. 4 A care bundle ensures the application of all relevant interventions is consistent for all patients at all times.
Although ICPs and care bundles are recommended to improve outcomes for people with dementia in acute hospitals, the evidence for this approach is unclear. We therefore searched the literature for evidence to answer the research question: what is the effectiveness of ICPs and/or care bundles for dementia care in the acute sector?
Methods
Searches were completed in the following databases: PubMed, and Cinhal and Medline via Ebsco.
Inclusion criteria were articles that reported data on the effectiveness of an ICP and/or care bundle for dementia care in an acute hospital. Exclusion criteria were articles that did not report evidence of effectiveness; articles that reported on a sample, which included people with dementia, but was not limited to people with dementia; articles that focused exclusively on people with young-onset dementia; and articles that focused exclusively on end-of-life care.
The specific search terms used and hits returned can be seen in Table 1. Only 1 paper which met the inclusion criteria was found during this systematic search. The nonacademic gray literature was also searched, using similar search terms, via a Google web search. Following this search, 1 reference was included regarding ICPs (duplicate of the above), as well as 3 nonpeer-reviewed references regarding 2 care bundle interventions.
Details of Systematic Search Strategy.
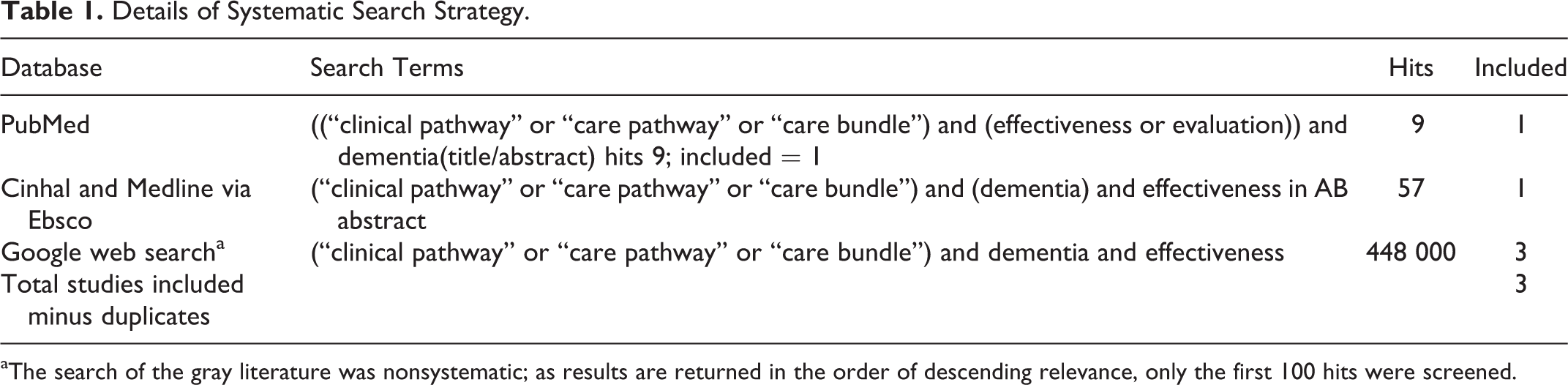
aThe search of the gray literature was nonsystematic; as results are returned in the order of descending relevance, only the first 100 hits were screened.
Due to the limited publications on the effectiveness of ICPs and care bundles, a “literature overview” is presented providing a broader picture of ICPs and care bundles in dementia and other patient groups, followed by the results of the systematic search for papers investigating the effectiveness of these interventions.
Results
Literature Overview
Overview of ICPs and care bundles for dementia care in acute settings
There are some examples of ICPs for dementia such as the National Institute of Health and Clinical Excellence (NICE), 5 the National Health Service (NHS) Forth Valley ICP for Dementia, 6 the Dementia Services Pathway in Australia, 7 and the Dementia Care Pathway in New Zealand. 8 These pathways offer guidance to various multidisciplinary members across a multitude of services, and they include recommendations for acute care. There are also examples of care pathways for dementia with a specific focus on 1 area, such as primary care, 2,9 -11 and end-of-life care. 12 No similar published pathway focusing solely on dementia care in an acute setting was located.
Two comprehensive literature reviews on dementia care in acute hospitals, spanning 1986 to 2013, did not address any research involving dementia ICPs or care bundles. 13,14 There is, however, an increasing onus on acute hospitals to develop and implement ICPs for dementia. 15,16 National hospital audits in Ireland, Northern Ireland, England, and Wales in 2013/2014 found that 5.7% to 36% of acute hospitals self-reported that they had developed or were using an ICP for dementia in their hospital. 17 -19 However, Larner 20 argues that the NICE/Social Care Institute for Excellence guidelines incorrectly imply that dementia is a “unitary, or uniform, condition,” and interpretation of existing ICPs requires careful consideration and cautious judgments on their suitability and feasibility through research. Hughes similarly discussed some of the issues around care pathways for dementia, specifically how individual circumstances influence care choices and consequently recommended general guidelines as opposed to definitive, restrictive pathways for dementia care. 21
There appears to be limited research on the effectiveness of ICPs in general, across settings and diagnoses. Just 7 international randomized controlled trials on ICPs in both adult and pediatric settings were reported by Allen et al, concluding that there has been little economic evaluation of ICP development, implementation, or outcomes. 22 Not all ICPs are beneficial; there is a lack of robust research on the effectiveness of ICPs in end-of-life care. 23 There is also uncertainty surrounding care pathway use for patients with stroke , 24 and ICPs may be more effective when used for routine procedures or in predictable contexts. 22
Integrated care pathway development
Successful ICP development is a process that requires cohesive links between various agencies involved in care provision. Creating good integrated dementia care between various services takes time, continuity of personnel, and shared interests. 25
Developing ICPs is a complex, iterative process guided by in-depth literature reviews, key stakeholder meetings, process mapping, and framework development, with eventual pathway implementation and evaluation. Carer/family members’ needs are often overlooked and should also be considered when developing pathways. 14 Equally, there should be user involvement in developmental stages. 22 Multiple assessment and review points should feature in an ICP for dementia to capture individual requirements as they change over time. 1 Integrated care pathways should be practical, be adaptable to different care contexts, and lead to improved patient, family, and staff outcomes. 14 There must be scope to enter the pathway at any point, and pathways should accommodate complex needs. 22 Additionally, Larner argued for the inclusion of entry referrals for a range of diagnostic services and dismissed the idea of a single point of referral. 20 Thus, a comprehensive ICP for dementia should incorporate the patient’s journey: from assessment and diagnosis, through support in the community, periods in acute care, potential transition to long-term care, and finally in end-of-life care.
The use of care bundles in acute hospitals for other patient groups
There is a possibility that, for acute hospital use, it is more appropriate to develop care bundles, which broadly identify a small set of crucial interventions, for all people with dementia, rather than ICPs. Extensive evidence supports the use of care bundles in hospital settings, including emergency departments (EDs), where they have vastly improved outcomes for patients with community acquired pneumonia and sepsis. 26 Within the Irish ED context, the “sepsis six” care bundle is increasingly incorporated as the standard of care for sepsis. Recent implementation of a chronic obstructive airways disease care bundle in an Irish ED was associated with substantial care improvements including fewer unnecessary interventions. 27 Focusing on older patients, 1 US study demonstrated that a targeted care bundle approach for high-risk older patients on discharge from medical wards reduced ED readmission. 4 Recently, the implementation of a care bundle for delirium identification and prevention, for older inpatients on medical and surgical wards in a Boston hospital, resulted in less antipsychotic medications and morphine prescribing and less frequent discharge to long-term care. 28
Care bundles for dementia have gained attention in recent years. In 2013, the Royal College of Nursing in the United Kingdom published a guidance document; “Dementia; Commitment to Care for People with Dementia in the Acute Hospital” and identified 5 main principles to improve care for patients with dementia, with the mnemonic “SPACE”; (1) Staff who are skilled and have time to care, (2) Partnership working with carers, (3) Assessment and early identification, (4) Care that is individualized, and (5) Environments that are dementia friendly. 16
A person with dementia may require care using one or more care bundles. For example, there are recommendations in the NHS Forth Valley ICP 6 to initiate a falls prevention care bundle when people with dementia are admitted to acute care settings, suggesting that the initiation of a number of pertinent care bundles may be relevant for people with dementia in the acute sector. The implementation and feasibility of this in clinical practice require some consideration.
Systematic Search Results
Evidence to support the effectiveness of ICPs for dementia in acute hospitals
Only 1 small prospective study has examined the effectiveness of a care pathway. Twenty-three patients with dementia received care using the care pathway, and 20 controls received usual care in an acute hospital in Japan. 25 Patients were recruited consecutively on presentation to a dementia ward over a 3-month period; the first 20 patients were assigned to the control group. The pathway incorporated diagnosis, treatment, and development of a care system and caregiver education. Its effectiveness was evaluated by comparing the length of stay and hospital costs between the groups. The findings showed that the pathway contributed to increased caregiver understanding and facilitated medical practice by supporting “the flow of medical treatment” and through supporting the development of a care system post discharge. Length of stay was significantly shorter in the care pathway group (25.3 vs 31.2 days) and hospital costs were therefore significantly less for this group (US$4767 vs US$5435 per patient). Questionnaires were completed by an unspecified number of caregivers, doctors, and nurses. Medical staff felt that the pathway limited their ability to choose alternative treatment methods and increased their daily workload. This was a small, nonrandomized study, and larger, robust studies are necessary to support these findings.
Evidence to support the use of dementia care bundles in acute hospitals
In Suffolk, an action learning project to improve dementia care identified 7 key recommendations for acute hospitals. 29 These were (1) “consistent use of This is Me booklet (written account of personal information about the person with dementia to inform health-care providers), (2) assessment and planning of needs of carers and people being cared for together in primary and secondary care, (3) include patients and primary carers in all consultations by NHS staff in clinics, during primary care visits, and throughout acute adult and mental health care, (4) promoting an open approach to care by copying all discharge, clinic, and referral letters to patients, (5) creating and piloting systems that provide safe and improved access of principal carers to acute services, allowing them greater access during ward rounds, case conferences, and meal times, (6) resolving issues related to emergency pressures created by ward closures, the resultant exclusion of carers, and the impact of this on people with dementia, and (7) promoting staff knowledge and understanding of dementia.” All of the recommendations were implemented with reported immediate benefits for people with dementia, with more primary carer involvement and reduced patient anxiety. 29 However, it is not clear how the outcome data were gathered and therefore how robust the findings of this project are.
The Royal Wolverhampton Hospitals NHS Trust developed a care bundle for dementia containing the following elements: (1) communication, (2) nutrition and hydration, and (3) the environment. The care bundle was supported with an “about me” document, a specialist dementia ward, outreach team, volunteers, staff training and development, a dementia-friendly environment, integrated dementia pathway, and organizational leadership and commitment to implementing excellence in dementia care. Relevant data were collected through staff interviews, questionnaires, clinical data (such as patient weights and incidence of catheterizations), and observations of practice. They found that these initiatives have had beneficial outcomes including improved personalized care for patients with dementia in the acute setting, less bed moves, better nutrition, reduced falls incidence, and increased satisfaction among patients and their carers and staff. 30,31 However, no raw data, statistical differences, or effect sizes were reported; hence, it is not possible to ascertain whether these improvements were statistically significant.
Conclusion
The extent to which ICPs for dementia improve outcomes or reduce costs are not clearly known. There is a lack of research into the effectiveness of ICPs in the acute settings, and the single study that evaluated such an ICP was a small prospective study. There are criticisms of ICP use in some complex care groups, such as stroke and the care of dying patients, and most of the evidence for ICPs comes from use in routine or predictable patient groups. However, ICP development is a potential means of improving care, enabling existing services to work in a more unified way. People with dementia entering the pathway at any stage will receive a set of interventions, assessments, supports, and treatments that are evidence based and targeted to meet their individual requirements. This could have a positive effect on the person, their family, and medical and support staff experiences. Overall, standardizing timely assessments, diagnostic and follow-up processes, streamlining transparent support services, providing evidence-based guidelines on best practice, and improving the transition between community and acute care could have a positive impact on care provision for people with dementia. Whether an ICP for dementia can direct this streamlined care process is yet to be evaluated.
Given that there is currently little evidence available to support the use of ICPs in acute hospitals, the next consideration was whether care bundles for dementia, possibly within an ICP framework to guide care provision, could be effective in the acute hospital setting. Although it has been found that care bundles have substantially improved outcomes in other patient groups, and there is growing recognition of their benefits for use in dementia care, there is little research as yet into their effectiveness for dementia care. The results from the 2 case studies reported here are promising, but they do not provide sufficient evidence to support the use of care bundles for patients in hospital with dementia.
Thus, despite international advances in the development of ICPs for dementia, there has been little research into their benefits, in terms of efficacy, effectiveness, or cost. It is important therefore that studies on the health-care utilization implications and on patient-related outcomes (including family carers) are performed in line with their development.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was performed to inform a Genio/Health Service Executive partnership Quality Improvement Project, and was supported by the Atlantic Philanthropies.