
Abstract
This literature review focused on the experience, care, and service requirements of people with younger onset dementia. Systematic searches of 10 relevant bibliographic databases and a rigorous examination of the literature from nonacademic sources were undertaken. Searches identified 304 articles assessed for relevance and level of evidence, of which 74% were academic literature. The review identified the need for (1) more timely and accurate diagnosis and increased support immediately following diagnosis; (2) more individually tailored services addressing life cycle issues; (3) examination of the service needs of those living alone; (4) more systematic evaluation of services and programs; (5) further examination of service utilization, costs of illness, and cost effectiveness; and (6) current Australian clinical surveys to estimate prevalence, incidence, and survival rates. Although previous research has identified important service issues, there is a need for further studies with stronger research designs and consideration of the control of potentially confounding factors.
Keywords
Introduction
The provision of evidence to underpin decisions on services and supports for people with younger onset dementia (YOD) or early-onset dementia (EOD) is an emerging field. There is an increasing recognition of the different etiologies, trajectories, and implications of the diagnosis of dementia for people who are aged younger than 65 years at onset.
Although there is some debate over which terminology should be preferred, 1 we refer to YOD throughout as this term is commonly used in Australia, and the articles reviewed used the terms YOD and EOD interchangeably. Younger onset dementia reviews have predominantly focused on Alzheimer’s disease or frontotemporal dementia (FTD). 2 Consequently, the definition of the term “younger onset dementia” was broad 1 and encompassed major forms of dementia that occurred in those younger than 65 years. It included people with early-onset Alzheimer disease (EOAD), vascular dementia (VaD), FTD, dementia with Lewy bodies (DLB), and dementia associated with other conditions such as Huntington’s disease, Down’s syndrome, HIV/AIDS dementia, traumatic brain injury (TBI), and alcohol-related dementia (ARD).
This rapid 3 literature review, encompassing a broad overview of YOD, was commissioned by an Australian Government agency to inform future service development. The review examined the literature relating to the epidemiological aspects of YOD, the issues faced by people with YOD and their families, their needs and care requirements, and current programs and service initiatives. Our aim was to establish key aspects for the design and delivery of effective services and programs to meet the needs of people with YOD which have been identified in the international literature.
The review considered social, economic, and environmental factors that enable and support people with YOD, drawing on information available within the community, disability, and health care sectors. The review examined psychosocial program and support interventions but did not include an evaluation of medical and pharmacological therapies.
Methods
The literature search included peer-reviewed international academic literature and “gray literature” (such as reports by government agencies, leading community advocacy and education organizations, service providers, and other Web-based information).
Academic Literature
Relevant bibliographic databases were searched including MEDLINE, CINAHL, Academic Search Complete, Psychological & Behavioral Science collection, Scopus, ProQuest Central, Informa Healthcare, Cochrane Collaboration, and Biomed Central. The search was limited to articles in English from the year 2000 to current as recent research was the focus of the review. However, where information from earlier literature was identified as relevant, this was included.
The following search terms were included: (“young onset” or “early onset”) AND dementia AND NOT “elderly” or “older”; “Alzheimer’s” or “vascular dementia” or “frontotemporal dementia” or “Huntington’s disease” or “HIV” or “AIDS” or “acquired brain injury” or “Parkinson’s disease” or “Lewy bodies” and “cognitive impairment” or “neurocognitive disorder”; “community support” or “community care programs/interventions” or “community services” or “community participation” or “service needs” or “employment participation” AND NOT “clinical”; and “special needs” or “Indigenous or Aboriginal” or “LGBTI” or “homosexual” or “lesbian” or “rural” or “lifestyle” or “living alone” or “homeless.”
Term groups were then combined using AND in the following manner: 1 AND 2 AND 3; 1 AND 3 AND 4; 1 AND 2 AND 4.
Nonacademic Gray Literature
The nonacademic literature search used terms similar to the academic literature search, which included the following components: surface Web (eg, Google); country searches (eg, health and community service departments and community advocacy organizations); dementia-specific site searches; and other areas such as international conferences and professional associations.
Protocol-driven search strategies 4 were supplemented with “snowballing” methods such as reference list and citation searches, author searches, and hand searching of key journals.
Procedures for Study Selection and Review
Criteria for inclusion of academic and nonacademic articles were (1) a primary or comparative focus on YOD and (2) relevance to the service needs and service provision for people with YOD. Abstracts were retrieved, examined, and reviewed for their relevance based on the inclusion criteria by 2 researchers. Where disagreement occurred, these abstracts were checked by a third researcher and consensus concerning article retrieval was reached. Full texts of articles retrieved were then rated concerning their strength of evidence (see Appendix A). Given the emerging nature of evidence in this research field, qualitative, quantitative, and mixed methods articles were included, but the discussion was guided by their level of evidence.
Following a thematic analysis of the studies, they were grouped into the following areas: epidemiological studies concerning prevalence, incidence, and survival; experiences of people with YOD, their carers, and families; special needs groups; particular programs (nonpharmacological program evaluations); and service utilization and service design and development.
Review and summary tables were developed and included details such as the author and date, location, topic, research design, strength of evidence, study numbers, and focus.
Results
The search identified 448 documents of which 304 were included in the review. There were 221 (73%) academic articles and 83 (27%) documents included from the gray literature. Literature was sourced from a range of countries including Australia (31%) and international literature (69%) with those contributions mainly being from the United Kingdom and Europe, the United States, and Canada. Overall, 53% of the articles cited here were classified as acceptable practice or better, 43% were rated as emerging practice or less, and 4% of the articles were considered as not applicable for rating (eg, policy statements). These proportions reflect the emerging nature of evidence in this field. Figure 1 provides an outline the study selection process. The results are described subsequently in relation to the content areas identified.
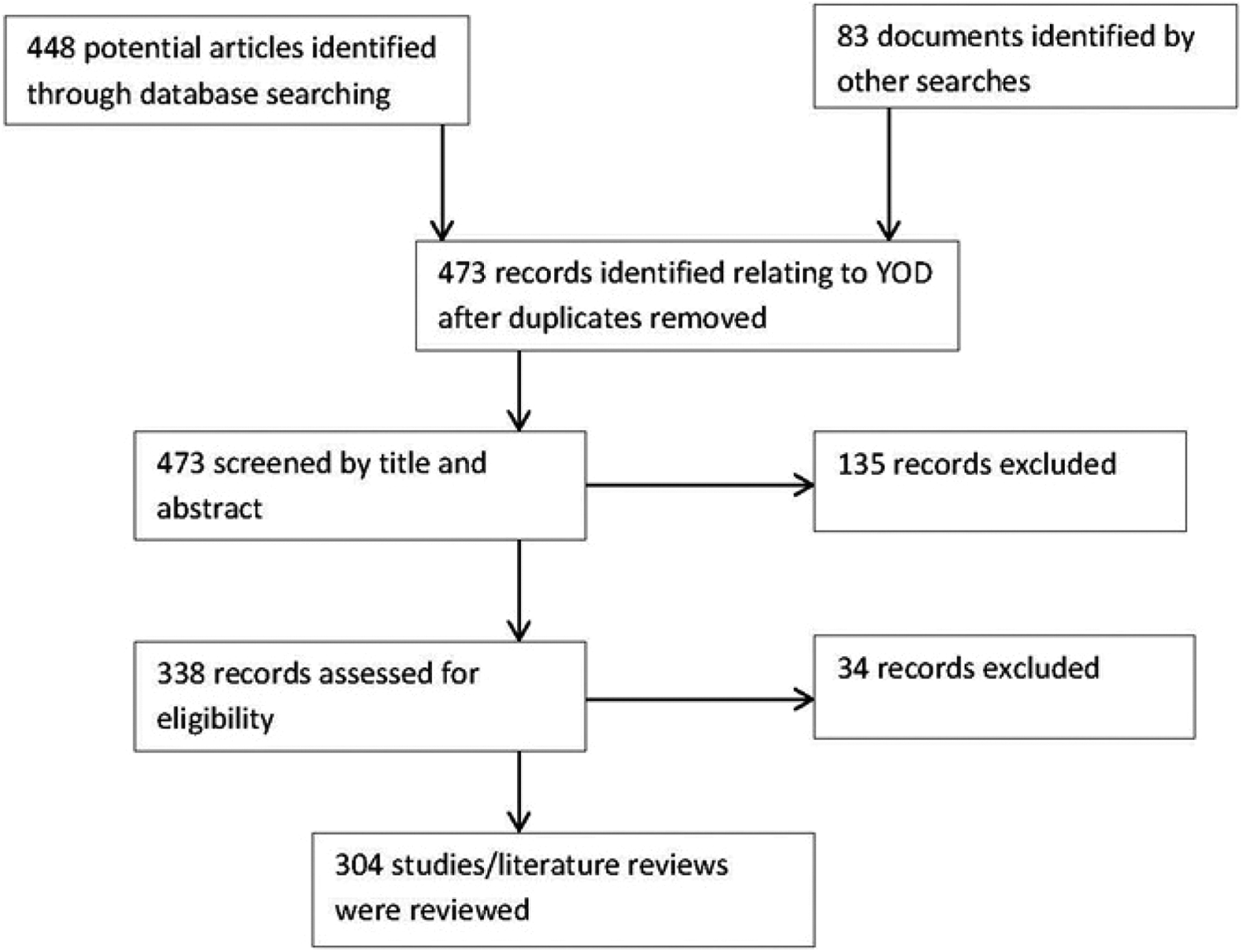
Younger onset dementia (YOD) Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart of study selection.
Epidemiological Studies Concerning Prevalence, Incidence, and Survival
These studies are important as they provide an estimate of the magnitude of these issues and are useful for service planning purposes. The review considered 21 articles of which 52% primarily presented Australian data 5 -16 and 44.5% international data. 17 -26 Most (86%) of these articles were considered to have an acceptable strength of evidence (see Appendix A).
However, most Australian and international estimates of prevalence were based on pooled data arising from meta-analyses of Western European and Northern American studies conducted in the 1990s. 5 -7,10,17,18,22,25 Many of these studies used different methods and had small samples and relatively few studies pertained to Australasia. 25 The accuracy of these estimates is debatable, given the international differences that have been reported. 19 Awareness of YOD may have changed in recent years, with improvements in neuroimaging technology and diagnostic procedures that may influence the identification of cases with dementia. 27 -29
The Australian Institute of Health and Welfare (AIHW) report 7 used United Kingdom estimates 17,18 for the under-60 age-group but data from a more recent meta-analysis 25 for the other age-groups. The AIHW 7 estimated that there were 23 900 Australians, younger than 65 years, with YOD in 2011. Studies by Access Economics 5,10 used United Kingdom figures 17,18 for the under-65 age-group and estimated that for 2011, there were 16 239 cases of YOD. 10 The differences in figures to those provided by AIHW 7 may be due to differences in calculating the rate for the 60 to 64 years age-group among other methodological differences. The AIHW 7 estimated that YOD represents about 8% of all dementias compared with the Access Economics estimate of 6.1%. 10
Limited data were found 12,13,30 concerning the prevalence and incidence of YOD in Australian Indigenous communities. Some of these studies did not have a particular focus on YOD or did not include persons younger than 60 years, but these suggested that the prevalence of dementia may be much higher than previously estimated.
Given the above-mentioned data, more accurate and current Australian research concerning prevalence, incidence, and survival is required, as these estimates may have major implications for service utilization and planning.
Prevalence studies vary considerably in their estimates of YOD diagnoses. In a United Kingdom 17,18 study undertaken in the 1990s, the major types of YOD were EOAD (34%), VaD (18%), FTD (12%), ARD (10%), DLB (7%), and other dementias (19%). A recent systematic review 26 identified considerable variation in the proportions of the various subtypes of YOD reported across studies. A recent Australian catchment study 15,16 reported a higher proportion of ARD.
A large French memory cohort study reported lower rates for EOAD (22%) compared with the later onset dementia (LOD) group, and FTD, ARD, TBI, and Huntington’s disease were more frequent EOD diagnoses. 24 Some studies have reported a slightly greater proportion of males (52%-58%) for the YOD groups, whereas women may be overrepresented in the LOD groups. 18,24
Some types of YOD such as ARD are potentially more preventable, and recent findings have indicated that potent combination of antiretroviral treatments for HIV/AIDS appear to reducing the incidence of this form of YOD. 31,32 This suggests that new treatments or health promotion interventions may have the potential to affect both the incidence and the prevalence of YOD and therefore future projections. 11
Evidence on the impact of dementia on survival is mixed with the average survival time from symptom onset appearing to be 7 to 9 years, but it may range from 3 to 10 years due to differences in diagnostic criteria, definition of onset, individual characteristics (eg, age, sex, and comorbidities), and the type and severity of dementia. 8 People with YOD may be more physically fit at the time of their diagnosis with less comorbidity. Estimated average survival ranged from 7.6 to 9.6 years from onset of symptoms 20,23 and 6.08 years from diagnosis. 20
The Experience of YOD
Overall, 44% of the literature for this section was rated as emerging practice or less and 75% of this literature was from international sources. Younger onset dementia commonly occurs in people aged between 40 and 65 years. This earlier onset raised a number of issues including loss or diminishment in roles such as provider, parent, and spouse and the significant adjustment to those changes that is required. Associated with the common loss of employment, people with YOD and their families experienced problems concerning loss of income and financial problems, 1,33,34 exacerbating an already difficult situation.
A major constraint facing people with YOD was in obtaining a timely and accurate diagnosis. Symptom overlap across YOD subtypes made differential diagnosis complex and difficult. 2,33 Standardized measures used to assess cognitive status were usually not those most sensitive to dementia status. 35 Problems experienced by people with YOD in obtaining a diagnosis (eg, time delays, initial misdiagnosis, or misrecognition of symptoms) were commonly reported in the research literature. 2,33,36 -41 A recent study indicated that the time to diagnosis for YOD from the onset of symptoms was on average 4.4 years compared to 2.8 years for LOD. 42
Evidence regarding the presence of behavioral and psychological symptoms of dementia (BPSD) was equivocal, with some studies reporting a higher presence for some subtypes such as FTD. 27,43 -48 However, BPSD were relatively common for most types adding to the needs and care requirements for people with YOD. 17,42 The most common BPSD for the EOAD group was apathy, 42 whereas aggression and disinhibition were more commonly reported for FTD. 27,43,44
Some types of YOD such as Huntington’s disease carry a high level of genetic transmission; Down syndrome carries a high risk for the development of dementia, and some forms of AD are more strongly associated with genetic risk factors. 49 For such affected groups, genetic counseling will be of prime importance.
Many of these issues were identified in the research literature that examined the experience of YOD from the perspectives of people with YOD, their partners, children and carers.
Some studies 50 -62 have interviewed people with YOD about their personal experience. Most could be characterized as qualitative thematic analyses of interviews based on small sample sizes of 20 persons or less. 52,54 -56,58,59 The common issues reported were the emotional shock of diagnosis, problems with obtaining a diagnosis, adjusting to the diagnosis and feeling stigmatized because of the dementia “label,” lack of referrals to support services, falling between the cracks of service systems, a lack of access to age-appropriate services and programs, and financial problems. Personal challenges identified included loss of independence, loss of employment, loss of empowerment, role changes, and the rebuilding and restructuring one’s life. Loss of empowerment was associated with the feeling that involvement in decision making was being denied often by well-meaning carers or service staff. There was a strong desire expressed by many to remain engaged and in control of their lives as best they could. 62
Spousal and family carers reported similar issues concerning services. Early recognition and referral was seen as a major area for service improvement by both people with YOD (94%) and carers (69%). 63
Other carer issues included managing BPSD, grief associated with the “loss” of spouse (the person as they were prior to dementia), juggling the caring role with other daily life responsibilities including employment, parenting, and difficulties in making plans for the future. 64 -75
Earlier diagnosis was seen as important as spouses reported that prior to diagnosis, they may have made mistaken attributions concerning their partner’s symptoms which may have negatively affected their marital relationship. 74 Many spouses experienced social isolation 76 -78 and found it difficult to balance addressing their own needs with their caring role.
Relatively few studies interviewed children of people with YOD, and the sample sizes generally included less than 15 children. 79 -85 This literature 78 -86 mentioned perceived stigma and associated shame/embarrassment, bewilderment, family conflict, high care burden, the physical challenge of caring, psychological issues, and problems at school. Many children reported undertaking a demanding caring role while facing the developmental challenges of growing up.
Coping strategies, family cohesion, and security of attachment were raised as issues. Some children reported positive effects of their caring role 83 such as maturation and the experience gained. However, these children have substantial needs for support, 87 and due to the care burden placed upon them, they may have a potential for psychological and social disadvantage 88,89 which needs further exploration. 90
Some studies used more quantitative approaches and standardized scales to assess carer burden, stress, unmet needs, the presence of psychiatric symptoms among carers, and health-related quality of life and well-being. These studies indicated high levels of stress and burden for carers, poorer quality of life, and unmet needs including social isolation, depression, and anxiety. 48,68,91 -94
Some studies used patient carer dyads to explore these themes, 33,48,73,95 allowing patient data (eg, severity, BPSD, etc) to be directly related to carer findings, thereby providing a somewhat higher level of evidence. Some studies compared YOD and LOD groups, 47,75,96 but some studies had poor control of potentially confounding factors (eg, the duration of the caring period, age, and diagnostic composition of the comparator groups). 73,84 Although more recent studies from the Netherlands 33 have addressed the course of illness, there is a requirement for further longitudinal research.
No studies were found that focused on the experience of people with YOD living alone or those who had no familial carer. There was little exploration of the experience of parental carers for people with YOD. It has been estimated that for dementia, overall approximately one-third of people with dementia live alone. 97 However, there were little data available concerning the YOD subgroup, which may be likely to have high service needs. 23,92 Premature placement in residential care facilities may be an issue for this group which requires exploration.
Studies focused on service experience issues 21,33,36,88,98 -103 noted the lack of a clear diagnostic pathway, poor provision of information, the lack of appropriate referrals to support services, and the high volume of informal care provided. High levels of unmet needs for people with YOD in such areas as daytime activities, communication, social companionship, intimate relations, and information were reported, 104 and these were significantly associated with the level and presence of neuropsychiatric symptoms.
These factors might suggest the earlier use of community support services may have the potential to delay institutionalization. 21,105 Despite the endeavors of major advocacy organizations for dementia to provide comprehensive information, the need for clear information and advice is still a major unmet need for carers and patients. It would be desirable if people with YOD and their families were routinely provided with clear written information at the point of diagnosis, 103 and consideration could be given to a telephone enquiry support service. 106
Special Needs Groups
Integral to inclusive service planning, development and delivery for any population are considerations of any special needs which people may have with regard to service access and equity, in addition to the primary diagnosis of YOD. Legislation regarding this issue varies internationally, but, for example, Australian Commonwealth legislation 107 recognizes a range of people as having special needs with regard to access and equity, including people from Aboriginal and Torres Strait Islander communities, non-English speaking backgrounds, and those residing in rural and remote areas. It also includes people who are financially or socially disadvantaged, veterans, homeless or at risk of becoming homeless, care leavers (people who had been raised in care homes), or lesbian, gay, bisexual, transgender, and people.
There were relatively few articles (19) that addressed these issues directly, of which only 3 articles discussed issues specific to YOD rather than to dementia overall, and 47% were classified as representing “emerging practice” or lesser levels of evidence (see Appendix A). The majority (74%) of this literature was Australian, but although the cultural mix varies across countries that make direct comparisons difficult, 108 the broad themes that emerged are likely to be relevant in other countries.
The key messages for these groups was to ensure the cultural, linguistic, and geographic factors were adequately identified and addressed in the planning, funding, and delivery of services. Importantly, there are people living with YOD who may be classified under multiple special needs groups and therefore may experience disadvantage on several fronts. 41
Barriers identified included: lack of access to culturally appropriate diagnostic services
41,108
-114
and the need for the use of culturally appropriate assessment tools
13,30,35,115
; denial of dementia within some cultural groups
105,108,110
; lack of linguistically and culturally appropriate services and appropriately trained staff
41,109,110,113
; lack of available information about existing services
41,110,116,117
; service access and transport availability issues – especially in rural and remote areas.
41,109,110,113
Living in a rural or remote region is likely to be disadvantageous because mainstream services may be scarce or nonexistent, restricting both choice and access. Given the rarity of YOD, it is highly unlikely that appropriate services for this group with special needs would be available, particularly in rural and remote areas. 41,64,110
The literature emphasized that the needs of these groups are complex, multifaceted, and dynamic and become more so with the onset of dementia, reinforcing the call for person-centered, culturally appropriate, flexible service options.
Particular Programs
A range of community-based programs and nonpharmacological interventions were identified for people with YOD, their carers, and families; however, the majority of the literature provided limited evidence concerning program effectiveness, and therefore, 50% of these articles were rated as “emerging evidence.” Recent initiatives such as INTERvention in DEMentia (INTERDEM), an interdisciplinary European collaborative research network on early and timely interventions in dementia, are endeavoring to improve the quality of research concerning the assessment of psychosocial interventions for dementia more generally. 120
Tailored physical activity programs, 121 -125 cognitive stimulation (eg, reminiscence therapy), 121,122,126 -129 and cognitive rehabilitation programs (using strengths to compensate for impairments) 120 have been shown to have positive outcomes on cognition. Support programs, particularly those that include both the person with dementia and the carer, were also helpful with promising results identified for memory loss programs/support groups. 130 -135
Facilitation of support groups through communication technology, such as e-mail and videoconferencing, showed some promise for carers. 78,136 -138 Although people with cognitive deficits often have difficulty with everyday technology, 139 some assistive technology programs (eg, to assist with television and telephone management) were found useful 140 -142 by people with YOD.
Programs that provide active meaningful participation, 114,122,143,144 horticulture, 145 -147 volunteering, 148 -150 supported workplaces, 151,152 and creative expression programs 153 warrant further study to clarify the design and delivery attributes that are most effective for people with YOD. Recent evidence on supported workplaces for people with dementia indicated positive impacts on self-esteem and life satisfaction and when combined with reflective therapies helped to bring about action and change within the individual. 151,152 Social groups can fill an important gap in services, providing semi-independent activity as well respite for carers. 154,155
Programs that provide individually tailored support 49,105 to people with YOD and their carers, such as case management or a key worker and carer training, 2,49,122,156 -158 warranted further research as did a self-management model for people with YOD. 159 It was also found that relatively few studies examined the cost-effectiveness of nonpharmacological interventions for dementia overall, and the application of these findings for the YOD group needs further assessment. 21,160
Given the limitations of the evidence underpinning programs, a culture of outcome evaluation should be developed. This should include the use of standardized outcome measures as well as qualitative approaches to evaluate effectiveness.
Service Utilization and Service Design and Development
As for dementia overall, few studies addressed the issues of service utilization and the costs of illness for the YOD group 17,161 or included consideration of social and informal care costs. 23,162 Studies indicated the period from the onset of symptoms to permanent residential care placement for people with YOD was quite long (eg, 6-9 years), and the level of informal care provided was high, placing a significant burden on these families. 23,162 Although some studies indicated a relatively high use of institutional services (eg, hospital admissions, nursing home respite, etc), 17,21,43 others reported that community service use was relatively low for this group. 23,34,43,99,100,162 This may reflect the absence of appropriate referrals to relevant support services but may also relate to attitudinal barriers or a lack of awareness about how these services might assist them. 98,163,164
Due to the earlier age of onset, service needs for those with YOD differ from those with LOD as many people with YOD could still be rearing children and may still be supporting a family financially. 1 Existing services for other disease groups, or for older people with dementia, may not have the flexibility and applicability required to respond to the broad range of needs a person with YOD and their family may require from a service. 17,62,88,161 For example, staff of dementia services for older people may not be skilled in providing referral support regarding the financial and employment issues that may arise when a person with YOD may feel pressured into taking early retirement. 60,165 Younger onset dementia service workers need to be able to work across sectors and link the person with YOD to services such as income support as well as helping them negotiate other services that may be required.
Suggested service improvements included the need for a central contact point for services or the adoption of case management and key worker approaches 2,33,105 that could provide individually tailored, person-centered services and for existing services to provide programs/services that are more age appropriate for people with YOD. 50,161,166,167
The examination of the literature by Koopmans et al 1 regarding YOD services and good practice models revealed that most evidence for good practice is not based on empirical studies, rather it is mostly the expert opinion of health professionals working with people having YOD or more recently from consumers. Our analysis also indicated that 44% of this literature was rated at the level of emerging practice or less.
Key themes from the literature regarding service design and development can, however, be identified.
1
The literature highlighted 2 key themes regarding services for people with YOD: At the system level, the overwhelming evidence from the literature identified service integration as being critical. There is a need to integrate diagnostic services and to streamline the pathway to diagnosis and to relevant service support. The use of multidisciplinary team approaches and the development of more effective links between the range of services providing assistance to people with YOD, their carers, and families along the dementia journey are required.
2,33,40,43,114,143,166,168
-176
At the service level, people with YOD need to be consulted in the design and delivery of services designed to support them. Underpinning an individualized approach is the need for flexibility to accommodate individual and family circumstances as they change over time.
49,105,166,173
A key requirement is the need for age-appropriate services,
49,105,143,174,177
-180
providing meaningful, stimulating, and potentially beneficial activities.
Some authors also recommended the introduction of specialist services for YOD, 21,33,50,181 -183 and such services are increasingly available internationally. Given the relative rarity of YOD, for countries that have vast areas of sparse population such as Australia, access to specialist services in rural areas presents challenges. Effective outreach strategies (eg, teleconferencing, video conferencing, and Web links) will need to be included in the design of specialist services. 78,175,184 Given that many people with YOD may not be able to directly access specialist services, local dementia and disability services staff will also need education and training to assist both community and residential services 185 in addressing the particular needs of YOD clients.
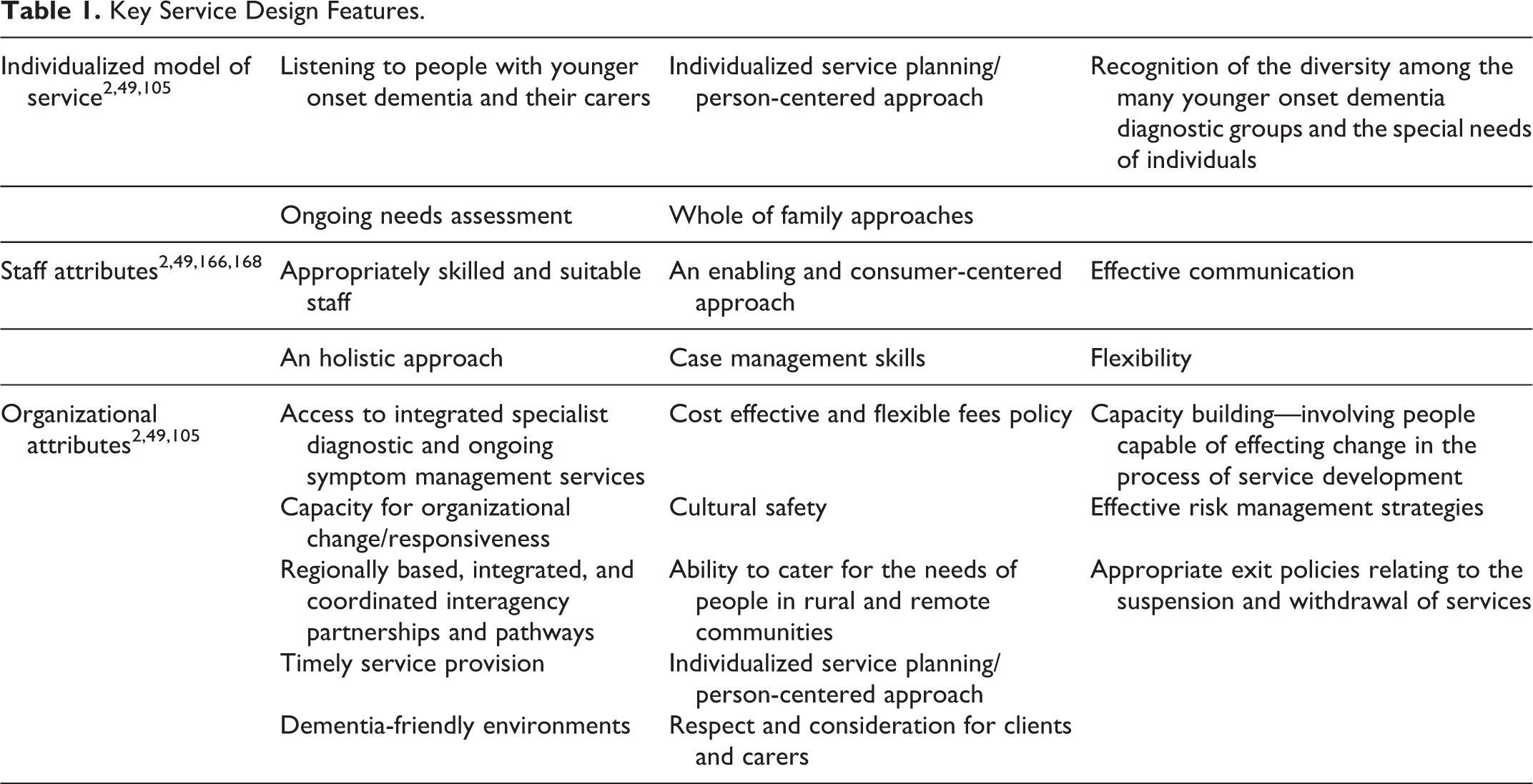
The key service design attributes that were identified in the literature can be applied across a range of service types, both specialist and generic. The features of the service model, staffing, and organizational attributes are outlined in Table 1 and could readily be incorporated into many mainstream services.
Key Service Design Features.
The concept of stages of the YOD disease trajectory is reflected in the literature as a useful concept for developing service responses for people with YOD. 33,74,105,186 In Australia, the Draft National Framework for Action on Dementia, 2013 to 2017, 187 identified 4 stages of dementia that relate to service delivery and design: risk reduction, assessment, management, and later stages of dementia/end of life. Due to the younger life stage of YOD, it was identified that an additional stage for people with YOD should be considered. Following diagnosis, a stage of “adjustment, enablement, and engagement” occurs (see Figure 2). Key elements of this stage are the adjustments in life made in response to the diagnosis of dementia. These include addressing their primary, family, and social relationships issues; developing new skills and strategies for remaining at work or transitioning to early retirement; and establishing financial and legal plans for the future. If people with YOD are appropriately supported during this critical stage, they may be able to maintain their independence for longer as well as preserving a sense of a “normality” and “control” in their changing lives.

Five stages of younger onset dementia support.
Conclusion
This rapid 3 but comprehensive literature review was undertaken within an Australian policy context that may limit the generalizability of some of the findings to other jurisdictions/countries. It is also limited to English language articles so has excluded some contributions from other countries.
However, the service principles identified are generic in nature and so may be effectively applied to a range of YOD service settings internationally. Effective service provision for people with YOD in Australia will only be possible if health, aged care, and disability service sectors work collaboratively to provide a holistic approach to supporting people with YOD, their carers, and families.
To strengthen the evidence, there is a need for further studies with stronger research designs, larger sample sizes, a triangulation of methods of outcome assessment, and consideration of the control of potentially confounding factors to enhance evidence-based practice in this field.
Footnotes
Appendix A
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The University of Wollongong received a grant from the Australian Government Department of Social Services.