
Abstract
A challenge in admitting individuals with Alzheimer’s disease and related dementias into memory care residential facilities is determining the appropriate level of service based on abilities and care needs. At intake, the incoming tenant’s functional performance capacity is obtained through family or proxy report corroborated with screening results of global cognitive function. Based on this information, the agency determines the level of service needs; if misjudged, inadequate placement can be stressful for the individual and family and costly for the facility. This study examined the predictive validity of a clinically administered assessment of cognitive-functional performance, Cognitive Performance Test (CPT), in gauging service needs in 4 activities of daily living (ADL; dressing, eating/feeding, showering, and toothbrushing) with 57 tenants residing in a memory care-assisted living facility. Linear regression results revealed a significant relationship between CPT scores and ADL performance in all areas (P < .001) with CPT scores accounting for 51% to 62% of the variability in performance.
Keywords
Introduction
Specialized, residential memory care has experienced a recent surge as health care has evolved to meet the increasing challenges of caring for persons with Alzheimer’s disease and related dementias (ADRD). Although 60% to 70% of all persons with ADRD live in the community, 30% are cared for in a facility designed to meet the needs of persons with moderate to severe cognitive deficits. 1 Memory care facilities range from assisted living facilities that provide varying degrees of supervision and assistance for persons with cognitive loss to full spectrum total care. Gauging the service needs is a complex process that impacts decisions about where the individual is cared for based on access to staff assistance and amenities.
Memory care facilities are designed to provide care for the person with ADRD over the course of the disease facilitating aging-in-place, but they do so at a cost. The 2012 report from the Alzheimer’s Association identified that 72% of assisted living facilities provide for memory care at the cost of $55 428 per year on average; memory care, apart from long-term care, is generally private pay. 2 Oftentimes, cost is congruent to the amount and type of services provided. Better methods for predicting service needs for incoming memory care tenants can inform families of the financial impact of memory care and anticipated financial burden as the disease progresses.
Intake processes for residential memory care typically include a family report of functional performance, screening for global cognition, along with a medical report of diagnosis and comorbidities. In memory care facilities, cognition is typically the primary factor impacting function in people with dementia and considered along with secondary impairments in motor and praxis, sensory perceptual, and language and communication skills, or even frailty.
Intake procedures may include a family/proxy report of activities of daily living (ADL) performance. Although information reported by the family or proxy has been found to be in agreement with the person with dementia regarding ADL performance, the accuracy of report decreases with severity of the disease. 3 A direct assessment of ADL function, the Functional Independence Measure (FIM), is an observational scale applied in each self-care task and has been considered the gold standard in functional evaluation. 4 It requires observed performance of the task and can be time consuming to administer. In an initial intake, for the tenant with cognitive impairment, it can be confusing and/or intrusive to be asked to perform self-care tasks in a new environment with a professional observer.
Interdisciplinary tools screen for global cognitive deficits and indicate the severity of cognitive limitations but do not link to function; the most prevalent is the Mini-Mental Status Examination (MMSE). 5 The St Louis University Mental Status Exam 6 and Mini-COG 7 are tools to screen for dementia and grade degree of cognitive impairment. These provide information on the presence or absence of cognitive impairment (impaired/not impaired) or a gross indication of the severity (normal/mild impairment/significant impairment) but do not fully address functional implications. Neuropsychologists have sensitive measures of cognitive processes that reveal patterns of deficits focal to specific areas of the brain but again, do not link to function. 8 There is current emphasis on the development of ecologically valid measures of cognition that predict functional skills. 9
The Cognitive Performance Test (CPT) is a standardized, performance-based assessment used in clinical and home care evaluation by occupational therapy (OT) practitioners to predict cognitive-functional capacity in IADL and activities of daily living (ADL).10,11 Administration is efficient, taking less than 30 minutes, and sensitive to the individual’s cognitive challenges. It is part of a broader OT evaluation used to determine optimal potential for engagement in daily living activities. This study examines the validity of the CPT to predict functional performance with tenants in a residential memory care facility in 4 ADLs, dressing, eating/feeding, showering, and toothbrushing. The CPT has been shown to predict risk of institutionalization but has not been applied to measuring ADL function in memory care assisted living. 11 Predicting ADL performance based on a clinical measure of cognitive capacity could guide intake planning by predetermining the appropriate placement and the amount of service support anticipated prior to residential placement.
Impact of Cognition on Functional Performance
Much of the cost associated with care provided in memory care facilities is related to assisting the person with ADRD with basic daily care or ADLs. Community dwelling individuals with mild cognitive impairments may need increasingly more assistance and support for instrumental IADL. By the time, residential change is considered, typically in the middle stages of the disease with moderate cognitive loss, the area of occupation most affected is ADL. Studies show that dementia can impact ADL performance due to diminished episodic, semantic, and working memory, executive function, and visuoperceptual processing. 12 The ability to dress declines rapidly in the moderate stage of dementia with clients showing a 25% decline in a 6-month period. 13 Cohen-Mansfield et al found that for nursing home residents with dementia, in 17 out of 20 instances, the staff completely dressed the residents. 14 For bathing (or showering), Mahoney, Trudeau, Penyak, and MacLeod found that individuals with dementia became aggressive toward caregivers and resistive to care. 15 Sloane et al found the aggression rate to be as high as 65% to 86%, posing a threat to health and safety of the client as well as the caregiver. 16 Individuals with dementia have problems with eating and/or feeding such as refusing food, inability to recognize food and utensils, difficulty moving food to mouth, poor chewing and swallowing, and changes in food preferences.17–19 Although there are few studies on grooming with persons with dementia, toothbrushing is included in other ADL studies. 20 Because these ADL tasks are well-learned habits, the performance skills are retained longer than higher level cognitive abilities. 21
Measuring Cognition
The challenge in cognitive evaluation is that standardized screening tools for global cognition do not link to the capacity to perform ADL. The CPT is not an IADL or ADL assessment; the test uses performance-based rating of familiar tasks (filling a medbox, shopping for a belt, selecting clothing, washing hands, following a map, finding information using the phone, making toast) to explain and predict the client’s capacity to perform and to track changes in performance over time. 21 Psychometric properties include test–retest reliability (r = .91), interrater reliability (r = .89), concurrent validity with the MMSE (r = .67), Lawton Scale for IADL (r = .64), and physical self-maintenance (r = .49). 5 The CPT 7-task version has been compared to the 5-task version for concurrent validity using an Altman-Bland comparison method. 22 The bias (−0.01; potential for the score between the 2 versions to increase or decrease) and limits of agreement (−0.3 to 0.27) indicate that the 5-task version can be used in lieu of the 7-task version effectively.
The CPT is based on cognitive disabilities theory that cognitive decline occurs in predictable, definable stages (see Table 1). 23 A client is instructed in a standardized manner to perform the task, while the therapist systematically varies the task cues and working memory requirements to assess severity levels. The score is reduced each time when the client requires additional support in the form of cues or probes to complete the task. There are distracters in each task to challenge the client in planning, problem solving, verbal and procedural memory, abstract versus concrete thinking, spatial orientation, and object use. The score is the summed performance scores on 7 tasks and each task scaled between 5.6 (normal) and 1.0 (severely impaired). For the practitioner, the CPT score, as a measure of global cognition, explains the performance challenges related to cognitive decline and is considered, along with other factors, in anticipating the person’s capacity to perform IADL/ADL and benchmark behaviors (ie, driving, managing finances and medications, living independently, dressing, grooming, and eating). As part of an interdisciplinary team evaluation, an OT performance-based assessment is a contribution to providing best practice intervention for persons with ADRD.
Cognitive Performance Test Scale.
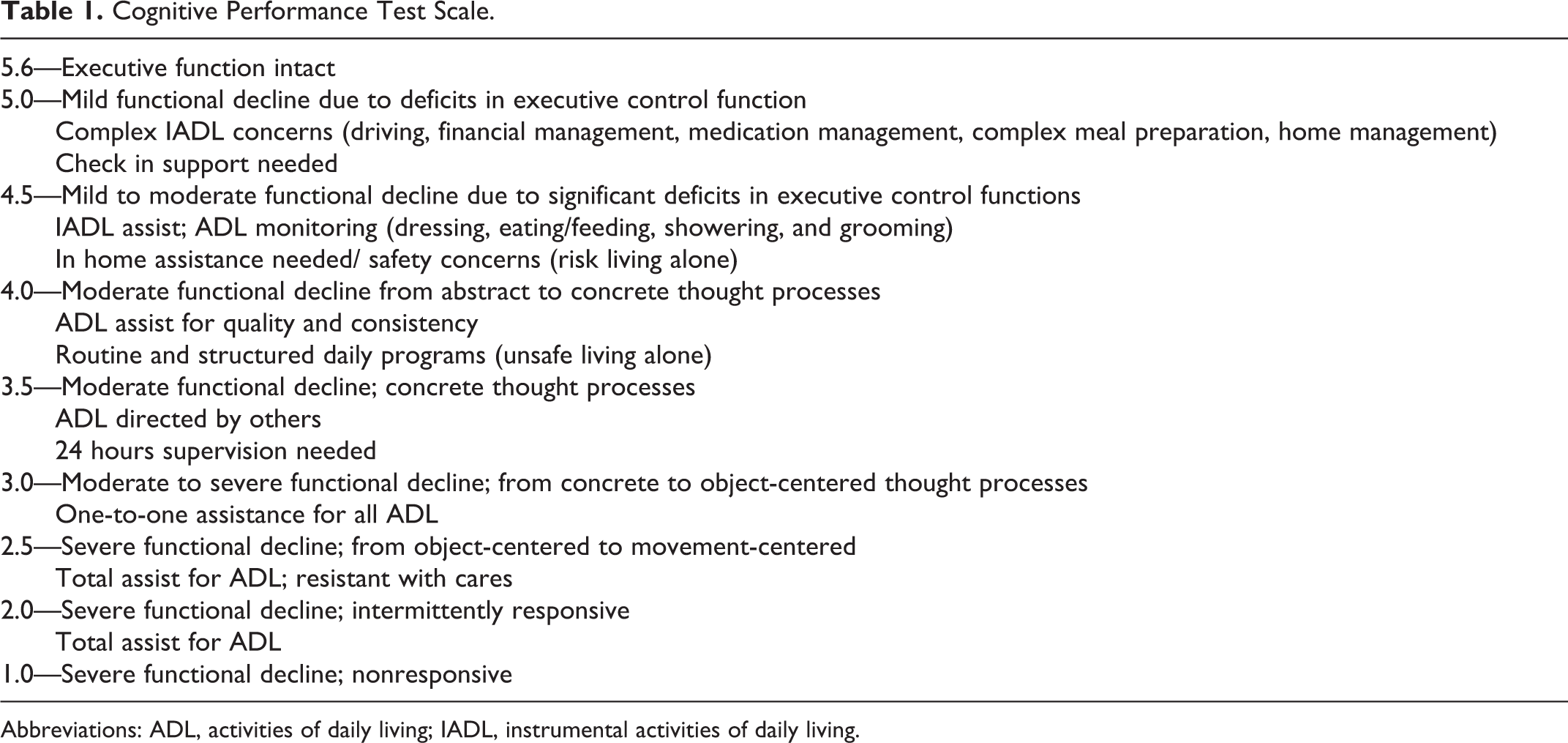
Abbreviations: ADL, activities of daily living; IADL, instrumental activities of daily living.
Measuring Function
The challenge in measuring functional performance via report with a person limited by declining memory and verbal abilities is the potential for inaccurate information. Family member report may be biased or limited by lack of direct observation of skills. Another challenge is that gross indicators, such as normal or impaired, do not pick up the subtle changes over time, characteristic of ADRD, or impact on actual performance skills.
The ADL scale used in this study was the FIM, a standardized outcome measure of functional performance that grades behavior from dependent to independent on a 7-point scale (1 = total assistance to 7 = complete independence). 4 The levels of FIM were operationalized by the type and level of assistance for each ADL (see Table 2). The FIM scale was reviewed by a panel of occupational therapists that specialize in dementia for accuracy and consistency.
Functional Independence Measure for ADL Scale With Operational Definitions.
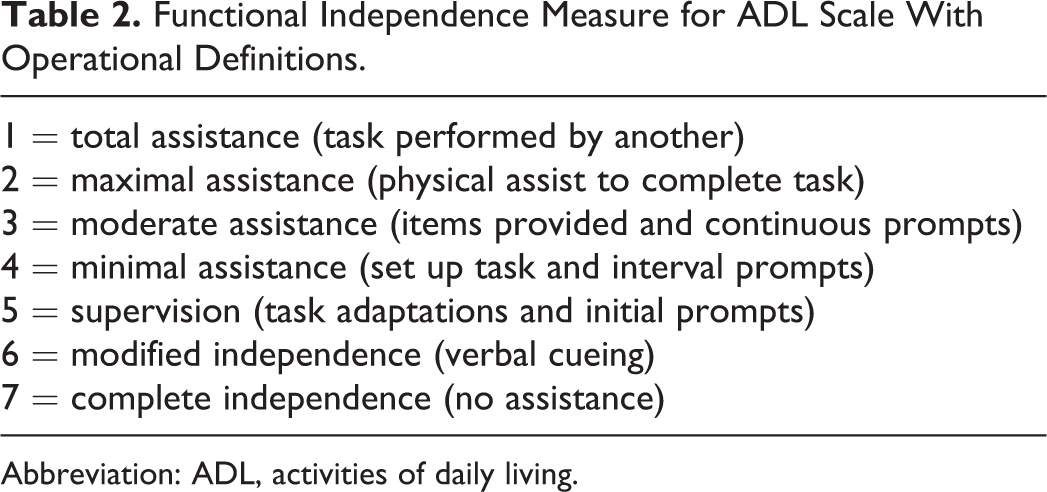
Abbreviation: ADL, activities of daily living.
Method
This study used evaluation results from 57 tenants of a memory care facility in the Midwestern United States who consented to participate by proxy. Memory care tenants had a primary diagnosis of dementia with cognitive decline in the moderate to severe range (mean MMSE = 10.9; standard deviation [SD] = 8.6). The CPT scores of the participants ranged from 4.9 (mild cognitive-functional decline) to 1.4 (severe cognitive-functional decline; mean CPT = 3.46, SD = .88). Tenants with comorbidities aside from the cognitive condition that impacted their ability to perform ADL were excluded from the study.
Sociodemographic profiles showed the participants to be about 85 years old (range 69-95), Caucasian (100%), female (80%; widowed 75%; married 19%; single/divorced 5%), with an average of 3 children and 13 years of education. In all, 55% had a diagnosis of dementia not otherwise specified, 27% Alzheimer’s disease, and 19% other cognitive disorder.
Tenants were administered the CPT (5 of the 7 tasks: medbox, shop, wash, toast, and phone) by a licensed occupational therapist upon admission to memory care-assisted living. The tenants were evaluated for functional performance on 4 ADL: dressing, eating/feeding, showering, and toothbrushing using the operationalized, 7-point FIM scale. A linear regression analysis yielded values to determine the association between each ADL (dependent variable) and CPT scores (independent variable). The values were rounded to the nearest whole or half number and extrapolated to determine the predicted level of functional performance at each level of the CPT scale (5.0, 4.5, 4.0, 3.5, 3.0, 2.5, 2.0, and 1.0; level 5.5 indicates total independence and level 1.0 total dependence).
Results
Linear regression results revealed a significant relationship between ADL performance and CPT scores in all areas (p < .001) for individuals with moderate to severe dementia (see Figures 1 to 4). Toothbrushing showed the strongest model fit (r2 = .624) while dressing had the lowest association (r2 = .514; see Table 3). This indicates that cognition, measured by the CPT, accounted for 62% of the variability in toothbrushing and 51% of the variability in dressing (55% for showering and 54% for feeding). Based on the regression equation, the CPT scores predicted the functional performance of the residents at each cognitive level. Functional performance ranged from 1 (total assistance) to 7 (no assistance). Table 4 displays the predicted functional performance of a memory care resident at each CPT level.
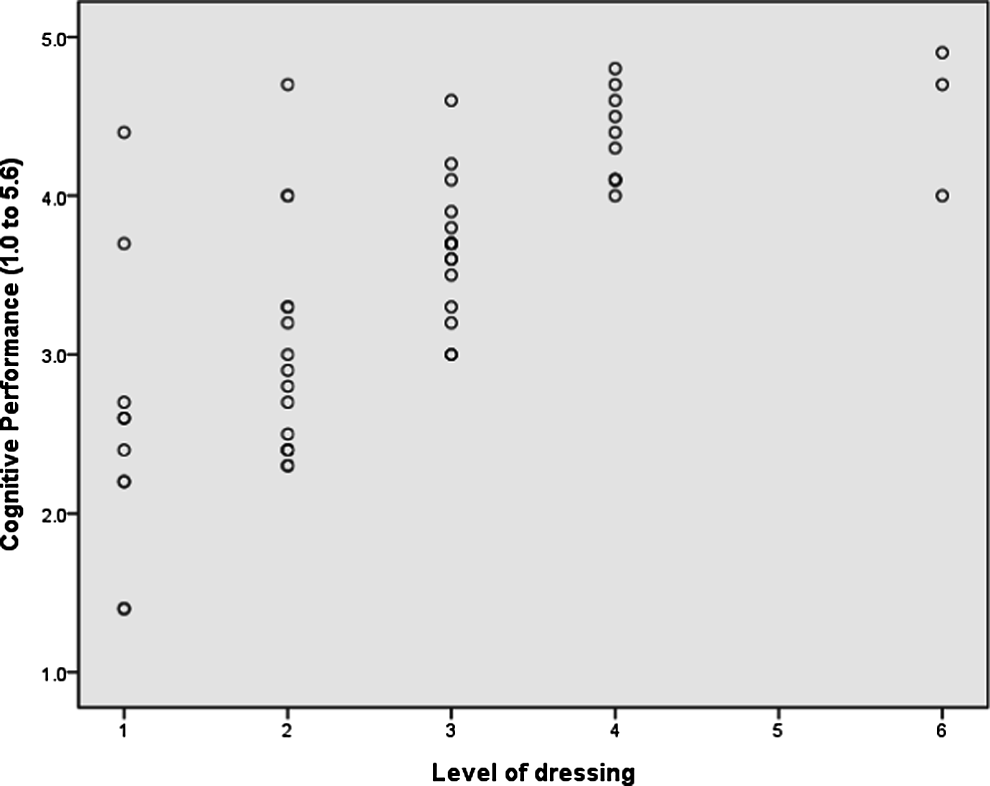
Scatterplot of Cognitive Performance Test scores and dressing.
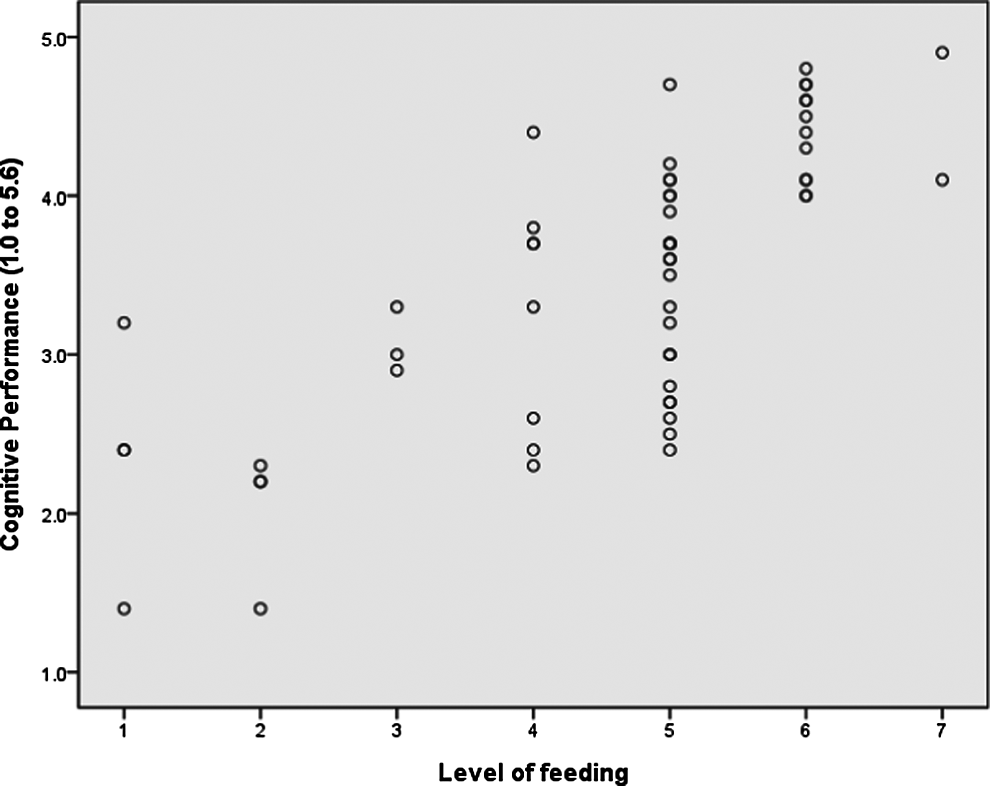
Scatterplot of Cognitive Performance Test scores and feeding.
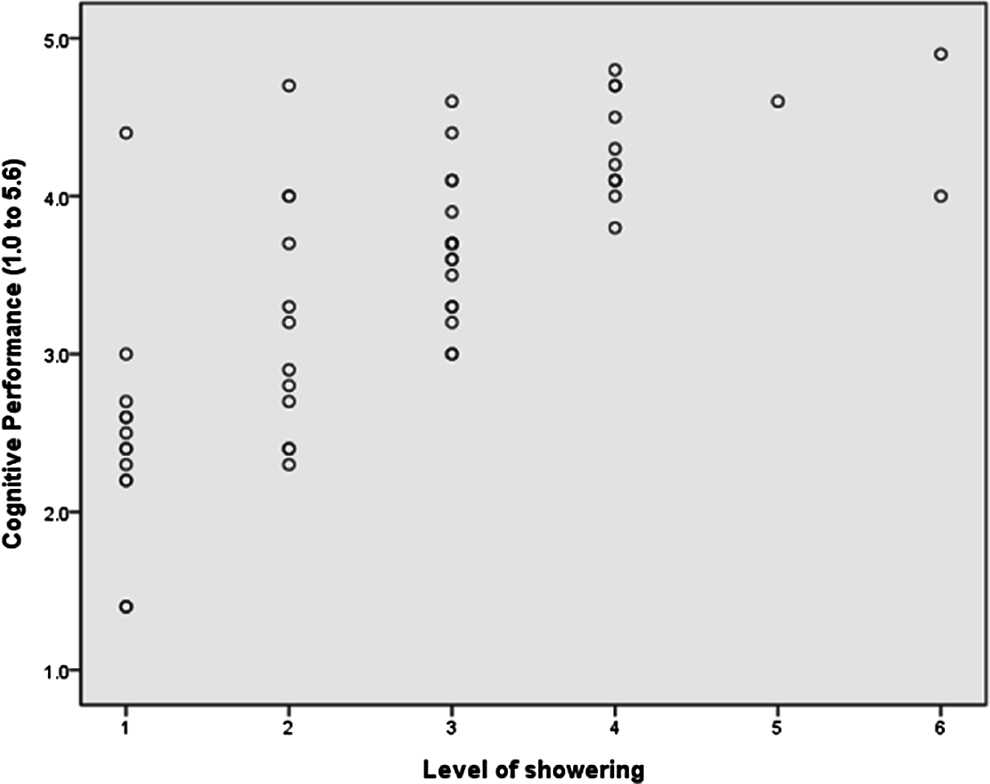
Scatterplot of Cognitive Performance Test scores and showering.
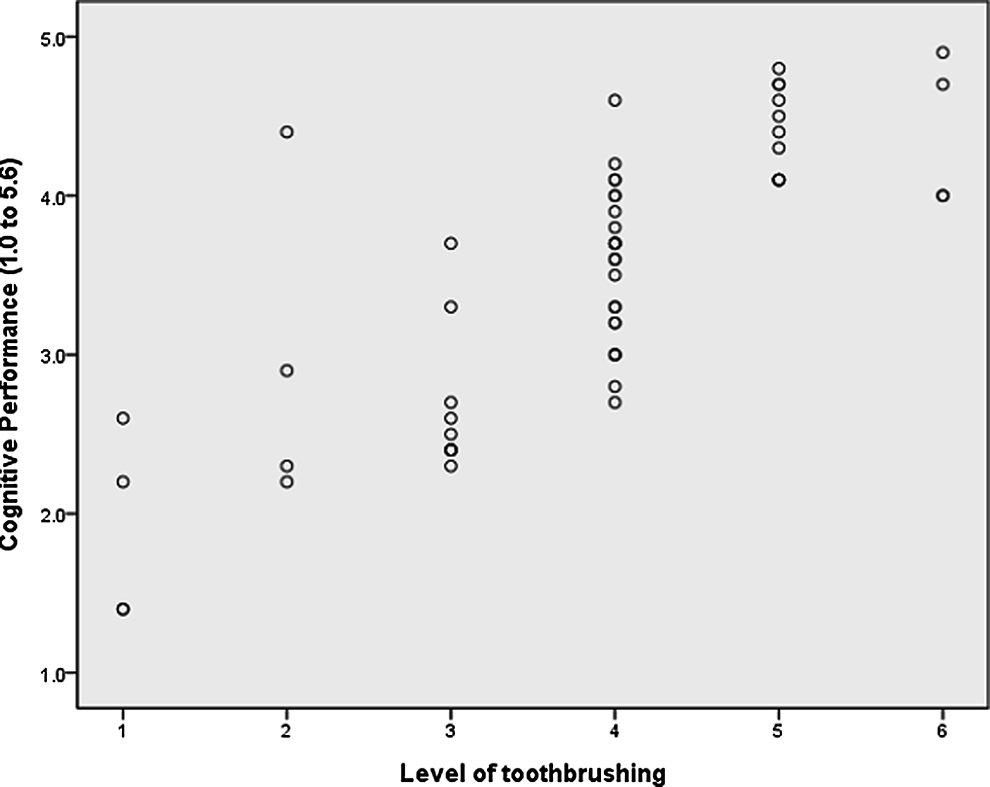
Scatterplot of Cognitive Performance Test scores and toothbrushing.
Summary of Linear Regression Analysis for Variables Predicting ADL.
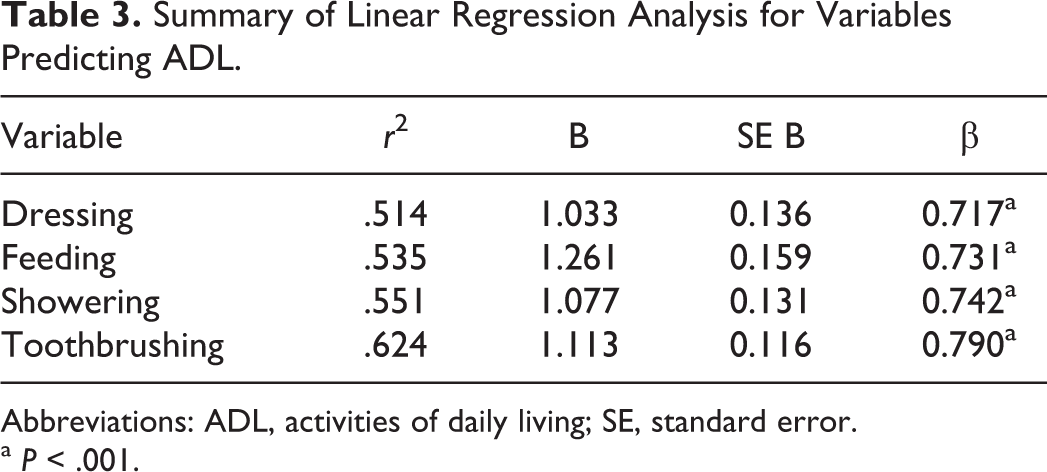
Abbreviations: ADL, activities of daily living; SE, standard error.
a P < .001.
Predicted ADL Performance at CPT Levels for Memory Care Residents.
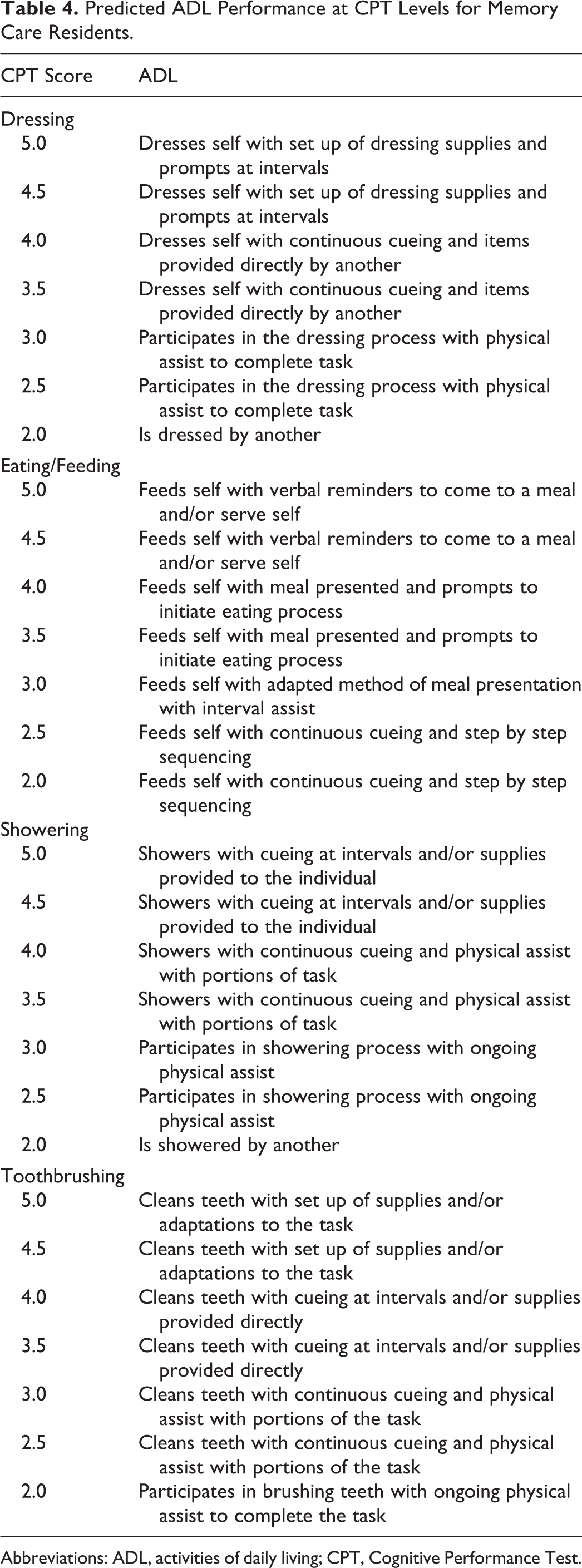
Abbreviations: ADL, activities of daily living; CPT, Cognitive Performance Test.
Results indicate that, of the 4 ADL studied, at each cognitive level, dressing and showering skills appear to require a higher level of assistance while eating/feeding and toothbrushing require less assistance. Physical assistance is required for showering (CPT level 4.0), dressing, and toothbrushing (CPT level 3.0); physical assistance is not a standard requirement for eating/feeding, even at CPT level 2.0 with sequencing of food and continuous cueing.
Discussion
This study supports the use of a cognitive-functional assessment to predict expected levels of functional performance in ADL for persons with moderate or severe dementia entering memory care facilities. The desired outcome of residential placement is achieving the balance of optimal task performance of the individual with facility-provided support when needed. A score that predicts key ADL performance may impact decisions around placement and staffing to provide adequate supports resulting in decreased stress for tenants and family members.
Another advantage to a more accurate prediction of performance is that the effects of institutionalization may be the barrier to engagement. Facility staff may find efficiency in providing total physical assistance when only set up and cueing are needed. Increasing staff expectations for task performance may impact the actual performance; further study on reasons why the ability to dress declines rapidly in the moderate state of dementia along with approaches to counter the decline are needed. 13 The dilemma of balancing time demands in providing efficient care against tenant’s autonomy in performing ADL is not a trite issue. It is one that influences self-esteem and quality of life on a daily basis.
Using a cognitive-functional measure as a starting point to plan care has potential utility in family education and caregiver training to tailor expectations, either lower or higher, around the performance. The study results highlight the significant role cognition plays in ADL performance with this population. Cognition, as measured by the CPT, was shown to account for the variability in performance from 51% to 62% based on the r2 values. Relative to standardized testing, these r2 values are considered high for 1 test; to obtain higher r2 values, other factors could be considered to explain the remaining variability of ADL performance of a specific activity. Cognition is a primary factor, albeit, not the only factor impacting performance. For example, if the tenant, scoring a CPT level 4.5 (indicating ability to dress self with set up of dressing supplies and prompts at intervals), is being dressed by another, other barriers to performance need to be considered. Orthopedic conditions, arthritis, diabetes, poor endurance, cardiac and neurological conditions, and depression are examples of comorbidities which affect a person’s ability to complete a dressing task. Ruling out and/or mediating these factors, a reasonable goal would be for the individual to dress self with set up of dressing supplies and prompts at intervals. On the contrary, a tenant scoring 3.0 at CPT with the expectation to dress self with set up and prompts may experience frustration and failure; based on the cognitive capacity, the tenant may require physical assistance to complete the task.
This study provides information about the relationship of the CPT score to specific ADL, information not provided by a global cognitive screening tool. Based on the study results, feeding and toothbrushing required less assistance than dressing or showering. This supports the study by Amella which found an individual’s ability to self-feed remains intact longer than performance of other ADLs. 17 Toothbrushing was also pursued with less assistance at different levels of cognitive decline. A study by Wattmo, Wallin, Londos, and Minthon identified grooming and bathing as the ADL with greatest decline while feeding and toileting had least decline. 24 Showering, as the ADL with the highest need for physical assistance at different cognitive levels, is consistent with the results of Sloan et al associating aggression, agitation, and discomfort with this task. 16 Understanding specific activity demands for each ADL is useful for guiding memory care personnel in planning for tenant's assistance needs and setting expectations that are within the cognitive capacity of the individual.
Limitations of this study include the need for a larger, more varied sample with participants represented across the spectrum of cognitive decline. The sample was a convenience sample, 100% Caucasian and an average of 13 years of education which exceeds typical groups of an older adult cohort. This study cannot be generalized to other institutionalized residents because of the unique structure of memory care or individuals with mild cognitive decline or mild dementia. Even with these limitations, this study can serve as a starting point in the development of intake protocols designed to link cognitive-functional performance to appropriate setting and service needs.
The challenge is to develop valid and reliable measures that gauge cognitive changes over time, and to translate the results into knowledge that has utility for the health care team. The question “What does the score mean?” once interpreted in a disciplinary context needs to be translated into useful information to serve the professionals and family members, providing prediction about anticipated level of occupational performance and in readjusting performance expectations.
The CPT can be administered in conjunction with or subsequent to an OT evaluation for persons with ADRD and reimbursed through Medicare and private insurance. Administration and interpretation of the CPT, a specialty area of OT practice, requires training and experience with clients with dementia. The OT intervention for ADRD in memory care is dynamic, episodic, and client-centered and parallels changes in cognition of the person over time. 25 With skilled services and accurate information, residential care coordinators can plan and manage daily life effectively and successfully, minimizing the deleterious effects of the disease and optimizing occupational performance throughout the course of the disease. These results may guide placement and care planning for persons entering or residing in memory care facilities to anticipate care needs and to promote greater engagement in daily activities.
Footnotes
Acknowledgments
The authors would like to thank Emerald Crest Assisted Living, a memory care residential facility located in Minnesota, for collaborating on this research project and for their support of research in occupational therapy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.