
Abstract
In the year 1907, Dr Alois Alzheimer published a case report on Mrs Auguste Deter. 1
On July 12, 1905, in the Psychiatric Unit at the University Clinic in Frankfurt, Dr Alzheimer recorded that Mrs Auguste Deter appeared completely dazed, was totally silent, and lay on her bed, with her knees drawn up, in a constant pool of urine and feces. She was also visibly losing weight. The last 15 lines of this communication described her final days. At the beginning of 1906, she developed decubitus ulcers, and her physical deterioration was progressive. Throughout the month of March 1906, she had a fever of up to 40°C. She was diagnosed with pneumonia and continued to be very agitated and cried out noisily. Finally, at quarter past 6 on April 8, 1906, she passed away. The initial autopsy showed cause of death to be septicemia due to the bed sores and blood poisoning.
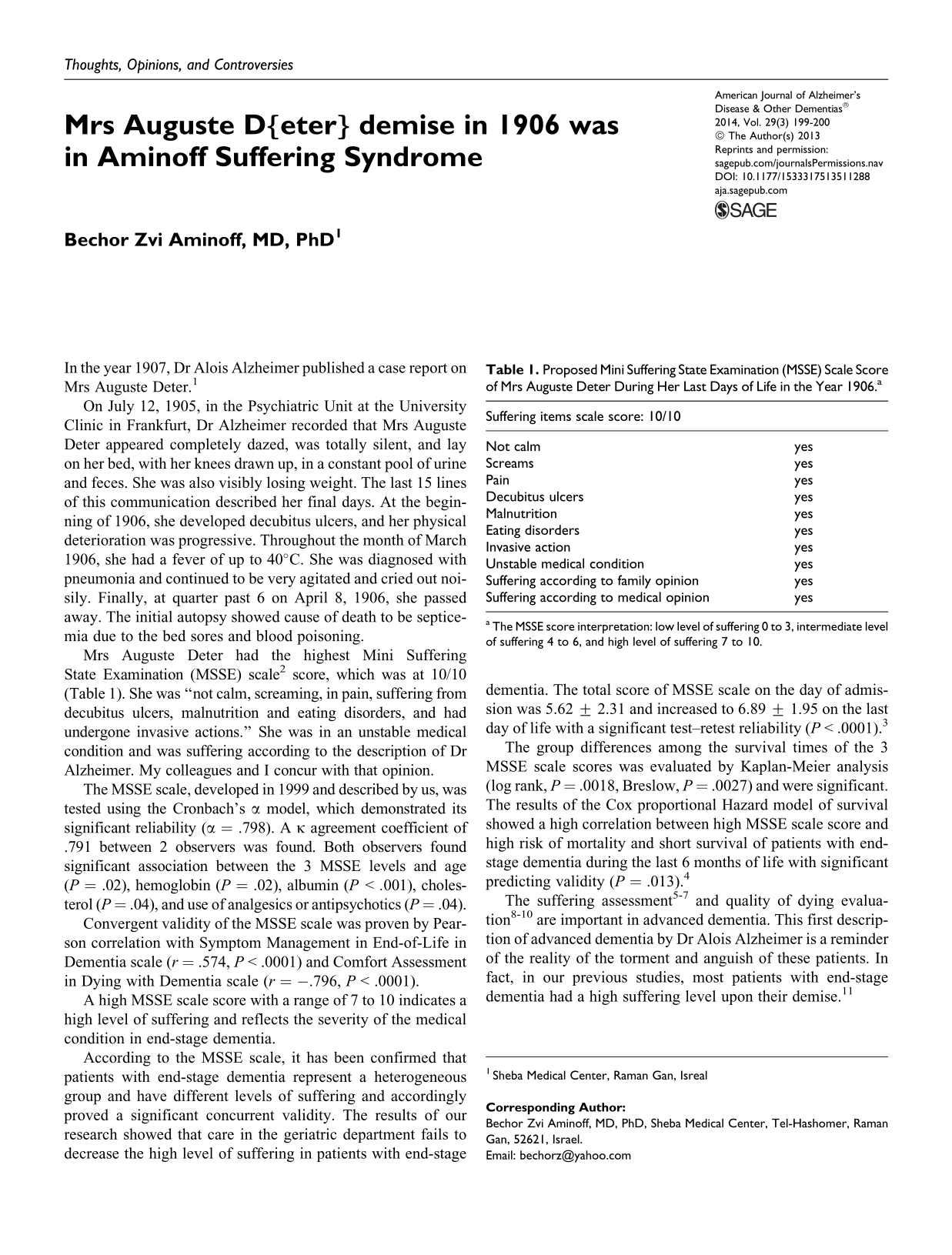
Mrs Auguste Deter had the highest Mini Suffering State Examination (MSSE) scale 2 score, which was at 10/10 (Table 1). She was “not calm, screaming, in pain, suffering from decubitus ulcers, malnutrition and eating disorders, and had undergone invasive actions.” She was in an unstable medical condition and was suffering according to the description of Dr Alzheimer. My colleagues and I concur with that opinion.
Proposed Mini Suffering State Examination (MSSE) Scale Score of Mrs Auguste Deter During Her Last Days of Life in the Year 1906.a
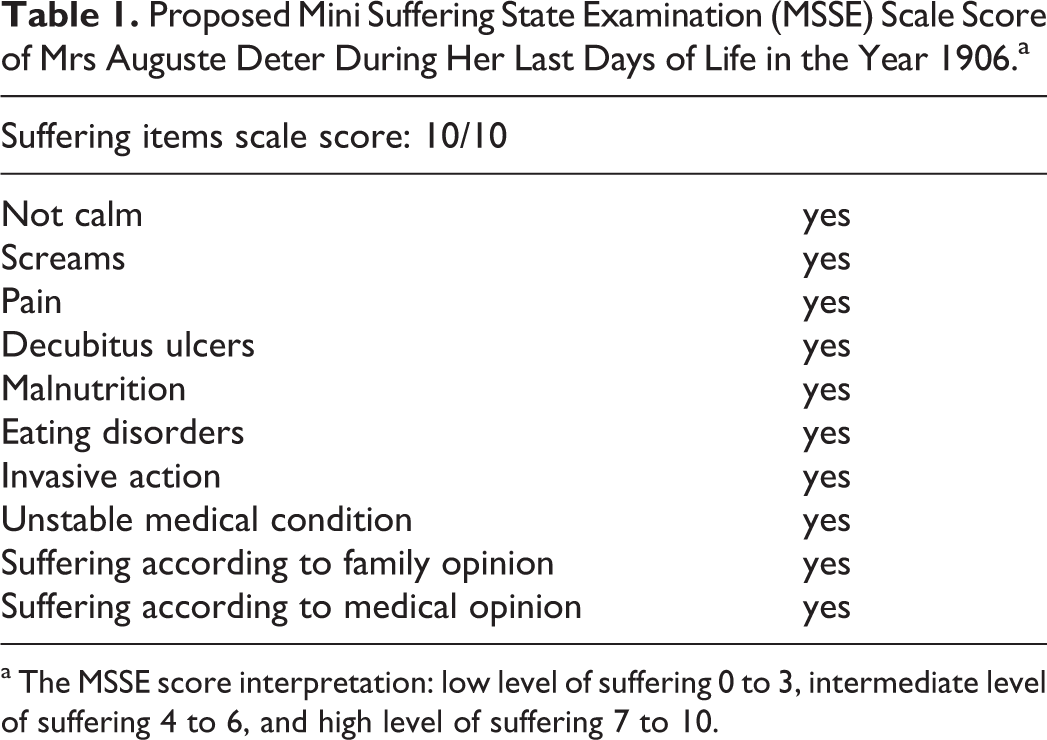
a The MSSE score interpretation: low level of suffering 0 to 3, intermediate level of suffering 4 to 6, and high level of suffering 7 to 10.
The MSSE scale, developed in 1999 and described by us, was tested using the Cronbach’s α model, which demonstrated its significant reliability (α = .798). A κ agreement coefficient of .791 between 2 observers was found. Both observers found significant association between the 3 MSSE levels and age (P = .02), hemoglobin (P = .02), albumin (P < .001), cholesterol (P = .04), and use of analgesics or antipsychotics (P = .04).
Convergent validity of the MSSE scale was proven by Pearson correlation with Symptom Management in End-of-Life in Dementia scale (r = .574, P < .0001) and Comfort Assessment in Dying with Dementia scale (r = −.796, P < .0001).
A high MSSE scale score with a range of 7 to 10 indicates a high level of suffering and reflects the severity of the medical condition in end-stage dementia.
According to the MSSE scale, it has been confirmed that patients with end-stage dementia represent a heterogeneous group and have different levels of suffering and accordingly proved a significant concurrent validity. The results of our research showed that care in the geriatric department fails to decrease the high level of suffering in patients with end-stage dementia. The total score of MSSE scale on the day of admission was 5.62 ± 2.31 and increased to 6.89 ± 1.95 on the last day of life with a significant test–retest reliability (P < .0001). 3
The group differences among the survival times of the 3 MSSE scale scores was evaluated by Kaplan-Meier analysis (log rank, P = .0018, Breslow, P = .0027) and were significant. The results of the Cox proportional Hazard model of survival showed a high correlation between high MSSE scale score and high risk of mortality and short survival of patients with end-stage dementia during the last 6 months of life with significant predicting validity (P = .013). 4
The suffering assessment 5 –7 and quality of dying evaluation 8 –10 are important in advanced dementia. This first description of advanced dementia by Dr Alois Alzheimer is a reminder of the reality of the torment and anguish of these patients. In fact, in our previous studies, most patients with end-stage dementia had a high suffering level upon their demise. 11
The medical, functional, cognitive, and emotional condition of Mrs Auguste Deter during her last months and days are characteristic of the Aminoff suffering syndrome.
Aminoff suffering syndrome in advanced dementia is a proposed symptomatologic and pathological entity 12 –14 with irreversible and intractable aggravation of suffering and medical condition until death and could be prognostic indicator of 6-month mortality 15,16 in elderly people with advanced dementia and a key criterion for enrolling patients to palliative settings or alternatively to relief of suffering units.