
Abstract
On the first few days after admission to the Geriatric-Internal Medicine department, the suffering level of patients with advanced dementia (Mini-Mental State Examination 0 of 30) was evaluated according to the Mini-Suffering State Examination (MSSE). During hospitalization, 14.8% (27 of 183) of patients with advanced dementia were died with a mean survival rate of 19.86 ± 26.9 days. The MSSE scale score of died patients was 7.56 ± 1.71 during the first few days of admission which indicates high suffering levels. The MSSE scale score of survived patients with advanced dementia was 3.99 ± 2.10 which confirms their low level of suffering. There was a significant difference (P < .001) between the groups. Patients with dementia who died and were diagnosed as having Aminoff suffering syndrome during the first few days of admission had a high suffering level and short-survival time.
Keywords
Introduction
Over the last 50 years, medical research has sought techniques to diagnose short-survival time in end-of-life patients. Since the establishment of the St Christopher’s Hospice in South London in 1967 by Cicely Saunders, whose work is considered the basis of modern hospice philosophy, 1 definition and diagnosis of terminal and dying medical conditions of the patients have become most essential.
Difficulty in diagnosing short survival is a known problem for enrolling patients for palliative and hospice treatment, 2 -4 eligibility for Medicare and Medicaid insurance companies in the United States, 5 establishing “The Dying Patient Act” in Israel, 6,7 and also in performing the “Oregon’s project.” 8,9
National Medicare Guidelines for determining prognosis in dementia, 10 Stage Seven C of the Functional Assessment Staging (FAST 7c) scale, 11 the Karnofsky performance scale, 12 and the Charlson Comorbidity Index 13 are some available cutoff points for enrollment in a hospice. The FAST scale is not associated with survival in a long-term follow-up study of dementia. 14 The results of another study suggested that the Hospice Medicare Guidelines for predicting survival of patients were invalid. 15 The increased risk score on a dementia rating scale, such as FAST, Mitchell Novel Risk Score (MDS/Mitchell score), and the Advanced Dementia Prognostic Tool (ADEPT) scales, was a commonly identified risk factor for short survival in the majority of literature. 16,17 Aminoff proposed the Mini-Suffering State Examination (MSSE) scale as a key criterion for enrolling patients with advanced dementia to palliative settings. 18 Further studies are essential to identify reliable, sensitive, and specific prognosticators that can be applied to the clinical setting and allow increased availability of palliative care to patients with dementia. 19
Methods
Study Population
Over a 6-month period, we studied all patients with advanced dementia admitted to a Geriatric-Internal Medicine Ward of a tertiary general hospital. Diagnosis was based on the Diagnostic and Statistical Manual of Mental Disorders (Fourth edition, Text Revision) criteria for dementia. 20 Inclusion criteria included severe dementia interference in verbal communication (Mini-Mental State Examination [MMSE 0/30]), 21 complete dependence in activities of daily living and functional movement (Functional Independence Measure 18 of 126), 22 and Stage 7c or higher of the FAST scale. 11 We recruited patients diagnosed as having Alzheimer's disease, multiinfarct and poststroke dementias, and dementia of unknown origin. The final analysis was composed of 183 patients (73 males and 110 females), aged 56 to 102 years. The study was authorized by the local Hospital Helsinki Committee.
On the first few days of admission (2.9 ± 4.3 days) to the Geriatric-Internal Medicine Department, patients were evaluated with the MSSE scale. For each patient, the following data were collected: total protein, albumin (AL), cholesterol (Ch), hemoglobin (Hb), white blood cells, total lymphocyte count, C-reactive protein (CRP), body mass index, use of nasogastric tube, and percutaneous endoscopic gastrostomy (PEG). The use of medications, such as antipsychotics, antidepressants, narcotics, analgesics, antibiotics, and infusion, was recorded. Diagnosis of Parkinson's disease, space occupying lesion (SOL), and cerebral vascular accident was also recorded in the medical history.
The Mini-Suffering State Examination
The MSSE scale, developed in 1999 by Aminoff 23 and described by us, 24 is the first objective clinical tool for evaluation of suffering level in advanced dementia which could be useful for medical and nursing staff and also for family members of patients with dementia. The MSSE scale is available in English, Hebrew, and Dutch, 25,26 and the translation and validation of Spanish and German versions are in progress. The MSSE scale comprises 10 items relating to the patients’ characteristics as well as the perception of their conditions by medical staff and families. Each item scores 0 (no) or 1 (yes). The total score ranges between 0 and 10, with higher scores reflecting elevated degrees of suffering levels. Based on clinical experience, the following items were included in the MSSE: not calm, screams, pain, decubitus ulcers, malnutrition, eating disorders, invasive action, unstable medical condition, suffering according to medical opinion, and suffering according to family opinion. Family thought by their own feeling that the advanced dementia patient was suffering.
The MSSE scale was tested using the Cronbach α model, which demonstrated its significant reliability (α = 0.798). A κ agreement coefficient of 0.791 between 2 observers was found. Both observers found significant association between the higher MSSE levels and older age (P < .02); low levels of Hb (P < .02), AL (P < .001), and Ch (P < .04); and higher use of analgesics or antipsychotics (P < .04). Convergent validity of the MSSE scale was proven by Pearson’s correlation with Symptom Management in End-of-Life in Dementia scale (r = 0.574, P < .0001) and Comfort Assessment in Dying with Dementia scale 27 (r = −0.796, P < .0001).
A high MSSE scale score with range 7 to 10 indicates a high level of suffering and reflects the severity of the medical conditions in end-stage dementia. According to the MSSE scale, it has been confirmed that patients with end-stage dementia represent a heterogeneous group and have different levels of suffering, and accordingly proved a significant concurrent validity. The results of our previous research showed that care in a geriatric department fails to decrease the high level of suffering of patients with end-stage dementia. The total score of MSSE scale on the day of admission was 5.62 ± 2.31 and increased to 6.89 ± 1.95 on the last day of life with a significant test–retest reliability (P < .0001). 28
The group differences among the survival times of the 3 MSSE scale scores were evaluated by Kaplan-Meier analysis (log rank, P < .0018, Breslow, P < .0027) and were significant. The results of the Cox proportional hazard model of survival showed a high correlation between high MSSE scale score, high risk of mortality, and short survival of patients with end-stage dementia during the last 6 months of life with significant predicting validity (P < .013). 29
Aminoff Suffering Syndrome in Advanced Dementia and End of Life
The Aminoff suffering syndrome defined by us 30 -32 is characterized by a high MSSE scale score, less than 6 months’ survival for terminal patients, less than 1-month survival for dying patients, irreversible and intractable aggravation of medical conditions, and suffering until demise.
Statistical Analysis
Univariate analysis was used to determine the relationships between each explanatory variable and the mortality group. The Pearson’s chi-square or Fisher’s exact tests were used to compare the groups with respect to categorical variables. Two sample t test were used to compare the groups with respect to variables that follow a normal distribution. Two sample Wilcoxon test was used to compare the groups with respect to variables that do not follow a normal distribution. Multivariate logistic regression was applied to identify the significant independent predictors of mortality by considering candidate variables with P values of <.05 in the univariate analysis.
The backward elimination model selection method was used to identify important factors from the full logistic model. The criterion of an effect to stay in the model is the 2-sided 5% significance level of the Wald’s chi-square. Statistical analysis was performed by SAS for windows version 9.2 (SAS Institute Inc., Cary, North Carolina).
Results
A follow-up of 183 patients diagnosed with advanced dementia (110 females and 73 males) who were admitted to a Geriatric-Internal Medicine ward is depicted in Table 1.
General Characteristics of a Population With Advanced Dementia Upon Admission to a Geriatric Internal Medicine Ward.
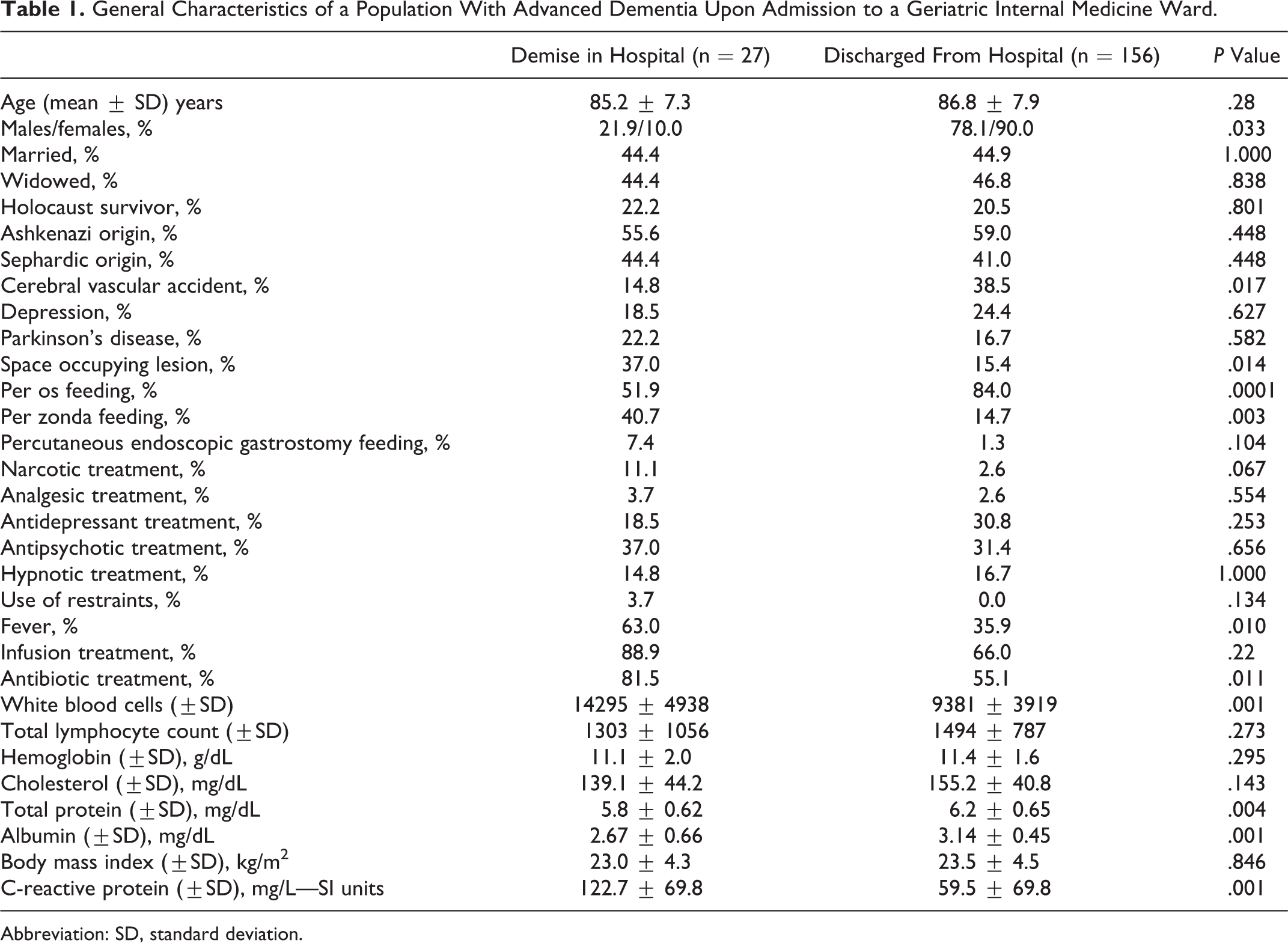
Abbreviation: SD, standard deviation.
During hospitalization, 14.8% (27 of 183; group 1) of patients with advanced dementia died (mean survival time 19.86 ± 26.9 days); 51.8% (14 of 27) of patients from group 1 died within 14 days of hospitalization, and 88.8% (24 of 27) of patients of group 1 died within 30 days of hospitalization. Of 183 patients, 156 (85.2%) were discharged after a mean hospitalization of 10.78 ± 12.3 days.
The MSSE scale score of patients with advanced dementia who died during hospitalization (group 1) was 7.56 ± 1.71, and the MSSE scale score of patients discharged from hospital (group 2) was 3.99 ± 2.10, with a significant difference (P < .001; Table 2).
Comparison Between Items (%) in the MSSE Scale Score of Patients With Advanced Dementia Who Died During Hospitalization and Those Who Were Discharged.
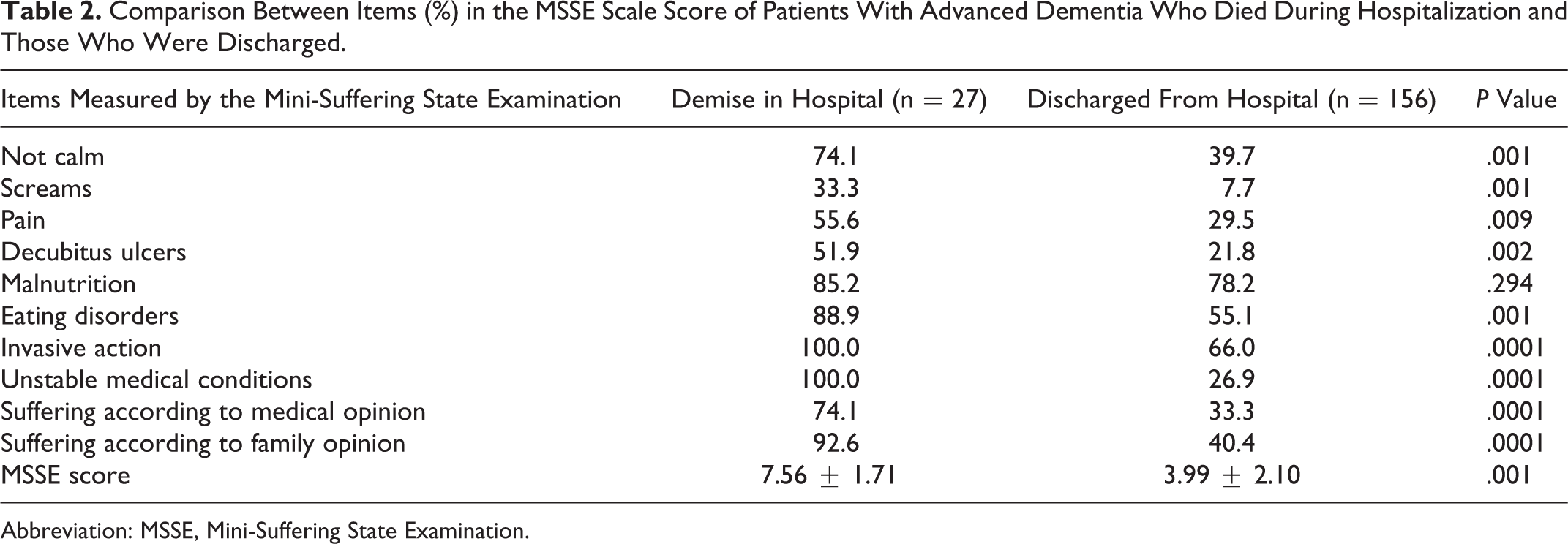
Abbreviation: MSSE, Mini-Suffering State Examination.
When a multivariate logistic regression model was applied to the data (Table 3), a high MSSE score (indicating a high level of suffering; P < .0001) and leukocytosis (P = .01) emerged as major significant risk factors for demise. Female gender versus male (P = .026) appeared to be “protective” against shorter survival.
Multivariate Logistic Regression Model Predicting Mortality of Patients with Advanced Dementia.
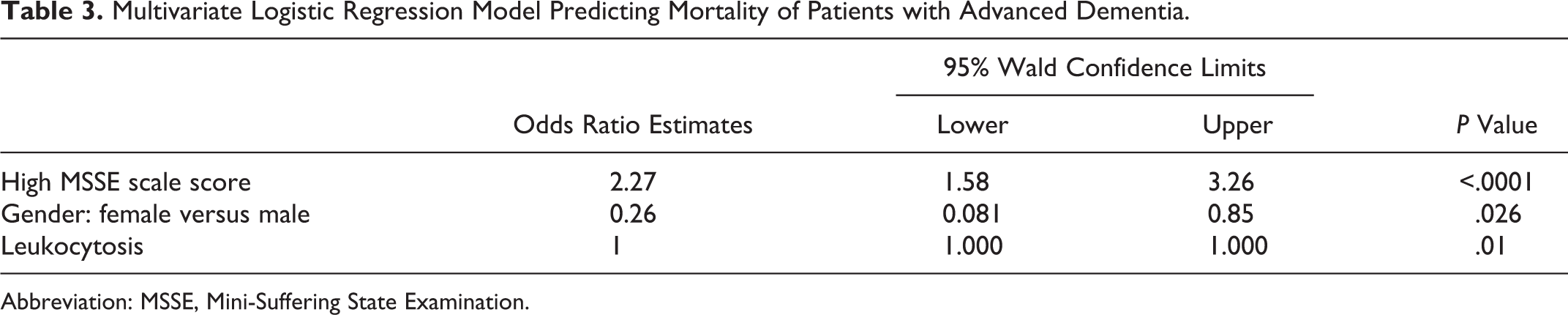
Abbreviation: MSSE, Mini-Suffering State Examination.
Most of the signs of suffering in patients who died were in the high range as measured by items of the MSSE, compared to patients who survived and were subsequently discharged from hospital.
In the group 1 patients, 88.2% had eating disorders, 85.2% had malnutrition, 51.9% showed existence of decubitus ulcers, 40.7% had nasogastric tube, and 37% reported SOL in medical history.
We could note that, unfortunately, “acute problems” of most patients with advanced dementia were treated until the end including futile invasive procedures. Screams was controlled by calming drugs. The high number of advanced dementia with PEG and nasogastric tube is typical for medical settings in Israel.
Most had signs of inflammation, 63% had fever, leukocytosis, very high CRP level, and 81.5% received antibiotic treatment compared to group 2 indicating a significant difference. All were in an unstable medical condition and underwent invasive procedures on the first day of admission to the Geriatric-Internal Medicine Department.
Discussion
This first description of advanced dementia by Dr Alois Alzheimer is a reminder of the reality of the torment and anguish of these patients. 33 The medical, functional, cognitive, and emotional conditions of Mrs Auguste D{eter} during her last months and days are characteristics of Aminoff suffering syndrome. 34 In fact, in our previous studies most patients with end-stage dementia had a high suffering level upon their demise. 35
The suffering assessment 36 -40 and quality of dying evaluation 41 -43 are important in advanced dementia. Some available instruments developed for suffering assessment are Initial assessment of suffering, 44 Pictorial Representation of Illness and Self Measure, 45 Suffering Assessment Tool, 46 State of Suffering-V, 47 The Suffering scales, 48 and Structured Interview for Symptoms and Concerns scale. 49 The MSSE scale remains the first objective valid tool for suffering assessment in advanced dementia.
In our study, those patients with advanced dementia who died during hospitalization had a high suffering level measured by the MSSE scale and short-survival time. All those patients had Aminoff suffering syndrome. Diagnosis of Aminoff suffering syndrome could prove beneficial in the prognosis of short survival in advanced dementia. Patients with advanced dementia having Aminoff suffering syndrome should receive intensive treatment to relieve suffering in palliative settings or alternative Relief of Suffering Units. 50,51 It should be borne in mind that high suffering level is not a marker of disease severity in advanced dementia. High suffering level of a patient is an indicator of inadequate nursing and medical treatment.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.