
Abstract
Characteristics of early- and late-onset dementia family caregivers were described and compared. Based on a theoretical model of role transition, data were collected through structured interviews from 48 caregivers of adults with Alzheimer’s disease or a related dementia older than the age of 70 and 48 caregivers of similarly diagnosed adults younger than the age of 60. A significantly higher proportion of caregivers of younger adults were spouses and gainfully employed compared with those of older adults; they had more years of schooling, took care of a person with more severe impairments, received more help, perceived themselves as better prepared to deal with future needs, and better informed about services. They did not differ from caregivers of older adults in terms of psychological distress, role confidence, self-efficacy, and social support. This study highlights differences and similarities to be considered in the development of services tailored to the specific needs of each group.
Introduction
In Canada as in many other countries, statistics show that a growing number of families are caring for a cognitively impaired relative with Alzheimer’s disease (AD) or a related dementia. 1 Over the past few decades, numerous studies have documented the experience of family caregivers of older adults with dementia as well as the impact that caring for these older adults has on various dimensions of the quality of life of their family members and significant others. 2 -4 Management of older adults with dementia is particularly demanding, especially on account of the near-constant supervision that the situation requires and the profound disruption of the relationship between caregiver and care recipient due to communication difficulties, increasingly asymmetrical and nonreciprocal exchanges, and disruptive behaviors often associated with the disease. 5,6 It is now recognized that the caregiver role has numerous repercussions not only on one’s physical and mental health but also on one’s personal and social life. In this context, many psychoeducational programs designed to help late-onset dementia family caregivers enact their role have been the subject of evaluative studies and meta-analyses. 7,8
However, the number of adults with early-onset dementia has been on the rise and little is known about the impact on family caregivers of managing such cases. The few studies conducted on the subject to date have observed that the level of stress of these family caregivers was equal to, if not higher than, that of family caregivers of adults with late-onset dementia. 9,10 The characteristics of early-onset dementia include a broader spectrum of expression, pervasiveness of certain cognitive symptoms, severity of neuropsychiatric signs, and changes in character and behavior. 11 In this regard, studies have demonstrated that early-onset dementia caregivers perceive a higher frequency and intensity of psychological and behavioral symptoms associated with dementia. 9,11
These few findings notwithstanding, much less is known about the characteristics of early-onset dementia caregivers than about their late-onset counterparts. Moreover, the empirical data do not yet allow clearly differentiating their specificities. In fact, the differences between the characteristics of these 2 groups of family caregivers of adults with AD or a related dementia are insufficiently documented to make it possible to propose support programs and services tailored to their specific needs. In this regard, it has been recommended for almost 2 decades that the content of intervention programs be modulated as a function of the different phases of the caregiver career, given that the process of adapting to a new situation occurs within a specific context. 12 Furthermore, carrying out interventions in a timely fashion allows the temporal dimension of the caregiver career to be taken into account. Interventions offered at particular points in time are more likely to be effective than those provided without consideration of the caregiver’s own care trajectory. 13,14
Against this background and in the aim of opening up differential avenues for clinical interventions by health and social services professionals to support family caregivers, we undertook to describe and compare characteristics of early- and late-onset dementia caregivers.
Theoretical Framework
We selected a theoretical framework suited to describe and compare the phenomenon of family caregiver role acquisition, namely, the role transition model developed by Meleis and colleagues. 15 According to this model, transition constitutes a period of instability accompanied by uncertainty. It represents the passage from one state or condition to another. Transition is associated with life development stages or with specific situations, such as the passage toward new roles, including that of family caregiver. Successful role transition in this case is characterized by the acquisition of new knowledge and skills, perceived self-efficacy in the face of the caregiving situation, coping strategies, and satisfactory relations with the social support networks, both formal (services) and informal (family and friends).
Method
Design
A comparative descriptive design was employed for the purposes of the study.
Setting and Sample
This multisite study was carried out in the province of Quebec, Canada, with a cohort of French-speaking family caregivers. Participants were recruited in cognition clinics across Quebec where geriatricians, neurologists, and psychiatrists regularly diagnose dementia as well as in Alzheimer societies where adults diagnosed with dementia are often referred. Two samples were formed, one consisting of 48 family caregivers of adults older than the age of 70 with late-onset dementia and another of 48 family caregivers of adults younger than the age of 60 with early-onset dementia. The persons cared for were diagnosed with AD or a related dementia (frontotemporal dementia, Lewy body dementia, Pick’s disease, vascular dementia, and mixed dementia). Participants in both samples had to meet the following selection criteria: be the person principally responsible for (notion of primary caregiver) a relative older than the age of 70 (sample 1) or younger than the age of 60 (sample 2) diagnosed with AD or a related dementia in the past 36 months. Participants were recruited by consecutive sampling based on whether they met the selection criteria. The number of participants was determined on the basis of study feasibility criteria and minimal requirements for running parametric statistical analyses.
Data Collection
The data collection period ran from September 2011 to September 2013. The caregivers were administered a standardized interview. The following sociodemographic data of the caregivers were gathered first: sex, age, income, years of schooling, kinship tie with relative, duration of caregiving, and cohabitation with relative. Data were collected also on services received (eg, housekeeping, home-delivered meals, personal care, nursing care, in-home respite care, and day center). Moreover, sociodemographic data (sex and age) were collected on the cared-for relatives as were data on the caregiving context. More specifically, relative’s degree of functional autonomy in activities of daily living (ADL; eg, eat, dress, and use the toilet) was gauged by caregivers on a 9-item scale. 16 The choice of responses ranged from “entirely able to perform activity” (1) to “not at all able” (5). Consequently, the theoretical score range was 9 to 45. The scale obtained an α coefficient of .82 in our study.
Relative’s degree of functional autonomy in instrumental activities of daily living (IADL) was evaluated with an instrument, 16 comprising 4 items (eg, using telephone and taking medication) for which the caregiver once again had to rate the cared-for relative’s ability, this time on scale of 1 (entirely able) to 4 (entirely unable). This scale had a theoretical score range of 4 to 16 and obtained an α coefficient of .73 in this study.
Finally, to document degree of severity of relative’s cognitive impairment, caregivers were asked to complete the 8-item Cognitive Status Scale developed by Pearlin and colleagues. 17 Research has demonstrated the validity of family informant ratings of a relative’s cognitive status. 18,19 The instrument has a theoretical score range of 0 (low) to 32 (high). Pearlin and colleagues obtained a correlation of .65 between caregiver report on the scale and the Mini-Mental State Examination 20 completed by professionals. The scale obtained an α coefficient of .81 in this study.
In addition, based on the theoretical framework of the study, 15 the following characteristics of the transition to the caregiver role were also measured: (1) preparedness for caregiving, (2) role confidence, (3) planning for future care needs, (4) knowledge of formal services, (5) self-efficacy, (6) coping strategies, (7) informal social support, (8) potential conflicts between family members and caregiver over perception of the caregiving situation, and (9) level of psychological distress experienced. These characteristics were measured using standardized instruments with sound psychometric properties employed in previous longitudinal caregiving studies. All measures were translated into French following a parallel back-translation procedure. 21
Measures
Preparedness for caregiving
The 8-item Preparedness for Caregiving Scale 22 served to measure degree of caregiver preparedness to provide care (eg, “How well prepared do you think you are to take care of your family member’s physical needs?”). The measure was evaluated in a methodological study with 50 caregivers of elderly relatives. 22 The choice of responses ranged from 1 (not at all prepared) to 5 (very well prepared). In our study, the instrument obtained α coefficients of .89 for caregivers of younger adults and .85 for caregivers of older ones.
Role confidence
The Self-Efficacy Scale 23 was used to measure this dimension. The scale comprises 15 items on which caregivers rate their level of confidence in dealing with caregiving situations (eg, dealing with your need to maintain most of your daily activities). The choice of responses ranges from 1 (not at all confident) to 5 (extremely confident). We obtained α coefficients for our 2 samples of .87 and .88.
Planning for future care needs and knowledge of formal services
These dimensions were evaluated using 2 scales developed by Sörensen and Pinquart 24 and validated on a sample of 590 older adults. The Planning for Future Care Needs Scale covered decisions made by caregivers to meet their relative’s future care needs (6 items; eg, “I have compared different options of help or care in the future and have decided which would work for me and which would not.”). The Knowledge of Services Scale served to assess how much caregivers were familiar with services (7 items; eg, “I know which home healthcare agencies are active in my area.”). For both scales, the choice of responses ranged from 1 (not at all true for me) to 5 (completely true for me). The α coefficients obtained with our 2 samples were .83 and .85 for the Planning for Future Care Needs scale and .86 and .88 for the Knowledge of Services Scale.
Self-efficacy
We used the Revised Scale for Caregiving Self-Efficacy 25 to measure this dimension. This scale comprises 3 subscales that specifically measure caregiver’s ability to obtain respite from family and friends (5 items; eg, asking a friend or family member to stay with your relative for a day when you want to take a break), to control disturbing thoughts about the caregiver role (5 items; eg, injustice of having to manage the situation), and to respond to relative’s disruptive behaviors (5 items; eg, responding without raising voice when relative interrupts activities repeatedly). Respondents rate their degree of self-efficacy on an analog scale from 0 (absolutely incapable) to 100 (fully capable). In our study, the subscales obtained α coefficients from .74 to .92.
Coping strategies
The Carers’ Assessment of Managing Index was used to assess frequency of utilization of the following 3 coping strategies: problem solving (13 items; eg, “Thinking about the problem and finding a way to solve it”), reframing (14 items; eg, “Realizing that the person you care for is not to blame for the way they are”), and stress symptoms management (9 items; eg, “Setting a little free time aside for yourself”). Developed by Nolan et al, 26 this tool was validated on a sample of 266 caregivers. The French-language version had previously been used in studies involving French-speaking Quebec caregivers. 27,28 Respondents rated frequency of utilization of these strategies on a scale of 1 (never/almost never) to 4 (very often/always). The α coefficients obtained in our study ran from .59 (stress management) to .76 (reframing). The stress management subscale was subsequently excluded from the analyses on account of its low α.
Informal social support
We used the Inventory of Socially Supportive Behaviors 29 to determine frequency of support received by caregivers from family (excluding the cared-for relative), friends, and neighbors. The French-language version of this instrument, which was validated on a sample of French-speaking caregivers, 30 showed the same robust psychometric properties as the original scale. The 3 subscales covered emotional support (11 items; eg, expressed interest in caregiver; α = .85), informational support (7 items; eg, indicated a person to see in order to obtain help; α = .81), and instrumental support (9 items; eg, provided caregiver with transportation; α = .60). Items were rated on a 4-point scale ranging from 1 (never/almost never) to 4 (very often/always). Cronbach’s αs in this study ranged from .64 (instrumental support) to .88 (emotional support). The instrumental support subscale was ultimately excluded from the analyses for having an α below .70.
Family conflicts
The Family Caregiver Conflict Scale 31 served to measure level of conflict between caregivers and family members. The 15-item instrument concerns disagreements over general aspects of caregiving (eg, ask the family to help me take care of my relative). Respondents had to indicate on an analog scale from 1 (not at all true) to 7 (very true) the degree to which each of the disagreements described applied to their situation since diagnostic disclosure. In our study, the instrument obtained α coefficients of .93 with caregivers of younger adults and .87 with those of older adults.
Psychological distress
We used the Psychological Distress Index (PDI), an adapted version of the Psychiatric Symptom Index, 32 to measure this variable. The 14-item instrument, of which both the French- and English-language versions have proved psychometrically sound, 33 had previously been used in a large-scale health survey of the Quebec population. 34 Respondents rated how often (1 = never/almost never to 4 = very often/always) they felt distressed in the past week (eg, “feeling tense or under stress”). The α coefficients obtained for the instrument were .87 and .90, respectively, with one and the other sample.
Procedure
This multisite project was approved by the Research Ethics Board of the Research Centre of the Institut universitaire de gériatrie de Montréal. A professional at each recruitment site was tasked with contacting potential participants to obtain their consent to forward their contact information to the project’s researchers. Then, the project coordinator contacted the caregivers to explain the objectives of the study, solicit their participation, and verify whether they met the inclusion criteria. Interviews were held at the Research Centre, at an Alzheimer society, or at home, at the participant’s discretion and convenience. The standardized interview took place only after the participant received an information sheet on the study and signed a consent form. Interviewers received 2 days’ training, for which a training guide designed by the researchers was used. Interviewers were professionals with mental health expertise. Interviews lasted on average 90 minutes.
Data Analysis
Descriptive statistics (means, standard deviations, and percentages) were calculated for the purpose of drawing the sociodemographic profile of the participants in both caregiver groups and that of their cognitively impaired relatives. The t tests and chi-square tests were performed to compare the 2 groups of caregivers and care recipients depending on whether the variables were, respectively, continuous or categorical. Data on characteristics of the caregiving context were compared using Hotelling’s T-square test, a robust multivariate test used when assumptions of normality and homogeneous covariance matrices are not met in cases where 2 samples are of equal size. 35 -37 These characteristics were grouped together conceptually for the multivariate analyses. Thus, the first of the 6 groups of variables concerned the relative’s impairments in 3 spheres, namely, ADL, IADL, and cognition. A second block of variables focused on confidence and preparedness of caregiver role. These included sense of being well prepared, degree of confidence, preparedness to face future needs, and knowledge of services. The next group of variables covered self-efficacy or self-perceived ability to request respite care, deal with relative’s behaviors, and control disturbing thoughts. The fourth group of variables had to do with strategies for facing the caregiving situation, including the coping strategies of problem solving and reframing. Variables regarding frequency of informational, instrumental, and emotional support received from the informal social network and perceived family conflicts made up the fifth group of variables. Finally, psychological distress was the last variable considered in the analyses (univariate analysis for this single indicator). When multivariate analysis results proved significant, t tests were performed to identify the variables that contributed to intergroup differences.
Results
Sociodemographic Characteristics of Family Caregivers
Caregivers in the early-onset group looked after persons with various types of dementia, namely, AD (64.5%), frontotemporal dementia (16.7%), Pick’s disease (4.2%), Lewy’s body dementia (2.1%), vascular dementia (2.1%), and mixed dementia (10.4%). The late-onset group was less heterogeneous in this regard, as caregivers looked after persons with AD (89.6%) or mixed dementia (10.4%) only. Table 1 gives these sociodemographic characteristics by caregiver group, that is, for the caregivers of younger adults and those of older ones.
Sociodemographic Characteristics of Caregivers by Group.
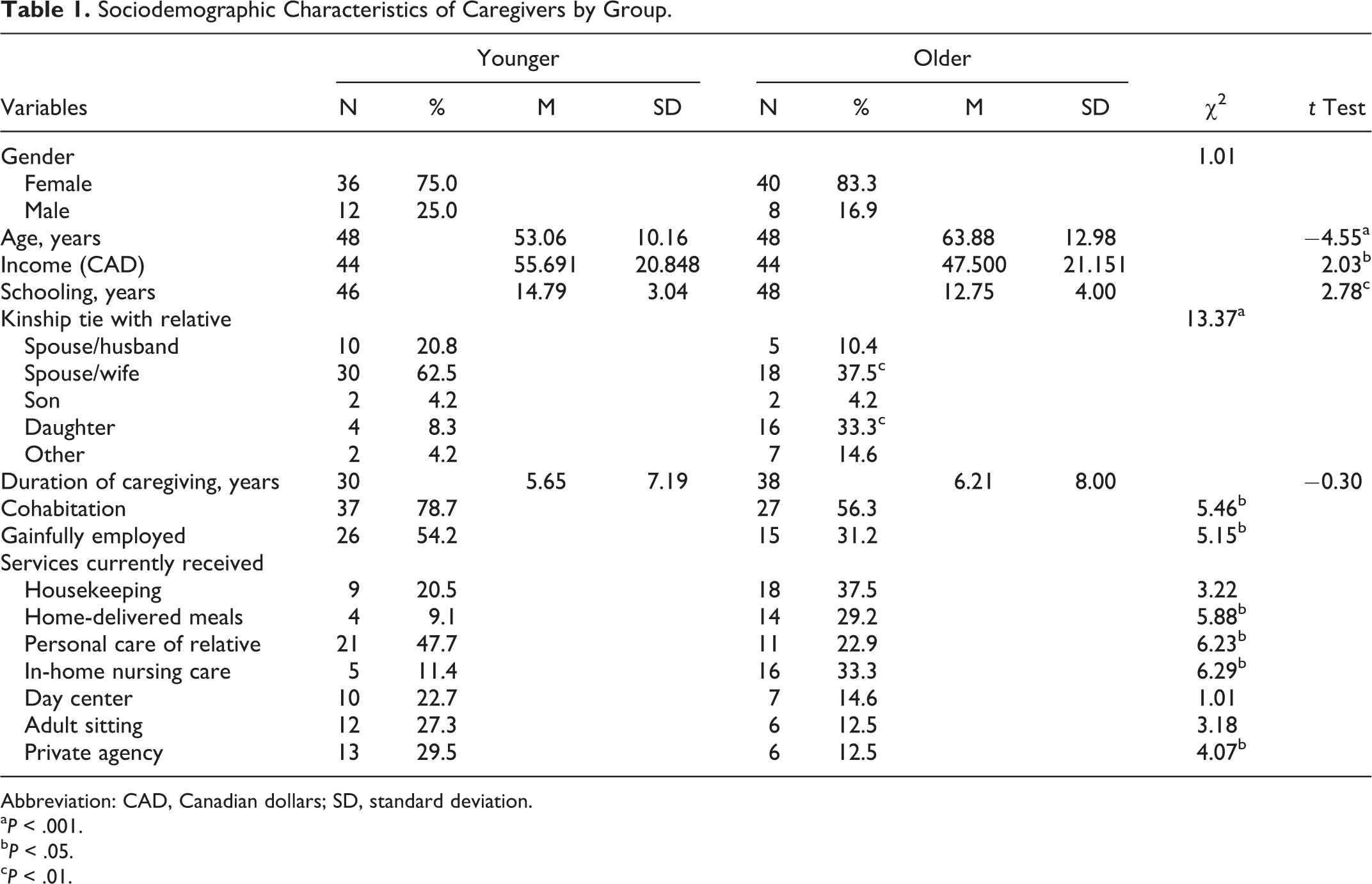
Abbreviation: CAD, Canadian dollars; SD, standard deviation.
a P < .001.
b P < .05.
c P < .01.
Overall, most of the caregivers were female and the results underscored the significant age difference between the 2 groups of caregivers. The early-onset dementia caregivers had more resources at their disposal to cope with their caregiving situation. In this regard, they enjoyed higher income, had significantly more years of schooling, and more of them were gainfully employed, compared with the late-onset dementia caregivers. Regarding kinship tie between caregiver and care recipient, there were significantly more female spouses in the younger group than in the older group and significantly more daughters in the older group than in the younger group. Despite the age difference between the 2 caregiver groups, the length of time the younger caregivers had been caring for their relative was not significantly different from that reported by their older counterparts, exceeding 5 years in both cases.
The group of early-onset dementia caregivers was composed mostly of female spouse caregivers (62.5%) cohabiting with their partner and gainfully employed. Among the late-onset dementia caregivers, the distribution of kinship ties was more heterogeneous, with a larger proportion of daughter caregivers (33.3%) who often did not cohabit with their cared-for relative.
Caregivers of younger adults received significantly more services for personal care and were more likely to use the services of private agencies. The caregivers of older adults, instead, received more support with meals (home-delivered meals) and more in-home nursing care. Regarding the cared-for relatives, there was a higher proportion of women in the older group (47.9% vs 27.2%). Mean age of the younger sufferers was 58 years, compared with 79 for their older counterparts (statistically significant difference).
Comparison Between Caregiver Groups on Variables Related to the Caregiving Context and to Transition to the Caregiver Role
Table 2 gives the mean scores obtained on the various scales measuring variables related to the caregiving context and to role transition for the 2 groups, the results of the multivariate analyses (Hotelling’s T2 test) and of the t tests on differences in means, and the results of the univariate analysis of psychological distress.
Comparison of Group Means.
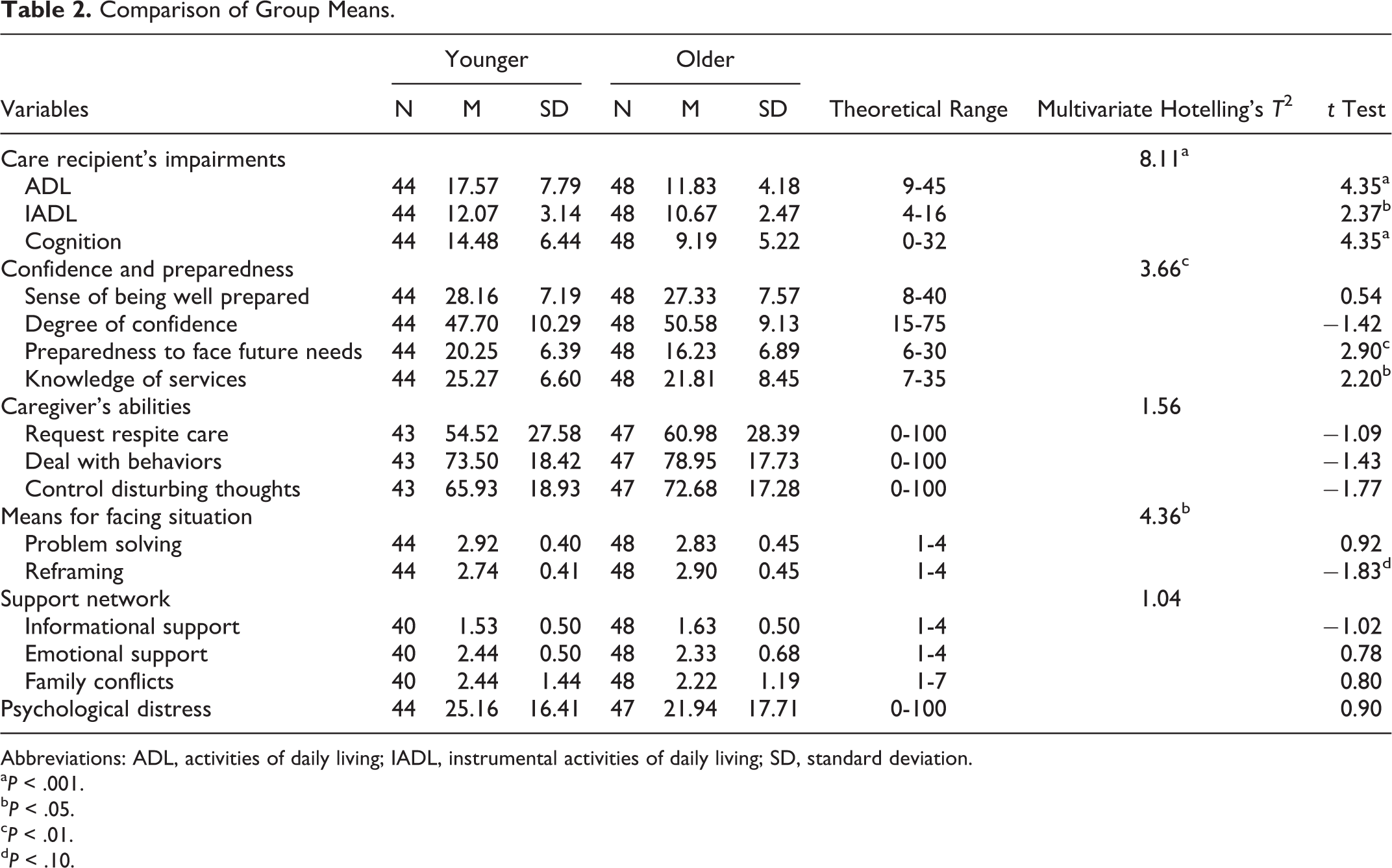
Abbreviations: ADL, activities of daily living; IADL, instrumental activities of daily living; SD, standard deviation.
a P < .001.
b P < .05.
c P < .01.
d P < .10.
The results revealed that, in general, adults with early-onset dementia presented more severe impairments. More specifically, these younger sufferers were significantly more impaired in ADL (partial η2 = .180) and IADL (partial η2 = .080). Moreover, their cognitive status was significantly more deteriorated than that of their older counterparts (partial η2 = .173).
The early-onset dementia caregivers perceived themselves to be better prepared to deal with the future needs of their cared-for relatives (partial η2 = .085) and to be better informed about services (partial η2 = .050). Otherwise, aside from a tendency toward less use of the coping strategy of reframing (significant multivariate analysis; partial η2 = .036), caregivers of younger adults did not differ from those of older adults on the other variables considered, be it sense of preparedness for caregiving, degree of confidence, perceived self-efficacy in requesting respite care, dealing with their relative’s behaviors or controlling their disturbing thoughts, perceived informal social support or presence of family conflicts. Nor did caregivers of younger adults differ significantly in terms of psychological distress. However, they did score higher on this dimension compared with their older counterparts and a higher proportion reached the PDI’s “high” distress threshold, based on the norms established by age (85th percentile: 40.9% younger vs 25.5% older).
In sum, the overall results of the study revealed that the 2 caregiver groups differed significantly on selected variables. More specifically, at the sociodemographic level, caregivers of younger adults had significantly more resources at their disposal (income and education) and significantly more of them were gainfully employed. This group comprised significantly more female spouse caregivers and significantly fewer daughter caregivers and a significantly higher proportion lived with the care recipient, compared with the group of caregivers of older adults. Moreover, caregivers of younger adults received more services for the personal care of their relative and more services from private agencies when caregivers of older adults received significantly more home-delivered services and in-home nursing care. As for the care recipients, the 2 groups differed in terms of impairment, with the younger adults more heavily impaired in terms of cognition, ADL, and IADL.
Finally, regarding variables related to the experience of the caregiver role transition, the caregivers of younger adults felt better prepared to face future needs and had better knowledge of services. However, in terms of coping strategies, these caregivers used reframing less often than did the caregivers of older adults to deal with problem situations.
Discussion
The aim of our study was to describe and compare characteristics of family caregivers of adults with AD or a related dementia younger than the age of 60 (early-onset dementia) and older than the age of 70 (late-onset dementia), respectively. At the sociodemographic level, the data obtained show that, despite the fact that early-onset dementia caregivers are younger and that dementia is more prevalent among women, 1 women continue, in line with numerous statistical profiles of family caregivers, 38,39 to be the ones in large part to assume this role, whether it be to care for a younger or older adult. Given the trend toward smaller families in the Western World, the growing number of single-child families and the gradual shift in traditional gender roles, 5 we could have expected to see a higher proportion of men caregivers in the sample. This finding suggests that differential roles and responsibilities persist for men and women in the sphere of caregiving. 40
Moreover, a cohort effect may explain why the younger group had more resources in terms of both schooling and income. Also in connection with their age, they might have been socialized more to use services and help from outside their informal support network (family, friends, and neighbors). Owing to a smaller family network, these younger caregivers may be less affected by the phenomenon of reluctance to use services documented among caregivers of older adults in the past 2 decades. 41 They may even be more inclined to pay for help with their caregiver role. As for caregivers of older adults, their values and beliefs regarding help seeking, autonomy, and the importance of reciprocity in the exchange of services may constitute cultural markers that influence their weaker service utilization. 42
Still, despite their younger age, these caregivers had filled their role for as long as the caregivers of older adults and took care of more functionally and cognitively impaired relatives. Compared with the caregivers in the late-onset group, those in the early-onset group looked after adults with a wider variety of dementia, including of the frontotemporal type. As mentioned before, early-onset dementia is often accompanied by numerous outward manifestations, including behavior problems. These are reportedly more significant and have a deeper impact on caregivers, particularly in the case of frontotemporal dementia. 43 These elements could certainly have had an influence on the results regarding the group of family caregivers looking after younger adults.
These caregivers are for the most part a spouse who, aside from already having a long trajectory of caregiving, faces a difficult caregiving context on a daily basis. 44 The fact of cohabiting round the clock with the cared-for relative, the proximity inherent in the spousal relationship, and the loss of identity that occurs when the normative spouse role is replaced with the caregiver role 45 undoubtedly modulate the caregiver’s perception of the caregiving context. This may explain some of the differences observed with the more heterogeneous group of late-onset dementia caregivers. As pointed out in the findings of various qualitative studies, 44,46,47 caregivers of younger adults are doubly stigmatized: They take care of a person with dementia and, what’s more, the sufferer, who is already stigmatized by the disease, is a young adult, which is far from normative.
If we take a closer look at the differences between the 2 groups regarding caregiving context, we note that caregivers of younger adults are better informed about services and feel better prepared to face the future. The fact of having more resources at one’s disposal, particularly in terms of schooling and income, may explain these differences in part. This younger cohort normally knows, among other things, how to browse the Internet for information on diagnoses, symptoms, and available support services. Moreover, the members of this cohort have, as mentioned before, learned to call upon professional help. It needs to be pointed out, also, that caregivers of younger adults are often gainfully employed and are forced to secure sitting services in order to keep working and avoid a loss of income at a young age.
Also, these younger caregivers do not perceive more self-efficacy or more frequent contacts with the members of their informal social network or fewer family conflicts. What’s more, they tend to make less use of the coping strategy of reframing than do caregivers of older adults. This supports the findings of other studies to the effect that the life experience of older adults allows them to develop a stronger capacity for cognitive restructuring. 48 Reframing is an internal coping strategy defined as the ability to approach problem situations differently in order to render them more manageable. 49 It is a form of coping that implies maturity. This may be why caregivers of older adults (who are themselves older) are able to make greater use of their personal resources to react to problem situations and major stressors in a more positive manner. 50
These comparative results are original and especially interesting for the purpose of developing targeted professional support interventions for dementia family caregivers. Our study provides data that highlight certain intergroup differences that should be taken into consideration in order to offer services tailored to the needs of each group. As mentioned by certain authors, 14,26 services must be designed according to the particularities of caregivers and their caregiving context in order to be effective. Many intervention programs have been developed for late-onset dementia caregivers. 7,8 However, in order to avoid a “one-size-fits-all” approach, more diversified forms of care and support delivered in various modalities, including information and psychoeducational interventions offered online, need to be developed and evaluated for early-onset dementia caregivers who often have more resources at their disposal. There is also a need to develop innovative forms of respite care for younger caregivers in the workforce and caregivers with children often still living at home. As the caregivers of younger adults are most often spouses who share their daily life with the care recipient, it is necessary to offer them support and respite adapted to their specific reality. Moreover, given the pervasiveness of certain cognitive symptoms, the severity of the neuropsychiatric signs, and the changes in character and behavior in younger adults with AD, the caregivers of these persons need to gain a better understanding of these behaviors and to learn skills to deal with them more effectively. Furthermore, although these caregivers report feeling better prepared to face the future and being more familiar with services, they are less inclined to use cognitive coping strategies, such as reframing. Fostering the acquisition of this type of coping strategy that allows cognitively restructuring difficult situations experienced on a daily basis and changing one’s perception must be considered in order to facilitate the family caregiver role transition.
Finally, despite certain limitations, including a relatively small sample, our study generated significant results through parametric analyses of data collected with psychometrically sound instruments measuring variables selected according to an explicit frame of reference for caregiver role transition. These variables, which were drawn from a theoretical model suited to the phenomenon under study, allowed documenting the caregiving context of early- and late-onset dementia family caregivers. Interventions must now be designed and evaluated in order to facilitate the transition to this demanding role—a transition differentially characterized by age of sufferer at onset.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Project funded by Fonds de recherche du Québec-Santé (FRQS), Canadian Institutes of Health Research (Canada), and Agence nationale de recherche (France).