
Abstract
This study tested the effect of written emotional expression on the ability to find meaning in caregiving and the effects of finding meaning on emotional state and psychological burden in 91 dementia family caregivers. In a pretest–posttest design, participants were randomly assigned to either an experimental or a comparison group. Experimental caregivers (n = 57) wrote about their deepest thoughts and feelings about caring for a family member with dementia, whereas those in the comparison group (n = 34) wrote about nonemotional topics. Results showed enhanced meaning-making abilities in experimental participants relative to comparison participants, particularly for those who used more positive emotion words. Improved meaning-making ability was in turn associated with psychological benefits at posttest, but experimental participants did not show significantly more benefit than comparison participants. We explore the mediating roles of the meaning-making process as well as some of the background characteristics of the individual caregivers and their caregiving environments.
Keywords
Introduction
Alzheimer’s disease has been described as the “most terrifying illness on the face of the earth.” 1 According to Alzheimer’s Disease International, 2 there are almost 47 million people with dementia worldwide, and this number is expected to almost triple by 2050, to an estimated 132 million. On average, people with Alzheimer’s disease live about 8 years from the onset of symptoms but can live up to 20 years. 3 It is the sixth leading cause of death, 3 but it is the chronicity of the disease that results in its most significant societal and personal impact. Most persons with dementia are cared for in their own homes by family members and other unpaid caregivers. Because dementia often progresses slowly, a third of caregivers provide care for 5 years or longer. While caring for a family member with dementia can be a satisfying experience, it can also be associated with a host of physical, emotional, and financial demands that may compromise the health and well-being of the caregiver. Due to their care recipient’s progressive loss of memory and judgment, difficulties in communicating, and changes in personality, family caregivers eventually need to provide help with even the most basic activities of daily living. And, as the illness progresses, caregivers are often required to manage difficult behaviors in the care recipient, such as disorientation, wandering, agitation and hostility, socially inappropriate behavior, and incontinence.
Negative health consequences of caregiving have long been documented by dementia researchers and include both physical and psychological symptoms. Seventy percent of caregivers reported a decline in physical health because of their support role. 4 Caregivers also report more chronic illnesses 5 as well as a higher prevalence of physical symptoms, poorer self-ratings of health than noncaregivers, and poorer overall health than a matched group of noncaregivers. 6
Dementia caregivers also report poorer mental health than the general population, and the mental health status for unpaid family caregivers is significantly lower than for paid caregivers. 7,8 Almost 90% of caregivers for persons with dementia report fatigue, anger, and depression directly due to the demands of caregiving. 9 A meta-analysis of 31 caregiver studies led Schulz and Williamson 10 to conclude that family dementia caregivers experienced substantially elevated rates of clinical depression compared to population norms. The more severely impaired the family member with dementia, the greater the depressive symptomatology in caregivers. 11 Caregivers of persons with dementia report higher levels of burden than noncaregivers, 12,13 and research has linked dementia caregiving to exhaustion and social isolation, 14 economic hardship, 15 and family conflict. 16 In the first study to show caregiving as an independent risk factor for mortality, Schulz and Beach 13 reported that caregivers expressing strain had mortality rates 63% higher than noncaregivers.
Significant distress in caregivers may have a negative impact on the caregiver’s ability to care for the persons with dementia. 17 Dunkin and Anderson-Hanley 18 found that the physical health of and burden experienced by the caregiver were stronger predictors of the care recipient’s subsequent institutionalization than variables associated with the care recipient himself or herself. The health consequences of caregiving on the caregiver create a critical need to “find new ways to improve families’ ability to better manage their everyday care responsibilities, reduce their own burdens and health risks, and promote a better quality of life for both older adults receiving care and the family members providing it.” 19 (p6) Since dementia caregivers are often living at home with the care recipient, effective interventions designed to reduce caregiver stress and burden that can be implemented in the home environment have even greater relevance. To this end, the purpose of this study was to test a structured version of written emotional expression (SWEE). The intervention is designed to decrease the physical and emotional stresses and burdens experienced by dementia family caregivers by having participants write about their deepest thoughts and feelings about their experiences while caring for a family member with dementia.
Structured Written Emotional Expression
Structured version of written emotional expression is an effective and efficient intervention that involves asking participants to write brief accounts expressing their deepest thoughts and feelings about a stressful topic. Controlled studies have found significant health benefits of SWEE, including reduced stress, enhanced physical health, increased immune function, reduced time in medical visits, and improved mood or affect. 20 -25 Empirical studies have documented the effectiveness of written emotional expression in a wide range of populations, including students dealing with the stress of entering college 26 as well as those coping with a variety of medical conditions, such as cancer, 27 rheumatoid arthritis, 28 and cystic fibrosis, 29 and adjustment difficulties in American veterans returning from wars in Afghanistan and Iraq. 30
Meta-analyses support the conclusion of SWEE’s wide-ranging efficacy. Smyth’s meta-analysis 31 of 13 studies found a significant and positive effect size of r = .230, whereas Frisina et al’s 32 meta-analysis of 9 experimental studies in clinical populations resulted in an effect size of r = .101. In Frattaroli’s 33 comprehensive meta-analysis of 146 randomized experimental studies, written emotional expression was found to produce significant health benefits with an overall effect size of r = .075, including reduced stress, decreased depression, improved immune function, and improved cognitive function. Not all studies have shown a significant benefit, but Frattaroli documented that 70% (102) of the studies she reviewed showed a positive effect. Together, the meta-analyses suggest that written emotional expression works most of the time, and while effective sizes in the range of 0.075 to 0.230 may be modest, expressive writing provides an easily administered and cost-effective option.
In order to help clarify how written expression exerts its effects on long-term physiological and psychological health and to provide a means to efficiently examine the narratives generated in studies of emotional expression, Pennebaker et al 34 developed the Linguistic Inquiry and Word Count (LIWC) computer-based text analysis program. The LIWC is an automated method of counting words in specific semantic and syntactic categories (eg, words conveying affect or causal relationships). Pennebaker and colleagues report that the use of affective words and certain “cognitive mechanics” words, such as causal words (eg, because, effect) and insight words (eg, think, consider), result in greater health improvements. 35,36
Despite the plethora of SWEE studies, only a couple have examined the impact of SWEE on reducing stress and burden in caregivers. Schwartz and Drotar 37 tested written emotional expression in family caregivers of children with chronic illness. Four months after the intervention, they found no psychological benefits in the group writing about their deepest thoughts and feelings relative to a group writing about activities from the previous summer. The authors suggested that the caregivers may have been too distressed to benefit from the intervention, particularly since most of them carried out the writing in their child’s hospital room. Mackenzie et al 38 compared primary caregivers of adults attending a day program who were assigned to 1 of 3 writing groups: expressive emotional writing, time management (how they spend their time), or history writing (an important world event). A month after the intervention, the authors found no beneficial effects of SWEE. Only participants in the time management condition showed positive changes. The authors proposed that, whereas the expressive writing focused on negative emotions and “unmanageable sources of stress,” the time management condition may have fostered “a form of problem-focused coping that allowed participants to view their demanding care responsibilities in a manageable way.” 38 (p304) Both of these studies emphasize the need for a better understanding of the cognitive and affective mechanisms underlying the SWEE intervention for caregivers in order to maximize its likelihood of success. Many caregivers already seem to be aware of the potential healing powers of written emotional expression. There are a multitude of memoirs written by caregivers about their experience of caring for a family member with Alzheimer’s disease. A quick search on Amazon.com for the specific phrase “Alzheimer’s disease caregiver memoirs” yielded 67 results. We aim to investigate how such writing benefits caregivers of those with Alzheimer’s disease by examining the role played by the ability to find meaning in caregiving, a form of “problem-focused coping.” Our conceptual approach is outlined below. We aim to contribute to this effort by examining the role played by the ability to find meaning in caregiving, a form of “problem-focused coping.” Our conceptual approach is outlined below.
Conceptual Framework
The purpose of this randomized controlled trial was to test the effectiveness of SWEE in enhancing the experience of caregiving among family caregivers of persons diagnosed with dementia. We based our framework on Noonan’s and Tennstedt’s 39 caregiving stress process model, which outlines the relationships among background or contextual variables, stressors, mediators, and outcomes. Background/contextual variables include demographic and environmental characteristics of the caregiver and the care recipient; stressors are the problematic conditions and difficult circumstances experienced by caregivers; outcomes refer to the consequences of stressors on health and well-being; mediators are the social and emotional resources that modify or regulate the relationship between contextual variables and stressors/facilitators on one hand and outcomes on the other.
Consistent with this model, the most common explanation for why written emotional writing can lead to health outcomes is the cognitive-processing theory, which proposes that the act of writing helps to organize and integrate a source of stress or a traumatic experience into one’s self-schema. 40 -44 The linguistic representation enables the caregiver to gain perspective about the experience through a process of cognitive reorganization. Noonan and Tennstedt 39 suggest that the management of meaning is a strategy for coping by searching for a larger understanding of the illness. Thus, the SWEE intervention in this study was postulated to enhance the ability to make meaning and thereby mediate the promotion of health benefits in caregivers.
Figure 1 illustrates our adaptation of the Noonan and Tennstedt 39 model. We include facilitators and stressors, where facilitators are factors that may ameliorate aspects of caregiving, such as the availability of support systems. We also combine the background/contextual and stressor/facilitator categories, since background/contextual variables may act as stressors or facilitators. The model includes a variety of factors that have the potential to act as stressors or facilitators on coping resources and responses. However, in this study, we selected just 3 of these to focus on, one from each of the subcategories of demographic characteristics, care recipient factors, and environmental factors. These factors were selected based on their hypothesized effect on coping: older caregivers may find it more difficult to adapt to the requirements of caregiving because of their own increasing health needs; the number of hours of care required may stress the ability to cope; on the other hand, the availability of support (in particular, perceived support) may free up coping resources. Coping resources consisted of preexisting psychological status and the ability to find meaning in caregiving (both self-reported), whereas coping responses were reflected as changes in the ability to find meaning following the intervention. Measured outcomes were changes in self-reported symptoms of depression and caregiver burden across the course of the study. The SWEE intervention itself is hypothesized to mediate the health outcomes by improving the ability to manage the meaning of caregiving. In particular, the use of affect words and cognitive mechanics words is hypothesized to underlie the effectiveness of the SWEE intervention.
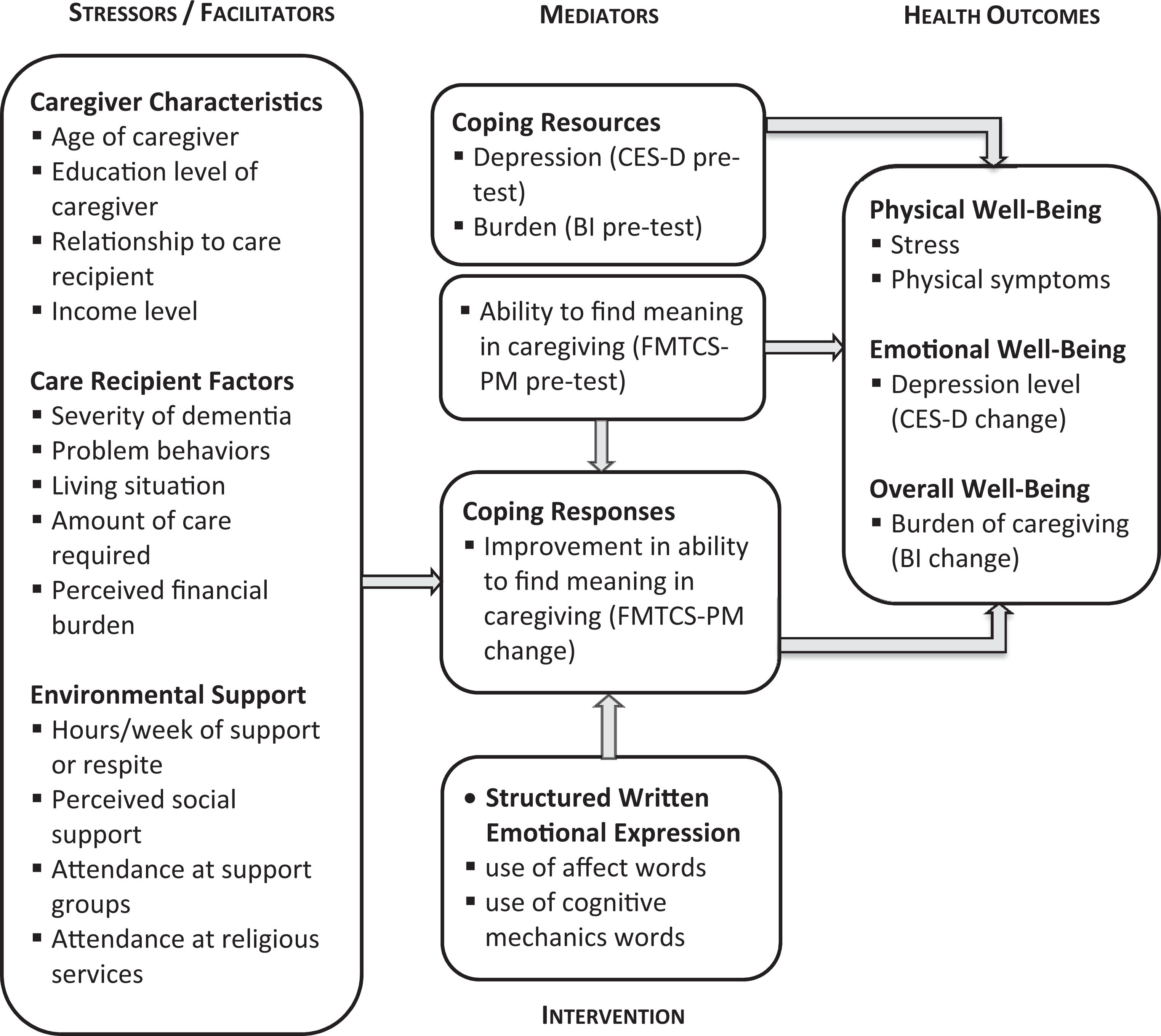
Conceptual model of factors affecting health outcomes. Adapted from Noonan and Tennstedt. 39
Methods
The SWEE intervention was tested in 2 different studies, which had identical designs but different methods of administration. In the first study, the researcher administered the pre- and posttests and provided instructions for the intervention in person at the caregivers’ homes. In the second study, pre- and posttests and the intervention were administered via a dedicated website that allowed us to capture a larger and more diverse sample of caregivers. Both studies were approved by the institutional review board of University of Iowa.
Participants
Family caregivers of individuals with dementia were recruited. By “family caregivers,” we refer to caregivers who provided unpaid care to someone with whom they shared a social or familial relationship. The vast majority of caregivers in the study were spouses or offspring of the care recipient. For the in-person study, participants were recruited through newspaper ads, caregiver support groups, and the UI’s Seniors Together in Aging Research registry. For the online study, participants were recruited through Alzheimer’s Association and caregiver support group websites, National Alzheimer Association chapters, newspapers ads, and TrialMatch, a registry for clinical trials with people who have Alzheimer’s disease.
Inclusionary criteria for both studies were that the caregiver must be 18 years of age or older; able to read and write in English; currently caring for someone who has been diagnosed by a physician as having Alzheimer’s disease, vascular, or a mixed type of dementia; unpaid for the care they provide; and the person who spends the most time helping the care recipient (at least 4 hours per day). In addition, participants in the online study had to be computer literate and be able to connect to the Internet using a home computer. Exclusionary criteria were having a serious illness requiring hospitalization or extended rest in the last 3 months or having depression or anxiety requiring the use of medications. A total of 139 participants were recruited, of which 98 completed the study: 49 for the in-person study (44 completed) and 90 for the online study (54 completed). Of those who completed the online study, 7 were excluded because they reported providing fewer than 4 hours per day of care. To achieve sufficient power, we combined data from the 2 studies, resulting in 91 participants altogether, 57 in the experimental (SWEE) and 34 in the comparison groups. Characteristics of the final groups are shown in Table 1.
Participant Characteristics by Group.
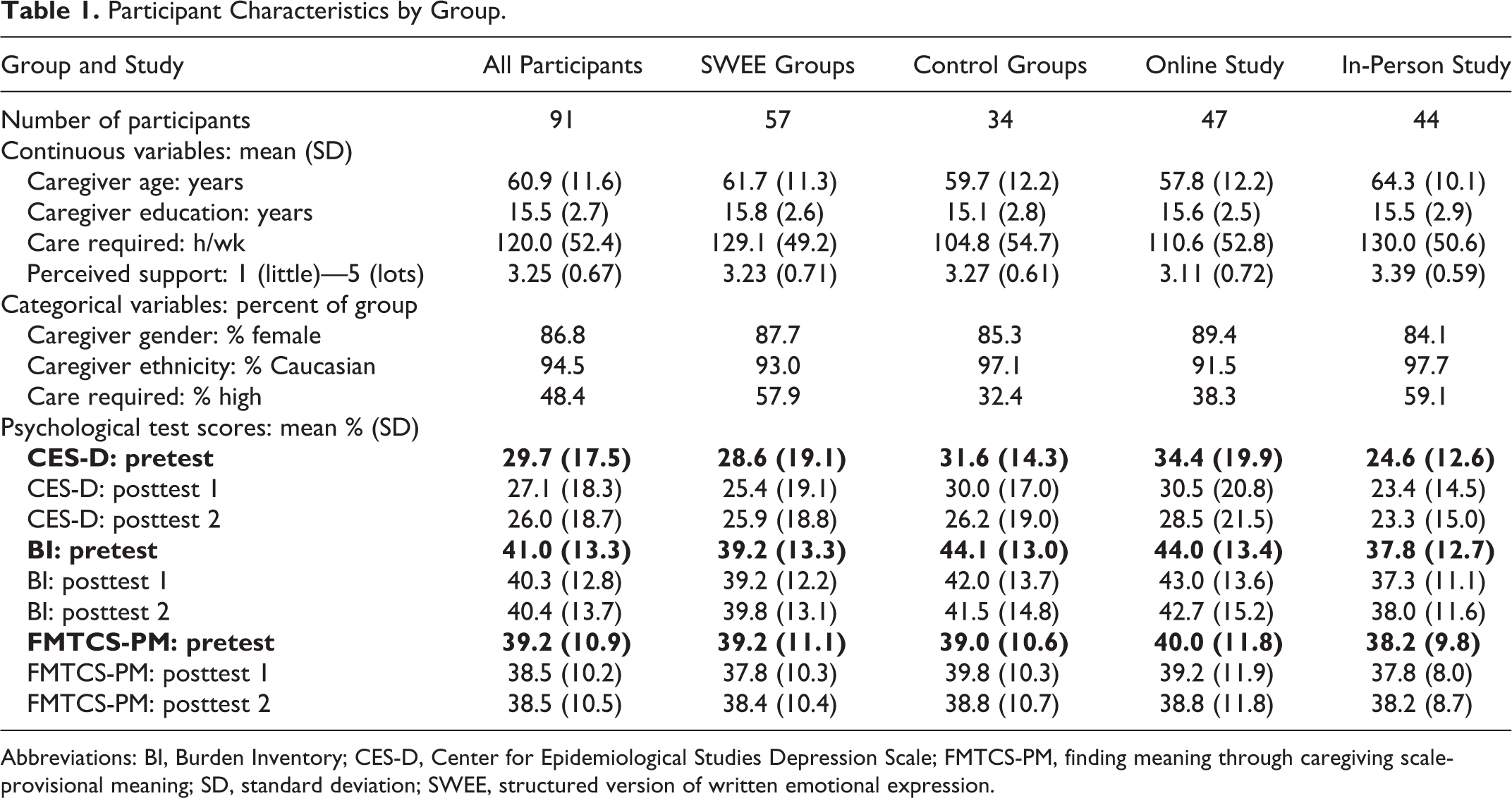
Abbreviations: BI, Burden Inventory; CES-D, Center for Epidemiological Studies Depression Scale; FMTCS-PM, finding meaning through caregiving scale-provisional meaning; SD, standard deviation; SWEE, structured version of written emotional expression.
Study Design and Procedures
In both the in-person and online versions of the study, participants were randomly assigned to either the SWEE or the comparison groups. Within a week after completing the consent form and the pretest measures, the participants underwent their first day of writing. Three writing sessions were scheduled every other day (days 1, 3, and 5) in order to reduce the risk of fatigue and provide extra time to integrate and gain insight about their caregiving experience. 31,33 Participants completed posttesting on the sixth and/or seventh days following the first writing session and a month after the final writing session.
Participants in both studies were given exactly the same writing instructions for each of the 3 writing sessions. Both groups were instructed to write continuously for 20 minutes during each session and to ensure that they were not interrupted. They were told to write without being concerned about grammar, spelling, or sentence structure. In the SWEE groups, family caregivers were asked to write about their deepest emotional thoughts and feelings about caring for a loved one, family member, or friend. They were assured that their writing would be anonymous. Caregivers in the comparison groups were asked to write about neutral topics related to their everyday activities (session 1: nutrition and food preparation; session 2: medications and vitamins; session 3: leisure and physical activities). For each session, participants were asked to be as objective and detailed as possible and not to write about their emotions.
Data Collection
Information on stressors and facilitators was gathered through a questionnaire. The factors assessed in the current study were caregiver age (in years), hours of care required per week, and perceived social support. Caregiver age was reported in years and was analyzed below as a continuous variable. Hours of care per week was reported as a raw value but subsequently dichotomized into a group reporting a high load (≥112 hours per week, or 16 hours per day, n = 59) and a group reporting relatively low-to-moderate care loads (<112 hours of care provided per week, n = 32). The value of 112 hours represents 16 waking hours a day, 7 days a week, which we felt was a more meaningful division than the median of 140 hours per week. Perceived support was scored by participants by endorsing several statements (eg, The people close to you let you know that they care about you; You have someone whom you feel you can trust) on a 4-point scale (1 = strongly disagree; 4 = strongly agree). These scores were averaged and then dichotomized using the median of the 5-point rating scale into those who perceived moderate levels of support (<3.4, n = 43) and those who perceived high levels of support (>3.4, n = 48).
To reflect coping resources and coping response, participants filled out the Finding Meaning through Caregiving Scale (FMTCS) 45 before and after the intervention. Unlike other scales designed to measure meaning, the FMTCS is specific to dementia caregiving. This measure has 3 subscales: (a) loss/powerlessness, (b) provisional meaning (PM), and (c) ultimate meaning. The PM subscale is the scale that we expected would be most sensitive to the SWEE intervention, since PM refers to those transitory experiences that give meaning to life. 46 The items on the PM subscale reflect caregivers’ day-to-day positive experiences with caregiving, such as “caregiving makes me feel good that I am helping” and “I am glad I am here to care for my relative.” Each item is scored on a scale of 1 (strongly agree) to 5 (strongly disagree), with higher scores (more disagreement) reflecting less meaning-making ability. Thus, the direction of the scale corresponds to the other 2 instruments, in that higher scores are less desirable outcomes.
Two outcomes measures were selected to reflect caregiver well-being before and after the intervention. The Center for Epidemiological Studies Depression Scale 47 is a self-report scale of symptoms of depression. Higher scores represent greater levels of depression, and scores over 16 differentiating depressed from nondepressed community-residing adults. The Burden Inventory 48 is a self-report scale designed to assess the extent to which caregivers of elderly and disabled persons perceive their roles and responsibilities as burdensome. Higher scores signify higher levels of burden.
Analysis Approach
The analyses outlined below follow the logic laid out in the model depicted in Figure 1. First, we tested the validity of the intervention by comparing the types of words used by the SWEE and comparison groups. Next, we assessed the impact of 3 sets of hypothesized contributors to changes in the ability to find meaning in caregiving, our index of coping response. The first set consisted of coping resources, indexed here by pretest scores on the FMTCS-PM measure. The second set consisted of the SWEE intervention itself: the contrast of SWEE and comparison groups and the LIWC measures that differentiated the SWEE and comparison groups. The third set included the 3 selected background variables hypothesized to act as stressors or facilitators (caregiver age, care load, and perceived support). After having determined which of these factors influenced the ability to find meaning (FMTCS-PM change scores), we examined whether those changes in turn affected health outcomes (CESD or Burden Inventory [BI] scores) and whether this relationship differed for the comparison and SWEE groups. Statistical analyses were conducted using STATISTICA 10. 49
Results
Testing the Validity of the Intervention
To assess whether the SWEE intervention succeeded in promoting emotional expression and reflection, we used Linguistic Inquiry Word Count 34 to compare the narratives of each group. It was hypothesized that caregivers in the SWEE groups, instructed to write about their deepest thoughts and feelings, would produce more affect words, conveying both positive emotion (eg, hope, worthwhile, lucky) and negative emotion (eg, distress, hate, scary), than would caregivers in the comparison groups. Furthermore, under the hypothesis that emotional expression increases the cognitive processing of stressors, we predicted that the SWEE groups would produce more words in cognitive process categories, specifically insight words (eg, consider, meaning, understand) and causal words (eg, because, depend, purpose). To balance these hypotheses, we also included 3 LIWC word categories hypothesized to be produced more by the comparison groups: ingestion words (corresponding to the topic of nutrition and food preparation), health words (topic: medications and vitamins), and leisure words (topic: leisure and physical activities).
A 3-way analysis of variance tested the effects of 2 between-group factors—group (SWEE vs comparison) and study (in-person vs online)—and 1 within-group factor—word category (the 7 categories described above)—on the proportion of words produced. There was no significant main effect of study or interactions of study with the other variables, illustrating that findings were consistent across online and in-person administrations, so this variable was removed from the model. In the final model, significant main effects (all P values <0.001) were found for both group (η2 p = .293) and word category (η2 p = .337), as well as an interaction between group and category (η2 p = .613). These findings, shown in Figure 2, illustrate that the SWEE groups produced more emotion words (both positive and negative) and more insight words than the comparison groups. The proportion of causal words was not significantly different. The difference was greater for negative emotion words (P < .001) than for positive emotion (P < .01) words, which is not surprising, given the topic. By contrast, the comparison participants produced significantly more words than the experiment participants in each of the health, ingestion, and leisure categories.
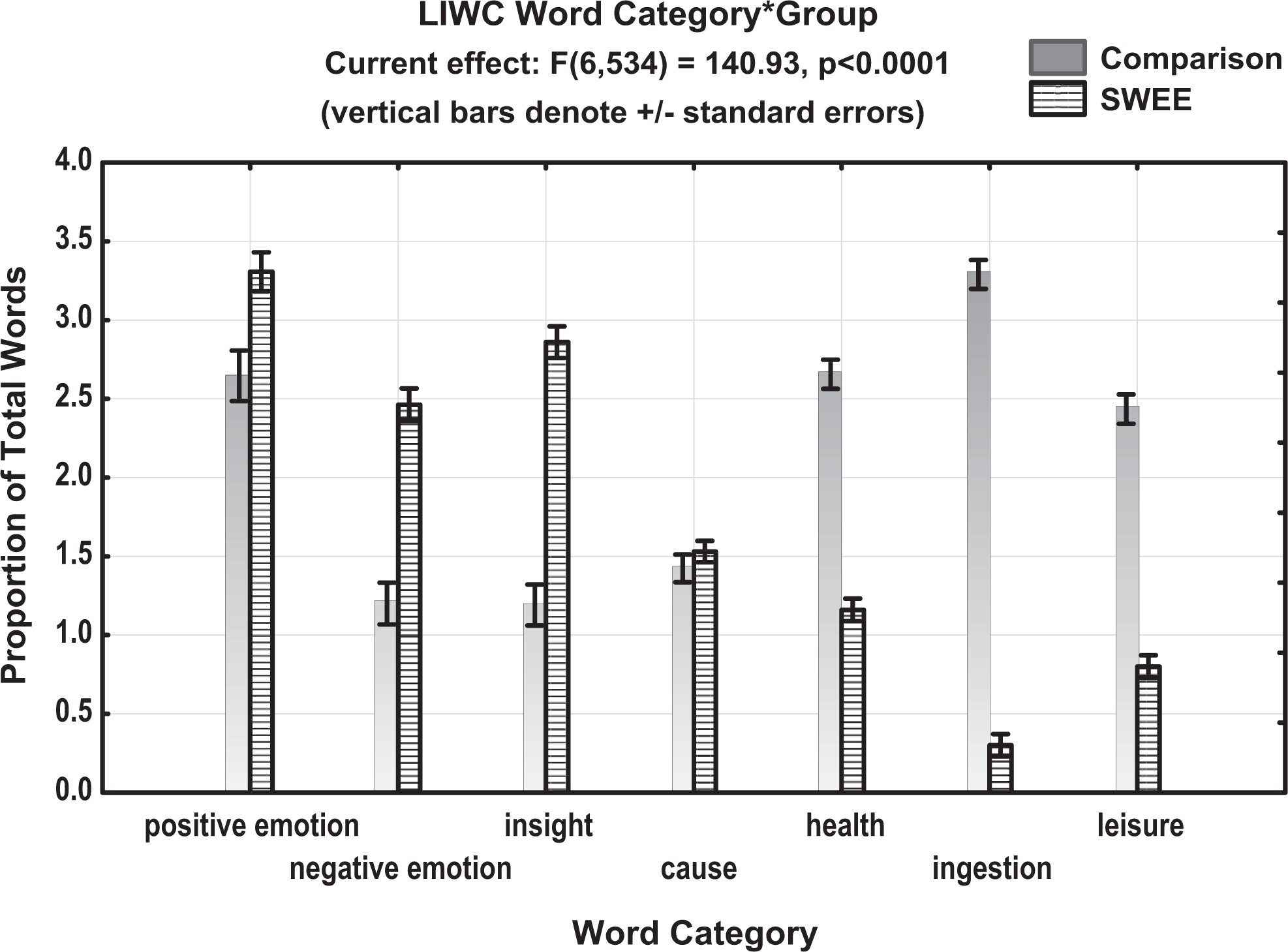
Word production in selected categories by structured version of written emotional expression (SWEE) and comparison participants.
Testing the Efficacy of the Intervention
First, we converted the scores on each psychometric measure (FMTCS, CES-D, and BI) to a percentage of the total possible points in order to place the different measures on the same scale. To compensate for initial group differences, we used change scores as our outcome measures and included the initial scores on each measure as covariates in the relevant models. Change scores were calculated by subtracting postintervention scores from preintervention scores, such that a positive change indicates a reduction in depressive symptoms or burden or an increase in meaning-making ability.
Factors affecting coping response (meaning-making)
A series of repeated-measures analyses of covariance (ANCOVAs) were conducted to examine the factors influencing changes in the ability to find meaning in caregiving, beginning with coping resources and the intervention, then examining stressors/facilitators to the model. Change in FMTCS-PM scores at posttest 1 and posttest 2 was the repeated dependent measure. The primary independent factor of interest was group (SWEE vs comparison): a main effect of group would indicate that the SWEE intervention was effective in facilitating meaning-making. As above, we also included study (in-person vs online), and the interaction between group and study, to determine whether changes in finding meaning depended on the administration method. The FMTCS-PM pretest scores were included as a covariate, following our hypothesis that this reflected initial coping resources. We also included as covariates the 3 word categories found to differentiate between the SWEE and comparison groups that are hypothesized to underlie the effectiveness of the SWEE intervention (positive emotion, negative emotion, insight) and the interactions of each of these with the group factor. Nonsignificant interactions, then main effects, were removed one by one according to their P values (highest P values removed first). To the remaining effects, we then added the stressor/facilitator factors: caregiver age, the amount of care required, and the amount of perceived support available. Each factor was crossed with group to test for differential effects attributable to the intervention. Again, nonsignificant interactions, then main effects, were removed to arrive at a final model.
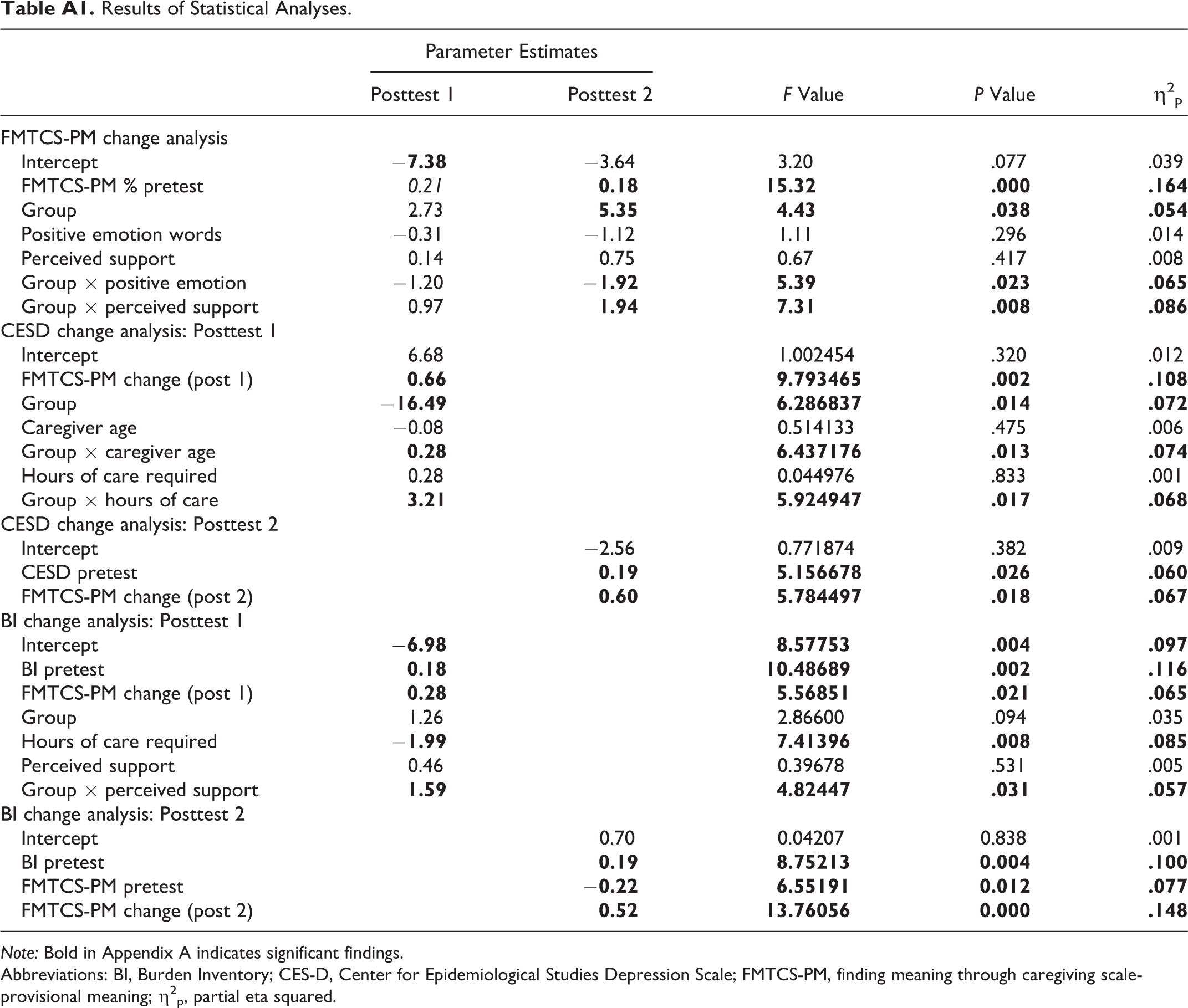
Table A1 shows the significant effects remaining in the final model. An improvement in PM scores was facilitated by having higher PM scores at pretest (P = .0002, η2 p = .164). In other words, the better able participants were at finding meaning initially, the more change they made over the course of the study, regardless of whether they were in the SWEE or comparison groups. A small but significant main effect of group was also found, such that SWEE participants showed greater improvement in PM scores than comparison participants (P = .038, η2 p = .054). The group effect was moderated, however, by the use of positive emotion words (P = .023, η2 p = .065). This interaction is illustrated in Figure 3, which shows that the use of positive emotion words is positively associated (albeit weakly) with greater change in PM scores for the SWEE groups. By contrast, for the comparison groups, the association is negative. Because the comparison participants were not writing about caregiving, this counter-intuitive finding is difficult to interpret, although it may be driven in part by the restricted range of positive emotion word use by the comparison participants relative to the SWEE group. A significant contribution to PM change scores was also found for the interaction between group and the degree of available support perceived by the caregivers (P = .008, η2 p = .086). As illustrated in Figure 4, the interaction arises because a higher level of support is associated with more positive change in PM scores for the SWEE group but not for the comparison group.
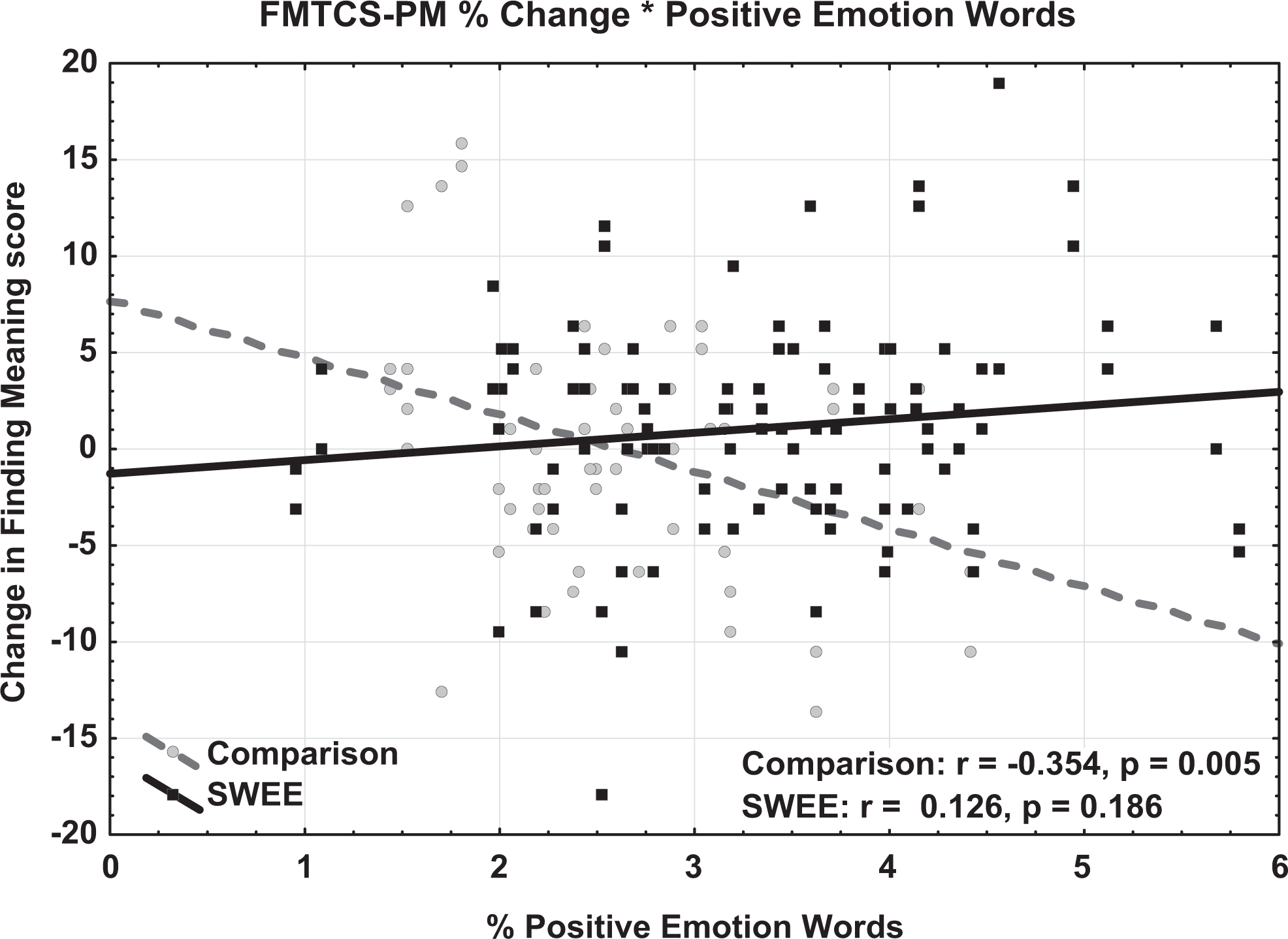
Effect of positive emotion words on change in provisional meaning scores.
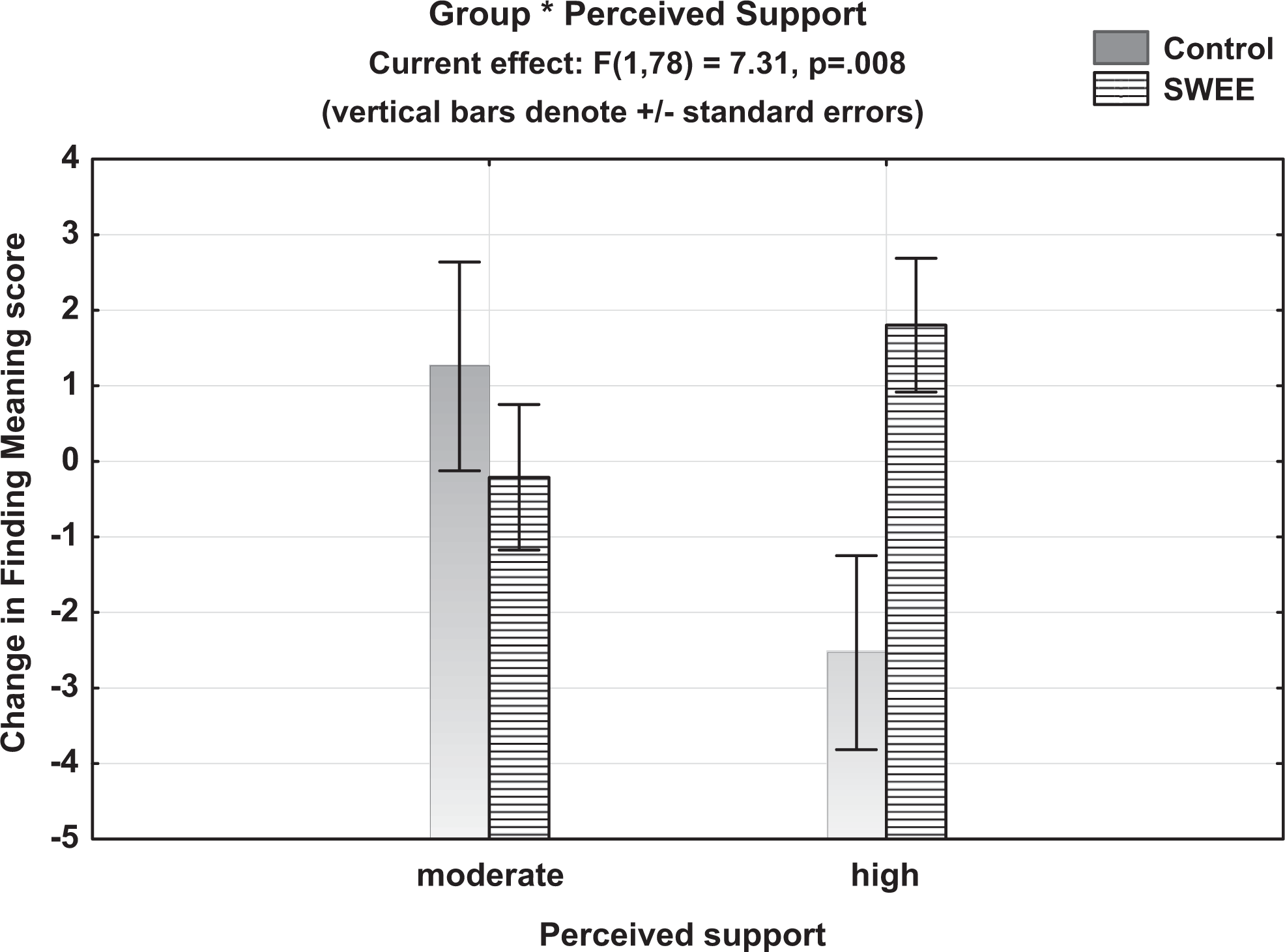
Interaction between group and perceived support on change in provisional meaning scores.
Factors affecting psychological well-being
For each outcome measure (CES-D and BI), we again conducted a series of ANCOVAs on the change scores at posttest 1 and posttest 2. As in the previous analysis, we included group (SWEE vs comparison) as the primary factor of interest, study (in-person vs online), and the interaction between group and study. As a covariate for each measure, we included pretest scores of the measure in question (ie, CES-D pretest for the analysis of CES-D change scores; BI pretest for the analysis of BI change scores), expressed as a percentage of the total possible points on the measure, and pretest scores of the Finding Meaning PM subscale. To test our hypothesis that a change in the ability to find meaning would moderate any psychological benefits, the change scores of the PM subscale were also included in each analysis and the interaction of PM change scores with group. This necessitated analyzing each posttest separately, since the PM change scores at posttest 1 were used to predict CES-D/BI outcomes at posttest 1 and the PM change scores at posttest 2 to predict outcomes at posttest 2. In each successive model, only significant contributors were retained. Then the ANCOVAs were rerun to test for any additional influence of the 3 stressors/facilitators outlined above.
Results of the CES-D analyses are shown in Appendix A. Across groups, PM change scores significantly predicted CES-D change scores at posttest 1 (P = .002, η2 p = .108), with a greater change on the PM scale (improved finding meaning) resulting in greater change in CES-D scores (reduced depression). In addition, group interacted with caregiver age: for the SWEE groups but not the comparison groups, older caregivers showed less change in depression scores (see Figure 5). An interaction was also found between group and hours of care provided. As shown in Figure 6, the SWEE participants who had high care loads showed more improvement in depression scores than those with lower care loads, whereas the opposite pattern was shown for comparison participants. At posttest 2, only CES-D pretest scores (P = .026, η2 p = .060) and PM change scores from posttest 2 (P = .018, η2 p = .067) predicted change in depression scores.
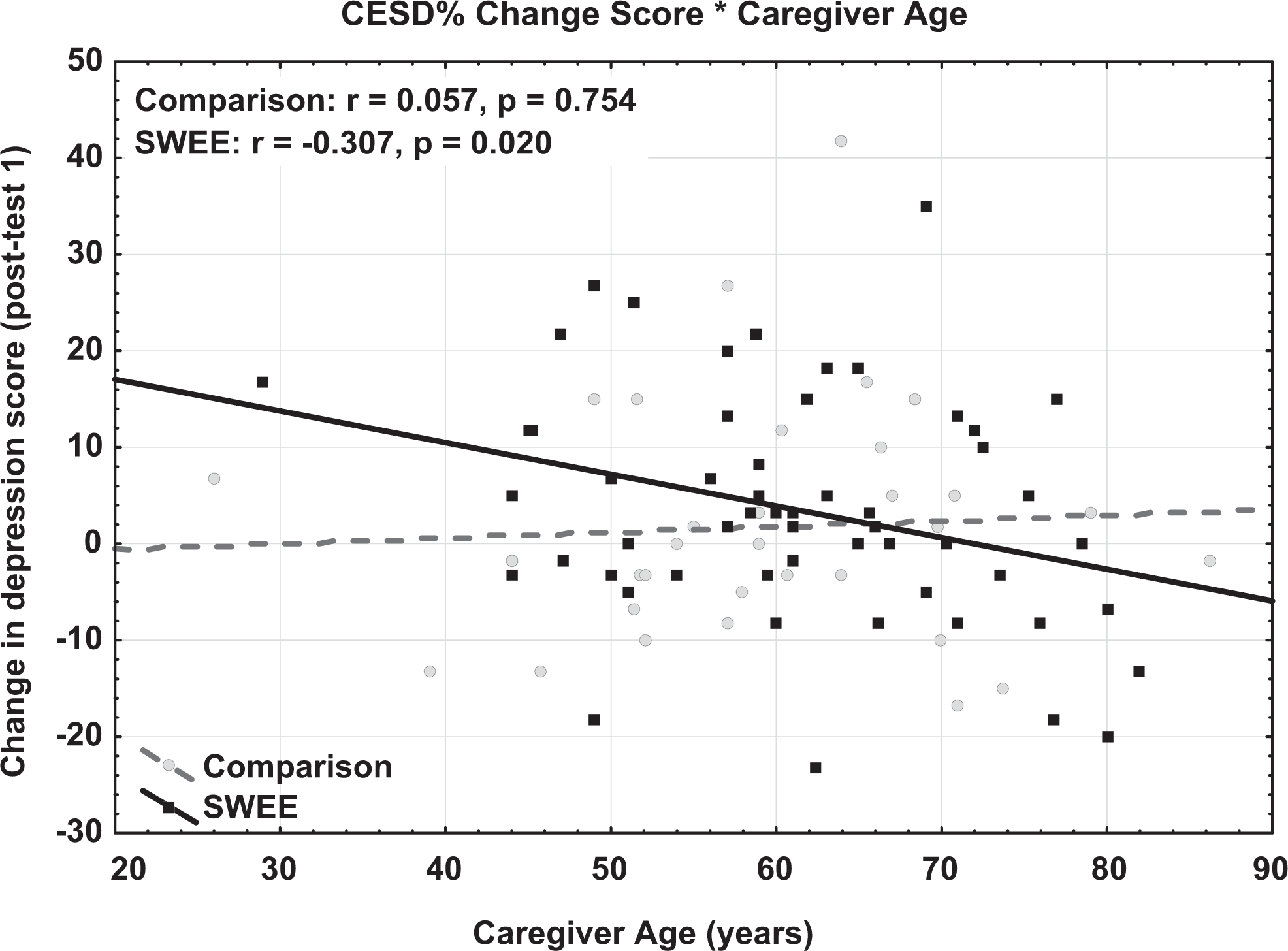
Interaction between caregiver age and group on change in CESD scores at posttest 1.
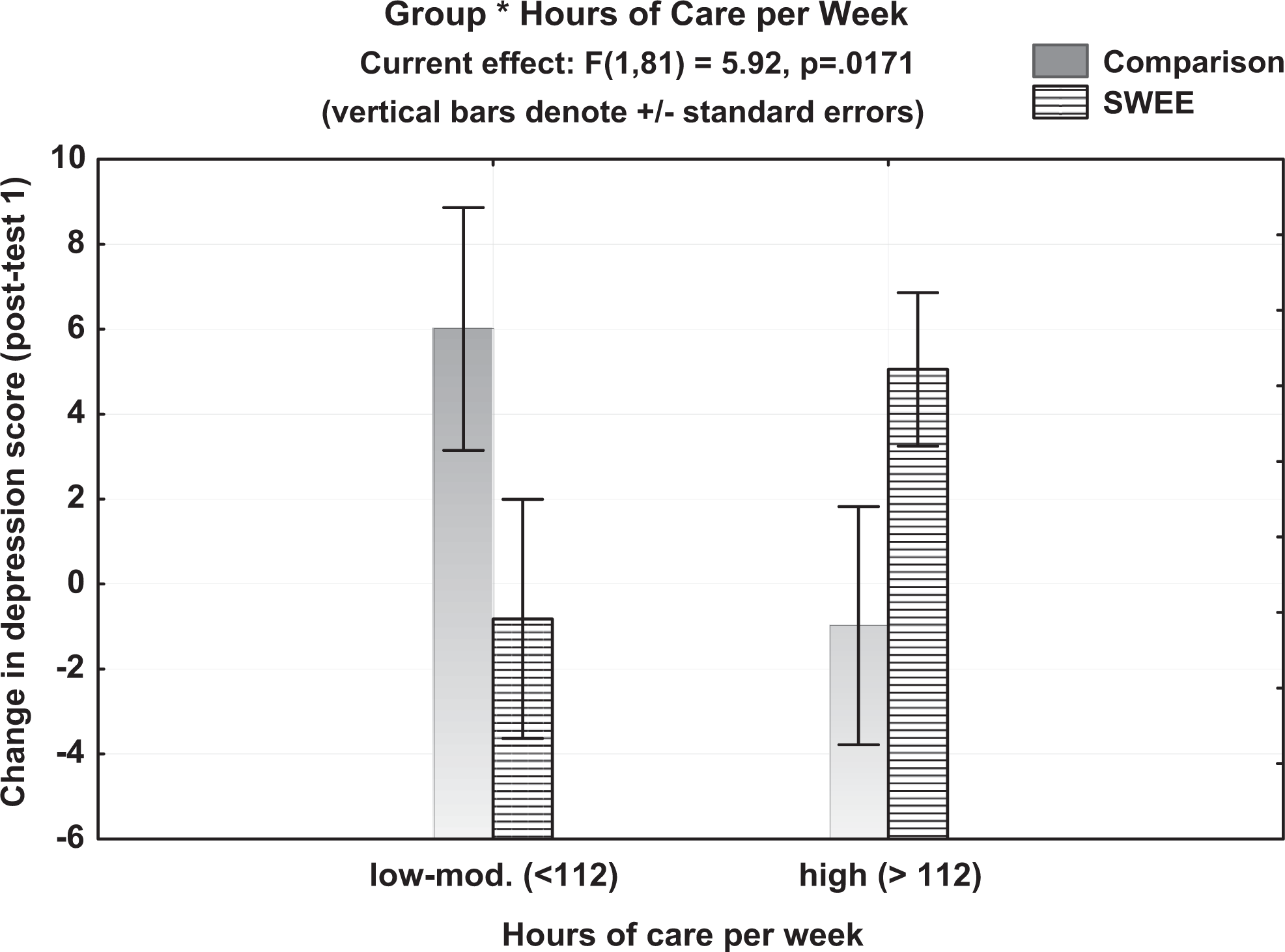
Interaction between care load and group on change in depression scores at posttest 1.
Our final analysis assessed change in BI scores at each posttest. As shown in Appendix A, at both posttests, significant effects were found for BI pretest scores (posttest 1: P = .002, η2 p = .116; posttest 2: P = .004, η2 p = .100) and PM change scores (posttest 1: P = .021, η2 p = .065; posttest 2: P = .0004, η2 p = .148), such that higher initial scores were associated with a greater reduction in burden. In addition, PM pretest scores contributed to change in burden scores at posttest 2 (P = .012, η2 p = .077). Both amount of care required and amount of perceived support affected change in burden at the first posttest. Burden was reduced more for individuals who provided a high level of care across the 2 groups (P = .0008, η2 p = .085). The effect of perceived support was moderated by group (P = .031, η2 p = .057); in the SWEE groups, caregivers who reported a higher degree of support showed a reduction in burden, whereas those reporting less support showed an increase in burden. In the comparison groups, those reporting less support showed a greater reduction in burden.
Discussion
In this study, we examined the effects of SWEE on 3 psychological measures (FMTC-PM, CES-D, and BI) self-reported by caregivers of individuals with dementia. Two studies—one administered in person, the other online—were conducted, and their data combined. The method of administration did not significantly affect the results, attesting to the feasibility of a novel online approach. Our analysis followed a conceptual model adapted from Noonan and Tennstedt, 39 which proposes a mediating role on psychological outcomes (measured here by the CES-D and the BI) for coping resources and responses. The focus here was on the mediating effects of the ability to find meaning in caregiving (measured here by the FMTC-PM).
Results showed that the SWEE intervention had the desired effect of promoting the disclosure of emotions to a significantly greater degree by SWEE than comparison participants. In addition, SWEE writers produced more insight words, suggesting that they were cognitively processing their emotions. In the next step, we found that the intervention fostered changes in the ability to find meaning. Participants in the SWEE groups, particularly those producing more positive emotion words, showed more growth than participants in the comparison groups in finding meaning scores at posttest. It is notable that although the SWEE and comparison groups were more clearly differentiated by the use of insight words and negative emotion words, it was the use of positive emotion words that contributed to the ability to find meaning.
These findings lend support to previous work attesting to the idea that linguistic processing of positive emotions underlies the effectiveness of written emotional expression by promoting the ability to find meaning from the emotional situation or event. Pennebaker and Chung 50 reported that the health of participants from a variety of populations improved more when they used more positive emotion words in writing about emotionally laden topics. On the other hand, negative emotion word use showed a curvilinear relationship to health change: those who used a moderate number of negative emotion words showed the greatest health benefits. One interpretation of this, offered by Pennebaker and Chung, 50 was that those who use many negative emotion words may be simply repeating negative feelings without resolving their feelings about the experience, while those who use few negative words may be repressing their emotions.
Our results provide only indirect evidence for the cognitive-processing model of SWEE, which proposes that participants make sense of an event by gaining insight. 51 Although we found that SWEE participants did produce more insight words, this difference did not contribute to changes in meaning-making. Ullrich and Lutgendorf 51 assessed the awareness of positive benefits of writing about trauma in students randomly assigned to 1 of 3 writing conditions: focusing on emotions related to a trauma or stressor, focusing on both emotions and cognitive processing of the trauma/stressor, or writing factually about media events. They found significant change in only the emotion and cognition group and suggested that engagement of both is necessary to foster a positive awareness. However, our results suggest that emotional expression may be sufficient to promote meaning-making for dementia caregivers writing about the caregiving experience. Of course, it is also possible that the count of insight words in our samples was not sensitive enough to adequately capture cognitive reorganization processes in our participants. Another possibility is that change in cognitive processing over time is more important than a single measure. Pennebaker and Chung 50 proposed that health benefits are greatest in people who move from using fewer to more insight and causal words throughout the course of their writing. This possibility could be assessed in future by analyzing the successive writing sessions separately. 52 -55
A consistent finding across the analyses assessing the outcome of the intervention was that psychological functioning at pretest appears to affect the potential for change: finding meaning pretest scores influenced change in finding meaning scores at posttest; depression pretest scores influenced change in depression scores (although this was only significant at posttest 2); burden pretest scores influenced change in burden scores at both posttests. This may simply be because participants with higher initial scores (greater disagreement with finding meaning statements; more symptoms of depression and burden) had more room to improve. In any case, it does illustrate the need to consider initial scores when evaluating change in these measures.
Our results also provide evidence that change in the ability to find meaning in caregiving is an important predictor of change in psychological well-being in this population. Specifically, increases in the ability to find meaning were associated with reductions in self-reported symptoms of both depression and burden. Although we found greater change in finding meaning scores for the SWEE group, the impact of changes in meaning-making on psychological outcomes did not differ by group. Thus, improvements in finding meaning, although facilitated by SWEE, cannot be attributed solely to SWEE.
What prompted these changes, if not the SWEE intervention? It may be that the writing intervention induces some psychological change, regardless of whether participants were in the SWEE or comparison groups. Such a placebo effect could arise from just being in a study that focuses participants’ attention on caregiving, or from the act of writing itself, regardless of the intended topic. Some evidence for this comes from our informal observations that participants in the comparison groups often expressed thoughts and feelings about caregiving, despite instructions to write objectively about neutral topics. Here are a few examples of comparison participants discussing food preparation, medications, and leisure activities: Well … for an objective topic, it’s amazing how much emotion surrounds the topic of food.… Maybe this is the way I see every chore, no matter how trivial, these days. She can’t control her wants or her spending, we always overspend when we go [shopping]. Yet it’s one of her very few pleasures and I feel bad denying her. No one told me how bad and constant the guilt would be—wish there was a medication for that! What is a leisure activity when you’re on stage 24/7 with an Alzheimer’s disease patient?
There were also some stressors and facilitators that directly affected the outcomes. For the psychometric measures (BI and CESD), these effects were only evident at posttest 1 and appear to have faded by the second posttest 2 a month later. In particular, a reduction in caregiver burden (BI) was more likely for individuals providing a more hours of care per week, regardless of group. A reduction in depressive symptoms (CESD) was also more likely for those with a high care load but only in the SWEE group. This may indicate that those who bear a greater caregiving burden are more in need of, and more susceptible to, interventions. If we entertain the possibility that some placebo effect was at work in the comparison group, this explanation may also have affected those assigned to write about neutral topics to some degree. The amount of support perceived to be available also affected outcomes differentially for the groups. For the SWEE group, those with more perceived support reported better finding meaning and burden scores at posttest than those with only moderate perceived support. There is evidence from other populations that the ongoing construction of meaning is related to social support among elderly people. 51 Researchers have found that providing social support to bereaved individuals can facilitate a meaning reconstruction process by providing emotional support and acceptance, offering different perspectives, and listening to survivors’ stories. 53-55
Our findings lend support to a number of previous findings regarding the mechanisms underlying SWEE, particularly the important role identified here for finding meaning in caregiving. Nevertheless, the SWEE manipulation did not translate to group differences in psychological well-being, as measured by the depression scale and the BI. Despite the large number of previous studies showing positive health effects of SWEE, such results are not uncommon. As Frattaroli 33 pointed out, effect sizes tend to be small and dependent on a variety of methodological factors. One of these is sample size, and our groups were just large enough to provide the power we estimated would be necessary to show effects. Another factor is the short time frame over which change is measured, although Frattaroli’s 33 meta-analysis showed that effect sizes on psychological outcome measures were greater in studies that followed participants less than 1 month after disclosure compared to those that followed participants for at least 1 month.
A more likely explanation is the nature of the participants. Caring for someone with dementia is an ever-present and increasingly burdensome source of stress, and the prospect for change has declined. Two previous studies which also involved caregivers 37,38 did not show significant effects of SWEE, as discussed earlier. Both proposed that benefit was hindered by a level of stress that did not seem to be remediable by expression alone. Mackenzie and colleagues 38 proposed that a more problem-focused approach would be effective, while our own results suggest that written expression is most effective in a context of high-perceived support. Perhaps combining SWEE with a more professionally guided and individualized psychological intervention focusing on potential coping mechanisms would maximize the meaning-making process, thereby enhancing its translation to psychological well-being. Support may also be provided by booster SWEE sessions at periodic intervals. This study demonstrates that improvement in the ability to extract meaning from caregiving appears to be crucial to the efficacy of the SWEE intervention. Such coping resources may be particularly important for caregivers of adults with dementia, who must continually adapt to new challenges as the dementia progresses. This enhanced meaning-making ability is, we propose, what prompts the desire in caregivers to write memoirs. However, our results also suggest that more may be needed to translate enhanced meaning into enhanced psychological well-being. Perhaps the meaning of the caregiving experience only becomes truly beneficial when shared with others in the caregiving community.
Footnotes
Appendix A
Results of Statistical Analyses.
| Parameter Estimates | F Value | P Value | η2 p | ||
|---|---|---|---|---|---|
| Posttest 1 | Posttest 2 | ||||
| FMTCS-PM change analysis | |||||
| Intercept |
|
−3.64 | 3.20 | .077 | .039 |
| FMTCS-PM % pretest | 0.21 |
|
|
|
|
| Group | 2.73 |
|
|
|
|
| Positive emotion words | −0.31 | −1.12 | 1.11 | .296 | .014 |
| Perceived support | 0.14 | 0.75 | 0.67 | .417 | .008 |
| Group × positive emotion | −1.20 |
|
|
|
|
| Group × perceived support | 0.97 |
|
|
|
|
| CESD change analysis: Posttest 1 | |||||
| Intercept | 6.68 | 1.002454 | .320 | .012 | |
| FMTCS-PM change (post 1) |
|
|
|
|
|
| Group |
|
|
|
|
|
| Caregiver age | −0.08 | 0.514133 | .475 | .006 | |
| Group × caregiver age |
|
|
|
|
|
| Hours of care required | 0.28 | 0.044976 | .833 | .001 | |
| Group × hours of care |
|
|
|
|
|
| CESD change analysis: Posttest 2 | |||||
| Intercept | −2.56 | 0.771874 | .382 | .009 | |
| CESD pretest |
|
|
|
|
|
| FMTCS-PM change (post 2) |
|
|
|
|
|
| BI change analysis: Posttest 1 | |||||
| Intercept |
|
|
|
|
|
| BI pretest |
|
|
|
|
|
| FMTCS-PM change (post 1) |
|
|
|
|
|
| Group | 1.26 | 2.86600 | .094 | .035 | |
| Hours of care required |
|
|
|
|
|
| Perceived support | 0.46 | 0.39678 | .531 | .005 | |
| Group × perceived support |
|
|
|
|
|
| BI change analysis: Posttest 2 | |||||
| Intercept | 0.70 | 0.04207 | 0.838 | .001 | |
| BI pretest |
|
|
|
|
|
| FMTCS-PM pretest |
|
|
|
|
|
| FMTCS-PM change (post 2) |
|
|
|
|
|
Note: Bold in Appendix A indicates significant findings.
Abbreviations: BI, Burden Inventory; CES-D, Center for Epidemiological Studies Depression Scale; FMTCS-PM, finding meaning through caregiving scale-provisional meaning; η2 p, partial eta squared.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by funds from the National Institute of Nursing Research #1R15NR8213-01; the John A. Hartford Foundation Building Academic Geriatric Nursing Capacity Claire M. Fagin Post-Doctoral Scholars Program; The University of Iowa Informatics Initiative Grant; and an Interdisciplinary Research Grant from the Obermann Center for Advanced Studies at the University of Iowa.