
Abstract
To compare the accuracy of different neuropsychological tests and their combinations for deriving reliable cognitive indices for dementia diagnosis in Parkinson’s disease (PD). One hundred forty consecutive patients with PD were recruited and administrated an extensive battery of neuropsychological tests. Discriminant analysis and receiver–operator characteristic curve were used to evaluate their correct classifications and validity. Patients with PD having dementia (PDD; 23.5%) performed significantly worse in all tests than patients without dementia. Age of onset, disease duration, Hoehn-Yahr grade, Unified Parkinson’s Disease Rating Scale part III scores, and education were associated with dementia in patients with PD. Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment, and Block Design (BD) showed better specificity and sensitivity when used alone, and combined use of MMSE and BD further increased the validity. Our results indicated that the accuracy of MMSE was better in dementia diagnosis of Chinese patients with PD, and combined use of MMSE and BD could further increase the validity of dementia diagnosis.
Introduction
Parkinson’s disease (PD) is one of the most common chronic progressive neurodegenerative movement disorders, affecting approximately 1.7% of the elderly patients aged 65 years and older in mainland China. 1 Characterized by degeneration of dopaminergic neurons in the substantia nigra and ventral tegmental area, PD may result in a multitude of motor and nonmotor behavioral disturbances that dramatically impact the quality of life and consequences of the disease. 2
Cognitive impairment is a common feature of PD, with deficits being most prominent in the domains of memory and executive functions. 3 The neurological deficits may range from slight impairment (PD without dementia [PDND]), impairment only demonstrable by means of neuropsychological tests, up to dementia (PD with dementia [PDD]), a condition that may worsen the prognosis and impose significant negative personal and socioeconomic impacts. 4 Estimated prevalence of PDD varies from 4% to 93%, with an average of 40%. 5 Parkinson’s disease carries an approximately 6-fold increased risk of dementia when compared with the general population, 6 and it is an independent risk factor for cognitive impairment and dementia in the elderly patients aged 55 to 74 years. 7
Comprehensive neuropsychological assessment is suggested to be the best way to define cognitive decline in patients with PD and critical to a better understanding of the impairment of cognitive function in the process of dementia diagnosis. 8 Various neuropsychological batteries have been used for dementia screening. However, wide variation, low sensitivity, and poor specificity have been reported for these screening tools in patients with PD. 9 To our best knowledge, currently, no single diagnostic approach for dementia in patients with PD is highly sensitive, specific, and accurate. The utilization of an extensive neuropsychological battery has been recommended. 10 The objective of the present study was to determine the specificity, sensitivity, and accuracy of various neuropsychological tests, including Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), Block Design (BD), Fuld Object Memory Evaluation (FOME), Digit Span (DS), and Rapid Verbal Retrieve (RVR), and any of their combinations in Chinese patients with PD, and to identify the best short screening test for dementia in PD in order to facilitate clinical diagnosis.
Methods
Participants
This study was approved by the Medical Ethical Committee of the First Affiliated Hospital of Xi’an Jiaotong University and conducted in accordance with the Declaration of Helsinki. Informed consent was obtained from all participants prior to their participation. A cohort of 140 (82 male and 58 female) patients with PD were recruited consecutively between March 2010 and October 2013. The diagnosis of PD was established by a neurological expert in movement disorders according to the United Kingdom Brain Bank criteria. 11 Patients with Lewy body dementia, non-PD parkinsonian syndromes, or Parkinson plus syndrome, confirmed by brain magnetic resonance imaging, were excluded. Dementia was defined according to the following criteria: cognitive deficits in at least 2 domains and impaired activities of daily living (ADLs) due to the cognitive deficits. Disability in basic and instrumental activities was evaluated using the modified ADL index as described previously. 12
Neurological and Neuropsychological Assessments
A neurologic examination was performed on all patients to confirm the diagnosis of PD. Major demographic data including gender, age, onset age and duration of the disease, education level, and medical history were collected. The duration of the disease was defined as the time since appearance of the first motor symptoms reported by the patients. Severity of the disease was determined by the modified Hoehn and Yahr scale 13 and the Unified Parkinson’s Disease Rating Scale part III (UPDRS-III). 14 Each participant was interviewed by a licensed neuropsychologist. An extensive battery of neuropsychological tests was administered to assess multiple cognitive domains. 11,15 –18 The MMSE and MoCA are commonly used as standard clinical tests for cognitive dysfunction, especially in Alzheimer’s disease. It has been shown that MMSE is superior to MoCA for more advanced stages of the disease with functional impairment but is insensitive as a screening instrument for mild cognitive impairment and executive function, 19 whereas MoCA, originally developed as a tool to screen patients with mild cognitive deficits, usually works well in patients with a normal range of MMSE score. 20,21 In this study, the modified Chinese versions of MMSE and MoCA were used to evaluate the total cognition function, the FOME was used to evaluate delayed memory function, RVR was used to evaluate language fluency, BD subtest of the Wechsler Intelligence Scale for Children Revised (WISC-III) was used to evaluate visuospatial function, and DS subtest of the Chinese version of the Wechsler Adult Intelligence Scale Revised (WAIS-RC) was used to evaluate immediate memory and concentration problems. 22
The cutoff score was 11 for FOME 23 and 20 for ADL. For the other tests, cutoff thresholds were determined based on education levels of the patients. For illiterate (not formally educated) patients, those with primary school education (6 years or less), and those with middle or high school education (more than 6 years), the cutoff values were 15, 20, and 25, respectively, for RVR, 24 10, 15, and 20, respectively, for BD, 25 5, 6, and 7, respectively, for DS, 26 and 17, 20, and 24, respectively, for MMSE. 27 For MoCA, the threshold score was 26 for patients with >12 years of education and 25 for those with ≤12 years of education. 28 Neuropsychological evaluation was administered by a single neuropsychologist when the patients were on their best conditions.
Statistical Analysis
Normally distributed continuous data were expressed as means ± standard deviation (SD) and analyzed by t test. Categorical data were expressed as frequency distributions and analyzed by χ2 test. The average percentages of correct classifications based on different neuropsychological rating scales were obtained and validated by discriminant analysis. Diagnostic accuracy was defined as the proportion of patients correctly categorized. The sensitivity, specificity, and accuracy defined as the proportion of patients correctly categorized were determined for each of the rating scales in relation to dementia diagnosis by receiver–operator characteristic (ROC) curve. The relative 95% confidence intervals were also estimated. Comparisons of areas under the curve (AUCs) were performed using Z test. All calculations were performed using SPSS software version 13.0 (SPSS Inc, Chicago, Illinois). P < .05 was considered as statistically significant.
Results
Demographics and Clinical Characteristics
The basic demographics and clinical data of the participants are summarized in Table 1. Thirty-three (23.60%) patients with PD receiving neuropsychological tests were diagnosed with dementia. Their average age was higher than that of patients with PDND, but the difference did not reach the statistically significant level (P = .856). Patients with PDD and PDND significantly differed in both the onset age (P = .014) and the duration (P = .008) of the disease. The proportion of females was significantly higher in patients with PDD (60.6%) than in patients with PDND (35.5%; P = .011). The UPDRS-III values were also significantly higher in patients with PDD than in patients with PDND (P < .001). In contrast, education levels were significantly lower in patients with PDD than in patients with PDND (P < .001). Hoehn-Yahr grade was significantly different between the PDD and the PDND groups (P = .001).
Demographic and Clinical Characteristics of Patients Having PD With and Without Dementia.
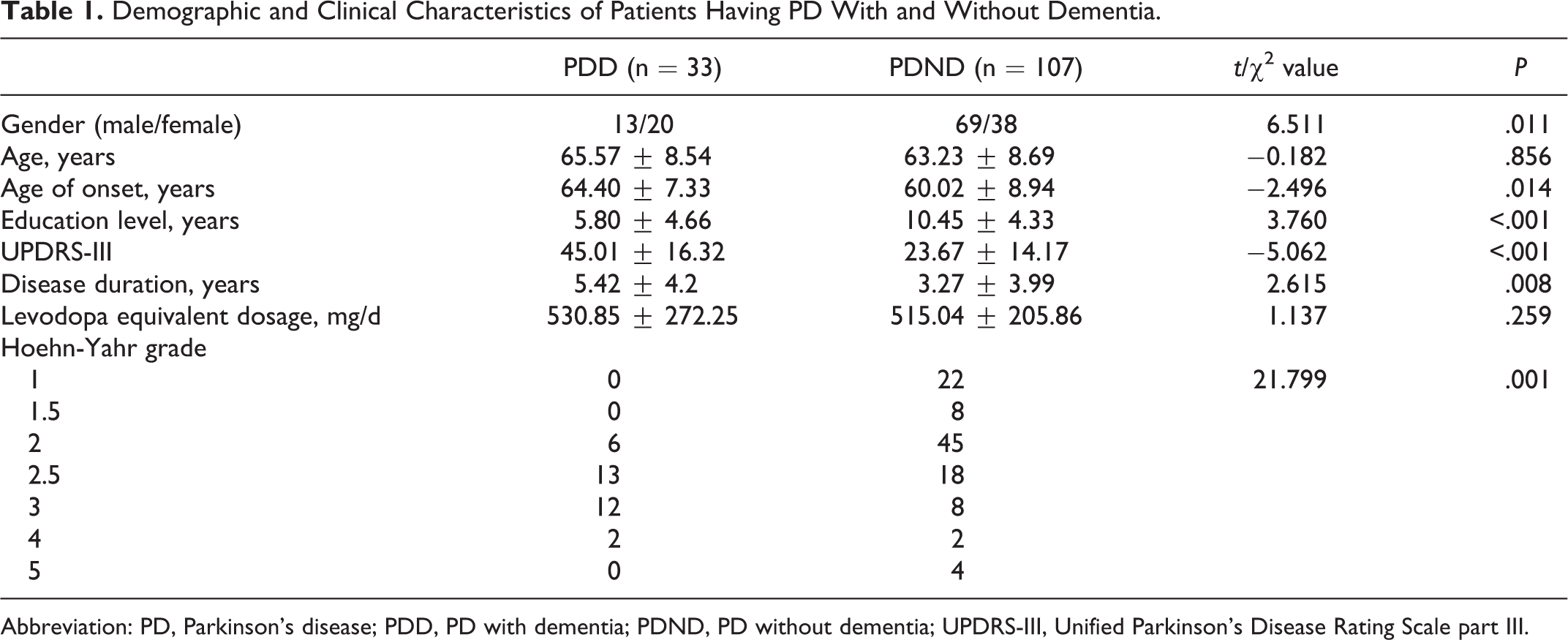
Abbreviation: PD, Parkinson’s disease; PDD, PD with dementia; PDND, PD without dementia; UPDRS-III, Unified Parkinson’s Disease Rating Scale part III.
Neuropsychological Findings
Presented in Table 2 are the results of the various neuropsychological tests performed. The MMSE, MoCA, RVR, FOME, BD, and DS scores were all significantly lower in patients with PDD than in patients with PDND (P < .001). In contrast, the ADL score was significantly higher in patients with PDD than in patients with PDND (P < .001).
Scores (Mean ± SD) of Various Neurological Tests in Patients With PDD and PDND.
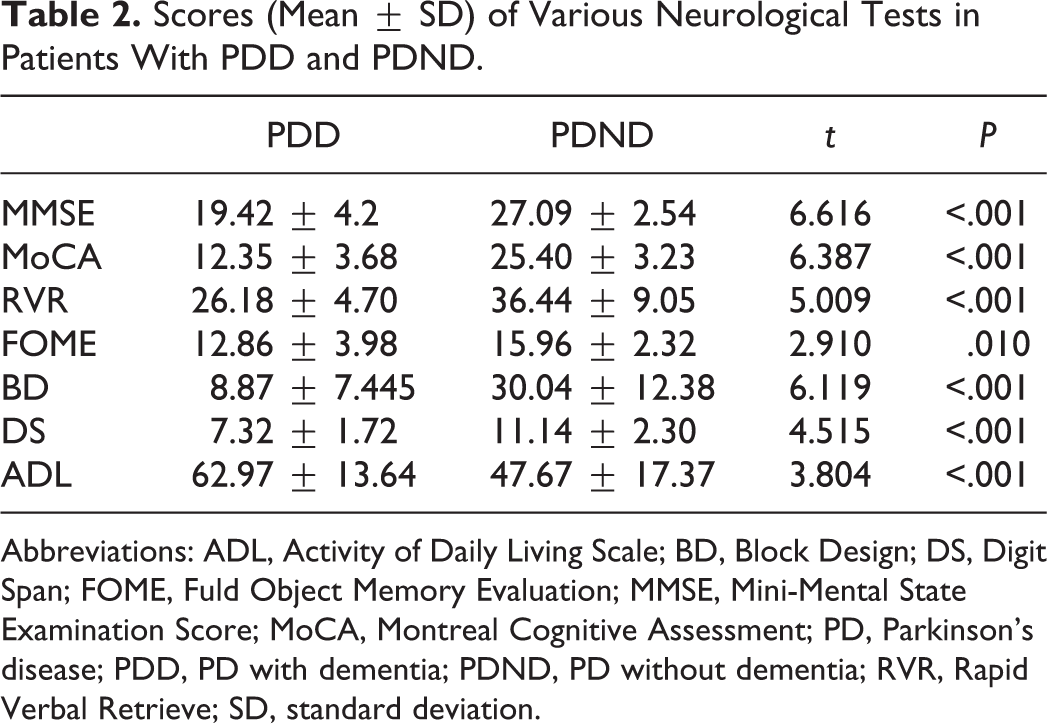
Abbreviations: ADL, Activity of Daily Living Scale; BD, Block Design; DS, Digit Span; FOME, Fuld Object Memory Evaluation; MMSE, Mini-Mental State Examination Score; MoCA, Montreal Cognitive Assessment; PD, Parkinson’s disease; PDD, PD with dementia; PDND, PD without dementia; RVR, Rapid Verbal Retrieve; SD, standard deviation.
Validity of Individual Neuropsychological Tests in the Diagnosis of Dementia in Patients With PD
The results of the discriminant analysis are presented in Figure 1A and Table 3. Among the 6 neuropsychological tests performed, MMSE had the highest total accuracy in distinguishing PDD from PDND, followed by MoCA and BD. By contrast, FOME, DS, and RVR were less accurate in identifying dementia in patients with PD. As demonstrated by the analysis of the area under the ROC curve, MMSE, MoCA, and BD were more accurate than DS, RVR, and FOME in distinguishing PDD from PDND (P < .001).
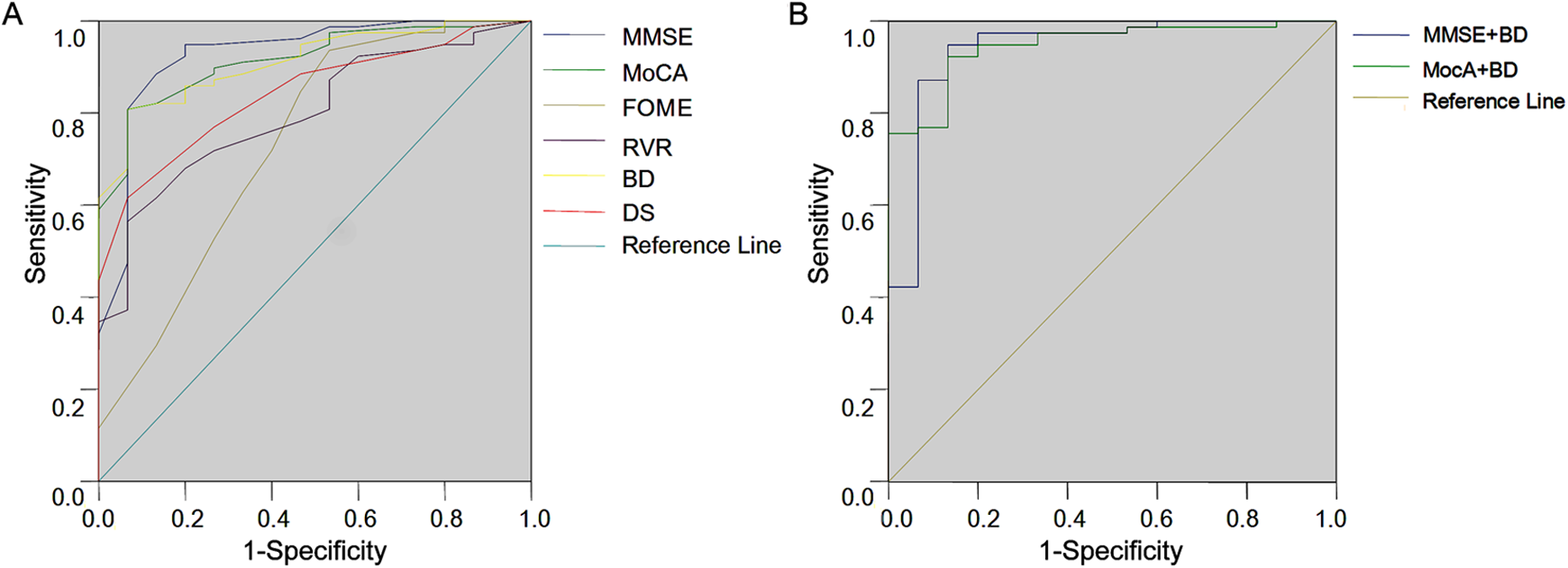
Receiver–operating characteristic (ROC) analysis of the dementia diagnosis in patients with Parkinson’s disease (PD) by neuropsychological tests. A, Receiver–operating characteristic curve of the various neuropsychological tests. B, Receiver–operating characteristic curve of Mini-Mental State Examination (MMSE) or Montreal Cognitive Assessment (MoCA) in combination with Block Design (BD).
Percentages of Correct Classifications and Validity of the Single Neuropsychological Scale in Discriminant Analysis.
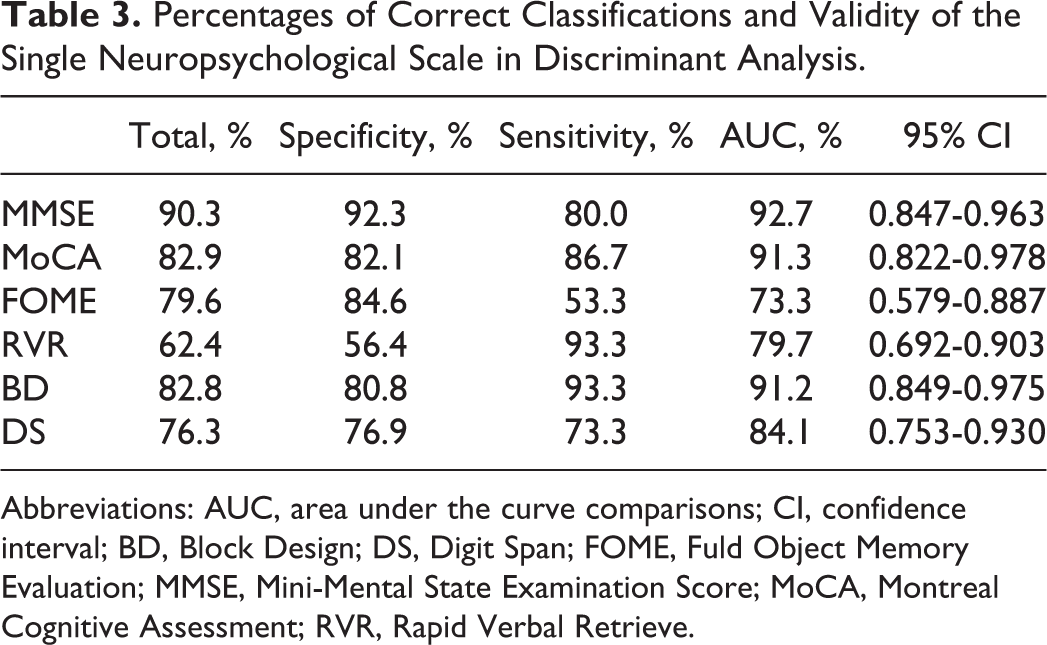
Abbreviations: AUC, area under the curve comparisons; CI, confidence interval; BD, Block Design; DS, Digit Span; FOME, Fuld Object Memory Evaluation; MMSE, Mini-Mental State Examination Score; MoCA, Montreal Cognitive Assessment; RVR, Rapid Verbal Retrieve.
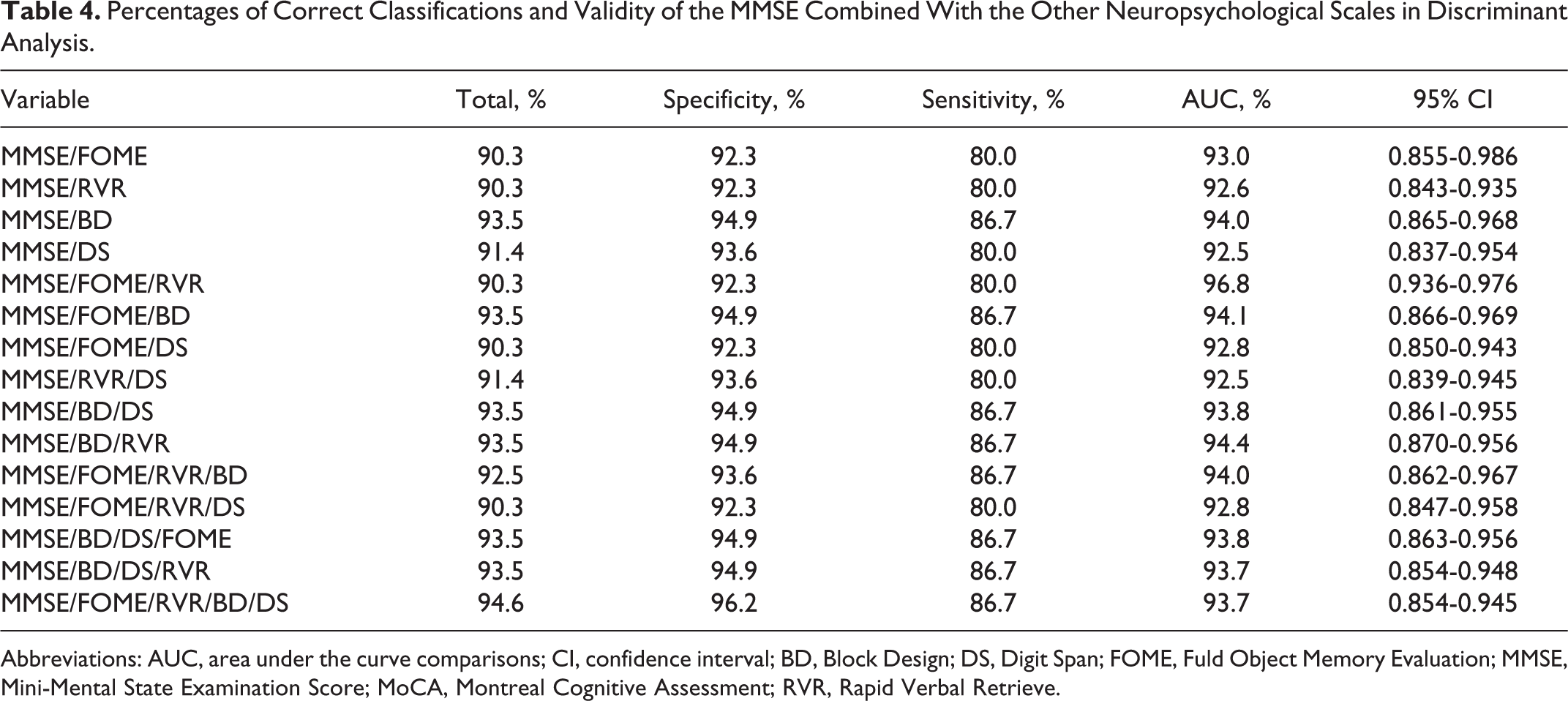
Validity of MMSE Combination With Other Tests in the Diagnosis of Dementia in Patients With PD
The results of the discriminant analysis of MMSE in combination with other tests are presented in Table 4. The overall accuracy, specificity, and sensitivity to distinguish PDD from PDND were all significantly improved when MMSE was combined with BD as compared with MMSE used alone (P < .001). In contrast, when MMSE was combined with FOME, DS, or RVR, no significant improvement was observed. Moreover, the combination of MMSE with 2 or more other tests did not show further improvement in the overall accuracy either.
Percentages of Correct Classifications and Validity of the MMSE Combined With the Other Neuropsychological Scales in Discriminant Analysis.
Abbreviations: AUC, area under the curve comparisons; CI, confidence interval; BD, Block Design; DS, Digit Span; FOME, Fuld Object Memory Evaluation; MMSE, Mini-Mental State Examination Score; MoCA, Montreal Cognitive Assessment; RVR, Rapid Verbal Retrieve.
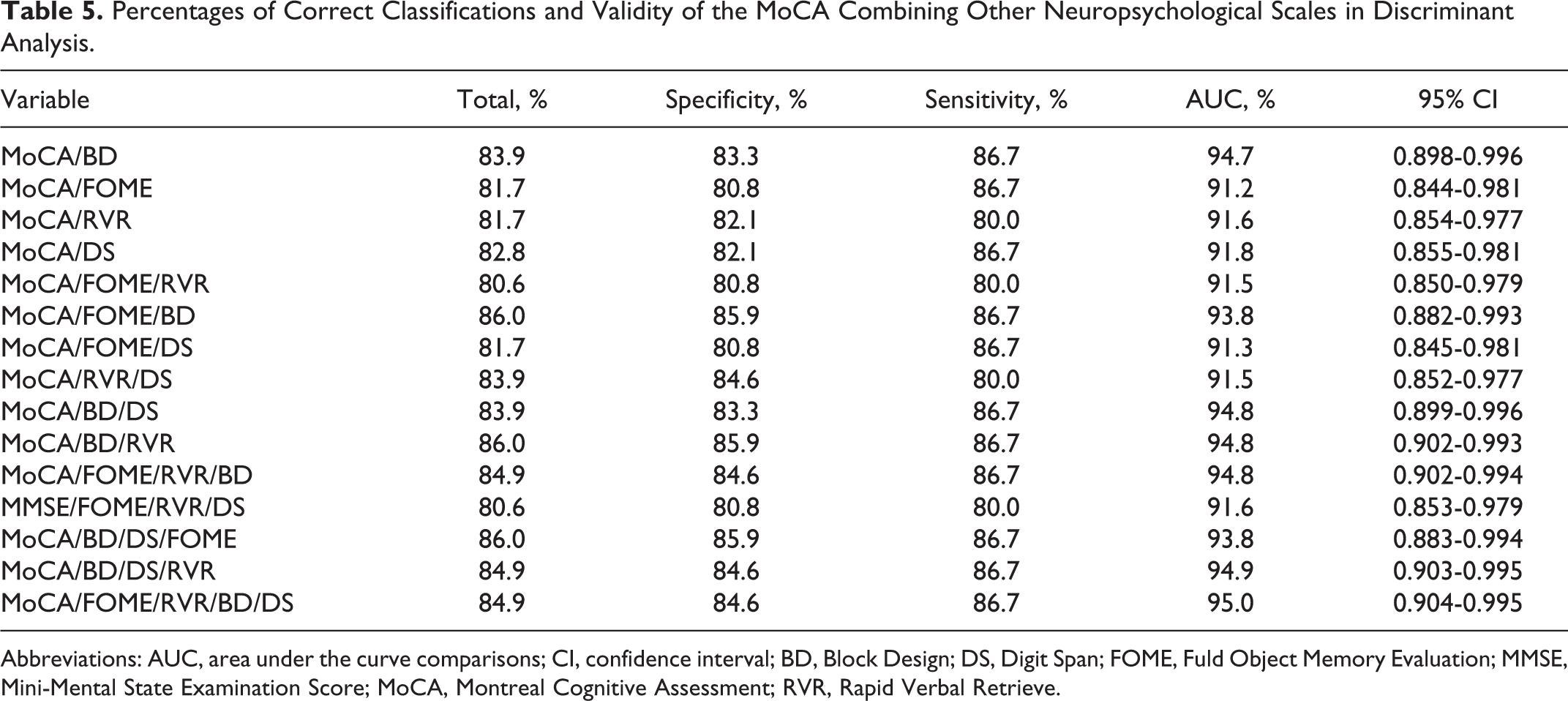
Validity of MoCA Combination With Other Tests in the Diagnosis of Dementia in Patients With PD
The results of the discriminant analysis of MoCA in combination with other test are presented in Figure 1B and Table 5. The combination of MoCA and BD significantly improved the overall accuracy of dementia diagnosis in patients with PD as compared with MoCA and BD each used alone (P < .001). The specificity was also significantly improved (P < .05), but the sensitivity was not affected (P > .05). Compared with the MMSE/BD combination, the MoCA/BD combination had a similar sensitivity (P > .05) but a relatively lower specificity (P < .05). In contrast, the combination of MoCA with one or multiple other tests (RVR, FOME, and DS) failed to improve the performance in PDD diagnosis.
Percentages of Correct Classifications and Validity of the MoCA Combining Other Neuropsychological Scales in Discriminant Analysis.
Abbreviations: AUC, area under the curve comparisons; CI, confidence interval; BD, Block Design; DS, Digit Span; FOME, Fuld Object Memory Evaluation; MMSE, Mini-Mental State Examination Score; MoCA, Montreal Cognitive Assessment; RVR, Rapid Verbal Retrieve.
Discussion
Parkinson’s disease is a progressive neurodegenerative disorder characterized by a combination of classical motor and nonmotor symptoms. Among nonmotor symptoms, cognitive impairment is very common and may eventually lead to the development of dementia syndrome, thus not only affecting the quality of life of the patients but also imposing increased burdens to their caregivers. 29 Therefore, screening for dementia in patients with PD is extremely clinically important to the establishment of diagnosis and the initiation of proper treatments. To this end, it is urgently needed to develop an easily obtainable, reproducible, and validated test battery with high specificity and sensitivity.
Different neuropsychological scales have been proposed to aid dementia diagnosis in patients with PD. Mini-Mental State Examination is the most commonly used instrument to document cognitive impairment in clinical geriatric research and can evaluate several cognitive function domains. 30 However, it was originally designed for screening Alzheimer’s disease and does not encompass all cognitive deficits, such as executive dysfunction. Moreover, MMSE is associated with ceiling effects and inadequate sampling of various cognitive domains. As a result, MMSE is generally considered unsuitable for reliable PDD identification. 31 Montreal Cognitive Assessment, a brief and potentially useful tool developed to assess a broader range of domains frequently affected in PD, is more sensitive than the commonly used MMSE in cognitive impairment, especially in the screening of mild cognitive impairment. 32 Executive function, language abilities, and visuospatial processing can be more rigorously assessed with MoCA than MMSE in patients with PD. 33 After having investigated the validity of the MoCA and MMSE in the detection of cognitive impairment in PD, Hoops et al suggested that additional assessment was necessary for a positive screening. 34 Moreover, the study by Di Biasio et al also recommended the use of an extensive neuropsychological battery in the diagnosis of dementia in patients with PD. 10
Other neuropsychological assessment batteries include RVR, BD, DS, and FOME. These tests usually test multiple separate cognitive domains that may collapse to form composite measures. However, there are various methods for defining these tests and their composites. To date, the usefulness of these tests, either each alone or in a combination with MoCA or MMSE, in the diagnosis of dementia in patients with PD has never been evaluated. In this study, we compared the accuracy of 6 different methods for deriving single or composite indices of cognition for predicting dementia in the 140 patients with PD. We found that 23.6% of patients with PD receiving the tests were diagnosed with dementia. This incidence was comparable to that found in some studies 35,36 but was inconsistent with that reported in some other studies. 32,37 –39 To our expectations, all the examined dementia scales (MMSE, MoCA, BD, RVR, DS, and FOME) demonstrated significant differences between patients with PDD and PDND. In ROC curve analysis, MMSE, MoCA, and BD showed better specificity and sensitivity when used alone. Mini-Mental State Examination had a relatively higher specificity, whereas MoCA had a relatively higher sensitivity. Mini-Mental State Examination was more accurate than MoCA in diagnosing dementia in PD; this finding is partially consistent with the results from a previous study where a sensitivity of 59% and a specificity of 89% were demonstrated for MoCA and a sensitivity of 77.2% and a specificity of 75.0% for MMSE. Inconsistent data on AUCs were obtained in previous studies. In the study of Hu and colleagues, AUCs for MoCA and MMSE were 0.794 and 0.841, respectively. 40 In some other studies, AUCs for MoCA and MMSE were 0.903 (0.96) and 0.82 (0.90), respectively, for major (minor) neurocognitive impairment in PD, 41 –43 indicating that MoCA performed better than MMSE as a test for detecting neurocognitive impairment in PD. A sensitivity of 0.915 (0.921) and a specificity of 0.831 (0.801) were obtained for MoCA and a sensitivity of 0.602 (0.692) and a specificity of 0.706 (0.806) for MMSE in detecting major (minor) neurocognitive disorder associated with PD in these studies. Given the suboptimal specificity for either MMSE or MoCA, 34 we evaluated the various combinations of MMSE or MoCA with other tests. We found that the combined use of MMSE or MoCA with BD further improved the overall accuracy of dementia diagnosis in our patients with PD and that the MMSE and BD combination was superior. However, the combination of 3 or more tests had a relatively low sensitivity and failed to further improve the diagnosis. The reason for this failure remains unclear, but the involvement of different cognitive domains in MMSE and MoCA tests might be a partial explanation. Montreal Cognitive Assessment can detect the cortical and subcortical function, whereas MMSE is insensitive to subcortical dementia. 44 Block Design mainly detects subcortical visuospatial function, whereas RVR, FOME, and DS detect cortical function. Therefore, the combination of MMSE with BD may compensate the inability of MMSE to detect subcortical function. Together, we demonstrated that all neuropsychological batteries tested in this study were able to assess the neuropsychological performance of patients with PDD, and the combination of MMSE and BD had the highest specificity, sensitivity, and accuracy in distinguishing PDD from PDND among all individuals or combinations of tests evaluated.
In conclusion, our results demonstrated that the accuracy of MMSE was higher than those of MoCA, RVR, BD, DS, and FOME in dementia diagnosis in Chinese patients with PD. Although MMSE or MoCA is still the recommended tool for dementia screening for patients with PDD in China, the combination of MMSE and BD may offer a better option for dementia diagnosis. However, the clinical benefits of the combined use of MMSE and BD in screening dementia in patients with PD have to be further evaluated in large cohort studies in the future.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.