
Abstract
We examined initiation of cholinesterase inhibitors (ChEIs) to determine whether ChEIs were being newly prescribed without sufficient evaluation for dementia and/or delirium and to explore whether there are differences in outcomes, such as mortality, hospital readmission rates, and duration of hospitalization, between patients newly started on ChEI and those who continued such medications prior to admission. Patients hospitalized in fiscal year 2008 and prescribed ChEI were identified. We reviewed electronic medical records. Of 282 patients, 15.6% (44) were new-starts and 84.4% (238) were continuations. Median length of stay was 16 days in new-starts versus 6 days in continuations (P < .05). Of new-starts, 38.6% were also treated of infection. Chart review additionally suggested possible treatment of delirium by initiation of benzodiazepines and antipsychotics in 11.4% and 22.7% of new-starts, respectively. We observed a substantive practice of initiating ChEIs in hospitalized elderly patients at risk of delirium. Although there was no difference in the 30-day mortality or readmission rates, new-starts were more likely to have a longer hospital stay than continuation patients.
Introduction
Older adults account for one-third of hospitalizations and nearly half of the national hospital bill. 1 The hospital stays of elderly patients are costly, largely because of their multiple chronic illnesses. Dementia is a major comorbidity, and its prevalence increases with age. 2 Dementia is one of the most debilitating challenges facing the geriatric population. 3
The diagnosis of dementia involves historical and clinical evidence of cognitive impairment severe enough to impair the social and occupational life of the patient. 4 History and physical examination are regarded as a guide to individualize the diagnostic approach in altered mental status. 5,6 The recommendation of use of standard mental state examinations in the clinic, a neuropsychology test, brain imaging, and blood tests checking vitamin B12 and thyrotropin levels are important to classify dementia types and to rule out other conditions that would look like dementia. 5 –8
Studies have suggested a depletion of the neurotransmitter acetylcholine (Ach) in patients with dementia; and “cholinesterase inhibitors” (ChEIs), which increase Ach availability by inhibiting Ach metabolism, may therefore be a possible treatment of dementia. 9 –11 It is recommended that one begin ChEI as soon as a diagnosis of mild to moderate dementia is made to benefit the patient 12 ; however, current primary care guidelines suggest initiation of ChEI based on individualized assessment. 13
The hospital setting may be unfavorable for initiating ChEIs for numerous reasons. The outpatient setting may be more appropriate than the inpatient setting for a thorough workup of cognitive impairment because of greater ease in assessing the longitudinal or historical aspects of cognitive function. Hospital-based physicians may encounter patients only acutely and for acute illnesses. Older hospitalized patients are at high risk of delirium, which may confound a diagnosis of dementia or develop independent of dementia. Studies have found that almost half of the hospitalized elderly individuals have delirium. 14 In a hospital setting, where delirium is highly prevalent, it is a challenge to clearly distinguish dementia from delirium because a diagnosis of dementia requires an in-depth collateral history and knowledge about prehospitalization functioning.
Studies have implicated Ach in the pathogenesis of both delirium and dementia, with a difference in chronicity: chronic Ach depletion is suggested in dementia, and shorter term depletion of Ach is suggested in delirium. 14,15 Despite this hypothesis, prior studies have not shown a benefit but rather adverse effects of the use of ChEI in delirium. 16 –18 For example, delirium was prolonged by 1.6 times, and mortality rates were 3 times higher in a multicenter, double-blind, and randomized trial of rivastigmine in intensive care unit patients with delirium. 19 Since delirium is highly prevalent in hospitalized older adults, it is difficult to make a new diagnosis of dementia during a hospitalization; and ChEI, rather than seeming to be helpful for delirium, instead may contribute to unfavorable outcomes in delirium; the issue of ChEI initiation during hospitalization deserves more attention. The goal of this study was to describe the prevalence of newly initiating ChEI in hospitalized patients and to compare outcomes of such patients with those of patients who continued ChEI during their hospitalizations, that is, those who had previously begun ChEI treatment in an outpatient setting. The first aim of the study was to determine whether, for patients with suspected dementia upon hospital admission, dementia medications (ChEIs) were being prescribed without a minimally sufficient evaluation for dementia and/or delirium; the second aim was to describe differences in outcomes, such as mortality, hospital readmission rates, and duration of hospitalization, between patients newly started on ChEI and those who continued such medications. We postulated that patients newly started on ChEI are more likely to have adverse outcomes, such as increased mortality, increased hospital readmission rates, and increased duration of hospitalization.
Methods
Data Sources, Sample, and Definitions
This retrospective electronic medical record review was conducted at the Michael E. DeBakey Veterans Affairs Medical Center in Houston, Texas, with approval from Baylor College of Medicine institutional review board and the MEDVAMC Research and Development Committee. All veterans who were prescribed ChEI during a hospitalization during fiscal year (FY) 2008 (October 1, 2007, to September 30, 2008) were included in the study. The local MEDVAMC pharmacy database provided a list of all hospitalized patients who had received ChEIs during FY 2008. We then used the computerized patient record system for in-depth review of the medical records of identified patients. Records were abstracted primarily to differentiate between patients who were newly initiated on ChEI during the hospital stay, defined as not having a history of ChEI use for at least 3 months prior to their hospital admission (“new-starts”), and patients who had been taking ChEI before their hospital admission and who continued on ChEIs during their hospitalization (“continuation group”).
On the basis of the review of admission notes and the history and physical notes documented in the computerized patient record system, we abstracted information on the following: age, race, place of residence (home, nursing home, assisted living, and personal care home), discharge location, type of dementia, documented presence of comorbidities: diabetes, hypertension, chronic kidney disease, cirrhosis, stroke, coronary artery disease, and heart failure, number of medications on admission, and evidence of active infection during admission (extrapolated by those who were initiated on antibiotics during hospital stay).
In this study, we use the term dementia to denote the most common dementias, that is, Alzheimer’s disease, vascular dementia, mixed dementia, and dementia with Lewy bodies. A detailed distinction is not possible, as often the diagnosis coding is dementia instead of specific subtypes of dementia. We abstracted evidence for specific workup for dementia, including vitamin B12 level and thyrotropin level, brain imaging (computed tomography or magnetic resonance imaging), and standardized cognitive testing prior to starting ChEI for presumed dementia. We abstracted the charts for any coding or other documentation of delirium, use of the confusion-assessment method, or anything to suggest delirium. Given the absence of “delirium” as a diagnosis in chart reviews, we used prescription of initiation of benzodiazepines or antipsychotics as a surrogate marker for delirium, 20 because use of such medications is often highly suggestive of the presence of delirium.
Statistical Analysis
Descriptive analyses were conducted on both the new-start and the continuation group patients. We used chi-square tests to analyze the differences in race, ethnicity, living situation, discharge location, reasons for admission, dementia types, comorbidities, types of medication used, services initiating ChEI, and workup done to assess impaired cognition between the 2 groups. The chi-square test was chosen, because all these data were presented as categorical. Similarly, categorical data on mortality differences were also compared using the chi-square test. To compare the mean age and number of medication uses between the 2 groups, we used t tests. A survival analysis was conducted to examine the hospital length of stay between the 2 groups, those newly started and those already taking ChEI. To test whether the patients newly started on ChEI were more likely to experience a rehospitalization or death earlier than those already on ChEI, a Kaplan-Meyer analysis was conducted.
Results
There were 282 hospitalized patients who received ChEI in FY 2008 among the 13 756 hospital admissions that year. 21 Of those, 44 (15.60%) patients were newly initiated on these medications during their hospitalizations. Among the newly started patients, 36 (82%) were ChEI naive; and 8 had taken ChEI in the remote past (>3 months earlier). Tables 1 to 5 compare the characteristics of new-starts and patients in the continuation group.
Demographics of the New-Start and Continuation Groups.
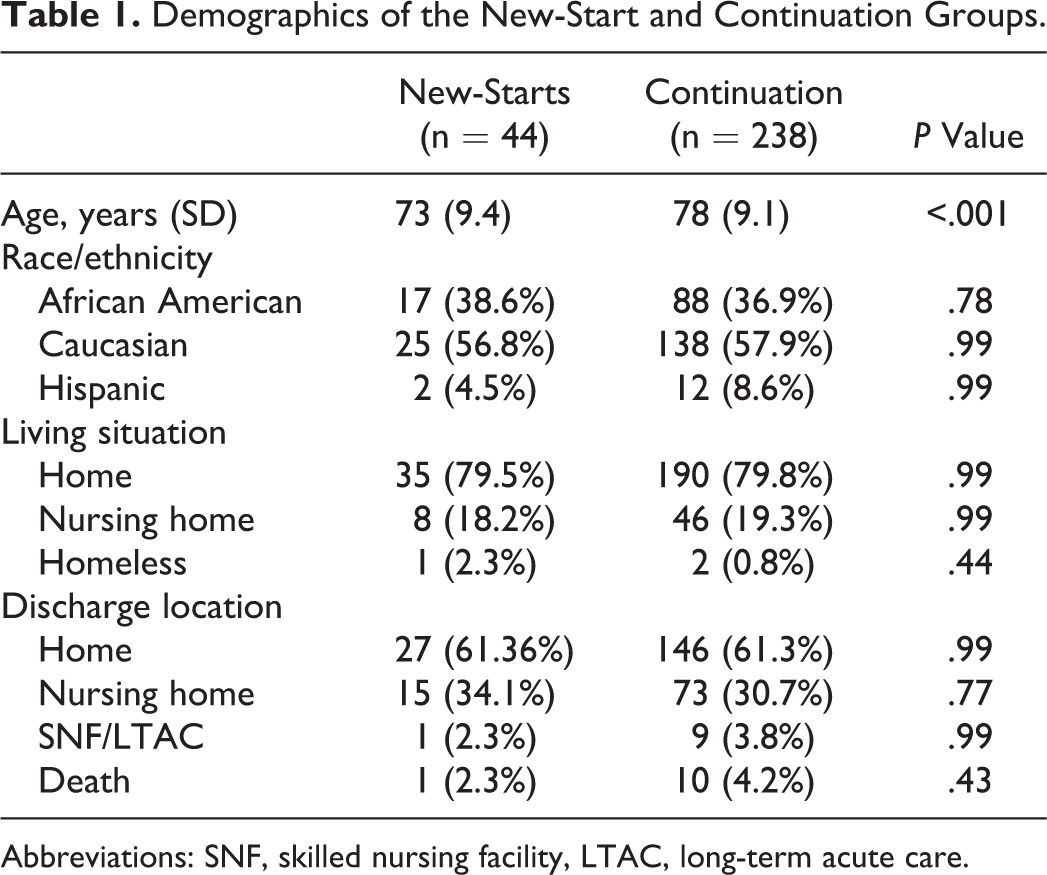
Abbreviations: SNF, skilled nursing facility, LTAC, long-term acute care.
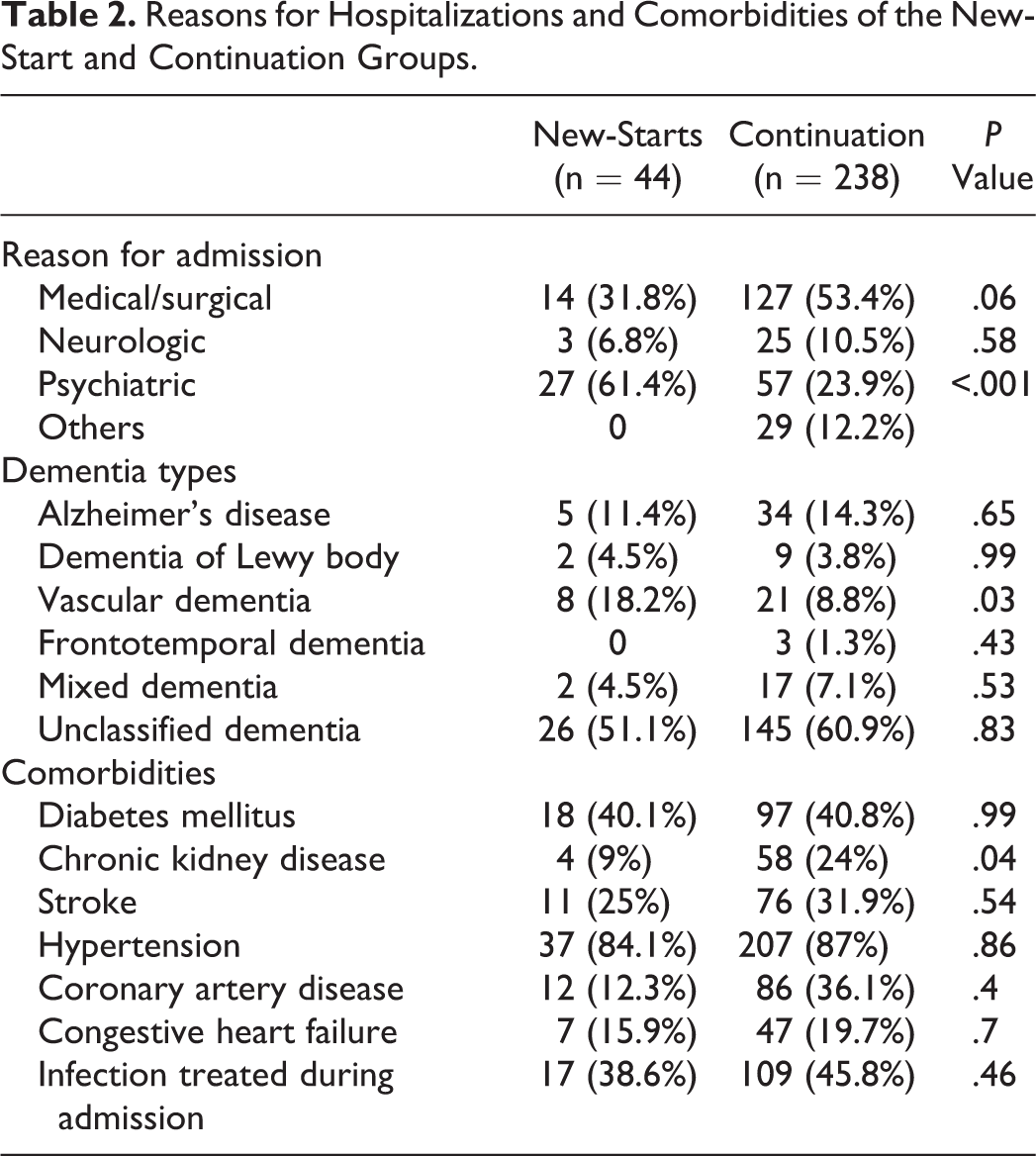
Table 1 presents differences in demographics. Given the Veterans Affair (VA) setting, there were almost no women patients (1 in new-starts and 4 in the continuation group). New-starts were significantly younger than continuation patients. Racial/ethnic distribution, living situation, and discharge locations between the 2 groups were similar. Table 2 presents admission reasons, dementia diagnosis, and comorbidities at the time of admission. Many admissions in the new-starts group were due to behavioral and psychiatric reasons; and, thus, this group had a higher rate of psychiatric-related admission. Comorbidities were similar in both the groups, except for a higher prevalence of chronic kidney disease in the continuation group. We also abstracted evidence for the treatment of an active infection during the hospitalization. While there was no difference in infection treatment between the groups (P = .46), the high prevalence of infection (39% among new-starts and 46% in the continuation group) was a significant potential predisposing factor for the development of delirium, suggesting that adequate evaluation was not done to rule out delirium prior to initiating ChEI.
Reasons for Hospitalizations and Comorbidities of the New-Start and Continuation Groups.
We examined the use of memantine, tricyclics/antihistamines, antipsychotics, and benzodiazepines besides the use of ChEI (presented in Table 3). Additionally, we abstracted which type of service started the ChEI. Of newly started patients, 59% had the ChEI started by a psychiatry team. Almost all of these patients were admitted to the psychiatry service because of behavioral issues; only 2 patients were on a medicine floor, where a psychiatry service started ChEI through a consultant.
Medication Usage Between New-Start and Continuation Groups.
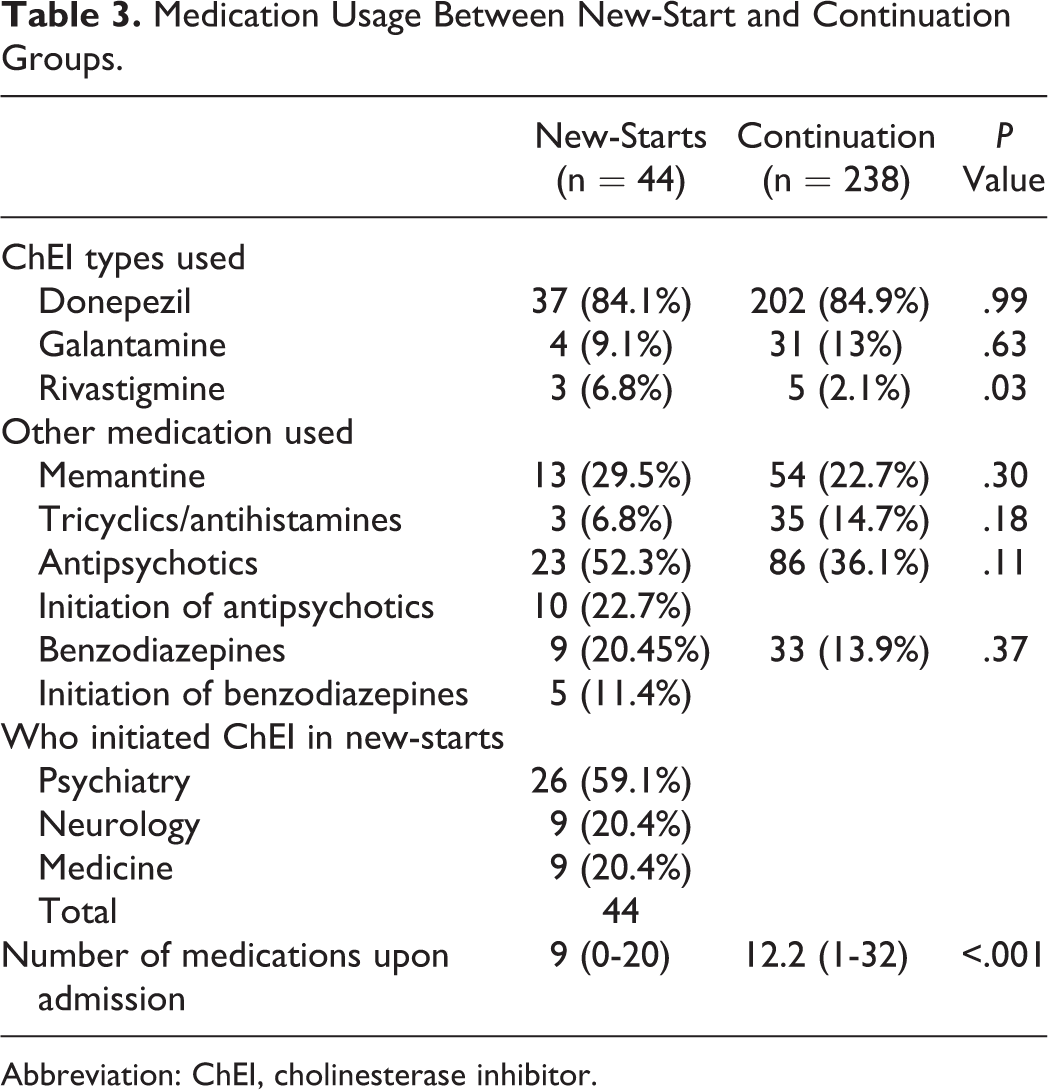
Abbreviation: ChEI, cholinesterase inhibitor.
The number of admission medications was documented and found to be significantly different between the groups: continuation patients were prescribed, on average, 3 more medications compared to the new-starts and polypharmacy (defined by use of 5 or more medications 22 ) was highly prevalent in both the groups. Among the new-starts, 23 (52.3%) and 9 (20.45%) patients were taking antipsychotics and benzodiazepines, respectively, during the hospital stay. In a further review of new-starts taking antipsychotics, 10 (22.7%) patients were initiated on antipsychotics during the index hospitalization, and 7 received the medicine intramuscularly, highly suggestive of active treatment of delirium. With regard to the use of benzodiazepines in the new-starts, 5 (11.4% of new-starts) of these patients were initiated on benzodiazepines during their hospital stay; 3 received the drug via the parenteral route. Antipsychotics and parenteral benzodiazepines are commonly used for symptomatic management of delirium. 14
Although most patients in both groups underwent blood tests for thyrotropin level and vitamin B12 level, as well as brain imaging, the new-starts were significantly more likely to undergo cognitive screening tests (Mini-Mental State Examination, Montreal Cognitive Assessment Tool, and St Louis University Mental Status Examination) than continuation patients (P ≤ .001), suggesting that these patients’ clinical presentation posed more of a challenge and that the treating team made some effort to establish a diagnosis of dementia (presented in Table 4). However, the overall rate of 57% of such testing in new-starts was still low.
Workup to Assess Impaired Cognition Between New-Start and Continuation Group.
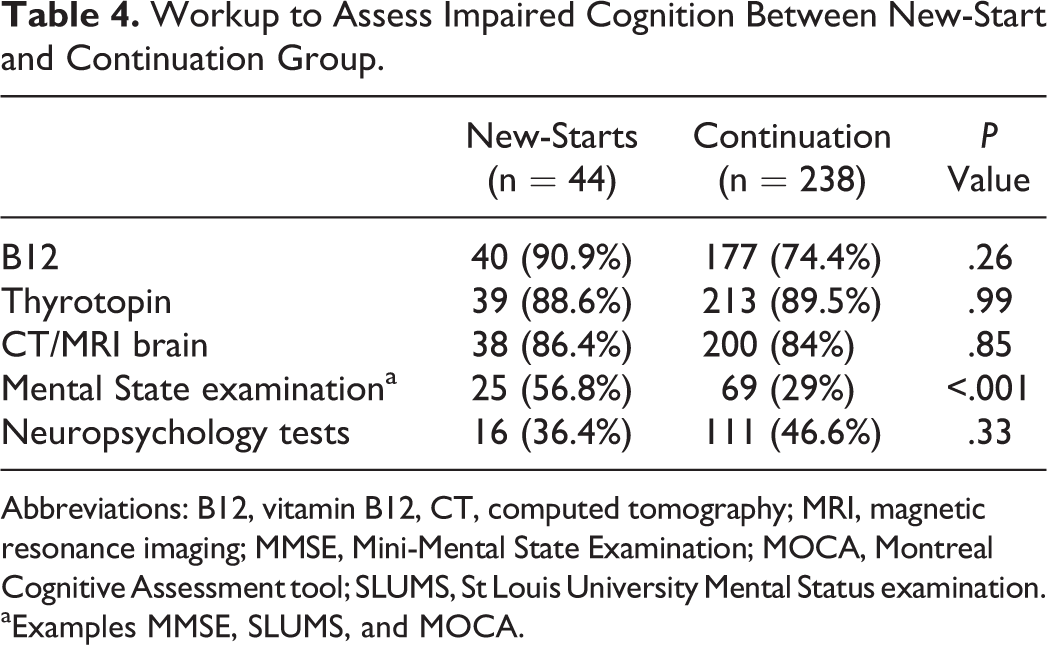
Abbreviations: B12, vitamin B12, CT, computed tomography; MRI, magnetic resonance imaging; MMSE, Mini-Mental State Examination; MOCA, Montreal Cognitive Assessment tool; SLUMS, St Louis University Mental Status examination.
aExamples MMSE, SLUMS, and MOCA.
Evaluation of our clinical outcome is presented in Table 5. A survival analysis was conducted to examine hospital length of stay between the new-start and the continuation groups. The hazard function differed between these 2 groups (with 1 degree of freedom, Mantel-Cox log-rank test statistic 28.5, P < .01; see Figure 1). As a group, the newly prescribed patients had a longer length of stay. For those newly prescribed, half had been discharged by the 16th day of the index hospitalization; whereas half of those already prescribed had been discharged sooner, that is on the 6th day. The mean length of stay of new-starts was 28.5 days, whereas the mean length of stay of the continuation group was 9.2 days. Mean lengths of stay in days between new-starts who were initiated by nonpsychiatric services and those initiated by psychiatric services were not statistically different (29.8 vs 27.9 days, respectively; P = .88).
Patient Outcomes New-Start Versus Continuation Groups.
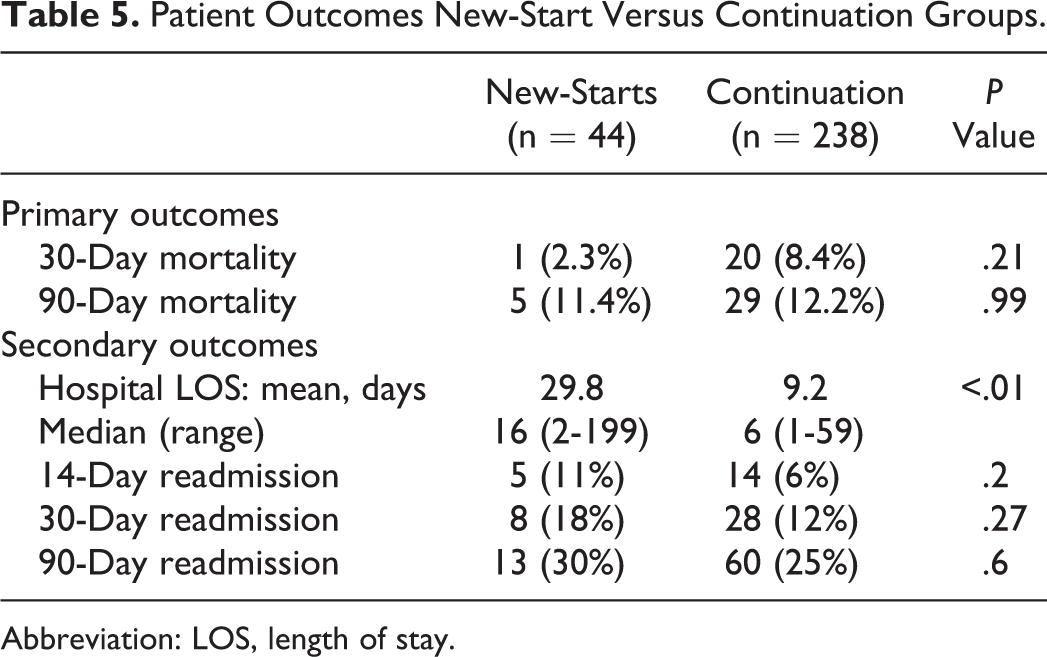
Abbreviation: LOS, length of stay.
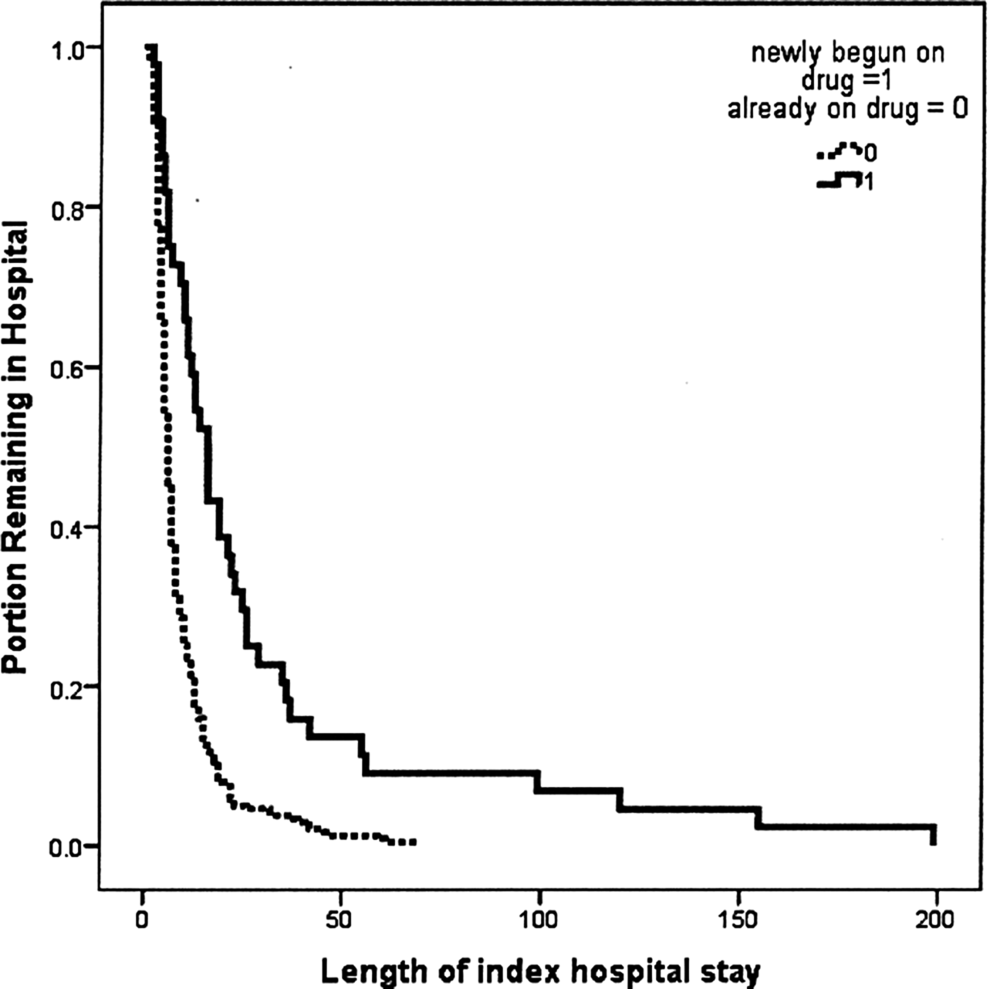
Survival analysis examining hospital length of stay between new-start and continuation groups.
In addition, to test whether the patients newly started on ChEI were more likely to experience a rehospitalization or death earlier than those already on ChEI, a Kaplan-Meyer analysis was conducted (see Figure 2). The value for the Mantel-Cox log-rank statistic (with 1 degree of freedom) was 0.043, with a significance of .84, indicating that the survival functions for the 2 groups were not statistically significantly different; across this surveillance period, neither group was more likely to have an earlier time to readmission. Comparison of 14-, 30-, and 90-day readmission data showed no statistically significant difference between the groups but did show a trend for more readmissions in the new-starts.
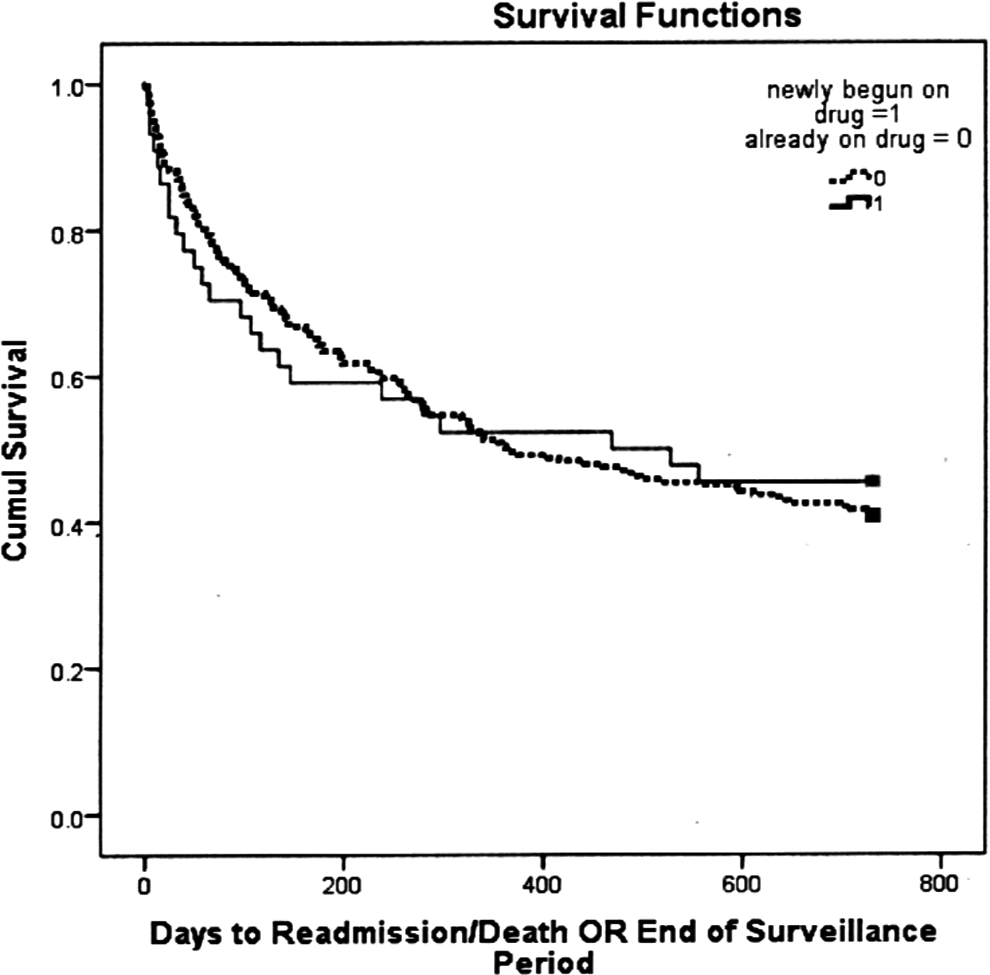
Survival analysis examining composite outcome of hospital readmission or death between new-start and continuation groups.
Discussion
This study is the first to examine the prevalence of ChEI initiation in a VA setting. Our study showed that 15.6% of hospitalized patients receiving ChEI had these drugs initiated during their hospitalization. This frequency seems very high as ChEI is used for long-term treatment. Many of the new-start group patients were not adequately evaluated to rule out delirium prior to ChEI initiation, as shown by rates of infection, antipsychotic and benzodiazepine use, and their advanced age.
Prudent use of medications is a modifiable factor for decreasing common iatrogenic adverse events, 23 and identifying such practices can help avoid adverse health consequences and health care costs, thus constituting a public health concern. Physicians might initiate ChEI in patients hospitalized for dementia; however, there is a high likelihood of having at least a coexisting acute delirium. On the other hand, physicians might initiate ChEI in patients hospitalized for delirium; however, there is no evidence base for such a practice. Several investigators have examined the usefulness of ChEI in patients with delirium, but none has found any evidence to support their use for this indication. 16 –19
van Eijk et al 19 conducted a randomized, double-blind, and case–control study in multiple intensive care unit settings in the Netherlands, looking for duration of delirium, in which patients received ChEI as a treatment of delirium in comparison with controls who received the usual standard of treatment without ChEI. The study had to be prematurely stopped by the Drug Safety and Monitoring Board because of increased mortality among the patients. Results of the study showed that the mortality rate in the treated group was 22% (n = 54) and in the nontreated group was 8% (n = 50), during the course of treatment. This triggered the cessation of the study for crossing the benefit/risk threshold. The difference in mortality outcomes in our study was not statistically significant. However, difference in mean length of hospital stay (28.5 days in new-starts vs 9.2 days in continuation group) was statistically and clinically significant (P < .001) in our study.
Marcantonio et al studied donepezil for preventing the incidence of delirium in elderly patients undergoing hip surgery. 24 Although the sample size of the study was small (n = 16), the donepezil group had a higher incidence of side effects, such as insomnia and diarrhea; and there was no difference in the incidence of delirium between the 2 groups. 24 Even though long-term use of ChEIs has been shown to prevent delirium, 25,26 it seems that, at the time of acute alterations in cognitive function, initiation of ChEI is not justified. Up to 72% of delirium remains unrecognized during acute hospitalization, 19,27 which may be another manifestation of the difficulty discriminating between dementia and delirium in an inpatient setting.
Inappropriate addition of medications increases problems with polypharmacy, consistently recognized as an independent predictor of adverse drug reactions in elderly patients. 28 Polypharmacy is also reported to increase hospital length of stay and hospital costs. 29 Prior studies have shown that polypharmacy is associated with functional decline, morbidity, and mortality, 30 and increasing the number of medications seems to correlate with increased risk of drug–drug interactions. In our study, we saw that many elderly patients were taking >10 medications at admission. A prior VA study showed the prevalence of unnecessary medication use at 42%. 31 A thorough review of the medication list, along with a medical and surgical history, prior possible drug–drug interaction, comprehensive geriatric assessment, and consideration of goals of care and life expectancy, has been proposed by prior studies to prevent polypharmacy. 32,33 We found polypharmacy to be an issue in this study, and it needs to be further explored. However, this supports our argument against adding another new medicine (ChEI in this case) without proper evidence in patient population, where polypharmacy is already a prevalent issue.
This study has several limitations. It was conducted in a single hospital, an urban tertiary care VA medical center; and, thus, the predominantly male sample limits generalizability. We did not prospectively assess for the development of delirium, and medical record review may have been limited by incomplete documentation. The assumption that parenteral administration of antipsychotics or benzodiazepines signaled delirium may also be tenuous. The strength of our study was the availability of an integrated electronic medical record system that allowed easy data collection, and information about mortality and readmission rates was readily available. The readmission data may underestimate readmission rates, as patients could have been admitted to hospitals other than the Michael E. DeBakey Veterans Affairs Medical Center. However, this underestimation would similarly affect both new-start and continuation patients. Results from this study may impact formulary decisions for the inpatient setting. By recommending against initiation of ChEI in an inpatient setting, adverse events from inappropriate medication use may be prevented, and unnecessary costs of hospitalizations reduced.
We observed a practice of not adequately ruling out delirium prior to initiation of ChEI in an inpatient setting. Older, hospitalized veterans are at increased risk of delirium secondary to medical and surgical conditions, infections, and so forth. An inpatient setting may not be optimal for newly diagnosing dementia or initiating ChEI treatment, and good support for such treatment of delirium is lacking; additionally, it may prolong length of stay. To prevent adverse events in the vulnerable, chronically ill elderly patients, ChEIs are best initiated in an outpatient setting, where chronicity of cognitive impairment is better assessed than in an inpatient setting, and the chances of delirium are lower.
Footnotes
Authors’ Note
The views expressed reflect those of the authors and not necessarily the policy or position of the Department of Veterans Affairs, the US government, the Health Resources and Services Administration (HRSA), or Baylor College of Medicine.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partly supported by resources and facilities of the Houston VA HSR&D Center of Excellence (HFP90-020). Dr Wagle was supported by the Huffington Center on Aging and the John A. Hartford Foundation Center of Excellence in Geriatrics. Dr Braun was supported by a Geriatric Academic Career Award, KO1HP20480, through the HRSA.