
Abstract
The delusional misidentification syndromes (DMSs) are psychopathologic phenomena in which a patient consistently misidentifies persons, places, objects, or events. Although often described in relation to psychotic states including schzofrenia, it is, nevertheless, widely considered that these syndromes have an anatomical basis because of their frequent association with organic brain disease; studies have pointed to the presence of identifiable lesions, especially in the right frontal lobe and adjacent regions, in a considerable proportion of patients. The purpose of this article is to examine the phenomenon in people with dementia. We searched the electronic databases for original research and review articles on DMS in patients with dementia using the search terms “Delusional Misidentification Syndrome, Capgras syndrome, Fregoli syndrome, reduplicative paramnesia, and dementia.” The DMSs are a frequent problem in dementia. The violence and dangerousness in patients with dementia having these syndromes are well documented, and forensic aspects are highlighted. Pathogenetic viewpoint and management are considered.
Keywords
Introduction
The delusional misidentification syndromes (DMSs) are psychopathologic phenomena in which a patient consistently misidentifies persons, places, objects, or events; according to the French clinicians of the early 20th century, their central feature is patient’s belief in the existence of double. The concept of the double appears very frequently in the traditions, myths, literature, religious beliefs, and metaphysical notions of all cultural and ethnic groups, which explains the universality of these syndromes. 1 Stevenson described the experience of double in his novel The Strange Case of Dr. Jekyll and Mr. Hyde. 2 Because misidentification appears to occur more often in association with certain symptoms, such as depersonalization, derealization, and paranoia, it may qualify as a syndrome. Originally, Christodoulou 3 described DMS as consisting of a set of 4 psychiatric disorders, Capgras syndrome (CS), Fregoli syndrome, intermetamorphosis, and subjective doubles. Some researchers included misidentification of mirror image and misidentification of television as symptoms of DMS. 4 Burns et al 5 classified phantom boarder syndrome (PBS) in patients with Alzheimer’s disease (AD) as a misidentification, because it does not fulfill the definition of delusion and because of its association with other misidentifications. Hwang and colleagues 6 sustained that PBS is a common symptom in dementia of various etiologies, and they suggested that it may be more productive to classify PBS as a type of misidentification, instead of as a delusion, but other authors do not agree with this concept. 7 Others included reduplicative paramnesia into DMS. 8 Physical and/or psychological delusional misidentification in relation to the self has also been described. 9–11 More recently, Mulholland and O’Hara have reported a new variant of DMS named “delusional hermaphroditism.” 12 Finally, nurturing syndrome is an increasingly recognized delusion, clustering with phenomena of misidentification, in which the patient believes a dead family member to be alive. 13 These patients often request the police to search for their missing relatives and feed and sleep with pictures of the dead family members. 14 In many cases, 2 or more misidentification syndromes and related phenomena are present in the same patient, 15–17 which may indicate similar underlying pathophysiological mechanisms. In various case reports, several authors have also made contradictory comments on questions concerning classification, etiology, and assignment to a possible entity of DMS. 18 Early explanations of the delusion were predominately psychodynamic interpretations, but results of structural and neuroimaging studies of the variegated misidentification syndromes provide support for an organic etiology. 19
Brief Phenomenological Approach to DSM
The most commonly described and best known form of the variegated misidentification syndrome is known as CS or syndrome of doubles. In 1923, Capgras and Reboul-Lachaux published the first report of a syndrome they coined “illusion de sosies.” 20 The authors reported a 53-year-old paranoid megalomanic woman “who transformed everyone in her entourage, even those closest to her, such as her husband and daughter, into various and numerous doubles.” The disorder consists of the belief that a person or persons have been replaced by “doubles” or imposters without significant changes in the physical appearance of the misidentified objects. It is the selective duplication of people with whom the patient has strong emotional bonds and associative memories. These patients can consciously recognize familiar faces but cannot emotionally connect with them. The CS is not restricted to person misidentification but can also involve animals 21 or inanimate objects. 22 The most frequent doubles are the spouse (if the patients are married, divorced, or separated) and siblings (if the patients are single). 23 The double is usually assumed to have evil intent. A study conducted in an acute psychiatric service found that the CS rate was 2.5%, 24 and in another study that evaluated the previous 5 years of patients’ records in a university hospital, the rate was 1.3%. 25 This syndrome can affect both genders at all ages; however, some authors found higher prevalence in females than in males, with a 2:1 ratio. 26 Few reports have described this syndrome during childhood. 26,27 It was initially reported to be associated only with psychiatric diseases, including paranoid schizophrenia and schizoaffective disorder, 28,29 but more recently, with improved diagnostic technique, CS has also been described in neurological conditions and various organic disorders, including cerebrovascular disease, 30 subarachnoid hemorrhage, 31 head injury, 32 epilepsy, 33 pituitary tumor, 34 pseudohypoparathyroidism, 35 and myxoedema. 36 The CS may be transient or persistent and often includes more than 1 subject of misidentification. 37,38 It was also reported in a patient with blindness. 39 According to the author, the case suggests that intact vision is not necessary for CS, and that other senses and their misinterpretation, including hearing and touch, contribute to this phenomenon.
Fregoli syndrome was described by Courbon and Fail in 1927. 40 The eponym derives from the Italian actor Leopoldo Fregoli who was a great impersonator and mimic. In this disorder, the patients misidentify unfamiliar people and places as familiar ones. For example, they confuse a hospital room with their home and strangers with familiar people. Mojtabei 41 reviewed the literature and reported 34 Fregoli syndrome cases, their average age was 34.9 years and mainly male. In hospital settings, patients with Fregoli syndrome often misidentify members of the treatment team (eg, nurses, doctors, trainees, etc) who work closely with the patients; this misidentification may result in assaultive behavior toward the staff, 42 but the frequency of violence in the syndrome is unclear. 43 Christodoulou suggested that CS is a “hypoidentification” of a person closely related to the patient, whereas Fregoli syndrome is a “hyperidentification” of a person not well known to the patient. 28,44
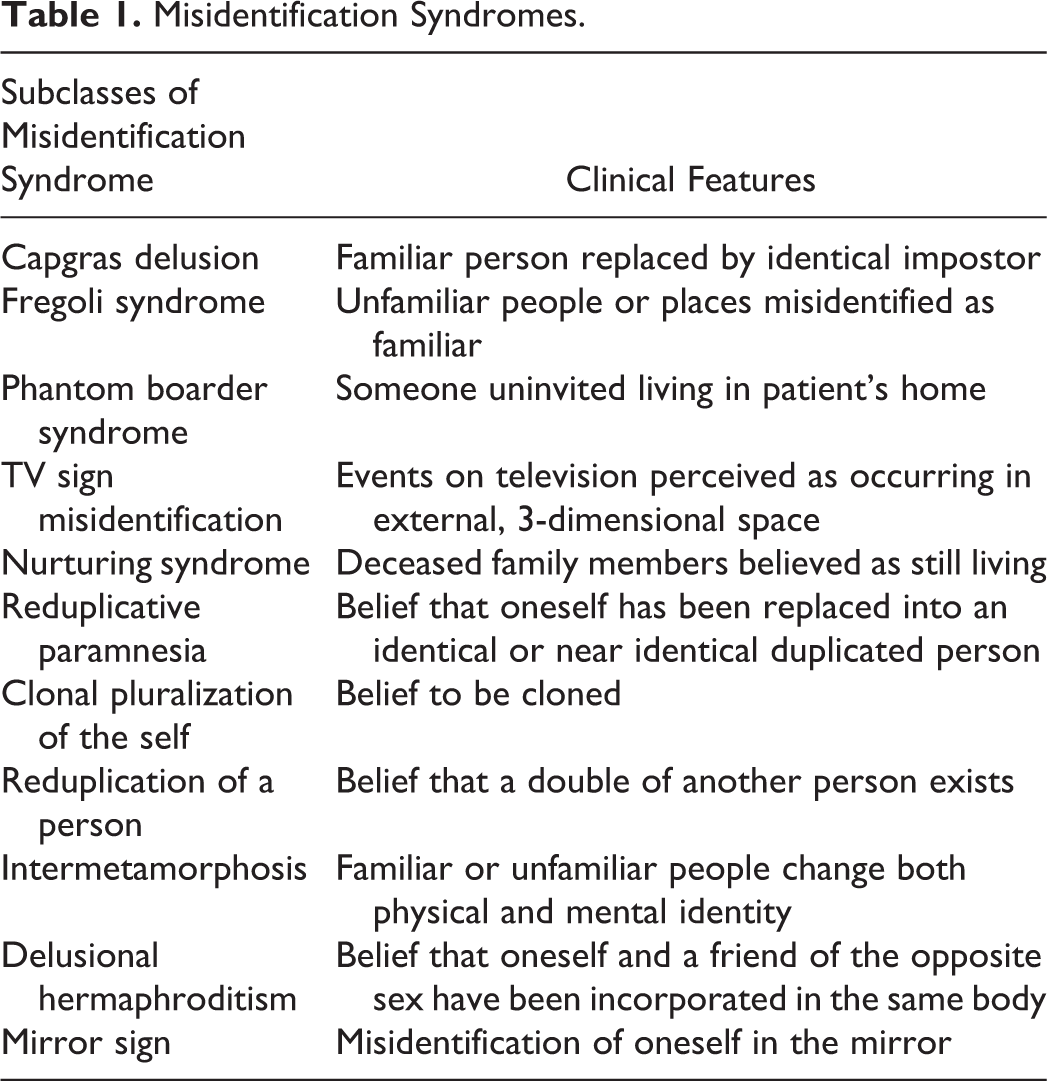
The syndrome of intermetamorphosis is characterized by the patient’s conviction that a person has changed both physically and psychologically. It was first described by Courbon and Tusques in 1932, 45 and it is exceedingly rare. It is possible that the syndrome has been tempered into a transient symptom by the widespread use of neuroleptics and is consequently underreported. 46 The term reduplicative paramnesia, also known as environmental reduplication, was first used in 1903 by neurologist Arnold Pick that described a case of a 67-year-old woman with a diagnosis of senile dementia who developed a conviction that there was a duplication of the same clinic in Prague, an “old” one and a “new” one, both headed by Professor Pick. 47 Reduplicative paramnesia was often used in several meanings in the related literature. Recently, its definition was narrowed down to the misidentification of places occurring in certain organic cerebral disorders; therefore, it has been discussed as a neurological syndrome. 48 In Table 1, we try to list subclasses of misidentification syndrome.
Misidentification Syndromes.
Dangerousness in DMS
The category of DMS is sometimes characterized by hostility toward misidentified objects and, subsequently, it can lead to significant danger of physical harm to others, 49–53 so that it has more than a simply academic interest, given its association with dangerous behavior, but most of the anglophonic psychiatric literature on misidentification syndromes and dangerousness has been reported as single-case studies with an occasional article devoted to a small series of cases. 50 However, reports exist on cases of violent acts in patients with CS including homicide, toward family members. 19 For example, Taj et al described a 70-year-old man with a diagnosis of vascular dementia (VaD). This patient declared that his wife had the same appearance, but was a double, and he showed occasionally violence toward her. The violence became exaggerated in the preceding 2 months leading up to hospitalization and he even set fire to his home in order to kill his wife. 54 It was explored the association of delusional misidentification and aggression in an individual with AD. 55 The authors described the case of Mr D, a 71-year-old man, who was admitted to a psychiatric hospital after threatening to shoot his wife. He was essentially unable to link the correct visual experience of his wife to her correct biography. Believing that her body harbored a different psychological identity than that of his wife, he concluded that she was an impostor. Despite numerous reports of assault associated with CS, the propensity to violence cannot be attributed solely to the delusion’s existence. Other factors are likely to influence the possibility of violent action. Most individuals with CS who have committed interpersonal violence are men with a history of aggressive behavior and (or) substance abuse; social withdrawal or isolation prior to the violent act is common, and the violence is usually well planned. 19 Silva et al provided a review of patients that have children as the misidentified objects and then discussed the relationship between misidentification and potential harm to these children. 56 Violence in less known Fregoli syndrome has been understudied but, due to the nature of the delusion, patients with this syndrome may present a subgroup who are in particular at high risk of violence. The study of violence and patients with dementia has recently received increasing interest, in part because the past solution of institutionalizing aggressive individuals with dementia has become increasingly fiscally problematic. 57 The relationship between aggression and delusional thinking in patients with dementia has been studied focusing on the specific content such as erotomania 58 or delusional jealously 59 in which there are specific targets in association with violent behaviors. Descriptions of patients with dementia who experience aggressive delusional misidentification, although not common, have usually lacked the sufficient phenomenological detail required to ascertain the chain of events culminating in aggression because many patients with cognitive impairment are not able to describe their subjective experiences in reasonable detail. 55 However, the dangerousness of these persons is well documented in those who are affected by AD 55 than those with VaD. 54
Pathogenetic Hypotheses
Cerebral dysfunction is believed to be a central feature in DMS. Discussing about reduplicative paramnesia, Pick 47 maintained that the phenomenon represented a disturbance of memory, specifically involving “a sense of familiarity” that plays “an important part in remembrance, especially in recognition.” Patients with CS and reduplicative paramnesia having unilateral brain lesions strongly implicate the right hemisphere, usually frontal. 60–62 Exclusively, frontal lesions were associated with delusions in 10 (34.5%) of the 29 patients. 60 Frontal dysfunction impairs the ability to monitor self and to recognize and correct inaccurate memories. 63 Observations in patients with bilateral neurodegenerative disorders support that misidentification of familiar places as foreign is associated with temporal and frontal pathology. 63 Underactivity in the perirhinal cortex seems to be responsible for loss of familiarity in Capgras, whereas overactivity seems to account for hyperfamiliarity seen in the Fregoli, intermetamorphosis, and subjective doubles syndromes. 63 The relatively higher frequency of occurrence of right hemisphere lesions in CS, compared with damage to the left side, has led to neuropsychological explanations that have focused on right hemispheric impairments in facial processing. Theoretical models of CS proposed that the patient can recognize a face but fails to receive a confirmatory feeling of familiarity, so that the joint information representing face recognition and affective response does not match a stored (and therefore expected) representation of the person. 64 Also, Hudson and Grace 65 sustained that, in some cases, the misidentification phenomena can be explained by disruption of the connections of highly specialized areas (fusiform gyrus) devoted to the identification of faces with the most anterior inferior and medial part of the right temporal lobe, where long-term memory and mechanisms for the retrieval of information that are required for the visual recognition of faces and scenes are stored; as a consequence, the patient is left with a distorted yet irresistible sense of familiarity, but not identity, about a place or a person. 66 A Single Photon Emission Computed Tomography (SPECT) study of patients with AD having misidentification delusions found bilateral hypoperfusion of superior and inferior temporal lobes in patients with delusions. This area of hypoperfusion corresponds with the location of the fusiform face area and parahippocampal place area, which shows increased activation after viewing faces and physical locations, respectively. 67 Young advocated an interactionist model 68 ; he argued that the delusional belief constitutes an attempt on the part of the patient to explain his or her initially odd and somewhat disturbed phenomenal content and, moreover, that the delusion then structures the patient’s experience such that what he or she perceives is an impostor. Neuropsychological, cognitive, and neuroanatomic findings converge and support the hypothesis that DSM symptoms are produced at least in part by a damaged or disfunctional brain, predominantly in the right hemisphere so that DSM appear as neuropsychiatric encompasses symptoms that lie in the gray zone between neurology and psychiatry. 26 Oyebode 69 described a common link between schizophrenia, schizophrenia-like psychosis of epilepsy, and DMS; it appears to be the involvement of limbic structures in their pathophysiology.
Delusional Misidentification Syndrome and Dementia Subtype
For many years, DMS due to dementia was not well appreciated, but more recently delusional misidentification occurring in the context of dementia has become the object of increasing study, as a high frequency of misidentification spectrum symptoms have been reported. On the basis of a semistructured interview with both patients and their reliable caregivers, Harciarek and Kertesz
70
studied the prevalence of DMS in different kinds of neurodegenerative diseases,; it was identified in 15.8% of patients with AD, 16.6% of patients with dementia with Lewy body (DLB), and in 8.3% of individuals with semantic dementia. None of the patients with behavioral variant of frontotemporal dementia (FTD), primary progressive aphasia, and corticobasal degeneration showed the delusional phenomena. As stated, CD is relatively common in patients with AD.
5,70–76
Interestingly, in many of these cases, it was accompanied by reduplication of place and, occasionally, by phantom boarder phenomenon; isolated experience of reduplication of place or phantom boarder delusions were, however, rarely observed.
70
Delusions of misidentification make up 25% to 47% of delusions in AD,
70,77,78
and they show a rate equal to that of persecutory delusions.
14
Some studies investigated that the mean age of CS in AD was, as previously reported, 73.29 years
70
or 72 years.
72
The mean time of the onset of DMS in AD from the beginning of illness was 3.51 years (range, 0.4-11 years). Interestingly, about 27% among patients with AD developed at least 1 form of misidentification phenomenon within the first year of illness.
70
Tsai and colleagues found that patients with probable AD were more than twice as likely to display aggressive behaviors if delusional misidentification was present.
79
Factor analysis studies, conducted in patients with AD, indicated that DSM is independent of paranoid delusions.
7,80
Mentis et al showed that AD with DMS have significant hypometabolism in paralimbic (orbitofrontal and cingulate areas bilaterally) and left medial temporal areas compared with AD without DMS.
81
Data from positron emission tomography studies of patients with AD and associated DMS indicate that dysfunctional connections among multimodal association areas, paralimbic structures, and dorsolateral frontal cortex are implicated as the predisposing neural deficit underlying DMS, causing cognitive–perceptual–affective dissonance, which under specific conditions results in “positive” delusion formation.
81
Little is known about the prevalence of delusions of misidentification in FTD. Mayeux et al has noted that the presence of extrapyramidal features may significantly contribute to the development of DMS in dementia;
82
different forms of reduplication have also been observed in patients with DLB
83–86
whose clinical features include cognitive fluctuations, recurrent visual hallucinations, and spontaneous features of parkinsonism. A study reported in detail the frequency and variety of psychotic symptoms in DLB
87
; the research describes the high frequency of hallucinations (78%), misidentifications (56%), and delusions (25%). It revealed that a wide variety of misidentification symptoms are commonly exhibited by patients with DLB (misidentification of people, of place, of objects, CS, phantom boarder, reduplication of place, reduplication of people, belief that deceased relatives are still alive, belief that absent relatives are in the house, and misidentification of television). Previous researchers reported the rates for DMS in patients with DLB; it varies from 38% to 78.3%.
83,88
Hirayama et al described a case of DLB presenting with geographic mislocation and nurturing syndrome.
89
According to Thaipisuttikul et al, patients with DLB having CS are more likely to have visual hallucinations, their caregivers tend to report more symptoms of cognitive fluctuations and rapid eye movement sleep behavior disorder, and patients report more symptoms of anxiety.
90
Patients with dementia having Lewy bodies have significant hypoperfusion in the bilateral frontotemporal and parietooccipital cortices compared to the controls, suggesting that the bilateral hemispheres might be dysfunctional in DLB with misidentifications.
91
A comparative clinicopathological study of DMS in AD and DLB showed DMS to be significantly more frequent in DLB (40%) than in AD (10%).
88
The DMSs were described in patients with Parkinson’s disease dementia (PDD)
92
that shares many clinical features with DLB, with more severe dysexecutive and visuospatial defects and a higher incidence of psychosis than AD. In a study performed to investigate the prevalence of DMS in a cohort of 30 consecutive patients with PDD, all patients with DMS (16.7%) exhibited hallucinations that were significantly more severe than in PDD without DMS.
93
Joseph studied CS and its relationship to neurodegenerative disorders. In those patients who presented with features of idiopathic Parkinson’s disease, the onset of CS occurred at a mean of 8 years later, when all of the patients had become demented and met criteria for PDD.
94
It was supposed that dopamine deficiency may lead to CS in PDD. Shiotsuki et al
95
reported a patient with PDD who showed Capgras delusions only during the “off” state. Increased doses of
Management
Neuropsychiatric investigations do not provide us with the “meaning of the delusional misidentification phenomena or answers as to why and how the mind creates doubles.” 1 To date, it is unclear whether there are differences between DMS, as it occurs in neurodegenerative compared with nonneurodegenerative diseases. 94 Fleminger and Burns 4 studied DMS in patients with and without the evidence of organic cerebral disorder, and they concluded that symptoms of delusional misidentification arising in patients with evidence of organic disorder appear to be as sensitive to pharmacological treatments as those arising from functional disorders. In addition, Devinsky 61 claims that the division between delusions in psychiatric (primary) and neurologic-systemic disorders (secondary) is artificial, since psychiatric disorders with delusions have functional and structural brain pathology. However, appropriate identification and adequate treatment of false beliefs have the potential to make a simple but important contribution to patient care and caregiver quality of life. If the patient is neither agitated nor combative and the delusional symptoms cause minima distress, then nonpharmacological interventions, including reassurance and redirection, should be considered before a medical trial. Educating caretakers about the patient’s delusional symptoms and encouraging them to maintain patience may contribute to reducing the patient’s emotional distress. A clinical imperative exists to identify those at risk of violent acts and to isolate the underlying mechanisms. There are no controlled studies about pharmacological treatment of DMS. In a article by Zanker, 98 the author states the symptoms of DMS are very refractory to treatment despite various neuroleptic therapies, but the literature indicates that they are sometimes responsive to typical and atypical antipsychotics such as olanzapine, 99 risperidone, 19 quetiapine, 100 sulpiride and trifluoperazine, 50 and pimozide. 101,102 Roane et al 92 proposed clozapine, an antipsychotic with specificity for mesolimbic DA receptors, as generally effective and well tolerated in patients with PDD plus DMS, confirming previous findings. 103 A study showed a positive outcome in a patient with CS after treatment with mirtazapine. 104 This antidepressant drug is also a serotonin 2A receptor antagonist, which could potentially afford its antipsychotic effects resulting in alleviation DMS. 104 Such a conclusion, however, is only speculative without controlled clinical studies to demonstrate a potential antipsychotic action of mirtazapine. Spiegel et al, however, confirm the efficacy of mirtazapine in significantly decreasing the symptoms in a case of CS. 105 With patients who have progressive dementia, such as DLB, in which DMS is common, cholinesterase inhibitors have demonstrated some ability to reduce psychiatric symptoms. 106
Conclusions
In the DMS, a patient incorrectly identifies or reduplicates persons, places, objects, or events. They are initially reported to be associated only with psychiatric diseases, but, more recently, they have also been described in neurological conditions, and especially in neurodegenerative diseases such as AD and DLB and other associated disorders. 70,94 During the past 2 decades, neurophysiological and neuroimaging studies have pointed to the presence of identifiable brain lesions, especially in the right frontal lobe and adjacent regions, in a considerable proportion of patients with DMS. Early appreciation of DLB may afford the opportunity to alleviate caregiver uncertainty, permit intervention using both pharmacologic and nonpharmacologic approaches, and improve the well-being of their caregivers.
A better understanding of its psychopathology and the underlying biological substrates may increase the screening of the syndromes and, subsequently, avoid violent behavior.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.