
Abstract
The Kingston Standardized Cognitive Assessment (KSCA) was designed to be a cognitive screening tool available for the health professionals who were not trained in specialized cognitive assessment techniques. It was introduced to bridge the gap between brief, narrowly focused rating scales and intensive, expensive, full neuropsychological assessments. We now present the mini-KSCA-Revised (mini-KSCAr). This is a shortened version of the full KSCAr that can be given in far less time and allows for a quick follow-up or screening technique retaining a substantial part of the full KSCAr’s effectiveness. It is specifically targeted for use by family physicians who require rapid and accurate in-office dementia screening.
Keywords
Introduction
As we endeavor to respond to the ever-increasing growth in dementia prevalence and resulting demands for appropriate care, 1 -4 there will be a greater need for accurate and time-efficient cognitive assessments that can be easily administered and interpreted and provide meaningful information. Over the past 20 years since the original Kingston Standardized Cognitive Assessment (KSCA) was first published, 5 it has proven to be an effective and efficient tool to assess cognitive functioning in individuals with progressive dementia, as has its revision, 6 which made the KSCA sensitive to very early dementia (see Wechsler Scale correlations in KSCA-Revised [KSCAr] article 6 ). It has been translated in a variety of languages 7 and is used in many settings worldwide (Hopkins R. Personal communication). These tools were designed to fill an important gap between rating scales that are too short, nonspecific, or narrowly focused, such as the Mini-Mental State Examination 8 or the Montreal Cognitive Assessment, 9 and more comprehensive but lengthy and expensive neuropsychological assessments. However, some individuals have found that the full KSCAr takes longer to administer than is practical in many primary care settings. To remedy this problem, a shorter version of the test that retains the power of the KSCAr to identify cases of dementia, and specifically designed for such settings, has been devised. This article introduces the mini-KSCAr.
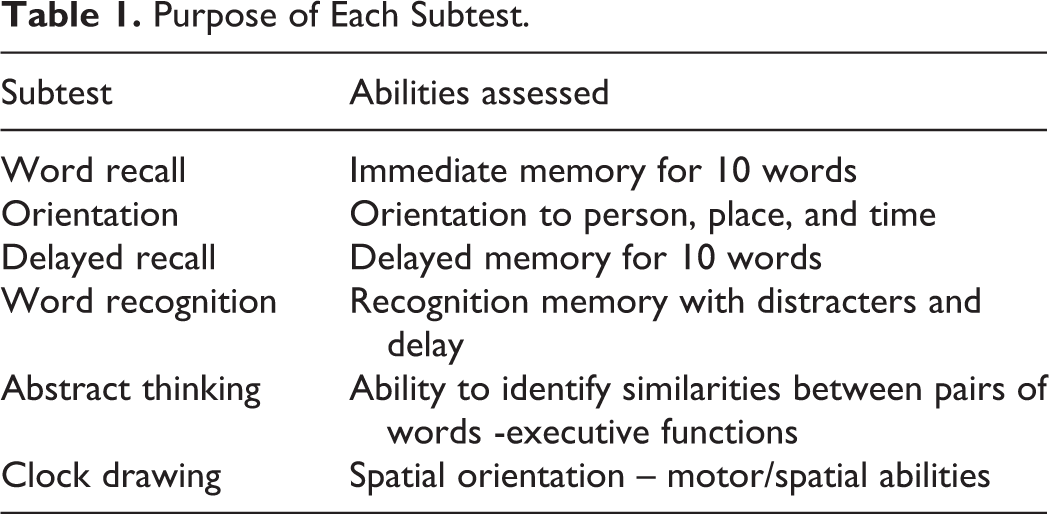
The mini-KSCAr is made up of 6 tasks from the full KSCAr that are most sensitive to early changes seen in cognitive functioning as seen in the cases of early Alzheimer’s disease from our clinic. It is normed on both community dwelling dementia cases and normal elderly controls, and like the KSCAr, the mini-KSCAr was designed to be administered by clinicians who do not necessarily have special training in psychometrics or test interpretation. Rather than using very short procedures that do not assess any particular function adequately, the mini-KSCAr is shorter by reducing the number of subtests used, from 19 to 6. The 6 subtests that comprise the mini-KSCAr are identical to their counterparts in the full KSCAr. The mini-KSCAr contains 4 memory tasks (orientation, word recall, delayed recall, and word recognition), 1 visual motor task (clock drawing), and 1 executive function task (abstract thinking; see Table 1 for more information about each subtest). These subtests were chosen after studying a group of high functioning patients with early Alzheimer’s disease for their sensitivity to the mild brain damage seen in the early stages of dementia as well as ease of administration. Any subtest that did not contribute to the variability due to early dementia was removed from the test.
Purpose of Each Subtest.
Of note, the 6 subtests comprising the mini-KSCAr may be familiar to clinicians in the field of geriatrics as they are modified versions of well-established cognitive tests, which also have a proven history as parts of the KSCAr and Brief KSCAr. 10
However, the advantage offered by the mini-KSCAr is the co-norming of the individual subtests such that performance across subtests can be directly compared as norms for each subtest come from the same clinical sample. This, in turn, serves to minimize error and increase sensitivity.
The mini-KSCAr can be administered at the same time or less than other screening tools (ie, about 7-10 minutes.). It yields a single total score out of 55, which can be easily transformed into a percentile, from charts on the front page of the Assessment Form (see Figure 1). Scores can be compared to 2 groups, the normal elderly group and a community dwelling Alzheimer’s disease group. Like the full KSCAr, the mini-KSCAr comes with an “Administration and Scoring Manual” 7 that outlines scoring procedures (with templates for the clock subtest), an interpretive guide for each subtest, and also contains norms for other groups such as mixed dementias and elderly patients with depression without dementia.
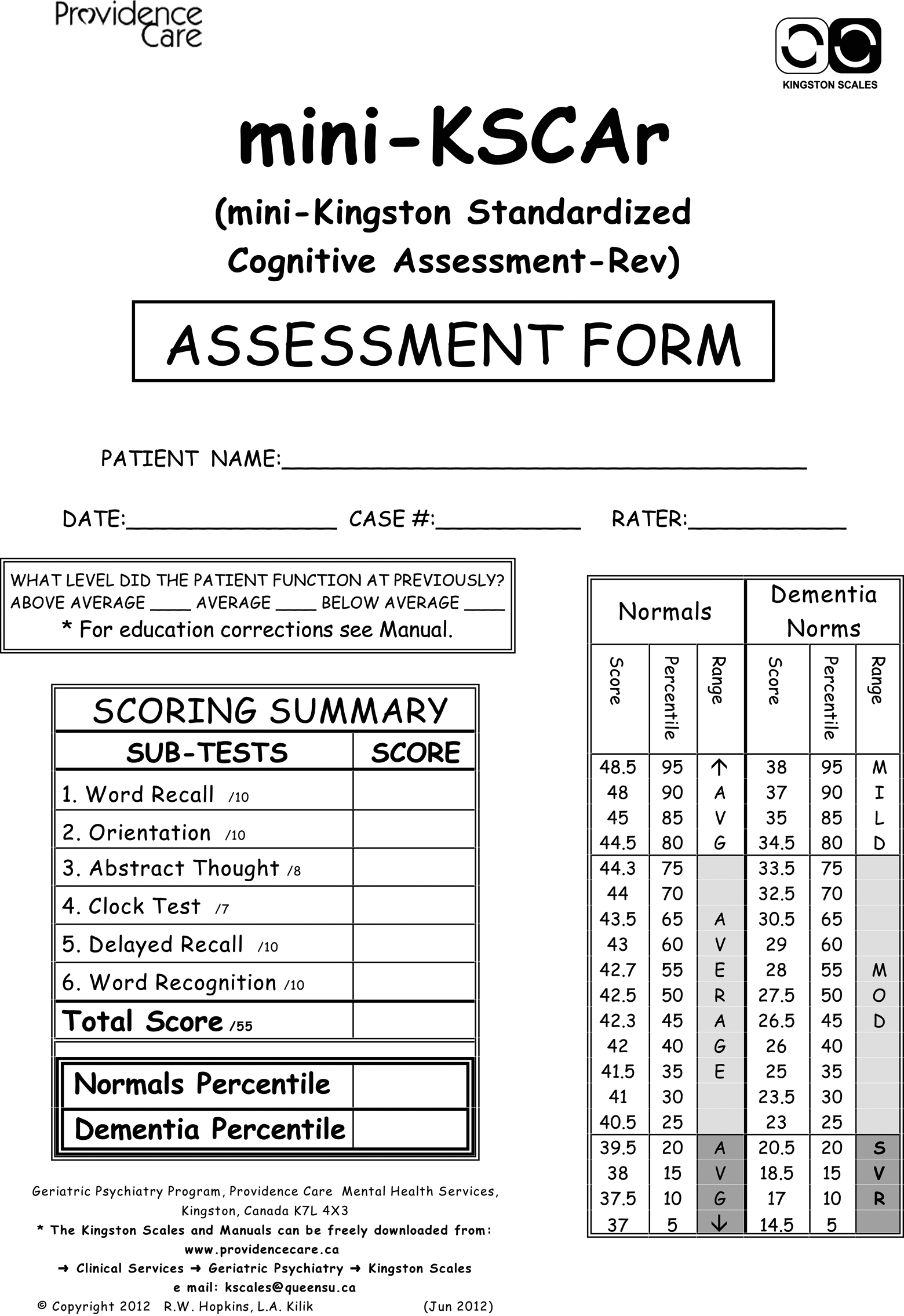
Mini-Kingston Standardized Cognitive Assessment-Revised (first page).
Methods
The psychometric properties of the original KSCA 5 and KSCAr 6 have been described. Data used for the norms were collected from community-living individuals aged 65 years or older, both with and without dementia. The dementia group comprises individuals who were referred to a regional geriatric psychiatry program and who were diagnosed with probable Alzheimer’s disease, according to both Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition) 11 and National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association 12 criteria. Inclusion and exclusion criteria as well as demographics for each group are provided in Table 2.
Comparison of Normal and Alzheimer’s Disease Groups.
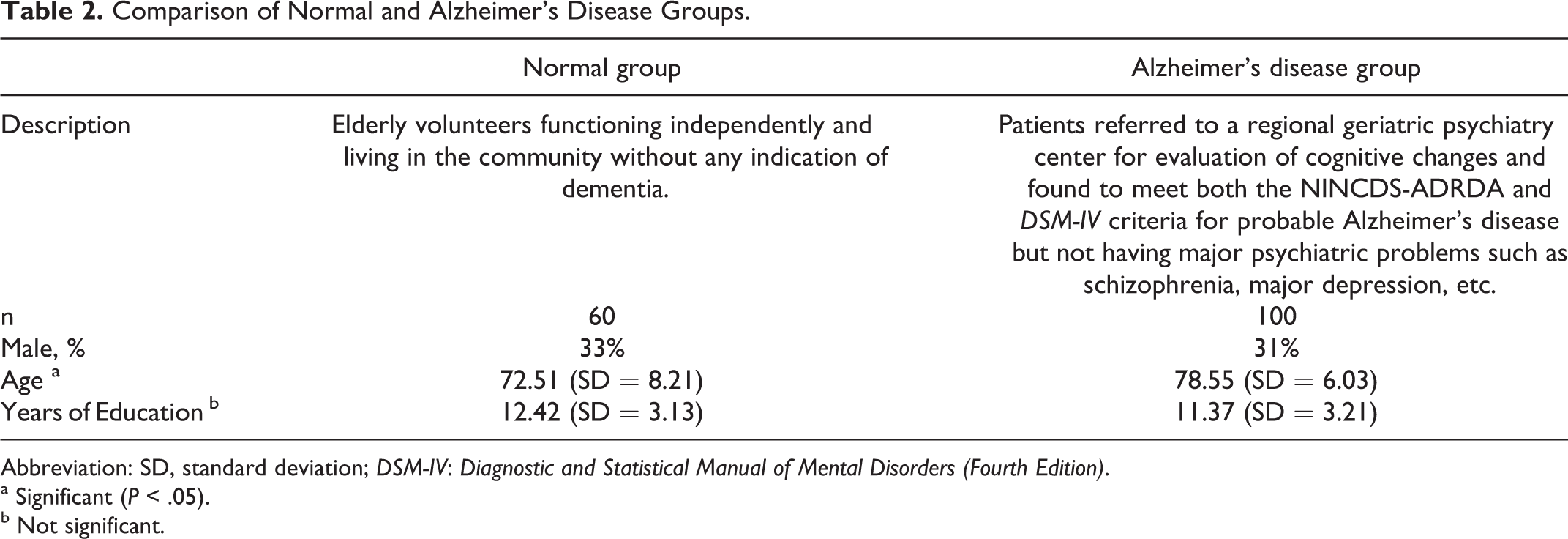
Abbreviation: SD, standard deviation; DSM-IV: Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition).
a Significant (P < .05).
b Not significant.
Results
The Mini-KSCAr total scores and subtest means for each group were calculated and are provided in Table 3. It should be noted that the Alzheimer’s group performed significantly (P < .01) more poorly than the normal group on all subtest scores as well as total score. Although the Alzheimer’s disease group was significantly older (P < .05), an analysis of covariance revealed that the score differences remained significant after controlling for the effects of age. Although age is associated with an increased risk of developing dementia, it is not simply an effect of age alone. Subtest rater reliability and subtest to total score correlations are found in Table 4.
Normative Statistics (Normal Elderly Controls and Alzheimer’s Disease Group).a
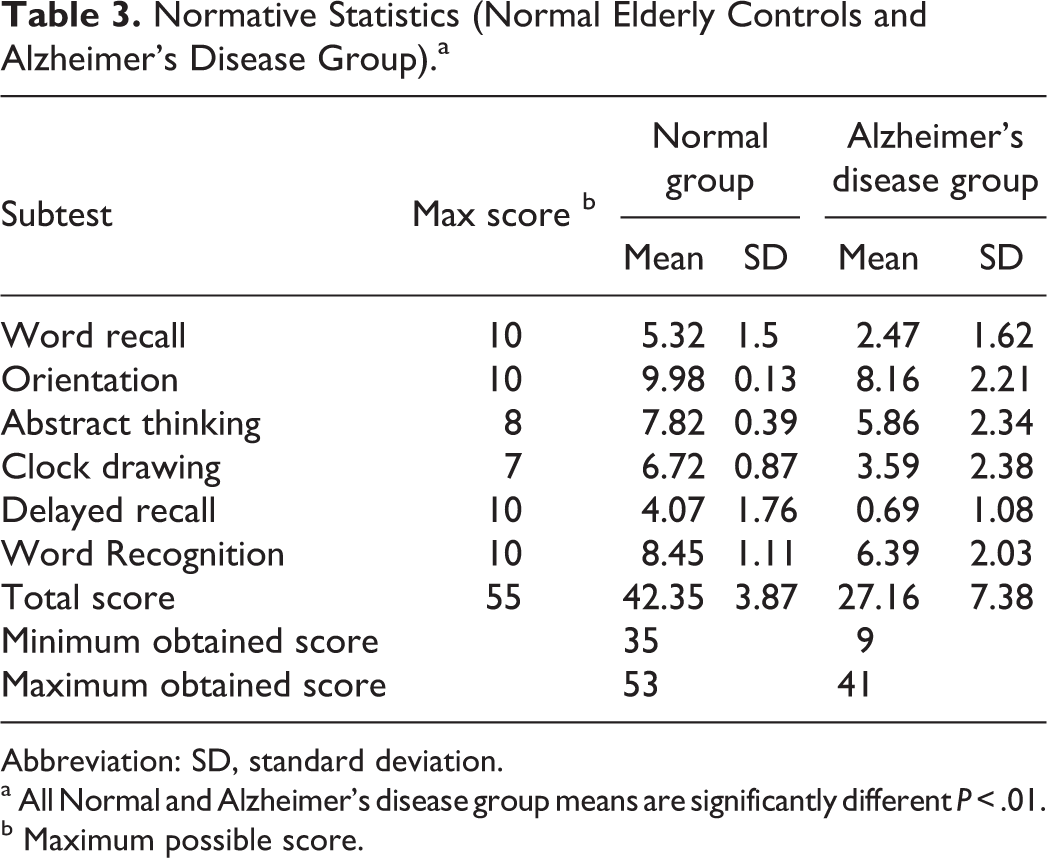
Abbreviation: SD, standard deviation.
a All Normal and Alzheimer’s disease group means are significantly different P < .01.
b Maximum possible score.
Subtest Correlations With Total Score and Subtest Interrater Reliability.
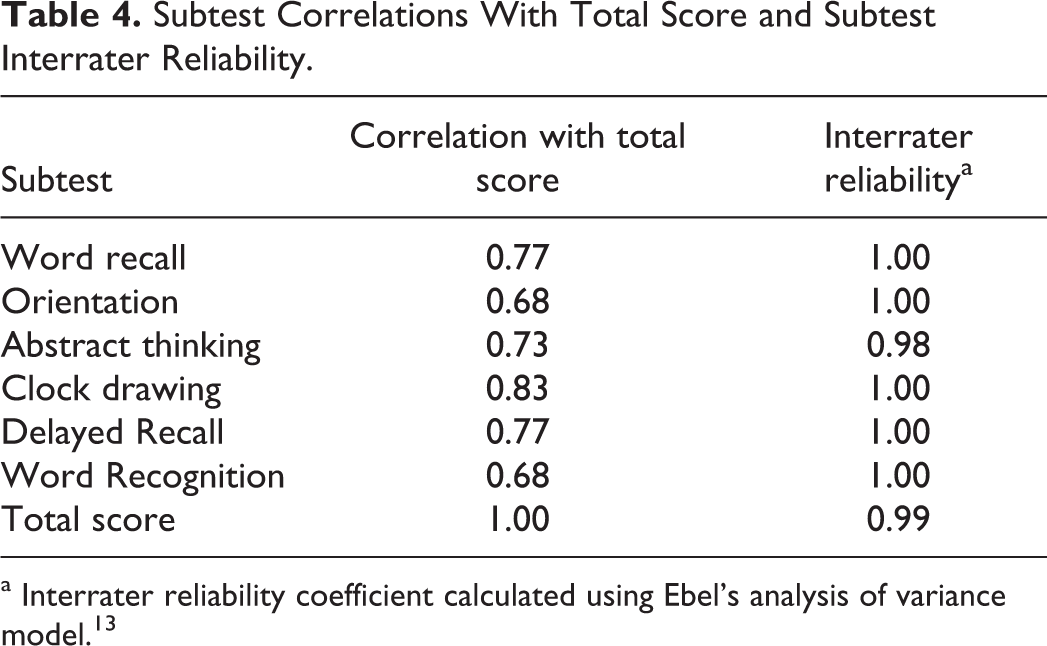
a Interrater reliability coefficient calculated using Ebel’s analysis of variance model. 13
As sensitivity to early dementia increases, it is also important to minimize the overlap between normal and dementia groups. The mean of total score for the normal group was 48.6 (standard deviation [SD] 4.2), while the mean of the Alzheimer’s disease group was 31.6 (SD 9.8). As can be seen in Figure 2, there is relatively little overlap between the distributions of the normal and the Alzheimer’s disease group.
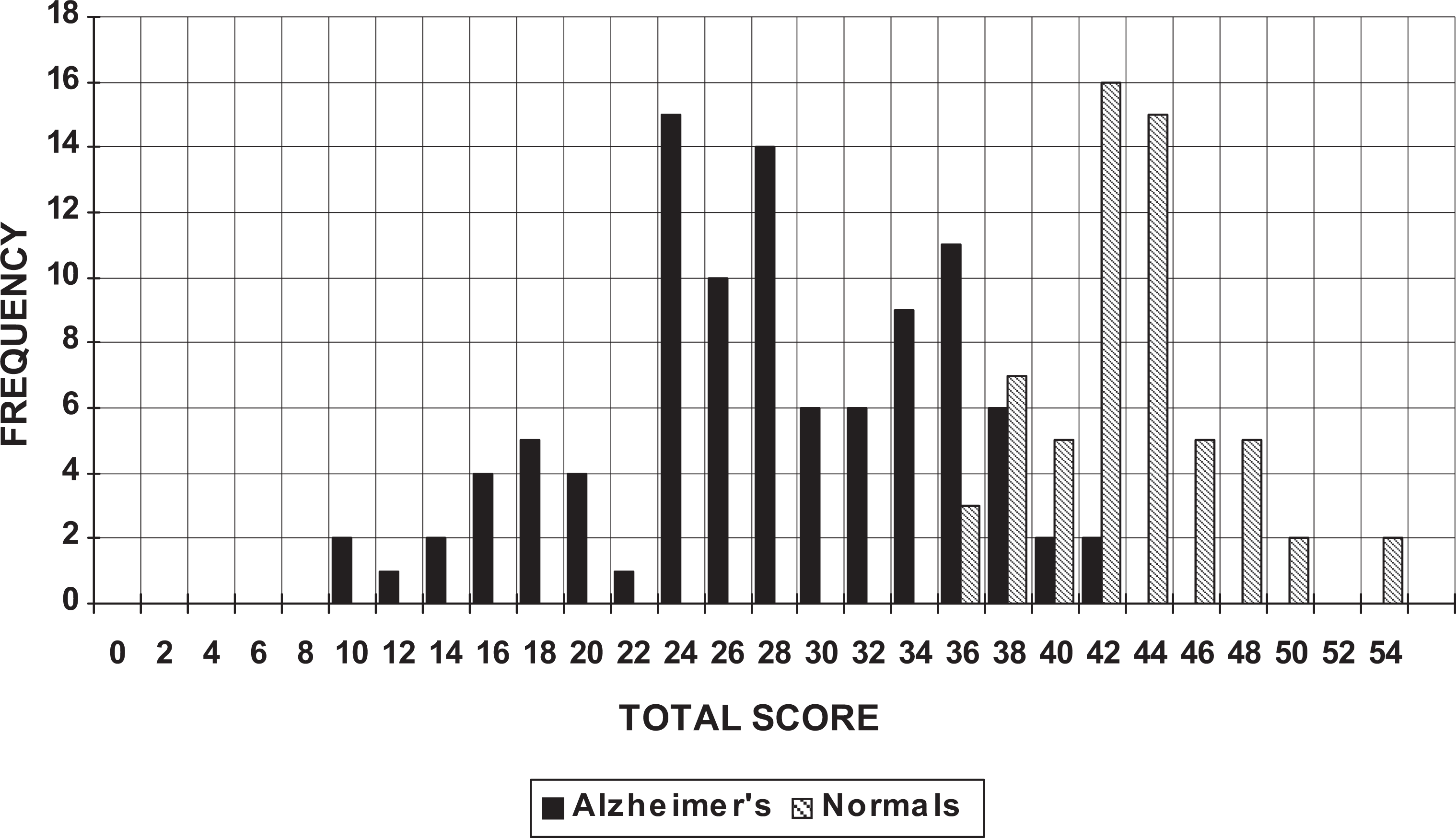
Total score distribution for normal and Alzheimer’s disease groups.
In addition, we performed a standard discriminant function analysis to demonstrate the mini-KSCAr’s ability to predict group membership. The standard discriminant function analysis was performed using the mini-KSCAr’s total score as the predictor of membership in the normal and the Alzheimer’s disease groups. Using the combined sample, 91.7% of the cases were correctly classified. The misclassified cases came from the Alzheimer’s disease group that was erroneously identified as “normal.” Although this method essentially relies on the derivation of a single cutoff score, which we strongly discourage, we include it as a basis for comparison.
In a study (unpublished) to assess test–retest reliability, 30 normal community-dwelling participants (all aged 65 years or older, mean age 73.2 years, SD 8.2) were tested and then retested 14 days later; mean scores increased only by 3.33 points (SD 3.28). This reflects the effects of some learning and familiarity with the test.
Discussion
Owing to the changing demographics and increasing public knowledge about dementia resulting from initiatives such as Alzheimer’s disease awareness campaigns, there is likely to be an increased demand for investigations of cognitive impairment in elderly persons. As a result, there will be a need for appropriate methods of cognitive evaluation which are both rapid and effective in detecting early dementia. To this end, we believe that the mini-KSCAr provides a useful tool for the primary care physician or others who need to rapidly screen for dementia. It strikes a balance between maximum clinical information gained and minimum assessment time. The mini-KSCAr can be administered quickly by clinicians not specially trained in mental measurement.
How short should a screening instrument be? Although brevity may be highly prized by busy physicians, a scale that is too short runs the risk of being incapable of adequately distinguishing normal individuals from those in early stage dementia or those with low premorbid intelligence from those with dementia. The diagnosis of a suspected progressive dementia is a very significant event for a patient. While this process, admittedly, should be efficient, it should not sacrifice quality for the sake of brevity.
In interpreting a patient’s performance, the mini-KSCAr uses distribution curves of normal participants and patients with Alzheimer’s disease as are commonly used in standard neuropsychological tests. In contrast, most other scales use a simple cutoff score (eg, 8-9, 16 -18 ), creating the problem of false positives and false negatives. The use of distributions for interpretation of performance, more realistically reflects the continuous nature of progressive dementias and the variations in individual baselines than do cutoff scores. The percentile ranks yielded by the distributions of both normal controls and Alzheimer’s disease groups facilitate clinical interpretation and communication of results. Despite the continuous nature dementia, which means that there will always be some overlap between normal and pathological distributions, the overlap between distributions with this scale is minimal, resulting in improved accuracy in the detection of early brain damage.
The choice of subtests used in the mini-KSCAr reflects the most common symptoms of early dementia, that is, memory loss (especially with a delay), motor/spatial problems, and executive function deficits. Memory is more thoroughly examined by the mini-KSCAr than most other screening tests, by examining orientation, immediate recall, delayed recall, and delayed recognition memory.
We feel that the clock test used in the mini-KSCAr is made more effective than those used in other screens, by breaking down the task into 4 stages, in decreasing difficulty to prevent learning, and by using a set of templates to facilitate accurate scoring. Also, the patient is never asked to draw a circle (circles are provided), which is a separate and somewhat unrelated skill. 19
That the mini-KSCAr yields a total score as well as individual subtest scores allows for a multi-level approach to interpretation of results. Unlike, the MoCA, for example, the mini-KSCAr individual subtests have established neuropsychological and psychometric roots that can stand alone, as apposed to being adapted fragments of cognitive tests with undetermined construct validity (see Table 5).
Mini-KSCAr Subtest and Total Score Correlations With MMSE and Wechsler Scales.
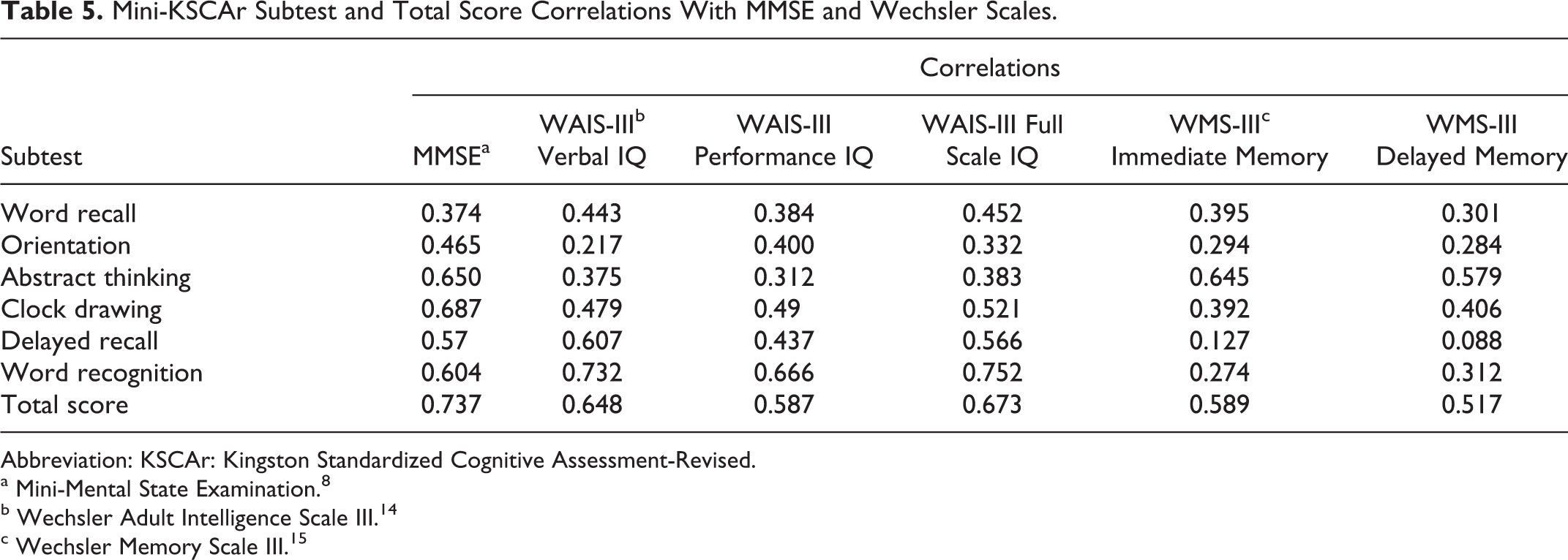
Abbreviation: KSCAr: Kingston Standardized Cognitive Assessment-Revised.
a Mini-Mental State Examination. 8
b Wechsler Adult Intelligence Scale III. 14
c Wechsler Memory Scale III. 15
When repeated over time, the mini-KSCAr can provide a valuable index of change. Also, while the mini-KSCAr (like the KSCAr) was designed as a clinical tool by clinicians, its breadth of sensitivity and demonstrated psychometric properties give it the potential to be a useful measure of cognitive status in a variety of research applications. The mini-KSCAr is made available from the authors free of charge and can be freely downloaded from our Web site. 7
Future Research
Future research with this instrument might include its use with more specialized neurological disease groups and in comparative studies with other screening tools. Its value as a measure to track effects in drug studies may also offer promise.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.