
Abstract
Dementia family caregivers display significant rates of psychological and physical symptoms. African Americans (AAs) are disproportionately affected by dementia. African American caregivers display unique patterns of symptomology and responses to interventions designed to promote caregiver well-being. This study analyzed qualitative focus group data from 32 AA caregivers to explore how issues of race and culture may be incorporated into a culturally sensitive intervention for AA dementia family caregivers. Caregivers were asked scripted questions about their caregiving experiences and to suggest alterations to an existing psychoeducation program. Analysis revealed 4 key themes: the tradition of family care, caregiving and caregiving issues, culturally appropriate care, and navigating without a map. Suggestions for an educational program included a focus on developing caregiver skills and knowledge for caregiving, promotion of self-care, and reflection on the AA family and community as resources for care.
Alzheimer’s disease (AD) affects approximately 5.3 million Americans and is a major contributor to morbidity and mortality in older adults. 1 –3 Approximately 11% of Americans older than 65 years have the disease, a figure that grows to 32% among those older than 85 years. As the baby boomer generation ages and life expectancies lengthen, Alzheimer’s prevalence is likely to grow to about 15 million in the United States. 1 It also now seems clear that African Americans (AAs) have an elevated risk of developing Alzheimer’s compared to older caucasians 1,4,5 ; it appears, too, that AAs live longer with their disease than those in other races. 6
Most Alzheimer’s care is provided at home by family members, 1 often at the expense of caregivers’ own health and well-being, as manifested in significant rates of psychological and physical health problems. 7 Caregiver well-being may vary along racial/ethnic lines, 8 although there are mixed findings regarding AA caregivers’ experience of stress, burden, depression, and anxiety. A number of seminal studies report that AA caregivers experience lower levels of psychological distress and burden compared with caucasian counterparts; 9 –18 however, other, mostly more recent, studies indicate that AA caregivers experience depression and anxiety at rates similar to other groups. 19 –23 Qualitative examinations of the impact of dementia caregiving among AA caregivers paint a more nuanced picture, suggesting that frustrations and difficulties are prevalent though not frequently voiced and that social circumstances, such as living arrangements, may influence affective symptoms. 24 –27
African American caregivers may have unique needs in terms of planning for and enacting the caregiver role. In addition to possible differences in perception of and responses to the challenges of caregiving, AA caregivers demonstrate different patterns of health-seeking behavior and responses to interventions aimed at promoting caregiver well-being compared to those from other groups. Older AAs utilize fewer formal health care services and depend more on home care than caucasian counterparts. 28,29 A major psychosocial intervention trial comparing AA, Hispanic/Latino, and caucasian caregivers found that only Latino and caucasian groups showed an overall improvement in quality of life (in terms of depression, burden, self-care, social support, and care recipient problem behaviors). 30,31 Compared to other racial groups, AAs show unique patterns of responses moderated by different personal characteristics. 32
This study reports on focus group examinations of the needs and experiences of AA dementia family caregivers. Although previous studies have indicated that differences in the caregiving experience appear to occur along racial lines and some work has attempted to elucidate the nature of those differences, there is currently a paucity of work to attend to these differences in the design of interventions. To date, we know of no intervention designed specifically to address the AA caregiving experience. The present study sought to address this gap by examining, through qualitative methods, whether and in what ways issues of race and culture might be incorporated in an educational intervention designed for AA family dementia caregivers.
Method
To gain a fuller understanding of AA dementia family caregivers’ experiences and learning needs, a series of 4 focus group conversations were held with 32 AA caregivers. Led by one of the authors (MP), the groups interactively examined the concerns and experiences of these caregivers and probed for information about participants’ needs and preferences for information, education, and support. The focus groups were part of a larger institutional review board-approved project aimed at developing and testing a culturally appropriate psychoeducation program to promote health and well-being in AA caregivers.
Participants were recruited, in the main, through the “Registry for Remembrance,” a community–academic partnership that seeks to improve the rates of participation of AAs in studies at the Alzheimer’s Disease Research Center of Emory University. One of the authors (MP) heads the Registry for Remembrance, a volunteer group that aims to promote more effective brain health and healthy aging education in the AA community and greater participation in Alzheimer’s research by AA individuals. These efforts included contacts at the Wesley Woods Geriatric and neurology clinics at Emory University, presentations to community groups, use of media materials in parish bulletins and health fairs, and other networking activities.
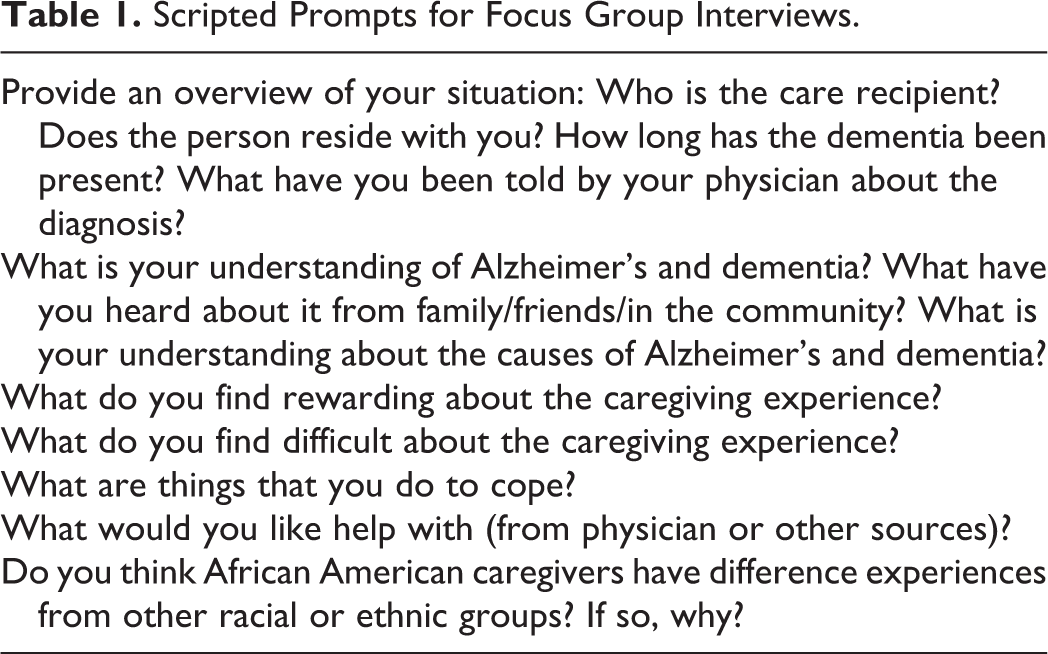
Participants were included on the basis of self-identification as AA and having current or past experience caring for a family member with Alzheimer’s or a related form of dementia and the ability to communicate in English. We did not include persons with sensory deficits that would limit or preclude participation. Participants were given a US$25 honorarium for their participation. The focus groups, held in a conference room at a geriatric care facility, were semistructured (see Table 1), audiotaped, and transcribed.
Scripted Prompts for Focus Group Interviews.
This was a grounded theory study that utilized constant comparison 18 to analyze transcripts from the focus groups. This analytic technique uses inductive reasoning to find meaningful categories in text and then to draw relationships between and among the categories. In this method, texts are read repeatedly in such a way that initial impressions are generated from the reading of a first text (here the first transcript) and represented as coding categories. These codes are applied in the reading of subsequent texts, but the experience of reading these texts produces new and may modify or expand the original codes. The original text is reread in the light of these new and/or modified codes, and the process continues until a final set of codes and themes can be fit to the entire set of texts. In the present investigation, an independent coder (ZS) read through focus group transcripts, identifying and giving names (codes) to text in which specific caregiving concerns and learning needs were expressed. Similar codes were grouped into categories, these, in turn, were grouped into broader themes, and specific examples were identified to illustrate the themes. A second independent coder (KH) then repeated the above process. The coders met after each transcript was coded, compared codes and themes, and arrived at a common understanding in any instances of differences of coding or interpretation. The coding of successive transcripts was informed by existing codes and themes, but newly emerging codes and themes were also used to reexamine previously coded transcripts. The preliminary results of this process were then reviewed by the 2 other authors (MP and CD), both of whom were involved in the focus groups and the development and testing of the resulting educational program. Their review and comments further elucidated the themes that emerged from analysis.
In our analysis, we followed agreed-upon procedures (independent coding of the transcribed audiotapes of the focus groups by 2 authors (ZS and KH) and a review of the codes and findings by the other authors [MP and CD]). Although we did not conduct follow-up groups with focus group participants to assess the credibility of our findings, 2 of the authors (MP and CD) have discussed the themes and the way in which they informed the subsequent educational program. These conversations have yielded general concurrence with the findings and the direction of the program. These conversations also corroborate that this work offers a glimpse of some of the social aspects of caregiving uniquely experienced by AA caregivers (eg, strong expectations of family care and stigma associated with nonfamily care) as well as the emotional impact of caregiving (at times guilt and strain and at other times reward and gratitude). The quotations chosen for inclusion are intended to represent the fit between the themes settled on in our analysis and the stated experience of participating AA caregivers.
Results
Four focus groups were conducted over the course of 2 months in 2009. All but 4 of the 32 participants were female, all were AA, and all were spouse or child caregivers; no additional demographic data were collected. Several key themes emerged from the analysis of the focus group transcripts that revealed issues pertinent to the AA dementia caregiving experience and highlighted the needs of caregivers.
A Tradition of Family Care
The cultural roots of family care and sense of stigma associated with using alternate forms of care, such as institutional care or assistance from a nonfamily caregiver, were repeatedly expressed linked themes. Family care for elders was described as a significant part of AA culture and family life: “Your family raised you to take care of you and … you know, yourself and your family.” Family care was the norm: “ … culturally … you took care of your parents at home; you never put a person in an institution.” Family care is understood as a fundamental, obligatory, and inviolable social exchange.
Caregivers expressed appreciation for the adversity that older AA generations had to overcome to achieve their dignity. They linked the importance of maintaining that hard-fought dignity with maintaining elders at home. I know everybody else [other groups] loves their family and they want [to maintain their] dignity too. But you’ve fought so long to get what you have and you wanna sort of keep it. And I want her to have dignity too as she wants it. [S]he fought hard to get her house and to you know, pay off her house and to have what she has and … I just think that’s part of what we have to deal with when we care for our parents and part of the African American culture. I had my mother go to a nursing home with her first stroke … and had she not gone she probably would have never walked again. Am I not being sensitive about my mother because I’m not really taking care of her[?] I know better than that but I still take some of that stuff on … although I know I’m doing the best I can do. [T]he struggle of African American caregivers as opposed to [others] is that we were brought up seeing the grandmother, grandfather … just extended family living under one room. And … we want to keep those values and keep that … tradition … We don’t have that opportunity to stay at home, so more of us are out working. So then, we’re stressed and we’re feeling … going through the grief process and guilty that I can’t take care of mom and I can’t take care of dad. I don’t have a problem with my mother eventually having to go into a home because all my sister and I want is for the best for her, … but in our communities it is sometimes looked upon as you are throwing her away. With African Americans there is guilt associated with even thinking about institutionalizing … But there is guilt associated with anything other than basically taking your parents into your home and taking care of them for the rest of their lives. [I] feel very blessed that I do not have to have her live with me. I don’t think I could be as good a caregiver if I didn’t have my own, my own space. I’m ashamed to say it, but that’s the way I feel.
Caregiving and Caregiving Issues
Participants reflected on their own caregiving experiences. The title of “caregiver” is not well-recognized in the AA community. The career of caregiving tends to unfold gradually. So many in our community if you ask if they are a caregiver they’ll respond no. Because the role of a caregiver … what’s a caregiver? They’re taking care of someone but I don’t think they are assigning themselves that title of caregiver. So, before you can help yourself you have to realize what you are.
Caregivers commented on both the positive and negative aspects of their experiences, expressing feelings of burden as well as physical and emotional strain. The patient’s health was prioritized while there was a tendency for some caregivers to ignore their own health and well-being. Sometimes people don’t even realize it’s affecting them. I mean I’m somebody who is supposed to know and I was driving to work every day crying and I didn’t know why—I was depressed.
Family involvement was described as both helpful and complicated and sometimes unhelpful. Family served as a source of practical and emotional support for some caregivers. Family helped mitigate the burden of caregiving. However, it was mentioned several times that caregivers often felt guilty turning to their families for help and couldn’t always rely on family members for help. As one caregiver put it: So it’s just myself. My daughter is around; she’s a nurse but she works and has her own life. So she will come once and a while and help me with him but other than that I’m the sole provider for him.
The role of the church, a hallmark institution in the AA community, was discussed, sometimes in positive terms, at other times in terms of disappointed expectations. Church played a supportive role for some caregivers, offering emotional and spiritual support, serving as a venue to express one’s feelings, and providing an outlet to cope. It helped some to deal with the “big” questions: why did AD happen to their loved one; might AD happen to me someday; how to accept not understanding everything about AD; and how to prepare for the death of a family member. For some caregivers, church was a unique place of acceptance of and receptiveness to the patient, although some attended church less as the patient’s behavior became more erratic. Others continued to feel welcome in church and found relief when members of their congregation assumed temporary responsibility for the patient. However, others felt that Church could potentially provide additional sources of support, for example, starting senior ministries to assist in elder care, offering day care to allow caregivers to continue to attend church services and activities, and assisting with transportation. One participant described the potential: We have a lot of ministries within the church … we have ministries that go to prison—prison ministries whatever but, that’s an area that I’ve never heard of a church having one called in this area. And uh, that could be a ministry, you know.
Desire for Culturally Appropriate and Familiar Care
When caregivers sought care outside the family, they wanted to be confident that their family members were receiving high-quality and culturally respectful treatment. In some measure, concerns emanated from experiences of racial discrimination that AA families observed in institutional care settings. I know back in the day it was just taboo to talk about it and to even think about putting your parents somewhere. They always stayed at home … And of course, due to the racism thing there wasn’t any facilities for us anyway. The African American thing (sic) did come up when we were choosing some place to go to for day sessions … The thing that attracted me was the first day I visited, um, there was a speaker there from the Tuskegee Airmen. And there was a child’s choir that was coming in … and you know, things were very pretty. The diet, you know … the dishes that … your parents grew up enjoying—that’s another challenge. That affects their health. That affects everything.… So, every part of the culture and the person’s history—especially since they’re so locked into the early parts of their lives in terms of their preferences—becomes critical. [P]erhaps this is why she thinks she is at home because the furniture looks like furniture that most people of their age group would have had. Her dining even … In the mornings when you got there for breakfast there was a nice table set and at one while her name was on the table. I have [a] problem with even other accents. Even though I can find other black caregivers they may be from other countries and the accent difference is very, very critical.
Navigating Without a Map
On reflection, participants were able to identify a wide range of areas in which they found themselves operating without sufficient or adequate information and skills. At a very basic level, participants recognized that they entered the caregiving role not knowing their parents’ wishes. As one noted, “I think that’s a big issue with caregiving for parents … you don’t have those serious conversations with your parents.” Participants agreed that this lack of knowledge of their care recipients’ wishes has generational and cultural roots: In our culture we don’t talk about medical issues—very private. Especially that older generation … that sense of pride keeping everything in and you don’t admit weakness and … you have to always be that person in charge and nobody can do anything for you. You have to have that continuous dialogue with you parents on how are you going to take care of them. What’s the long term outcome.… I think for us we don’t have those conversations with our parents because our parents kind of push us away—“I know what I’m doing. Don’t you worry about it; I got money.” I wish I’d done a living will earlier … I should have. I didn’t face up to it. She won’t do it now it’s too late. But I wish I had been told the importance of doing it. I was still going, oh no, we don’t need that. But I wish I had been told earlier then I would have taken care of it.
One participant indicated “A lot of our families don’t even deal with financial planning—in good times.” A number of participants reported practical problems that resulted from not having had advanced conversations or being able to make informed decisions about important issues. [A]s caregivers we’re not educated in terms of understanding how do you plan economically, how you plan legally. You may have one person that has power of attorney but another person is the executor of the estate and you have all these other issues in terms of handling money, handling legal issues A lot of things were unresolved … before he … got so far. Some decisions could have been made about what to do about land and we never did any of that. We just kind of just let it go. [I]t was really bad including, not keeping up with life insurance policies. It’s a real mess.
As they moved into the caregiving role, participants indicated that advocacy was an important part of the job description. They stressed the importance of learning how to navigate the health care system for their loved one. One participant indicated that the advocacy role included managing interactions with the health care system: I think one other thing that I’ve learned taking care of my grandmother is being an advocate for her … I think that it’s important to understand your rights, the rights of that patient when they are dealing with hospitals and different things like that. If I don’t fight for her and she had to do this herself she wouldn’t get it. [A]lthough you are a professional in the field and you know a lot of information … when it comes your turn it’s like: where is that information. Somehow you can’t seem to pull it up. You can be working in the field … and then when something happens you just don’t know what to do. [W]e’re not always privy to information and we don’t always share information. African Americans don’t always know what’s out there available to us … [T]hey (whites) pass information amongst each other but we tend to hoard things.… [It’s as though] I don’t want to tell them [because they] might take away from mine.
Discussion
This study sought to explore the experiences and the informational and educational needs of AA dementia family caregivers in order to design a culturally appropriate program aimed at strengthening these caregivers’ caregiving activities. Analysis of transcripts from 4 focus groups with caregivers yielded 4 main themes: the tradition of family care, caregiving and caregiving issues, culturally appropriate care, and navigating without a map. These themes are, in many ways, interrelated.
Congruent with previous findings, the tradition of family care is a powerful force for AA dementia family caregivers. These family care norms were described as arising from multiple dimensions of AA history: close-knit family structures with multigenerational households, a culture of self- and intra-family reliance, and responses to the experience of racial discrimination. Caregivers felt strongly about preserving the patient’s dignity and were highly conscious of the discrimination and adversity that elders endured to earn their accomplishments. Accordingly, some positive appraisals of caregiving involved a sense of repayment to a loved one. This mirrors other work that links family obligations and positive appraisals of caregiving 33 and may reflect the importance of providing exemplary care among AA caregivers. 34 This tradition promotes sustained care. Group members’ sentiments surrounding family care are consistent with other work that shows AAs tend to have lower rates of institutionalization 35 and lower desires to institutionalize than caucasians. 36
The tradition of family care also appears to discourage extra-familial sources of care, and breaking the tradition appears to be stigmatized, a possible source of tension and guilt should caregivers’ personal circumstances not permit full-time, at-home caregiving. Thus, even though some caregivers preferred turning to outside sources of care because they felt it would enable them to be better caregivers, they still either admitted to feeling guilty or were cognizant of the expectation of guilt. Previous work suggests that among AA caregivers, the ability to provide exemplary care (ie, care beyond what is just adequate, involving meaningful social interactions and promoting dignity) promotes continuation of family-based care. 36 It is not surprising that within our sample, decisions to use outside care were discussed in terms of ability to be better caregivers. Still, this rationale could not completely ameliorate guilt that seemed inherent in the decision to utilize nonfamily care. It is possible that decisions to utilize alternate care sources challenged assumptions of one’s place in the family and was perceived as disrupting family structures.
At least among those interviewed, caregiver was not perceived as something much different from “family member.” It was not that caregiving was an “unexpected career 37 ;” it was more that it was an unacknowledged role. Participants endorsed the positive value of this construction in promoting continuity of care for persons living with dementia and they affirmed that caring for their elders provided rewards. At the same time, however, participants indicated that this caregiving norm had downsides. Consistent with other qualitative findings, recognizing and admitting that the day-to-day tasks of caregiving could be frustrating or that acknowledging negative feelings, such as depression, were difficult. Such admissions might be seen as being disloyal or indications of being ungrateful. 24 Likewise, the norm appears to promote the isolation of the “one” who finds herself (generally) in the role of caregiver and also makes it more difficult to ask for help from within the family, let alone from outside the family.
The theme related to culturally appropriate care appears to reinforce the themes of family and family caregiving and it also underscores the importance of person-centered care endorsed by these caregivers. Again consistent with other qualitative findings, caregivers’ observations about the care needs of their family members reflect both their own interactions with systems of care that might be helpful in the situation and the earlier experiences of their family members in a de facto segregated society. 26,38 Comments about the importance of family members’ preferences for familiar foods, music, furnishings, language, values and traditions, and people who looked like them reflect a person-centered sensitivity but also emphasize the difficulties of accommodating these preferences in the larger system of care. Thus, not only are there strong gravitational pulls to keep things close to home and community, there are experiential and historical factors that limit the options caregivers feel they have for obtaining outside care.
The fourth major theme, Navigating Without a Map, revealed another dimension within which AA dementia family caregivers might feel isolated, and this, too, reinforces the weight as well as the tradition of family caregiving. Part of this issue appears endemic across all caregivers in our sample and is likely widely felt among caregivers across all races when managing a new and unfamiliar disease process: inadequate information about and appreciation of the effects of AD and other dementias. In this sample, inadequate planning existed alongside lack of knowledge for local resources. Other work documents low utilization of health services and dependence on home care among older AAs 28,29 as well as frustration in the AA community with health care services, perceptions of racism, and absence or deficient knowledge of available local support. 39,40 Our participants found it similarly difficult to identify help within their own communities and this appeared to hinder their planning efforts. At the same time, the problem of moving into uncharted waters appears to be the product of the strength of the family and the tradition of respect for elders. Caregivers find themselves in something of a double bind: it is not only that there may be a lack of specific knowledge or know-how (eg, about legal or financial planning), it is also that it goes against the grain to interfere in an elder’s affairs. Thus a caregiver is faced not only with acquiring skills and knowledge to enable him or her to advocate on behalf of an elder within spheres of health care, social services, or legal or financial systems, it is also that the caregiver has to jump the emotional hurdle of taking that task away from the elder.
Descriptions of the supportive function of church are consistent with literature that, overall, has described the beneficial role that churches and religiosity/spirituality play in elder care among AAs. 41 –43 Caregivers also suggested using church as a venue for secular, day-to-day types of support, like for transportation services and day care for patients. In light of a desire for culturally familiar care, these suggestions hint that culturally familiar institutions, like church, could provide services that appeal to caregiver needs beyond the purely spiritual. Undercurrents in the conversations also made it clear that churches might not always be optimizing the role they could play in supporting caregivers or their elder congregants who are living with dementia.
In considering the educational and informational needs of AA dementia family caregivers, participants endorsed the educational objectives of the template program (Savvy Caregiver 44,45 ) and offered suggestions for additions to the curriculum. Several suggestions centered on self-care, which involved taking breaks from the stresses of caregiving, sharing caregiving responsibilities with other family members, and information on the potentially harmful health consequences of caregiving. These ideas seem to argue against assuming the role of solitary caregiver and promote the idea of more fully informing the family about the situation and engaging other members in care responsibilities. Caregivers sought enhanced knowledge about the disease itself, which could mitigate the “surprise factor” surrounding the disease and its effects on the person; they saw this as important in delivering care and also in improved care planning. Caregivers suggested incorporating a list of local resources, including local AA providers. Identifying an ethnic and culturally similar provider could be important for caregivers seeking culturally respectful treatment, particularly if previous health care experiences were characterized by frustration and racial prejudice. 39
Conclusions
This work adds to the body of knowledge about the AA dementia caregiving experience in several important areas. It elaborates on AA family care strategies and preferences via discussion of its historical and cultural roots. Our open-ended discussions also exposed challenges that individual AA caregivers face when they either cannot or prefer not to enact the full-time, “expected” caregiver role. For instance, some caregivers shared preferences for alternate sources of care and expressed broader desires for knowledge about local resources, despite long-held and historically rooted tendencies for family care. This study highlighted specific learning and planning needs, particularly in areas in which the individual intersects with the institutional worlds or law, finance, and health care. Knowledge deficits were acknowledged. Caregivers felt blindsided when faced with an AD diagnosis and did not know what to expect. They regretted the lack of long-term health, legal, and financial planning within their families, driven somewhat from cultural emphasis on privacy, particularly surrounding medical issues. Participants likewise found it difficult to identify help within their own communities. The study also delineated caregivers’ wishes for more attention to self-care and for the possibility of a broader distribution of caregiving responsibilities within families—and even beyond families to larger social networks and trusted institutions, especially churches. Finally, it emphasized the need for culturally sensitive and authentic care in the AA community, as a way to show respect for the patient, the patient’s family, and the patient’s history.
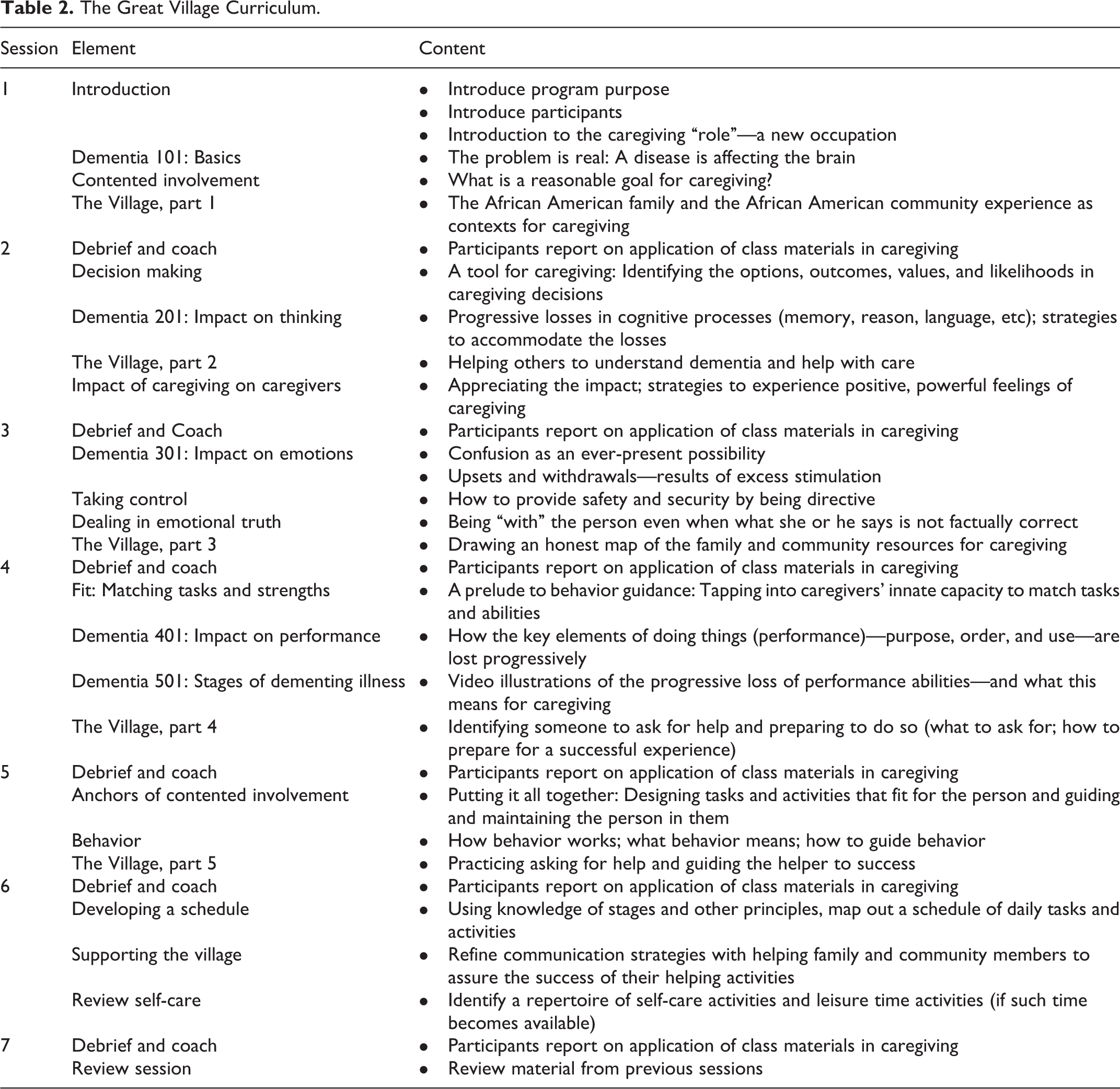
In practical terms, the findings of this effort were applied to the development of a psychoeducational intervention—The Great Village—whose impact was later tested in a systematic manner. The 14-hour, 7-session Great Village program employed talks and exercises designed to develop caregivers’ skills and knowledge about the impact of dementia on cognition, behavior, emotions, and performance of everyday tasks and to deploy strategies to accommodate these losses and promote calm days. In addition, the program included elements that flowed directly from focus group findings regarding the broader familial, community, and societal networks within which caregiving is occurring. The program contextualizes caregiving within a broad framework of the values of family, family responsibility, respect for elders, and the expectation of caring for one’s own. The curriculum acknowledges these values but also prompts participants to examine whether the expectations for help and support that inhere in these values are being fulfilled—or disappointed—in their own caregiving experience. A segment drawn from historical and sociological studies of AA families was added to aid caregivers in assessing the strengths of the family resources on which they might draw and to provide strategies for bolstering that resource, where possible. 46,47 Finally, in addition to providing lists of local service resources, the program engaged participants in an environmental mapping exercise. In this exercise, caregivers examine the family, community, and organizational relationships in which their caregiving is embedded. The exercise prompts them to assess the strength and direction of the relationships (how strong are they and do they give or take away strength for caregiving or self-care). The exercise ends with caregivers identifying ways in which the resource network might be strengthened, perhaps by making clearer demands on some, and perhaps by creating greater distance from others. Table 2 provides an outline of the Great Village curriculum.
The Great Village Curriculum.
This was a small study of 32 caregivers and its purpose was principally one of educational design. Its limitations are evident. The sample is not large and it was drawn from persons from a metropolitan area in the Southeastern United States whose connection to the investigators and sponsoring institution marks them as relatively homogenous. Thus, although our sampling was race based, our findings cannot be said to reflect the experiences of all AA caregivers. It is impossible to represent the diverse experiences, beliefs, and desires of a racial/cultural group in this or any single study. However, recognition that larger samples of AA caregivers respond differently than other races to interventions comes largely from quantitative data, 31,32,48 which called for an exploration of the forces behind these differences. Small focus group conversations provide an apt way to explore rich, albeit personal, experiences within a broader cultural framework. The open-ended format facilitated nuanced discussions of previously documented cultural themes and gleaned new information that may not have arisen within the constraints of survey or questionnaire-based data. Future work could explore the findings of this investigation with more controlled techniques. Additionally, data were collected in 2009. However, its relevance today is suggested by more recent work that reports on themes echoed in the transcripts of our focus groups, such as family obligation in caregiving 33 and the desire to provide exemplary care. 34
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Institute for Nursing Research PO1-NR011587; Caregiver Stress: Interventions to Promote Health and Well-Being.