
Abstract
The purpose of this exploratory study was to determine whether the balance of positive to negative affect can discriminate states of well-being in nursing home residents with dementia and whether affect balance is associated with activity engagement. Baseline data from a randomized clinical trial were used in this secondary analysis. Participants were 128 residents recruited from 9 nursing homes located in Pennsylvania. Participants were primarily female, Caucasian, and had a mean age of 86 years. Measures of agitation and affect were taken from video recordings of 10 observational sessions. Measures of engagement and self-reported mood were taken in real time. Ten percent of participants were categorized as having high well-being. These participants had a mean ratio of positive–negative affect of 2.21 (±0.50), a ratio significantly different than that of participants with moderate or low well-being. Affect balance was related to greater engagement in activity (r = .23; P = .008).
Introduction
Emotional well-being is an important component of quality of life (QOL) in the nursing home. 1 Many nursing home residents with dementia experience low well-being. These residents exhibit negative affect because their needs for care are not addressed and they have few opportunities for expressing positive affect. 2
Affect balance is a concept first advanced by Bradburn 3 who hypothesized that well-being is a global judgment people make by comparing the relative frequency of experiencing negative affect versus positive affect. According to this theory, the absence of negative affect is not the same as the presence of positive affect. This concept has enjoyed substantial support over the years from the frequent finding that positive and negative affect correlate with different variables. 4 For example, positive and negative affect differentially associate with approach and avoidance inclinations toward alcohol and drug cues. 5
Recently, Fredrickson 6 has advanced a theory about the mechanism behind why balance between positive and negative affect may enhance well-being. Her Broaden-and-Build theory holds that a high ratio of positive to negative affect widens the behavioral repertoire and predicts resilience to adverse events. 7 Positive affect is also important for function as it reflects a tendency to engage rather than disengage with the environment. 8
In later work, Fredrickson and Losada 9 suggested that a positivity ratio of 2.9 distinguishes young adults who are flourishing from those who are languishing. Although the mathematical approach for establishing this critical minimum ratio has been questioned, 10 Fredrickson 11 has argued that there is evidence supporting the association of higher positivity ratios to well-being that has not relied on the flawed mathematical models. Baumeister and his colleagues have also argued that to achieve well-being a ratio of approximately three positive emotions to one negative emotion is needed to offset the tendency for negative events to exert a stronger impact than positive events (negativity bias). 12 Diehl and colleagues 13 also demonstrated that a 2.9 affect ratio differentiated young adults on measures of well-being.
Only a few studies have examined the positivity ratio in older adults and results are conflicting. In the study by Diehl and colleagues, 13 the investigators reported positivity ratios of 3.2 (±4.0), 17.3 (±34.6), and 26.7 (± 34.3) for the subsample of community-dwelling older adults who were assessed as having low, moderate, and high well-being, respectively. In a larger study, 14 we found that positivity ratios of 2.40 (±1.72) and 3.99 (±1.58) characterized community-dwelling older adults with low/moderate and high well-being, respectively. In that same study, we examined a separate sample of 53 cognitively intact nursing home residents. These volunteers were recruited from 5 nursing homes in the Louisville, Kentucky area, and were primarily male and caucasian, with a mean age of 74 (±13.24) years. We asked participants to self-report their affect and well-being using standard instruments. We hypothesized that a higher positive-to-negative affect than 2.9 would be needed to distinguish those with high well-being from those with low/moderate well-being, given the greater degree of comorbidity and disability in this group compared to community-dwelling older adults. Contrary to our expectations, we found that positivity ratios of 1.63 (±0.96) and 3.53 (±1.27) characterized those with low/moderate and high well-being, respectively, ratios similar to our community sample, but quite different from the Diehl sample. Despite the differences in mathematical ratios across these studies, which may reflect both sampling and measurement differences, we note that in all of these studies, the positive to negative affect balance was related to well-being.
Nursing home residents with dementia retain the capacity to express a range of emotions despite their cognitive impairments. 15 We do not know the degree to which affect balance is associated with greater well-being and better function in nursing home residents with dementia. The movement to person-centered care is making QOL a primary goal of care. 16 An examination of affect balance and its association with well-being and functioning, indicated by engagement in activity, is timely and would afford the opportunity of examining the relevance of the Broaden-and-Build theory for understanding and promoting well-being in nursing home residents with dementia.
In this exploratory study, we use a novel theoretical approach to examine the association of affect balance to well-being in residents with dementia. In line with the existing literature and our previous study of affect balance,
14
we pose these research questions: What is the positive to negative affect ratio in nursing home residents with dementia? Does this affect ratio discriminate levels of well-being in nursing home residents with dementia? Is the positive to negative affect ratio related to engagement in activity?
Methods
The data for this secondary analysis were taken from the baseline period of a previously published randomized clinical trial that tested the efficacy of an individualized activity intervention for reducing behavioral symptoms in nursing home residents with dementia. 17 The trial received approval from the university institutional review board.
Sample
A total of 128 participants were recruited from 9 community-based nursing homes in Pennsylvania. Participants were female (77%), caucasian (88%), 65 years of age or older with a mean age of 86.11 (± 6.0) years, and 12.26 (±3.1) years of education. They had moderate to severe cognitive and physical impairments as indicated by mean scores of 14.25 (±4.5) on the Mini-Mental State Examination 18 and 12.98 (±7.4) on the physical capacity subscale of the Psychogeriatric Dependency Rating Scale. 19 None had any new psychoactive drugs prescribed from prebaseline through final observation.
Procedure
Following written consent, participants entered a 5-day baseline period where measures of agitation and affect were taken twice each day (morning and afternoon) from video-recorded sessions that lasted 20 minutes. Measures of self-reported mood and observations of engagement were taken in real time during each session. Trained research assistants rated the videotapes and collected the data in real time using the instruments described subsequently.
Measures
We selected measures from our clinical trial data that are conceptually congruent with affective and well-being measures used in prior studies of affect balance in older adults. Additionally, our measures were taken prospectively over multiple days and times.
Affective ratio
We used an observer-based measure, the Apparent Affective Rating Scale (AARS) 20 to construct a measure of positive to negative affect balance. This observational scale has descriptive indicators for 6 affective states: pleasure, anger, anxiety/fear, sadness, alertness, and attention. The rater is instructed to estimate the portion of a 20-minute behavior stream during which any of these affects are evidenced. Scores are obtained for each affect on a Likert-type scale and can range from 1 (never) to 5 (>10 minutes). We used the intraclass correlation coefficient (ICC) to assess interrater reliability. We obtained interrater reliabilities (ICC) of 0.60 for pleasure and 0.58 for anxiety/fear. We did not obtain adequate reliability for anger or sadness possibly due to the low rate of occurrence for these 2 affects. Most of the variance in negative affect was in the anxiety/fear measure. Alertness and attention are primarily neutral facial expressions that give no indication of emotional state. Thus, the affect balance was calculated using the anxiety/fear and pleasure subscales.
Well-being
Our study included individuals with moderate to severe cognitive impairments, making complex self-report of well-being difficult. We reasoned that daily self-reports of mood states combined with behavioral observations of distress may be salient indicators of well-being in this group because neurodegeneration and memory deficits result in behavior that is more stimulus bound. 21 Thus, persons with dementia tend to live in the “here and now,” and this change in temporality would make their self-report of mood and observations of their behavior important indicators of well-being. Based on this rationale, we measured well-being using the Dementia Mood Picture Test (DMPT) 22 and the Cohen-Mansfield Agitation Inventory (CMAI). 23
Dementia Mood Picture Test—this instrument measures self-reported positive and negative moods (bad, good, angry, sad, happy, and worried) from the perspective of the cognitively impaired participant. Each mood can receive a potential score of 0 to 2 with higher scores representing greater intensity in that mood. We used ICC to assess interrater reliability. We obtained an interrater reliability of .99 when using this instrument.
Cohen-Mansfield Agitation Inventory—is a caregiver-rated questionnaire that consists of 29 agitated behaviors modified for direct observation. Scores range from 0 to 29 with higher scores indicating greater agitation. Measures were taken from video recordings every 5 minutes over the 20-minute observation session. We used ICC to assess interrater reliability. We obtained an interrater reliability of 0.64 for measures taken from video recordings.
Engagement in activity
Engagement was measured by direct observation using a modified version of a molar coding scheme. 24 The instrument has descriptors for behaviors that depict time use: 1 = asleep; 2 = doing nothing; 3 = informal activity (resident initiated); and 4 = organized activity (staff initiated). The one behavior that predominated over the observation period (>50% of the time) was selected as the score. Percentage agreements ranging from 0.92 to 0.97 and weighted κs ranging from 0.94 to 0.97 were obtained for this measure.
Analysis and Results
1. What is the positive to negative affect ratio in nursing home residents with dementia?
The affect ratio was calculated based on the AARS data. The numerator incorporated the pleasure data, and the denominator incorporated the anxiety/fear data. Pleasure and anxiety/fear scores were averaged within patients over the 200 minutes of observation for each patient. Standardized positive and negative scores were calculated by dividing the mean pleasure and anxiety/fear scores by their maximum possible score (5). We divided the standardized positive score by the standardized negative score. In this sample (N = 128), the mean ratio of positive to negative affect was 1.31 (±0.7); range = 0.2 to 3.5. 2. Does this affect ratio discriminate levels of well-being in nursing home residents with dementia?
Using an approach from prior work, 14 we constructed an index of well-being using DMPT and CMAI data. Classification of well-being was based on the 2 scores, averaged for each participant. We grouped scores into the upper, middle, and lower third for each scale. Participants were considered to have high well-being if their DMPT score was in the top third of the respective sample distribution and their CMAI score was in the lowest third of its sample distribution. Participants were considered to have low well-being if the reverse was true, for example, their DMPT score was in the lowest third of the respective sample distribution and their CMAI score in the highest third of its sample distribution. All others were assigned to the moderate well-being group. Affect ratio scores were compared among the 3 well-being groups using mixed-model analysis of variance, accounting for the effect of clustering of observations within facilities. Facility was included as a random effect in the model, and well-being category was included as a fixed effect. Residual analysis showed the sample distributions to be essentially normal after accounting for differences among facilities. Follow-up pairwise comparisons among the 3 well-being groups utilized Tukey’s adjustment for multiple comparisons.
Approximately 10% (N = 13) of the sample was classified as having high well-being and their mean affect ratio was 2.21 (±0.50); 83% (N = 106) was classified as having moderate well-being and the mean affect ratio for this group was 1.25 (±0.63); and 7% (N = 9) was classified as having low well-being with a mean affect ratio of 0.85 (±0.37). The means and standard deviations for the DMPT and CMAI scores that comprised the well-being groups are in Table 1.
Mean (SD) for DMPTa and CMAIb by Well-Being Groups.
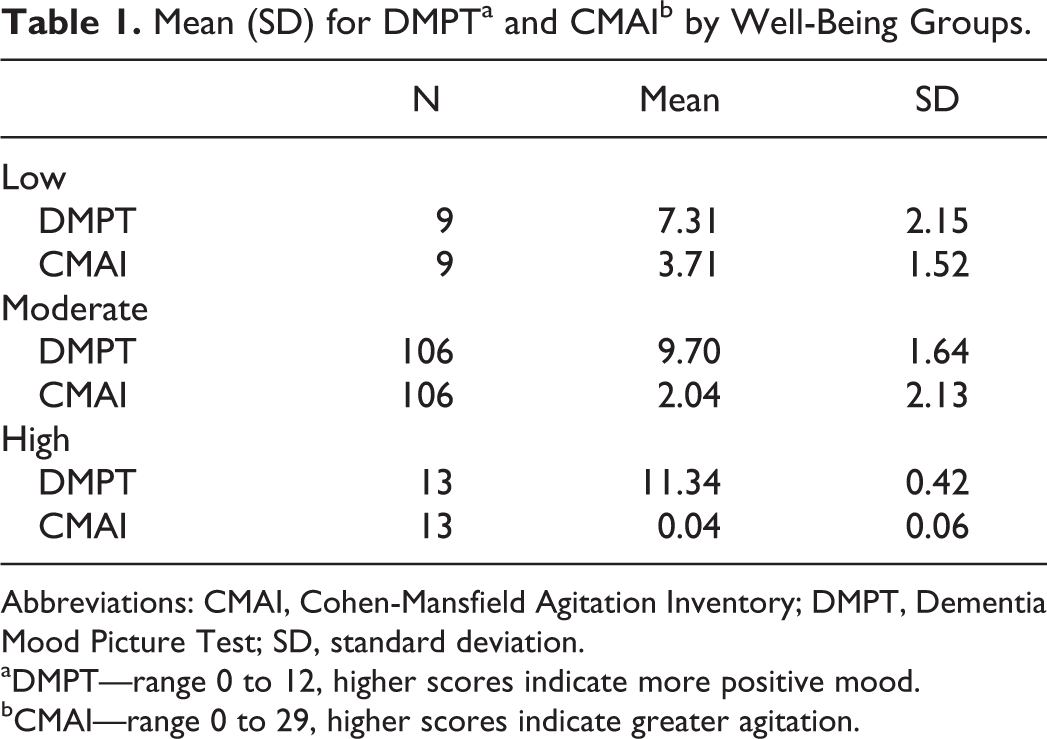
Abbreviations: CMAI, Cohen-Mansfield Agitation Inventory; DMPT, Dementia Mood Picture Test; SD, standard deviation.
aDMPT—range 0 to 12, higher scores indicate more positive mood.
bCMAI—range 0 to 29, higher scores indicate greater agitation.
The mean affect ratios differed significantly among these well-being groups (F 2,125 = 17.46, P < .001). Tukey’s test indicated that the affect ratio for the high well-being group was significantly different than the moderate or low well-being groups at the P = .05 level. There was no statistically significant difference in the affect ratios for the moderate and low well-being groups (Figure 1). We found no differences in age (F 2,125 = 1.48, P = .23), gender (χ2 [2, N = 128] = 0.43, P = .80), race (χ2 [2, N = 128) = 1.39, P = .49), years of education (F 2,125 = 1.35, P = .26), mental status (F 2,122 = 1.00, P = .37) or physical function (F 2,125 = 1.77, P = .17) among the well-being groups.
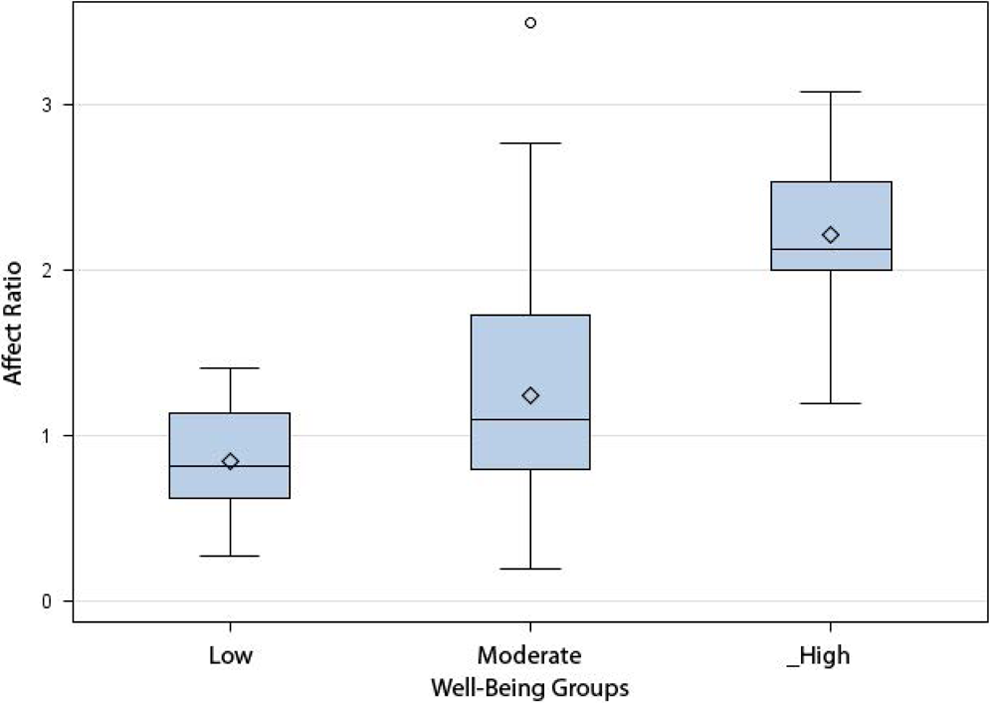
Distribution of affect ratio scores by well-being group. Using the Apparent Affective Rating Scale data, the affect ratio was calculated by dividing the standardized positive score by the standardized negative score. The index of well-being was constructed based on grouping the distribution of scores from both the Dementia Mood Picture Test and Cohen-Mansfield Agitation Inventory into the upper, middle, and lower third for each scale.
3. Is the positive to negative affect ratio related to engagement in activity?
Using the observational data, 24 we collapsed the informal and formal activity categories into one category of active engagement and recoded categories: 0 = dozing; 1 = doing nothing; and 2 = active engagement. Engagement scores were averaged for each participant. Linear association between the affect ratio and the mean engagement scores was evaluated using Pearson’s correlation coefficient. We found a small but positive and statistically significant correlation between the affect ratio and engagement (r = .23; P = .008).
Discussion
To our knowledge, this is the first study to use the framework proposed by Fredrickson 6 to conceptualize well-being in nursing home residents with dementia, a perspective that considers the balance between positive and negative affect and not just one affective state in an isolated fashion. Previous research in community-dwelling adults has suggested an average affect balance of approximately 2:1 25 and in a national representative sample of older adults, 20% experienced high well-being. 26 In our sample, affects were more evenly balanced, with a mean ratio of 1.31 (±0.7). This finding was not unexpected, given the high burden of negative affect and physical comorbidities that are common in nursing home residents with dementia. Unlike most studies of older adults, only 10% experienced high well-being. In prior studies, well-being was measured by in-depth self-report using a variety of psychological scales, an approach we could not use in this study. Nevertheless, the residents we classified as having high well-being consistently self-reported very high mood and displayed very few agitated behaviors. We found no association between well-being and important demographic and clinical variables, including mental status. The results support the notion that even under challenging situations, well-being is possible and should be a goal of care across all stages of dementia.
We found that an affect balance of 2.21 (±0.50) characterized residents with high well-being. This ratio is less than what has been reported for cognitively intact nursing home residents, 14 and much less than that reported in community-dwelling older adults. 13 To explain their very high affect ratios for older adults, Diehl and colleagues argued that young adults more commonly encounter daily stressors in work and educational settings than older adults. Research shows that older adults are able to exert control over stressors by avoiding people and situations they find unpleasant. 27 The nursing home environment is at least as stressful as the work environment, particularly for residents who have little control over the people and situations they encounter. Data also demonstrate a curvilinear relationship between the positivity ratio and the optimal functioning under stressful situations, with little advantage to ratios above 3. 28 Being very positive and/or having little negative affect in adverse circumstances might have the effect of eliminating an appropriate response to negative situations.
Importantly, we found a significantly higher affect balance in the high well-being group compared to the other 2 groups. This finding supports the Broaden-and-Build theory and underscores the utility of considering affect balance, rather than just one affect in isolation, when assessing well-being in individuals whose life circumstances, such as having a neurodegenerative disease, result in a high burden of negative affect. This is particularly important clinically, since negative affect resulting from dementia and related disorders may be difficult to modify, 29 whereas positive affect may make a more malleable target.
We found a significant association between engagement and higher affect balance. Garland and colleagues 7 argue that by increasing positive affect relative to the level of negative affect lasting functional outcomes can be attained for individuals who experience emotional dysfunctions. In support of this perspective, more positive self-reported mood in nursing home residents was found to be associated with greater engagement and a higher level of attention during structured activities. 30
We recognize several limitations in our approach. This was a secondary analysis and the measures we used to calculate the affect balance and well-being were not the same as those used in earlier studies, making comparisons across studies less precise. The reliability of our AARS data was not high. Our measures are, however, conceptually congruent with those previously used in the literature, we selected the most reliable subscales in the AARS and used repeated measures to compute the affect balance measure and the index of well-being. Despite limitations our findings support a theoretical perspective on well-being that could inform outcome measures for practice and research.
In summary, we found that 10% of our sample experienced high well-being and that these residents had a higher positive affect balance than residents with moderate or low well-being, supporting the Broaden-and-Build theory. Greater engagement in activity was associated with a higher positive affect balance. A realistic goal for improving well-being among nursing home residents with dementia may be to improve affect balance via engagement and other approaches focused on increasing positive affect relative to negative affect.
Footnotes
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Nursing Research or the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the National Institutes of Health/National Institute of Nursing Research (Grant # R01 NR008910) awarded to Ann Kolanowski.