
Abstract
Background:
Recently, interest in nonpharmaceutical interventions in dementia care has increased. Animal-assisted therapy has been shown to be one promising intervention but more knowledge is needed. The present article reports on a pilot study involving an 84-year-old woman with vascular dementia who was systematically trained with a therapy dog team for 8 weeks.
Methods:
A quasi-experimental longitudinal interventional design with pre-post measures was used. Data were collected on 3 occasions. Descriptive statistics were used for data analysis.
Results:
Some effects on the woman’s ability to walk and move were identified. In addition, some effects in the woman’s cognitive state were observed.
Conclusions:
Physical, psychological, and/or social training with certified therapy dog teams can have effects on behavioral and psychological symptoms in people living with dementia. Further research is needed.
Introduction
Different dementia diagnoses have different symptoms, but all types of dementia involve behavioral and/or psychological symptoms (behavioral and psychological symptoms of dementia [BPSD]). 1 Behavioral and psychological symptoms of dementia include behaviors such as screaming, wandering, aggression, and also psychiatric manifestations such as depression or psychosis. 2, 3 All types of dementia disease lead to deteriorated performance of daily activities such as dressing or eating. 4 As a result, living with dementia leads to suffering for the people with dementia, their families, and for professional caregivers.
In order to alleviate suffering and to reduce symptoms, pharmaceutical interventions are used. However, for persons with dementia, side-effects from medication can diminish the quality of life. The importance of identifying alternatives or complements to pharmaceutical treatment, thus, is increasingly emphasized. In addition, scientific support and evidence for nonpharmaceutical interventions is increasing. 5 One important justification for nonpharmaceutical interventions is the poor safety profile of antipsychotics in cases of dementia. The aims of nonpharmaceutical interventions are to improve the quality of life for people with dementia and to maintain their remaining abilities as much as possible. Nonpharmaceutical interventions are not limited to specific types of dementia. No serious side effects from nonpharmaceutical treatments in dementia have been reported. It is, however, a challenge to identify nonpharmaceutical interventions that minimize or alleviate BPSD. Examples of nonpharmaceutical interventions are physical training, 4, 6 music therapeutic caregiving, 7 music therapy 8 or animal-assisted therapy (AAT). 9, 10 Animal-assisted therapy programs exist in the United States, Canada, India, Japan, Korea, Mexico, Sweden, and elsewhere. 11
Animal-Assisted Therapy
Animal-assisted therapy has been defined in a variety of ways: resident dogs, assisted animal interventions, animal visitation, pet therapy, and so on, 12 which also reflects a diversity of practices. However, AAT is usually described as the interaction between a client and a trained animal, facilitated by a human handler, with a therapeutic target such as relaxation or pleasure. 13 Fine 14 proposes defining AAT as “a goal-oriented intervention in which an animal meeting specific criteria is an integral part of the treatment process. This service is delivered by a health or human service professional working within the scope of his or her professional role.” It is believed that the efficacy of AAT involves a positive emotional response by the client to the animal.
Animal-Assisted Therapy in Dementia Care
When used in dementia care, AAT takes advantage of the human–animal bond to reduce behavioral and/or psychological symptoms and to increase social engagement and communication. The purpose is to reduce symptoms of BPSD and/or to train daily activities or functions (Table 1). In AAT, dogs are used commonly. 11, 12 The training is always tailored in accordance to the needs of the person with dementia.
Examples of Capabilities and Features That can be Trained With a Certified Therapy Dog Memory
A review of the literature suggests that AAT can be beneficial in cases of dementia. Animal-assisted therapy can decrease agitated behaviors and increase social interaction. 10, 13 The presence of a dog in nursing homes reduces aggression and agitation among people with dementia. 13 They smile and laugh more when a dog visits or lives among them. 13 Other social behaviors that are significantly more displayed are looks, leans, and touches. 13 Dog-visitation therapy can reduce the incidence of yelling and screaming and reduces the heart rate as well. 12
To sum up, AAT with dogs seems to be well suited for persons with dementia because the dog provides companionship regardless of the person’s cognitive function, and the dog listens without judgment. 15 Despite studies suggesting AAT as a valuable tool in dementia care, scientific knowledge about the effects is limited, bringing several questions to mind: Does AAT affect BPSD? What are the effects of AAT on the activities of daily living (ADLs)? Is cognitive ability in dementia affected by AAT? What is the impact of AAT concerning quality of life for people with dementia?
In Sweden, AAT usually involves systematic training with a certified therapy dog and a dog handler (DH). With the aid of the therapy dog team, different functions such as balance, walking ability, and much more are trained (Table 1). The therapy dogs are selected and systematically trained to work in a variety of health care settings, for example in the care of people with dementia. Hence, a therapy dog is a kind of assistance dog.
The dog and the DH form a “therapy dog team.” The therapy dog team is trained for about 40 hours with an instructor. In addition, the therapy dog team is trained clinically for approximately 200 hours (6-12 months) in different environments. The breed is not important for the dog’s suitability. Instead, the dog's personality is crucial. Since AAT is provided on prescription, licensed health care professionals (eg, registered nurses, occupational therapists [OTs], and/or physiotherapists) are also educated.
However, in spite of promising results, some criticism against previous research has been raised. The criticism concerns matters such as small sample sizes, lack of randomization, and either inappropriate or no control groups. 15, 16 Therefore, before AAT can be accepted as a valid treatment in dementia care, more evidence-based research is needed.
This article reports on a pilot study conducted in 2011 in Sweden. The purpose for the present single-case study was to gain detailed descriptions of possible effects of AAT in 1 case of dementia. The aim of the pilot study was to investigate the effects of AAT on pharmaceutical treatment; behavioral and psychiatric symptoms; ADLs; cognition and orientation; quality of life; pain and fall risk.
Methods
The pilot study was undertaken as a quasi-experimental longitudinal intervention study in a municipal nursing home in the middle part of Sweden. The nursing home comprises a total of 12 care units (129 apartments). Each resident has 1 or 2 contact personnel (primarily enrolled nurses) that in collaboration with other staff (registered nurses, OTs, and/or physiotherapists) are accountable for providing help and care according to the residents’ needs.
Indications for AAT were increasing anxiety, regression (the person is an introvert and does not participate in activities or social relations), communication problems leading to loss of or reduced ability to engage in social relations, reduced physical capabilities, or unwillingness to train otherwise, low mood, behavioral, and/or psychological symptoms.
Inclusion criteria—fulfilling one or more indications for AAT, diagnosed with dementia, living at the nursing home for more than 4 weeks prior to the intervention, not allergic to dogs. Exclusion criteria—known to have expressed anxiety toward dogs earlier in life or otherwise not considered by staff as appropriate for AAT (for instance being very aggressive or getting upset when meeting the dog).
Study Design
A pre-post study with follow-up measurement was used. Measurements were performed before the intervention (prestudy) and immediately after intervention (poststudy). The intervention lasted for 8 weeks. Follow-up was performed 3 months after the intervention was ended.
The Participant
The present case report involved Mrs Johnson (fictitious name) aged 84. She was a widow and had 1 daughter and 1 grandchild. Mrs Johnson used to work as a clothing retailer. Mrs Johnson was known to enjoy nature and animals and was active and goes for regular walks.
In 2007, Mrs Johnson was diagnosed with cancer in the tongue base. After surgery, she moved to a short-term nursing home. She then lived in 3 different nursing homes. Eventually, in 2010, she moved to the current nursing home. Mrs Johnson’s medical history also included atrial fibrillation, collapsed vertebra, and osteoporosis. In addition, Mrs Johnson’s body weight was low. Other limiting symptoms were chest pain and back pain. During Fall 2010, Mrs Johnson had swallowing problems which were believed to be caused by a cancer relapse. However, she was cleared. During 2011, the cancer relapsed and was not treatable.
According to her medical records, Mrs Johnson was diagnosed of vascular dementia, after surgery in 2007. The diagnosis was obtained through computed tomography (CT) and Mini-Mental State Examination (MMSE).
Recently, Mrs Johnson had started to wander and seemed to be upset and angry with staff or fellow patients. She did not get on with 1 new resident in particular. Nursing staff tried to calm Mrs Johnson through outdoor activities and other actions, with no obvious results.
Prescription of AAT
The need for AAT was first discussed at a meeting between staff nurses, registered nurses, and the branch manager of the nursing home. Under the circumstances Mrs Johnson was assessed to be in urgent need of AAT, she was therefore prioritized before other residents. Grooming and walking the dog seemed to be a possible way to make Mrs Johnson feel appreciated and needed. The aim was to reduce Mrs Johnson’s psychological symptoms.
In accordance with the nursing home’s guidelines, AAT was prescribed by an OT. Mrs Johnson was prescribed AAT once a week for 8 weeks. Every session lasted for approximately 60 minutes and was evaluated and documented in the care plan. The total time of observation was 5 months (April 2011-September 2011).
Intervention
The therapy dog team consisted of a 4-year-old flat-coated retriever and its handler who was an experienced enrolled nurse. The AAT involved grooming and walking the dog. The goals for the AAT included Mrs Johnson to spend time with the therapy dog, to walk, and to groom the dog. Every session included outdoor walking.
At every session, the dog stood next to Mrs Johnson, leaning against her legs, while she stroked him. She would tell the dog he was very handsome and then say to the DH “I think he recognizes me. I say, he is very handsome and clever as well!” She would also tell anyone near about the dog and how handsome and beautiful he was.
At most sessions, Mrs Johnson brushed the dog and gave him treats or water. She spoke to the DH about the dog’s fur, if it was wet, soft, warm, and so on. She also talked about the hard work of being an animal owner. Mrs Johnson told the DH she once owned dogs and horses. Indeed, Mrs Johnson earlier competed in horse dressage. She also told the DH she was no longer able to have a dog on her own since she was very old and was no longer able to exercise a dog.
The DH's task was to acknowledge Mrs Johnson. Hence, she said things like “Yes, you are right about [whatever Mrs Johnson told].” When the dog sat in front of Mrs Johnson who stroked his fur, the DH talked to Mrs Johnson about the dog “Look, can you see that he closes his eyes when you touch his cheek? That is because he likes your touch, he enjoys it, and he is feeling good right now!” When the dog made eye contact with Mrs Johnson the DH said “What do you think he is trying to tell you by looking into your eyes?” At that point Mrs Johnson would stroke the dog or give him treats, water, or similar. Sometimes the DH and Mrs Johnson enjoyed just sitting down together, watching the dog quietly. Often they held hands and frequently Mrs Johnson hugged the DH spontaneously. Sometimes Mrs Johnson picked flowers to give to the DH when they went back to the nursing home.
Care Plan Documentation
The systematic training was evaluated and documented by the OT and the DH 3 times during intervention: weeks 1, 4 and 6.
Week 1 (OT): . . . the training works very well. Mrs Johnson is laughing and joking; she pets the dog and tosses balls. She also brings the dog water. Today, I photographed Mrs Johnson and the dog. Later, I will bring her a photo album.
Week 4 (DH): Mrs Johnson joined me and the dog for a walk. She took the opportunity to pick some flowers along the way. We talked a lot about the flowers, their scent, and colors. “Isn’t my bunch lovely?” Mrs Johnson said. I answered “It looks like a bridal bouquet; all you lack is a man!” “Yes . . . ” Mrs Johnson answered, and in the next moment she said “I guess I can choose that fury one!” She pointed at the dog and laughed.
Week 4 (OT):Today, I brought Mrs Johnson a photo album with photos picturing her with the dog. She was very happy about the pictures.
Week 6 (DH): Mrs Johnson and I went for a walk with the dog. She picked a bunch of flowers. We talked about the flowers, about their beauty, and their scent. Mrs Johnson talked to people we met and asked a gentleman whether he found her flowers beautiful. She was very chatty and happy during the whole walk.
Data Collection
Data were collected on 3 occasions: (1) 1 week prior to AAT (baseline), (2) when AAT was completed, and (3) 3 months later. Data collection was conducted by a project assistant who was a registered nurse, 1 project assistant who was an OT and by Mrs Johnsson's contact person who was an enrolled nurse with good knowledge of Mrs Johnson. At baseline, the contact person completed the questionnaire together with one of the project assistants. Later, the contact person completed the questionnaires herself.
Background data (diagnosis, time at the nursing home and pharmacological treatment) were collected from medical records. The level of cognitive impairment was determined by the MMSE. Five instruments were used for the evaluation of the effects of AAT: Cohen Mansfield Agitation Inventory (CMAI), Multi-Dimensional Dementia Assessment scale (MDDAS), MMSE, ADL taxonomy, and Quality of Life in Late-stage Dementia scale (QUALID). The selection of instruments are widely in use, with validated versions available in Swedish, and easy to complete.
The CMAI is a caregiver questionnaire to assess elderly persons’ agitated or not agitated status. It was originally developed for research purposes in nursing homes 17 but is also used for clinical purposes by caregivers. The CMAI is also used to assess the impact of pharmacological or nonpharmaceutical interventions. The scale consists of 29 behaviors. Each item is rated on a 7-point frequency scale ranging from “never” (= 1) to “several times an hour” (= 7). Low scores indicate no agitated status. The CMAI has been validated with Cronbach α of 0.63 to 0.82. The behaviors are divided into 3 groups: physical aggressive behaviors (11 items; range 11-77); physical nonaggressive behaviors (10 items; range 10-70), and verbal agitation (8 items; range 8-56). Each item is based on an average frequency of occurrence over the last 2 weeks.
The MDDAS was originally designed in Swedish and has been used in several studies. 18 -20 The MDDAS has good inter- and intrarater reliability. 18 The MDDAS is designed to be answered by staff based on observations of the resident. The scale includes subscales concerning functioning in ADLs, behavioral symptoms (such as wandering, undressing in the lunch room, packing stuff), psychological symptoms (such as aggressive behavior, restless, passiveness), and cognition. The ADL subscore is calculated on the person’s ability to manage hygiene, dressing, eating, and bladder and bowel control. All categories are scored using scale of 1 to 5, except for bladder control which is scored between 0 and 4. Total scores range from 4 to 24. A higher ADL score indicates greater independence. The 25 behavioral symptoms (total score ranging from 0 to 75) and the 14 psychological symptoms (total score range from 0 to 42) are rated on a 3-point scale (3 = daily, 1 = some times per week, and 0 = never). Higher scores indicate more symptoms. Cognition is measured on a subscale of MDDAS. 21 It was designed to be answered by staff based on observations of the resident. The scale comprises 27 items measuring the persons’ orientation ability. A score of less than 24 is considered to indicate cognitive impairment. In addition to the MDDAS, separate questions concerning pain and fall risk were included. 19, 20 The caregiver rates the resident’s pain (from no pain [0] to worst thinkable pain [100]) and fall risk (from low risk [0] to high risk [100]) on a 100-mm Visual Analogous Scale (VAS).
The ADL taxonomy is used for different purposes in clinical work at individual level. In Sweden, the ADL taxonomy is an accepted way to describe capacity of activities in daily life. The ADL taxonomy covers 12 activities: eating and drinking, mobility, going to the toilet, dressing, personal hygiene, grooming, communication, cooking, transportation, shopping, cleaning, and washing. 22 Evaluation is made either through interviews or through observations. The results are then placed in a circle or in a form. When OTs use the circle, they are free to choose what information to code and how to code it. Because data are collected at ordinal level, numbers are not recommended for assessment. 23 In the present study, the ADL taxonomy circle was used to record what the persons with dementia “could do” on a 5-graded scale. Color coding was used.
The MMSE is a brief structured test to assess cognitive impairment. The test was originally developed for assessing cognitive impairment among psychiatric patients. 24 Currently, MMSE is primarily used in relation to dementia and can also be used to follow a person's cognitive development over time. The test is carried out by an interviewer who asks the person with dementia to answer a number of questions, refer to subjects and draw a shape. The test takes approximately 10 to 15 minutes and should be performed by a trained person. The results are interpreted as points (max 30) to express the degree of dementia: normal >25 points; mild impairment 25-20 points; moderate impairment 19-10 points; severe impairment 9-0 score. Reliability and construct validity have been judged to be satisfactory. 24, 25
The QUALID is a late-stage dementia-specific questionnaire with a 1-week recall period. 26 The Swedish version has been validated. 27 Assessments are made by staff. The Swedish version of QUALID has shown a satisfactory level of internal consistency and inter-rater reliability. It has also shown good criterion validity. 27 The scale measures 11 observable behaviors including both positive and negative dimensions of observable activity and emotional states. The items are rated on a 5-point Likert-type scale and total scores range from 11 to 55, with 11 representing best quality of life.
Ethical Considerations
The study was approved by The Regional Board of Research Ethics in Uppsala, Sweden. Since Mrs Johnson had dementia, proxy consent was obtained from her next of kin who were informed both orally and in writing about the study. The information included the aim of the pilot project, that participation in the study was voluntary, and that they could withdraw at any time without experiencing any loss of care. During AAT the DH carefully observed Mrs Johnson for any signs that indicated that she objected to participating in the study.
Results
Pharmaceutical Treatment
At baseline, Mrs Johnson was treated with aspirin (160 mg ×1) and lactulose once a day. During the training period, no changes were made to Mrs Johnson’s pharmaceutical treatment. Occasionally, when upset, she was treated with extra oxazepam (5 mg). However, at 3 months’ follow-up, she was treated with aspirin (160 mg 1 × 1), paracetamol (500 mg 2 × 2), oxazepam (5 mg 1 × 1), memantine (20 mg 1 × 1), and fentanyl patches.
Behavioral and Psychiatric Symptoms
Behavioral symptoms (CMAI)
According to the CMAI manual, Mrs Johnson did not fulfill the criteria for agitated status during the observational period. Yet, some changes were noticed. Total score at baseline, after AAT, and at follow-up was 36, 35, and 36, respectively (see Figure 1).
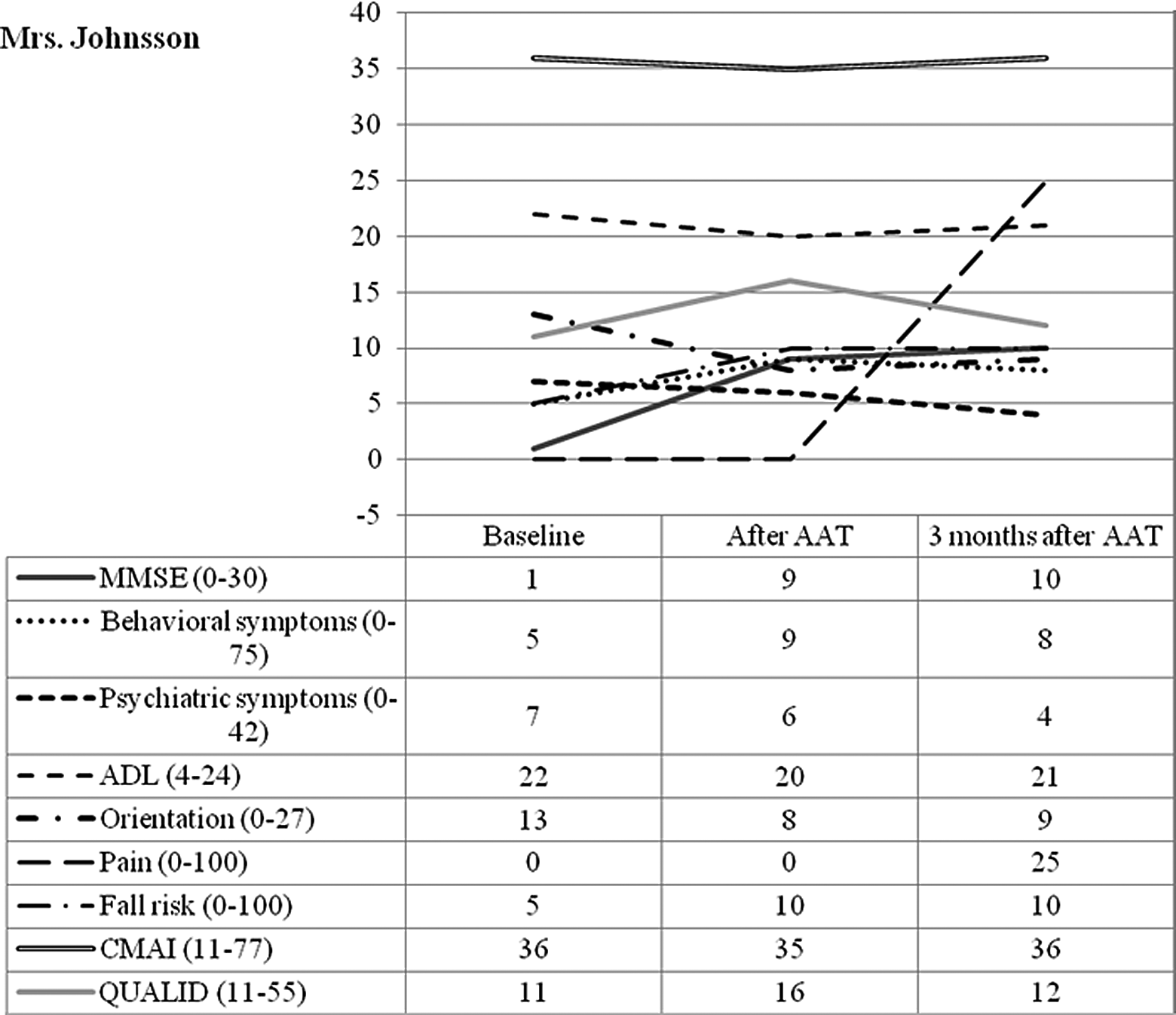
Illustration of results.
Physically aggressive behaviors: immediately after AAT, a new behavior was observed, that is Mrs Johnson was grabbing on to people. At 3 months of follow-up, grabbing was not observed.
Verbally agitated behaviors: at baseline, Mrs Johnson expressed repetitious sentences/questions several times a day. The behavior vanished immediately after AAT and at 3 months of follow-up. In addition, at 3 months of follow-up, Mrs Johnson was observed cursing, although less than once a week.
Physically nonaggressive behaviors: No changes.
Behavioral symptoms (MDDAS)
During the observational period, Mrs Johnson exhibited a low frequency of behavioral symptoms. However, some changes were observed. Total score at baseline, after AAT, and at follow-up was 5, 9, and 8, respectively (see Figure 1).
Resistance: at baseline Mrs Johnson resisted being dressed or undressed at least once a week. However, immediately after AAT the resistance increased to every day. Then again, at three months follow-up resistance was exhibited no less than once a week.
Attention seeking: immediately after AAT and at 3 months of follow-up Mrs Johnson sought attention from staff at least once a week, which she previously never used to.
Nighttime sleep: at 3 months of follow-up, Mrs Johnson’s nighttime sleep was interrupted at least once a week.
Wandering: at 3 months of follow-up, Mrs Johnson had started to wander back and forth alone or with other patients at least once a week.
Psychological symptoms (MDDAS)
Mrs Johnson manifested a low frequency of psychological symptoms. Total score at baseline, after AAT, and at follow up was 7, 6, 4, respectively (see Figure 1). Nevertheless, some changes were observed.
Ability to cooperate: At baseline, Mrs Johnson never cooperated with staff. However, immediately after AAT she cooperated at least once a week. At 3 months’ follow-up, she cooperated every day with staff.
Initiatives: Mrs Johnson’s exhibited capability of taking initiatives at least once a week immediately after AAT, while never at baseline or at 3 months’ follow-up.
Being suspicious: At baseline and immediately after AAT, Mrs Johnson was observed being suspicious at least once a week. However, at 3 months’ follow-up, this symptom was never observed.
Help-seeking: At baseline and immediately after AAT, Mrs Johnson was observed seeking help at least once a week. However, at 3 months’ follow-up, this symptom was never observed.
Distortion: At baseline, Mrs Johnson manifested distortion every day. Immediately after AAT, distortion was manifested not less than every week, although not every single day. Then again, at 3 months’ follow-up, distortion was not observed at all.
Restlessness: At baseline, Mrs Johnson displayed restlessness every day. Immediately after AAT, restlessness was displayed not less than every week, although not every single day. Then again, at 3 months’ follow-up, restlessness was not observed at all.
Activities of Daily Living
Taxonomy of ADLs
Movement: At baseline and immediately after AAT, Mrs Johnson needed assistance when moving between floors, walking into or out of the house, or when moving in the close external environment. However, at 3 months’ follow-up, she was able to move around on her own. Indeed, immediately after AAT, Mrs Johnson’s ability to move between rooms had improved from needing assistance to being able to move around on her own.
Communication: At baseline and immediately after AAT, Mrs Johnson did not need any kind of assistance to converse with other people. But at 3 months’ follow-up, she had to be encouraged to converse with other people.
Eating and/or drinking: At baseline, Mrs Johnson managed eating and drinking herself. However, at 3 months’ follow-up, she needed concrete help.
Grooming: At baseline and immediately after AAT, Mrs Johnson was able to comb her hair fully on her own. However, at 3 months’ follow-up, she needed encouragement in order to comb her hair.
Activities of daily living (MDDAS)
Mrs Johnson’s ADL scores during the observation period indicated only slight impairment. Total score at baseline, after AAT, and at follow up was 22, 20, and 21, respectively (see Figure 1).
Dressing: At baseline, Mrs Johnson was able to dress herself on her own initiative. Immediately after AAT and at 3 months’ follow-up she needed certain help.
Hygienic procedures: At baseline and immediately after AAT, Mrs Johnson required some help with her hygienic procedures. Conversely, at 3 months of follow-up, she accomplished her hygienic procedures after encouragement from staff.
Effects on Cognition and Orientation
Mini-Mental State Examination
Total MMSE score at baseline, after AAT, at 3 months’, and 6 months’ follow up was 1, 9, 10, and 7, respectively (see Figure 1). Thus, Mrs Johnson had severe dementia. At baseline, Mrs Johnson refused to cooperate with the project interviewer as with staff in general, and she would only answer one question in the MMSE (score 1). However, immediately after AAT she willingly cooperated and scored 9. At 3 months’ follow-up, Mrs Johnson’s willingness to cooperate remained, scoring 10 on the MMSE scale.
Orientation (MDDAS)
Mrs Johnson’s orientation scores during the observation period indicated moderate impairment. Total score at baseline, after AAT, and at follow-up was 13, 8, and 9, respectively (see Figure 1). Some changes were observed.
At baseline, Mrs Johnson was able to account for her own age; she knew in which town the nursing home was situated; she could distinguish between staff and patients; and she also understood when there were visitors. Immediately after AAT and at 3 months’ follow-up Mrs Johnson was no longer able to do any of that. In addition, at baseline and immediately after AAT, she knew her own birthday, which she did not know at 3 months’ follow-up.
Quality of Life (QUALID)
Even though Mrs Johnson was considered to have a good quality of life during all of the observational period, some changes were noted. Total score at baseline, after AAT, and at follow up was 11, 16, and 12, respectively (see Figure 1).
Immediately after AAT, Mrs Johnson exhibited facial expressions of discomfort, albeit, less than once a day. In addition, immediately after AAT, Mrs Johnson stopped enjoying touching or being touched. She also seemed to stop enjoying interacting with other people. At 3 months’ follow-up, none of these changes were present.
Pain and Fall Risk
Pain (MDDAS subscale)
Total score at baseline, after AAT, and at follow up was 0, 0, and 25, respectively (see Figure 1). At the end of the observational period, Mrs Johnson (according to the medical records) was affected by a facial tumor that was causing her pain.
Fall risk (MDDAS subscale)
Total score at baseline, after AAT, and at follow-up was 5, 10, and 10, respectively (see Figure 1). The change may be due to Mrs Johnson starting to walk on her own after AAT and she also started to wander back and forth.
Discussion
Previous studies show positive effects of AAT in dementia care. 10, 13, 15 However, to our knowledge no previous studies have studied the effects of systematic training with therapy dogs in detail or for a longer period of time. Therefore, the present study provides novel insights about the effects of systematic training with a certified therapy dog.
Concerning Mrs Johnson, no major changes where observed in her behavioral and/or psychological symptoms. Nevertheless, when results are summarized some of the observed changes can be assumed to be connected with the AAT. First, according to the ADL taxonomy there were effects on Mrs Johnson’s ability to walk and move around. Her improved walking ability persisted at the 3-month follow-up, indicating that physical training can improve or sustain physical capacity in people with dementia. Yet, no certain conclusions can be drawn since the present study was only a pilot study. There are no previous studies about ADL and AAT, and this has been largely unexplored in the literature which illustrates the importance of further research. However, the notion of being able to walk on one's own is presumed to promote integrity and autonomy.
In addition, effects on the MMSE were observed. Before AAT, MMSE was not possible to conduct since Mrs Johnson refused to cooperate, refusing to answer any questions. According to Mrs Johnson’s contact person, this symptom had been evident for quite some time before AAT. After AAT, Mrs Johnson was observed to cooperate much more in general; she gladly took her own initiative to engage in different activities and MMSE was performed without any problems. In addition, immediately after AAT, Mrs Johnson was considerably less distorted and restless. The change remained at 3 months of follow-up, implying that the contact with the therapy dog and the DH stimulated Mrs Johnson and that she experienced more well-being. The current results are supported by previous findings. 13 Other changes which were observed in Mrs Johnson seemed to be rather random and/or depending on the progress of her disease.
Mrs Johnson’s greater use of pain medication at the 3-month follow-up visit was notable. It is difficult to assess how pain affected her symptoms. It is possible that wandering and sleep disturbances, in particular, were consequences of the pain which she was in due to a facial tumor.
Strengths and Limitations
Some strengths and limitations need to be mentioned. To choose a single case design offers an opportunity to elucidate the exact effects of an intervention on an individual level, 28 which in this case was accomplished through systematic training with a certified therapy dog during a specific period of time. Through case studies, detailed and in-depth knowledge are obtained. The findings of a case study, thus, take research beyond statistical and quantitative variables. Instead, the description focuses on the individual. When both qualitative and quantitative data are used, case studies can be used to illustrate both a process and an outcome. 29 Considering this, we decided to carry out a single case study.
A methodological strength was that Mrs Johnson served as her own control with separate observations at baseline, immediately after AAT, and 2 follow-up observations. A second strength was the formulation of the intervention, which made it possible to individualize the training in accordance to each person’s needs and resources. Third, the longitudinal design is unique concerning research on AAT in dementia care.
However, some weaknesses need to be mentioned. First, the lack of research control, in particular that the circumstances around Mrs Johnson could not be controlled because the research team could not control potential influences from other sources or methods. Another weakness is that data were collected in “second hand.” That is, observer biases may have interfered with the observations, signifying reduced objectivity. In addition, it is possible that effects would have been more pronounced or prolonged if Mrs Johnson had trained more often or over a longer period of time. Finally, the major limitation of a case study is that the results from one single case cannot be generalized to other people with dementia. Still, it is possible that the single case may represent other people. Only further research will inform us about the extent to which the results of the present study are generalizable.
Conclusions
Currently, there are endeavors in dementia care to find methods that can complement or even constitute alternatives to pharmaceutical treatment, since psychotropic drugs and/or sedatives are assumed to reduce quality of life for people with dementia disease. Even if the present results are not possible to generalize, there is a tendency: physical, psychological, and/or social training with certified therapy dog teams can have effects on behavioral and psychological symptoms in people living with dementia.
Footnotes
Acknowledgments
The authors would like to thank Eskilstuna Municipality; the Social Contract (the City of Västerås, Eskilstuna Municipality, and Mälardalen University); and KPs Jubileumsfond for funding.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received financial support for the research, and/or publication of this article from Eskilstuna Municipality; the Social Contract (the City of Västerås, Eskilstuna Municipality, and Mälardalen University); and KPs Jubileumsfond.