
Abstract
Objectives:
The aim of this systematic review is to identify published randomized controlled trials (RCTs) that evaluated the use of acetylcholinesterase inhibitors for delirium in older adults (≥60 years).
Methods:
A literature search was conducted of PubMed, MEDLINE, EMBASE, PsycINFO, and Cochrane collaboration databases for RCTs in any language that evaluated the use of acetylcholinesterase inhibitors for delirium in older adults (≥60 years). Also, bibliographic databases of the published articles were searched for additional studies.
Results:
A total of 7 RCTs that evaluated the use of acetylcholinesterase inhibitors for delirium in older adults (≥60 years) were identified. In 5 of the 7 studies, there was no benefit for the acetylcholinesterase inhibitor in either the prevention or the management of delirium. In one study, there was a trend toward benefit for the active drug group on the incidence of delirium and the length of hospital stay, but both outcomes did not attain statistical significance. One study found a longer duration of delirium and a longer length of hospital stay in the active drug group when compared to the placebo group. The acetylcholinesterase inhibitors were well tolerated in 4 of the 7 studies. In 1 study, the mortality rate was found to be almost 3 times higher in the group receiving haloperidol and rivastigmine when compared to the group receiving haloperidol and placebo.
Conclusion:
Current evidence does not suggest efficacy of acetylcholinesterase inhibitors for the prevention or management of delirium in older adults.
Introduction
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) identifies delirium as a condition associated with a disturbance in attention, awareness, and cognition. 1 Although the rates of delirium are low in older individuals living in the community at 1% to 2%, their incidence increases significantly in hospital settings. 2,3 During admission to hospitals, the incidence rate of delirium is approximately 11% to 42%. The incidence rate of delirium during a hospital stay is over 50%. 3,4 In intensive care units (ICUs), the incidence of delirium in the elderly population is greater than 70%. 2,3 Postoperative delirium is very common in older adults with an incidence rate that varies between 15% and 60%. 2,3 It is currently estimated that in the United States, between one-tenth and one-half of all individuals ≥65 years in age who require hospitalization are affected by delirium. 5
The presence of delirium is associated with poorer patient outcomes including a worsening of their nutritional status, cognition, and medical comorbidities. 3 In addition, delirium results in a greater burden of care on the nursing staff, longer lengths of hospital stay, and greater cost of hospitalization. 6,7 Furthermore, delirium increases the risk of dementias, hospitalization, institutionalization, and death. 3,8,9 The average medical care cost for individuals with delirium is more than 2½ times the cost for individuals without delirium. 10
Acetylcholine is noted to be an important substrate for the modulation of cognition in humans. 11,12 Current evidence indicates that there is a disruption of the normal activity of the cholinergic system in the brain of individuals with delirium. 13,14 Additionally, it has been noted that drugs with anticholinergic properties can precipitate delirium, especially in the older individuals. 15,16
Available data from several studies indicate that acetylcholinesterase inhibitors that have shown efficacy in individuals with Alzheimer’s disease may also benefit individuals with delirium. 17 –21 However, the only meta-analysis that evaluated the efficacy of acetylcholinesterase inhibitors for delirium included only 1 randomized controlled trial (RCT) that compared donepezil to placebo. 22 The investigators found no significant difference between the treatment and the placebo groups for the duration of delirium from this 1 study. The mean duration of postoperative delirium for the donepezil group was 1.0 day (standard error, 0.0), whereas for the placebo group it was 1.3 days (standard error, 0.19). There were no other outcomes measured for the patients who developed delirium. The investigators concluded that there is no evidence from controlled trials that donepezil is effective in the treatment of delirium. In a recent systematic review that was not specific to studies conducted in older adults, the investigators did not find any evidence for the efficacy of acetylcholinesterase inhibitors in either the prevention or the management of delirium. 23
Given this conflicting information available in the literature, we wanted to systematically evaluate the evidence for the use of acetylcholinesterase inhibitors in the prevention and management of symptoms of delirium in older adults (≥60 years) from RCTs. If there is good evidence for the efficacy of acetylcholinesterase inhibitors in the prevention or management of symptoms of delirium in older adults, then these drugs could be used in lieu of or in addition to the antipsychotics. 24 Antipsychotics appear to have some efficacy in the prevention and management of symptoms of delirium, but their use is associated with serious adverse effects including cerebrovascular adverse effects and death, especially in individuals with cognitive impairment. 25
Search Strategy
This systematic review was conducted in accordance with the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 26 The purpose of this review is to evaluate the data on the efficacy and tolerability of acetylcholinesterase inhibitors for delirium in the older adults (≥60 years) from RCTs. We performed a literature search of PubMed, MEDLINE, EMBASE, PsycINFO, and Cochrane collaboration databases through June 30, 2015, using the following key words: acetylcholinesterase inhibitors, donepezil, rivastigmine, galantamine, delirium, and RCT. The search was not restricted by the age of the participants or the language of publication of the study. However, in the final analysis, we only included studies involving humans that were published in English-language journals or had official English translations. In addition, we reviewed the bibliographic databases of the published articles for additional studies.
Two of the authors (RRT and DJT) reviewed all the abstracts and full-text articles from the citations obtained via the search of the databases. The decision on which studies to be included or excluded from the final analysis was done after a review of the full-text articles by all the authors. Disagreements between the authors were resolved by a consensus. The quality of the included studies was assessed using the criteria developed by the Center for Evidence-Based Medicine (Figure 1). 27
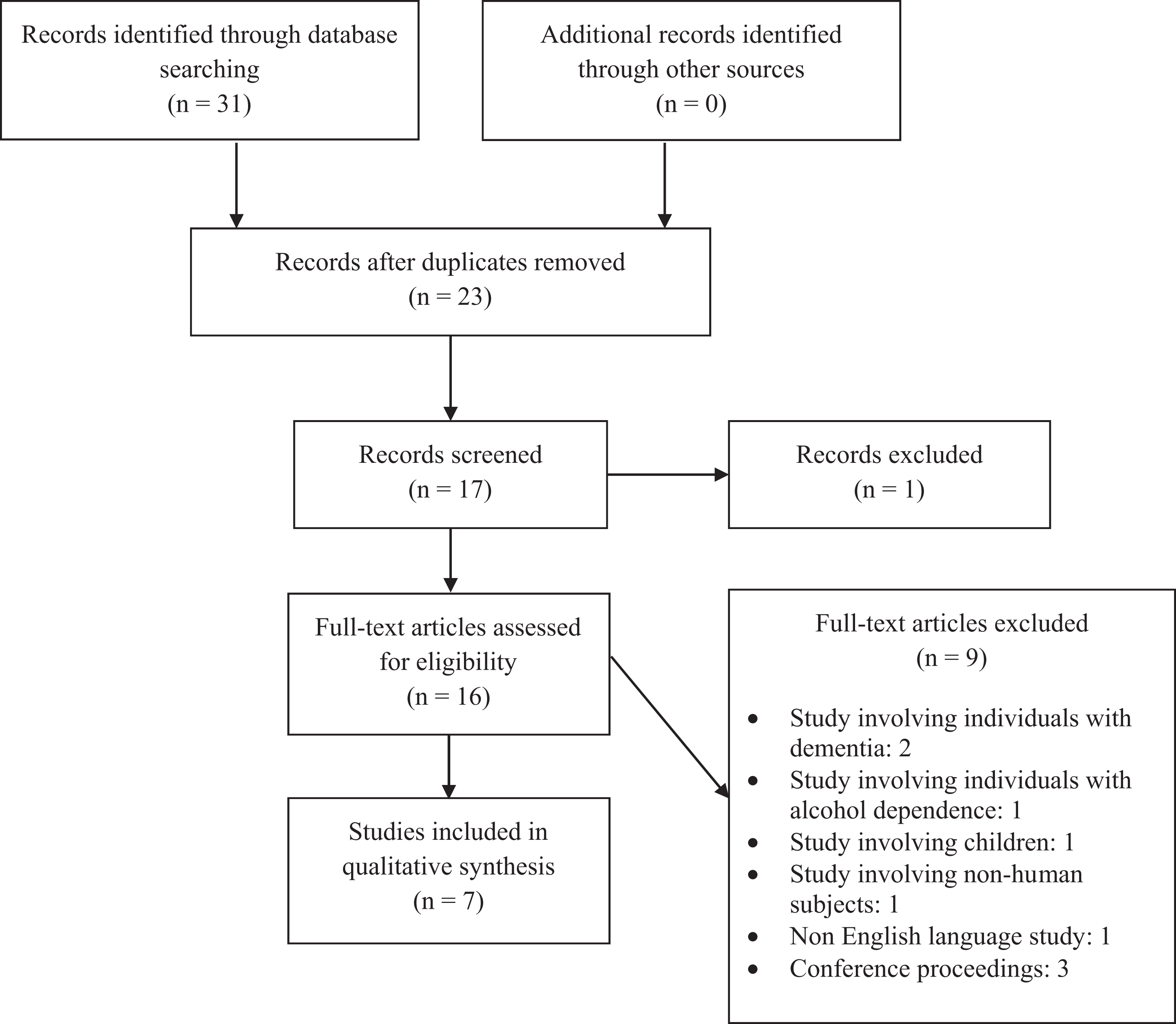
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
Results
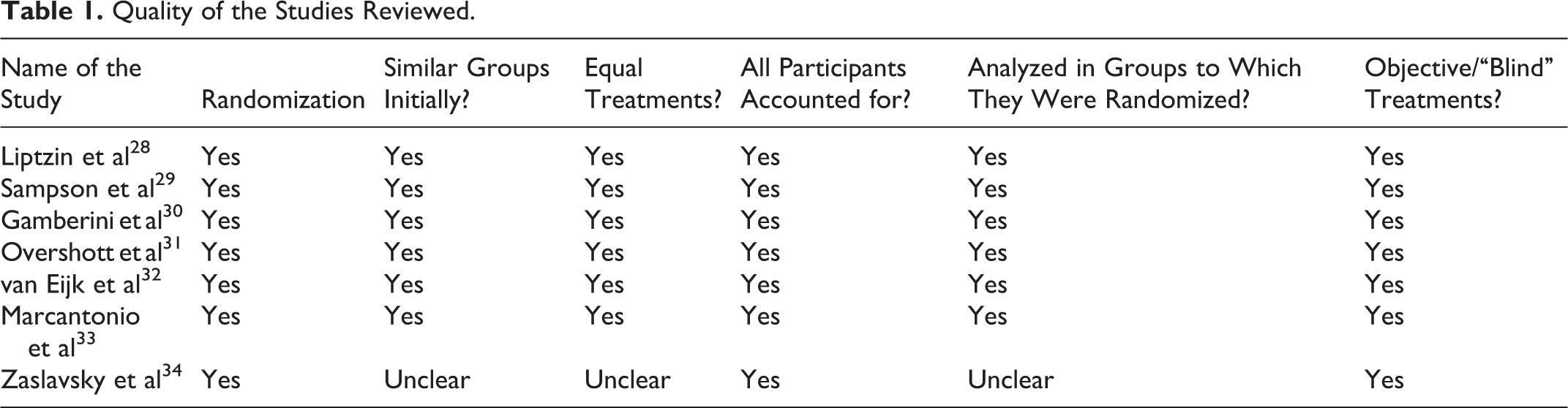
This systematic review of the literature identified a total of 7 RCTs that evaluated the efficacy of acetylcholinesterase inhibitors for the prevention and management of delirium in older adults (≥60 years). 28 –34 Six of the 7 studies were of good quality based on the criteria developed by the Center for Evidence-Based Medicine. 28 –33 Available data from 1 published study was limited (Table 1). 34
Quality of the Studies Reviewed.
Of the 7 studies, 5 were conducted in surgical settings. 28 –30,33,34 Three of these 5 studies included individuals who were awaiting skeletal joint repair surgeries. 28,29,33 Of the 2 other studies, one involved patients with cardiac disease 30 and one included individuals awaiting elective surgical procedures. 34 The study by Overshott et al was conducted in a medical setting. 31 The study by van Eijk et al included individuals in ICU who had medical and/or surgical problems (Table 2). 32
Summary of the Included Studies.
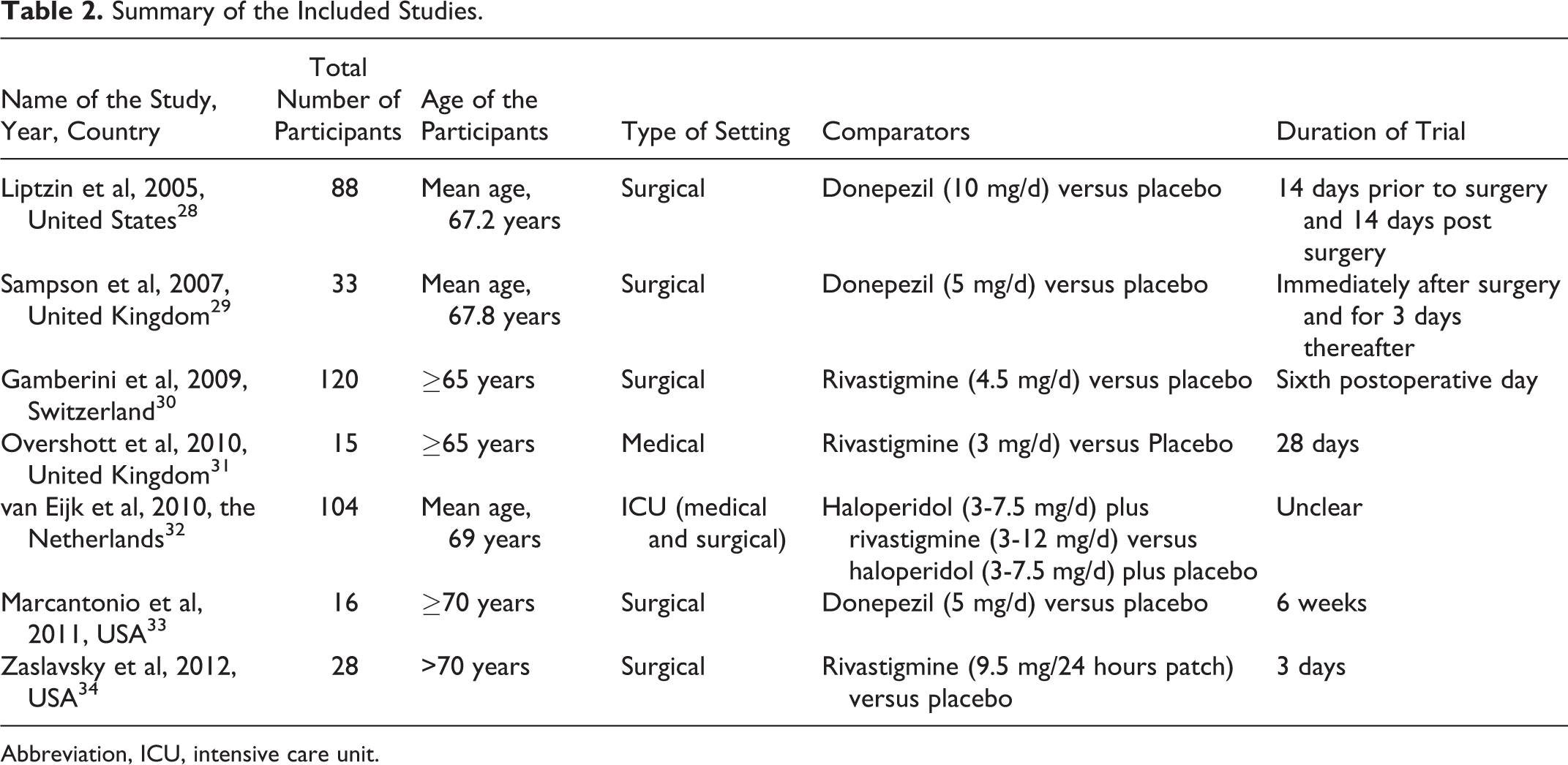
Abbreviation, ICU, intensive care unit.
Four of the 7 studies involved rivastigmine, 30 –32,34 and 3 studies used donepezil. 28,29,33 All 3 studies involving donepezil were conducted in surgical patients. Two of the 4 rivastigmine studies were conducted in surgical patients. 30,34 Six of the 7 studies compared an acetylcholinesterase inhibitor with placebo. 28 –31,33,34 In one study, rivastigmine or placebo was added to treatment with haloperidol. 32
The number of participants in these studies varied from 15 to 120. The duration of these studies varied from 3 days to 6 weeks. Four of the 7 studies targeted the prevention and management of delirium in older adults. 28 –30,33 Two studies targeted the management of delirium, 31,32 and 1 study evaluated the prevention of delirium. 34
Three of the 4 studies that evaluated the efficacy of acetylcholinesterase inhibitors in the prevention and management of delirium did not find benefit for the active drug when compared to placebo for either the prevention or the management of delirium. 28,30,33 The study by Sampson et al showed a trend toward benefit for the donepezil group when compared to the placebo group on the incidence of delirium and the length of hospital stay, but both outcomes did not attain statistical significance. 29 One of the 2 studies that evaluated the efficacy of an acetylcholinesterase inhibitor in the management of delirium found no benefit for the active drug in reducing the duration of delirium. 30 In the second study, the investigators found that the duration of delirium and the length of hospital stay were longer in the haloperidol plus rivastigmine group when compared to the haloperidol plus placebo group. 32 The only study that exclusively evaluated the efficacy of an acetylcholinesterase inhibitor for the prevention of delirium found no benefit for the active drug when compared to placebo. 34 There was no evidence for differential efficacy of acetylcholinesterase inhibitors when comparing studies involving patients in surgical settings 28 –30,33,34 versus patients in medical settings (Table 3). 31–32
Summary of Results From the Included Studies.
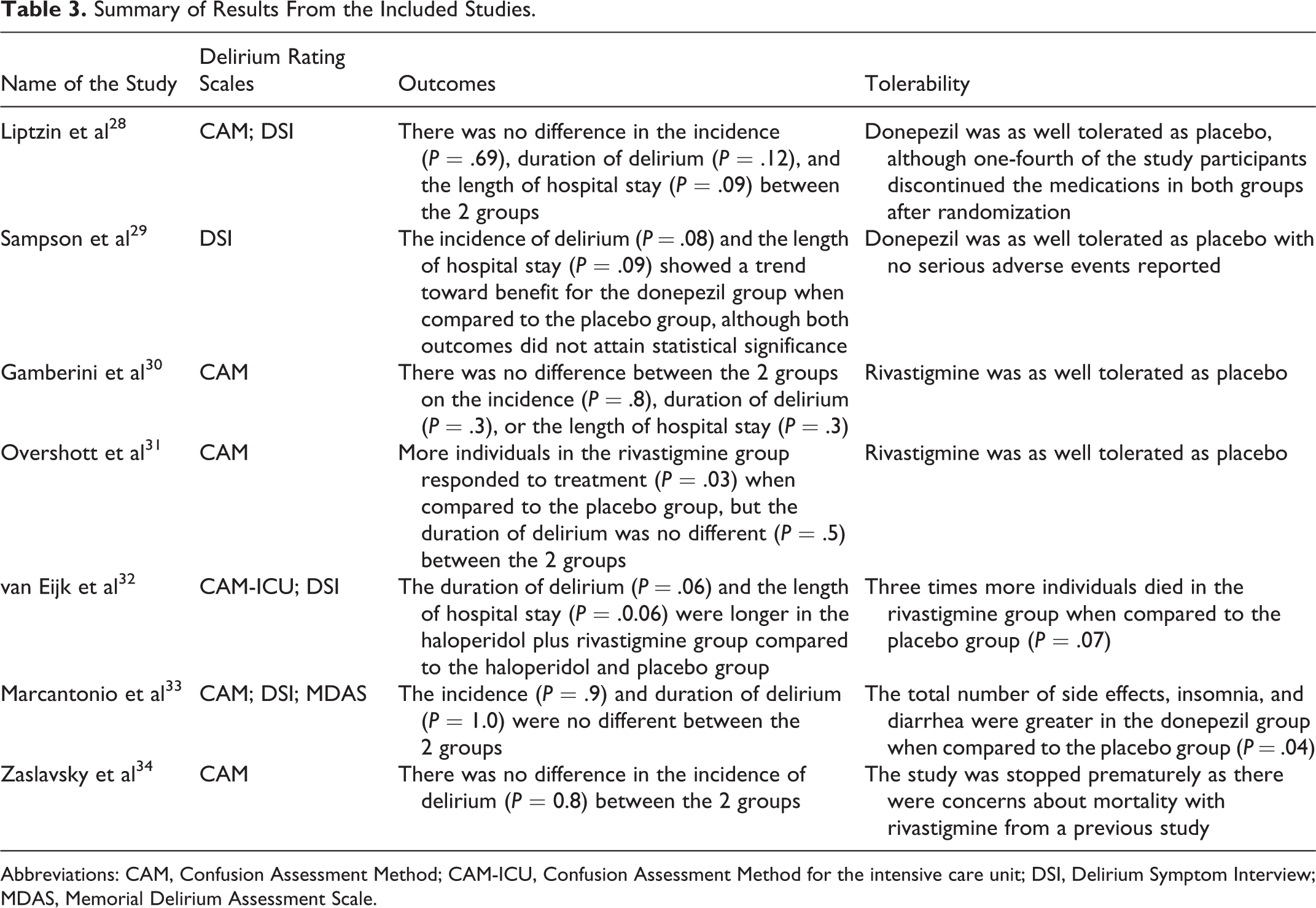
Abbreviations: CAM, Confusion Assessment Method; CAM-ICU, Confusion Assessment Method for the intensive care unit; DSI, Delirium Symptom Interview; MDAS, Memorial Delirium Assessment Scale.
The acetylcholinesterase inhibitors were well tolerated in 4 of the 7 studies, with the side-effect profile of the drug being similar to that of placebo. 28 –31 In the study by van Eijk et al, rivastigmine or placebo was added to treatment regimen with haloperidol in critically ill patients in ICUs. 32 In this study, the mortality rate was found to be almost 3 times higher in the group receiving haloperidol and rivastigmine when compared to the group receiving haloperidol and placebo (22% vs 8%, P = .07). The reason for the higher mortality rate in the rivastigmine group is unclear, and investigators opined that it could be possibly due to chance. In the study by Marcantonio et al, the side effects were greater in the donepezil group when compared to the placebo group. 33 The study by Zaslavsky et al 34 was stopped prematurely due to the increased risk of death noted with rivastigmine in older adults with delirium that was identified in the study by van Eijk et al. 32
Discussion
The data available from this systematic review indicate that acetylcholinesterase inhibitors cannot be recommended for the prevention or management of delirium in older adults. Although 6 of the 7 RCTs evaluated in this review were of good quality, these studies were underpowered to detect a difference between the active drug and placebo. Additionally, there was significant heterogeneity among the various studies. These studies were conducted in 4 different countries and used different validated methods to identify and manage delirium. These studies also used different dose equivalents of drugs, dosing strategies, and duration for the prescription of the drugs. Also, the disease burden among the participants in these studies was varied. Furthermore, one of the 2 larger studies included in this review had to be terminated prematurely due to the increased risk of death noted in the haloperidol and rivastigmine group when compared to the haloperidol and placebo group. 32
How do these data compare with the data on antipsychotic medications for the prevention of or in the management of delirium in older adults? In a meta-analysis by Lonergan et al that included data from 3 studies, the investigators found that the reduction in delirium scores was similar between the group of individuals who were treated with low-dose haloperidol (<3.0 mg/d) and groups treated with olanzapine or risperidone (odds ratio: 0.63, 95% confidence interval [CI]: 1.029-1.38, P = .25). 35 Low-dose haloperidol did not have a higher incidence of adverse effects when compared to the atypical antipsychotics, but high-dose haloperidol (>4.5 mg/d) was associated with a greater incidence of extrapyramidal adverse effects when compared with olanzapine. A meta-analysis that included data from 5 trials found that prophylaxis with antipsychotics reduces the incidence of delirium in older individuals receiving surgical procedures by about 50% when compared to placebo (relative risk: 0.51, 95% CI: 0.33-0.79, P < .01). 36 Data from 4 of the 5 studies indicated that prophylaxis with antipsychotic medications resulted in a reduction in the incidence of delirium (number needed to treat, 4.00-12.6). When compared to the data on antipsychotic medications, the data for using acetylcholinesterase inhibitors for the prevention or management of delirium in older adults is significantly weaker, with 5 of the 7 studies showing no benefit for the drugs and 1 study showing a worse outcome.
Despite a search strategy that was optimized toward identifying studies using acetylcholinesterase inhibitors for the prevention or management of delirium in older adults, the data we obtained were identical to the data obtained by Friedman and colleagues in their systematic review. 23 Our conclusions are also consistent with those of Friedman and colleagues.
Given the lack of evidence for the efficacy of acetylcholinesterase inhibitors for the prevention or management of delirium in older adults from 2 systematic reviews, is there a place for using these drugs for delirium in older adults? Unless data from larger well-conducted RCTs that are powered to detect a clear difference between acetylcholinesterase inhibitors and other active drugs or placebo are demonstrated, these drugs cannot be recommended for routine use in either the prevention or the management of delirium in older adults.
The strengths of this study include the systematic nature of the collection of data using different search terms from 5 large databases. Also, there were no time or language restrictions placed with the initial study search. Only 1 study was excluded from the final review due to a language restriction as it was in Russian and no official English translation was available.
The limitations of this review include the use of data exclusively from published RCTs. We only found 7 published RCTs on the use of acetylcholinesterase inhibitors in older adults with delirium. Majority of these studies were not adequately powered to detect a meaningful difference in outcomes between the active drugs and placebo. In addition, there was significant heterogeneity between the study populations, that is, surgical versus medical versus ICU patients. Five of the 7 studies involved surgical patients, whereas 1 study involved medical patients and 1 study involved patients in ICU. Also, did the adverse outcomes noted in the study by van Eijk et al occur as their study population in the ICU had greater burden of illness than individuals in the other studies? Furthermore, we did not utilize statistical methods to evaluate the heterogeneity between the included studies or assess the efficacy or tolerability of the active drugs.
Conclusion
The data from this systematic review does indicate the efficacy of acetylcholinesterase inhibitors for the prevention or management of delirium in older adults. Although these drugs were well tolerated in 4 of the 7 studies included in this review, there was concern from one study for greater mortality with rivastigmine. Strongly positive data from larger well-conducted RCTs will be needed before these drugs can be recommended for routine use in either the prevention or the management of delirium in older adults.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.